
Early and Late Response and Glucocorticoid-Sparing Effect of Belimumab in Patients with Systemic Lupus Erythematosus with Joint and Skin Manifestations: Results from the Belimumab in Real Life Setting Study—Joint and Skin (BeRLiSS-JS)
 , , , , , , , , , , , , , , , , , , and
, , , , , , , , , , , , , , , , , , and
Abstract
:1. Introduction
2. Patients and Methods
2.1. Inclusion Criteria
2.2. Data Collection and Management
2.3. Outcome Measures
2.4. Statistical Analysis
3. Results
3.1. BeRLiSS Cohorts for Joint and Skin Involvement
3.2. Follow-Up Data
3.3. Joint Involvement
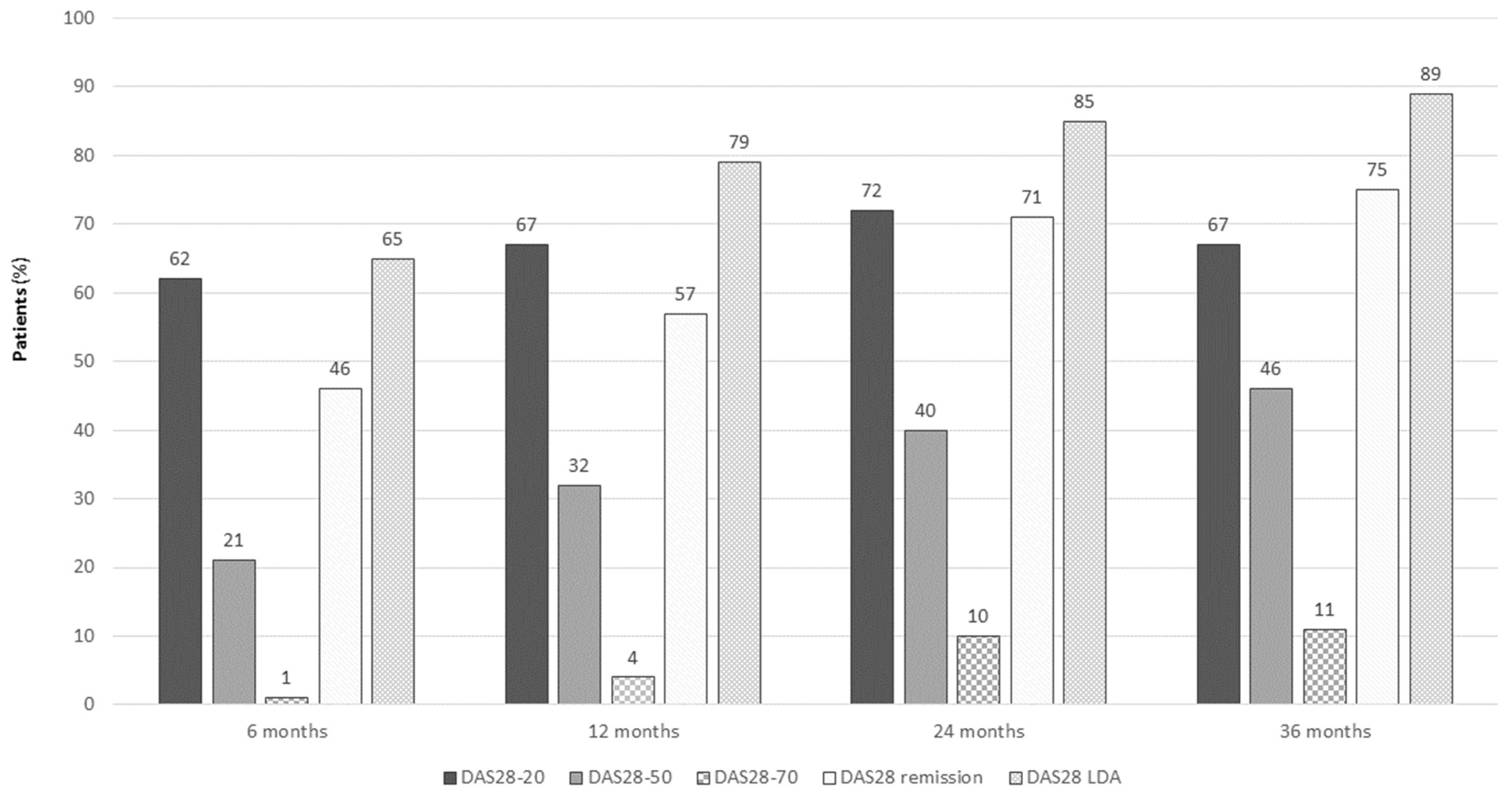
3.4. Efficacy of Belimumab in Patients with Joint Involvement
3.5. Skin Involvement
3.6. Efficacy of Belimumab in Patients with Skin Involvement
3.7. Multivariate Analyses of Baseline Predictors of DAS28 Remission, DAS28 LDA and CLASI = 0 at 6, 12, and 24 Months
3.8. Patients with Partial Response to Belimumab at 6 Months
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sarzi-Puttini, P.; Atzeni, F.; Iaccarino, L.; Doria, A. Environment and systemic lupus erythematosus: An overview. Autoimmunity 2005, 38, 465–472. [Google Scholar] [CrossRef]
- Nikoloudaki, M.; Nikolopoulos, D.; Koutsoviti, S.; Flouri, I.; Kapsala, N.; Repa, A.; Katsimbri, P.; Theotikos, E.; Pitsigavdaki, S.; Pateromichelaki, K.; et al. Clinical response trajectories and drug persistence in systemic lupus erythematosus patients on belimumab treatment: A real-life, multicentre observational study. Front. Immunol. 2023, 13, 1074044. [Google Scholar] [CrossRef]
- Trentin, F.; Gatto, M.; Zen, M.; Maddalena, L.; Nalotto, L.; Saccon, F.; Zanatta, E.; Iaccarino, L.; Doria, A. Effectiveness, Tolerability, and Safety of Belimumab in Patients with Refractory SLE: A Review of Observational Clinical-Practice-Based Studies. Clin. Rev. Allergy Immunol. 2018, 54, 331–343. [Google Scholar] [CrossRef]
- Iaccarino, L.; Andreoli, L.; Bocci, E.B.; Bortoluzzi, A.; Ceccarelli, F.; Conti, F.; De Angelis, R.; De Marchi, G.; De Vita, S.; Di Matteo, A.; et al. Clinical predictors of response and discontinuation of belimumab in patients with systemic lupus erythematosus in real life setting. Results of a large, multicentric, nationwide study. J. Autoimmun. 2018, 86, 1–8. [Google Scholar] [CrossRef]
- Iaccarino, L.; Bettio, S.; Reggia, R.; Zen, M.; Frassi, M.; Andreoli, L.; Gatto, M.; Piantoni, S.; Nalotto, L.; Franceschini, F.; et al. Effects of belimumab on flare rate and expected damage progression in patients with active systemic lupus erythematosus. Arthritis Care Res. 2017, 69, 115–123. [Google Scholar] [CrossRef]
- Wallace, D.J.; Ginzler, E.M.; Merrill, J.T.; Furie, R.A.; Stohl, W.; Chatham, W.W.; Weinstein, A.; Mckay, J.; McCune, W.J.; Petri, M.; et al. Safety and efficacy of belimumab plus standard therapy for up to thirteen years in patients with systemic lupus erythematosus. Arthritis Rheumatol. 2019, 71, 1125–1134. [Google Scholar] [CrossRef]
- Anjo, C.; Mascaró, J.-M., Jr.; Espinosa, G.; Cervera, R. Effectiveness and safety of belimumab in patients with systemic lupus erythematosus in a real-world setting. Scand. J. Rheumatol. 2019, 48, 469–473. [Google Scholar] [CrossRef]
- D’Cruz, D.; Eriksson, G.; Green, Y.; Hammer, A.; Ji, B.; Meizlik, P.; A Roth, D. Safety and efficacy of belimumab in older adults with SLE: Results of an integrated analysis of clinical trial data. Lupus Sci. Med. 2023, 10, e000830. [Google Scholar] [CrossRef]
- Fanouriakis, A.; Kostopoulou, M.; Alunno, A.; Aringer, M.; Bajema, I.; Boletis, J.N.; Cervera, R.; Doria, A.; Gordon, C.; Govoni, M.; et al. 2019 update of the EULAR recommendations for the management of systemic lupus erythematosus. Ann. Rheum. Dis. 2019, 78, 736–745. [Google Scholar] [CrossRef]
- Furie, R.; Rovin, B.H.; Houssiau, F.; Malvar, A.; Teng, Y.O.; Contreras, G.; Amoura, Z.; Yu, X.; Mok, C.-C.; Santiago, M.B.; et al. Two-Year, Randomized, Controlled Trial of Belimumab in Lupus Nephritis. N. Engl. J. Med. 2020, 383, 1117–1128. [Google Scholar] [CrossRef]
- Gatto, M.; Saccon, F.; Andreoli, L.; Bartoloni, E.; Benvenuti, F.; Bortoluzzi, A.; Bozzolo, E.; Brunetta, E.; Canti, V.; Cardinaletti, P.; et al. Durable renal response and safety with add-on belimumab in patients with lupus nephritis in real-life setting (BeRLiSS-LN). Results from a large, nationwide, multicentric cohort. J. Autoimmun. 2021, 124, 102729. [Google Scholar] [CrossRef]
- Gatto, M.; Saccon, F.; Zen, M.; Regola, F.; Fredi, M.; Andreoli, L.; Tincani, A.; Urban, M.L.; Emmi, G.; Ceccarelli, F.; et al. Early disease and low baseline damage as predictors of response to belimumab in patients with systemic lupus erythematosus in a real-life setting. Arthritis Rheumatol. 2020, 72, 1314–1324. [Google Scholar] [CrossRef]
- Zeher, M.; Doria, A.; Lan, J.; Aroca, G.; Jayne, D.; Boletis, I.; Hiepe, F.; Prestele, H.; Bernhardt, P.; Amoura, Z. Efficacy and safety of enteric-coated mycophenolate sodium in combination with two glucocorticoid regimens for the treatment of active lupus nephritis. Lupus 2011, 20, 1484–1493. [Google Scholar] [CrossRef]
- Depascale, R.; Gatto, M.; Zen, M.; Saccon, F.; Larosa, M.; Zanatta, E.; Bindoli, S.; Doria, A.; Iaccarino, L. Belimumab: A step forward in the treatment of systemic lupus erythematosus. Expert Opin. Biol. Ther. 2021, 21, 563–573. [Google Scholar] [CrossRef]
- Navarra, S.V.; Guzmán, R.M.; Gallacher, A.E.; Hall, S.; Levy, R.A.; Jimenez, R.E.; Li, E.K.-M.; Thomas, M.; Kim, H.-Y.; León, M.G.; et al. Efficacy and safety of belimumab in patients with active systemic lupus erythematosus: A randomised, placebo-controlled, phase 3 trial. Lancet 2011, 377, 721–731. [Google Scholar] [CrossRef]
- Furie, R.; Petri, M.; Zamani, O.; Cervera, R.; Wallace, D.J.; Tegzová, D.; Sanchez-Guerrero, J.; Schwarting, A.; Merrill, J.T.; Chatham, W.W.; et al. A phase III, randomized, placebo-controlled study of belimumab, a monoclonal antibody that inhibits B lymphocyte stimulator, in patients with systemic lupus erythematosus. Arthritis Rheum. 2011, 63, 3918–3920. [Google Scholar] [CrossRef]
- Manzi, S.; Sánchez-Guerrero, J.; Merrill, J.T.; Furie, R.; Gladman, D.; Navarra, S.V.; Ginzler, E.M.; D’Cruz, D.P.; Doria, A.; Cooper, S.; et al. Effects of belimumab, a B lymphocyte stimulator-specific inhibitor, on disease activity across multiple organ domains in patients with systemic lupus erythematosus: Combined results from two phase III trials. Ann. Rheum. Dis. 2012, 71, 1833–1838. [Google Scholar] [CrossRef]
- Albrecht, J.; Taylor, L.; Berlin, J.A.; Dulay, S.; Ang, G.; Fakharzadeh, S.; Kantor, J.; Kim, E.; Militello, G.; McGinnis, K.; et al. The CLASI (Cutaneous Lupus Erythematosus Disease Area and Severity Index): An outcome instrument for cutaneous lupus erythematosus. J. Investig. Dermatol. 2005, 125, 889–894. [Google Scholar] [CrossRef]
- Mosca, M.; Tani, C.; Aringer, M.; Bombardieri, S.; Boumpas, D.T.; Brey, R.L.; Cervera, R.; Doria, A.; Jayne, D.; A Khamashta, M.; et al. European League Against Rheumatism recommendations for monitoring patients with systemic lupus erythematosus in clinical practice and in observational studies. Ann. Rheum. Dis. 2010, 69, 1269–1274. [Google Scholar] [CrossRef]
- Zen, M.; Iaccarino, L.; Gatto, M.; Bettio, S.; Saccon, F.; Ghirardello, A.; Punzi, L.; Doria, A. The effect of different durations of remission on damage accrual: Results from a prospective monocentric cohort of Caucasian patients. Ann. Rheum. Dis. 2017, 76, 562–565. [Google Scholar] [CrossRef]
- Ugarte-Gil, M.F.; Hanly, J.; Urowitz, M.; Gordon, C.; Bae, S.-C.; Romero-Diaz, J.; Sanchez-Guerrero, J.; Bernatsky, S.; Clarke, A.E.; Wallace, D.J.; et al. Remission and low disease activity (LDA) prevent damage accrual in patients with systemic lupus erythematosus: Results from the Systemic Lupus International Collaborating Clinics (SLICC) inception cohort. Ann. Rheum. Dis. 2022, 81, 1541–1548. [Google Scholar] [CrossRef]
- Zen, M.; Bassi, N.; Nalotto, L.; Canova, M.; Bettio, S.; Gatto, M.; Ghirardello, A.; Iaccarino, L.; Punzi, L.; Doria, A. Disease activity patterns in a monocentric cohort of SLE patients: A seven-year follow-up study. Clin. Exp. Rheumatol. 2012, 30, 856–863. [Google Scholar]
- Baker, K.P.; Edwards, B.M.; Main, S.H.; Choi, G.H.; Wager, R.E.; Halpern, W.G.; Lappin, P.B.; Riccobene, T.; Abramian, D.; Sekut, L.; et al. Generation and characterization of LymphoStat-B, a human monoclonal antibody that antagonizes the bioactivities of B lymphocyte stimulator. Arthritis Rheum. 2003, 48, 3253–3265. [Google Scholar] [CrossRef]
- Wilkinson, C.; Henderson, R.B.; Jones-Leone, A.R.; Flint, S.M.; Lennon, M.; Levy, R.A.; Ji, B.; Bass, D.L.; Roth, D. The role of baseline BLyS levels and type 1 interferon-inducible gene signature status in determining belimumab response in systemic lupus erythematosus: A post hoc meta-analysis. Arthritis Res. Ther. 2020, 22, 102. [Google Scholar] [CrossRef]
- Petri, M.; Stohl, W.; Chatham, W.; Joseph McCune, W.; Chevrier, M.; Ryel, J.; Recta, V.; Zhong, J.; Freimuth, W. Association of BLyS™ with measures of disease activity in a prospective SLE observational study. Arthritis Rheum. 2004, 50, S603. [Google Scholar] [CrossRef]
- de Vos, L.; Guel, T.; Niebel, D.; Bald, S.; ter Steege, A.; Bieber, T.; Wenzel, J. Characterization of B cells in lupus erythematosus skin biopsies in the context of different immune cell infiltration patterns. Front. Med. 2022, 9, 1037408. [Google Scholar] [CrossRef]
- Itotagawa, E.; Tomofuji, Y.; Kato, Y.; Konaka, H.; Tsujimoto, K.; Park, J.; Nagira, D.; Hirayama, T.; Jo, T.; Hirano, T.; et al. SLE stratification based on BAFF and IFN-I bioactivity for biologics and implications of BAFF produced by glomeruli in lupus nephritis. Rheumatology 2022, keac528. [Google Scholar] [CrossRef]
- Sada, K.-E.; Katayama, Y.; Asano, Y.; Hayashi, K.; Miyawaki, Y.; Ohashi, K.; Katsuyama, E.; Katsuyama, T.; Takano-Narazaki, M.; Matsumoto, Y.; et al. Association of one-point glucocorticoid-free status with chronic damage and disease duration in systemic lupus erythematosus: A cross-sectional study. Lupus Sci. Med. 2022, 9, e000772. [Google Scholar] [CrossRef]
- Tselios, K.; Gladman, D.D.; Su, J.; Urowitz, M.B. Gradual Glucocorticosteroid Withdrawal Is Safe in Clinically Quiescent Systemic Lupus Erythematosus. ACR Open Rheumatol. 2021, 3, 550–557. [Google Scholar] [CrossRef]
- Urowitz, M.; Ohsfeldt, R.L.; Wielage, R.; Kelton, K.A.; Asukai, Y.; Ramachandran, S. A propensity scorematched study of organ damage in patients with systemic lupus erythematosus from the BLISS long-term extension trials versus the toronto lupus cohort: A post hoc longitudinal analysis [abstract no 2923]. Arthritis Rheumatol. 2017, 69 (Suppl. S10), 4217–4218. [Google Scholar]
- Rinaldi, S.; Doria, A.; Salaffi, F.; Ermani, M.; Iaccarino, L.; Ghirardello, A.; Zampieri, S.; Sarzi-Puttini, P.; Gambari, P.F.; Perini, G. Health-related quality of life in Italian patients with systemic lupus erythematosus. I. Relationship between physical and mental dimension and impact of age. Rheumatology 2004, 43, 1574–1579. [Google Scholar] [CrossRef]
- Emamikia, S.; Oon, S.; Gomez, A.; Lindblom, J.; Borg, A.; Enman, Y.; Morand, E.; Grannas, D.; van Vollenhoven, R.F.; Nikpour, M.; et al. Impact of remission and low disease activity on health-related quality of life in patients with systemic lupus erythematosus. Rheumatology 2022, 61, 4752–4762. [Google Scholar] [CrossRef]
- Briani, C.; Lucchetta, M.; Ghirardello, A.; Toffanin, E.; Zampieri, S.; Ruggero, S.; Scarlato, M.; Quattrini, A.; Bassi, N.; Ermani, M.; et al. Neurolupus is associated with anti-ribosomal P protein antibodies: An inception cohort study. J. Autoimmun. 2009, 32, 79–84. [Google Scholar] [CrossRef]
- Reddy, V.; Jayne, D.; Close, D.; Isenberg, D. B-cell depletion in SLE: Clinical and trial experience with rituximab and ocrelizumab and implications for study design. Arthritis Res. Ther. 2013, 15 (Suppl. S1), 1–16. [Google Scholar] [CrossRef]
- Petri, M.; Bruce, I.N.; Dörner, T.; Tanaka, Y.; Morand, E.F.; Kalunian, K.C.; Cardiel, M.H.; E Silk, M.; Dickson, C.L.; Meszaros, G.; et al. Baricitinib for systemic lupus erythematosus: A double-blind, randomised, placebo-controlled, phase 3 trial (SLE-BRAVE-II). Lancet 2023, 401, 1011–1019. [Google Scholar] [CrossRef]
- A Furie, R.; Morand, E.F.; Bruce, I.N.; Manzi, S.; Kalunian, K.C.; Vital, E.M.; Ford, T.L.; Gupta, R.; Hiepe, F.; Santiago, M.; et al. Type I interferon inhibitor anifrolumab in active systemic lupus erythematosus (TULIP-1): A randomised, controlled, phase 3 trial. Lancet Rheumatol. 2019, 1, e208–e219. [Google Scholar] [CrossRef]
- Zen, M.; Iaccarino, L.; Gatto, M.; Saccon, F.; LaRosa, M.; Ghirardello, A.; Punzi, L.; Doria, A. Lupus low disease activity state is associated with a decrease in damage progression in Caucasian patients with SLE, but overlaps with remission. Ann. Rheum. Dis. 2017, 77, 104–110. [Google Scholar] [CrossRef]
- Levy, R.A.; Gonzalez-Rivera, T.; Khamashta, M.; Fox, N.L.; Jones-Leone, A.; Rubin, B.; Burriss, S.W.; Gairy, K.; van Maurik, A.; Roth, D.A. 10 Years of belimumab experience: What have we learnt? Lupus 2021, 30, 1705–1721. [Google Scholar] [CrossRef]
- Morand, E.F.; Furie, R.; Tanaka, Y.; Bruce, I.N.; Askanase, A.D.; Richez, C.; Bae, S.-C.; Brohawn, P.Z.; Pineda, L.; Berglind, A.; et al. Trial of anifrolumab in active systemic lupus erythematosus. N. Engl. J. Med. 2020, 382, 211–221. [Google Scholar] [CrossRef]
- Doria, A.; Mosca, M.; Gambari, P.F.; Bombardieri, S. Defining unclassifiable connective tissue diseases: Incomplete, undifferentiated, or both? J. Rheumatol. 2005, 32, 213–215. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Joint Involvement | Skin Involvement | |
|---|---|---|
| Total patients, n (%) | 277 (100) | 151 (100) |
| Female, n (%) | 255 (92) | 140 (92.7) |
| Age at diagnosis, mean ± SD years | 30.22 ± 11.6 | 29.3 ± 11.1 |
| Age at belimumab initiation, mean ± SD years | 42.22 ± 11.8 | 40.6 ± 10.4 |
| Disease duration, mean ± SD years | 12 ± 9 | 11 ± 9 |
| Disease duration ≤ 2 years, n (%) | 47 (17) | 28 (18.5) |
| Total months follow-up, mean ± SD | 23.42 ± 14.44 | 25.2 ± 15.9 |
| SLEDAI-2K score, mean ± SD | 10 ± 3.0 | 10.0 ± 4.0 |
| SLEDAI-2K ≥ 10, n (%) | 129 (46.6) | 93 (61.6) |
| c-SLEDAI, mean ± SD | 6.23 ± 2.8 | 6.58 ± 3.4 |
| SDI, median (25–75%) | 1 (0–2) | 1 (0–1) |
| Chronic active pattern, n (%) | 100 (36.1) | 61 (40.4) |
| Smoking, n (%) | 51 (19.6) | 32 (21.9) |
| Antiphospholipid syndrome, n (%) | 44 (16.2) | 16 (10.9) |
| CLASI, median (IQR) | - | 4 (3–7) |
| DAS28, mean ± SD | 3.9 ± 4.2 | - |
| Serology | ||
| Anti-dsDNA, n (%) | 222 (90.7) | 125 (82.8) |
| Anti-Sm, n (%) | 70 (25.4) | 45 (30) |
| Anti-SSA, n (%) | 125 (45.3) | 84 (56) |
| Anti-SSB, n (%) | 49 (17.8) | 38 (25.3) |
| Anti-U1RNP, n (%) | 87 (31.5) | 53 (35.3) |
| Anti-P-ribosomal | 17(6.2) | 11 (7.3) |
| Antiphospholipid, n (%) | 95 (34.7) | 43 (28.7) |
| Low C3, mean ± SD (range) | 72.05 ± 22.83 | 70.01 ± 25.50 |
| Low C4, mean ± SD (range) | 11.25 ± 6.38 | 11.54 ± 7.67 |
| Concomitant treatment | ||
| Oral glucocorticoids | ||
| Daily PDN intake, mean ± SD mg | 10.15 ± 6.92 | 11.05 ± 8.15 |
| Daily PDN intake ≤ 5 mg, n (%) | 92 (33.2) | 41 (27.2) |
| Antimalarials, n (%) | 184 (66.4) | 110 (72.8) |
| Immunosuppressants, n (%) | 178 (64.3) | 97 (64.2) |
| Joint Involvement | Skin Involvement | |||
|---|---|---|---|---|
| Months | Patients in Follow-Up * | Patients Discontinuing Belimumab in the 6 Months before the Timepoint ** | Patients in Follow-Up * | Patients Discontinuing Belimumab in the 6 Months before the Timepoint ** |
| 6 months | 272 | 5 | 147 | 4 |
| 12 months | 215 | 36 | 118 | 20 |
| 24 months | 114 | 24 | 69 | 11 |
| 36 months | 59 | 15 | 42 | 7 |
| 48 months | 28 | 4 | 23 | 3 |
| A | ||||||
| DAS28 Remission at 6 Months | DAS28 Remission at 12 Months | DAS28 Remission at 24 Months | ||||
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| DAS28 | 1.02 (0.38–2.74) | 0.960 | 0.56 (0.427–0.735) | <0.001 | 0.54 (0.37–0.79) | 0.001 |
| Disease Duration | 1.09 (0.96–1.23) | 0.168 | 0.94 (0.91–0.99) | 0.008 | 1.030 (0.97–1.09) | 0.330 |
| Low C3 | 0.98 (0.93–1.04) | 0.551 | 1.002 (0.99–1.02) | 0.733 | 0.99 (0.98–1.02) | 0.812 |
| Smoke | 6.90 (0.63–72.86 | 0.113 | 0.52 (0.23–1.17) | 0.115 | - | - |
| SLEDAI-2K | 1.173 (0.816–1.686) | 0.389 | 0.92 (0.83–1.02) | 0.128 | 0.88 (0.74–1.04) | 0.135 |
| B | ||||||
| DAS28 LDA at 6 Months | DAS28 LDA at 12 Months | DAS28 LDA at 24 Months | ||||
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| DAS28 | 1.04 (0.91–1.19) | <0.001 | 0.59 (0.44–0.80) | <0.001 | 0.57 (0.39–0.89) | 0.011 |
| Disease Duration | 0.99 (0.95–1.04) | 0.751 | 0.94 (0.91–0.99) | 0.008 | 0.99 (0.92–1.07) | 0.783 |
| Low C3 | 1.01 (0.99–1.03) | 0.244 | 1.00 (0.99–1.02) | 0.576 | 0.99 (0.97–1.01) | 0.458 |
| Smoke | 2.69 (1.03–7.023) | 0.044 | 0.87 (0.34–2.21) | 0.076 | - | - |
| SLEDAI-2K | 1.04 (0.91–1.19) | 0.536 | 0.95 (0.91–0.99) | 0.412 | 1.05 (0.85–1.29) | 0.669 |
| CLASI Remission at 6 Months | CLASI Remission at 12 Months | CLASI Remission24 Months | ||||
|---|---|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI | p-Value | OR (95% CI) | p-Value | |
| CLASI | 0.71 (0.60–0.83) | <0.001 | 0.83 (0.73–0.93) | 0.002 | 0.78 (0.64–0.95) | 0.014 |
| Disease Duration | 0.94 (0.89–0.93) | 0.026 | 0.98 (0.93–1.03) | 0.397 | 0.91 (0.87–1.00) | 0.057 |
| SLEDAI 2K | 1.08 (0.97–1.21) | 0.244 | 1.01 (0.89–1.15) | 0.875 | 0.99 (0.81–1.22) | 0.997 |
| Anti-dsDNA | - | - | 1.82 (0.58–5.73) | 0.308 | 0.73 (0.14–3.86) | 0.715 |
| Low C3 | - | - | 3.11 (1.10–8.92) | 0.033 | 2.13 (0.46–9.80) | 0.331 |
| HCQ baseline | 0.70 (0.29–1.68) | 0.424 | 0.98 (0.38–2.54) | 0.969 | 0.92 (0.23–3.77) | 0.912 |
| Variables at 6 Months | DAS28 Remission at 12 Months | DAS28 Remission at 24 Months | ||
|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| DAS28 < 3.2 | 2.69 (1.03–7.00) | 0.043 | 1.07 (0.99–1.16) | 0.067 |
| Disease Duration | 0.97 (0.94–1.02) | 0.269 | 0.94 (0.91–0.99) | 0.013 |
| Low C3 | 0.99 (0.97–1.01) | 0.222 | 0.98 (0.950–1.01) | 0.163 |
| Low C4 | 0.97 (0.91–1.03) | 0.348 | 1.05(0.96–1.16) | 0.291 |
| SLEDAI-2K | 0.95 (0.81–1.11) | 0.497 | 0.83 (0.67–1.03) | 0.089 |
| Anti-dsDNA | 1.51 (0.45–4.99) | 0.502 | 2.88 (0.43–1.92) | 0.275 |
| Prednisone | 0.94 (0.84–1.06) | 0.330 | 0.92 (0.76–1.11) | 0.380 |
| Variables at 6 Months | CLASI Remission at 12 Months | CLASI Remission at 24 Months | ||
|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| CLASI | 0.69 (0.49–0.98) | 0.041 | 0.74 (0.49–1.11) | 0.145 |
| Low C3 | 0.99 (0.97–1.02) | 0.658 | 0.98 (0.94–1.02) | 0.576 |
| Low C4 | 0.94 (0.86–1.03) | 0.199 | 0.96 (0.87–1.07) | 0.481 |
| Anti-dsDNA | 2.33 (0.48–11.28) | 0.292 | 3.80 (0.41–34.87) | 0.238 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zen, M.; Gatto, M.; Depascale, R.; Regola, F.; Fredi, M.; Andreoli, L.; Franceschini, F.; Urban, M.L.; Emmi, G.; Ceccarelli, F.; et al. Early and Late Response and Glucocorticoid-Sparing Effect of Belimumab in Patients with Systemic Lupus Erythematosus with Joint and Skin Manifestations: Results from the Belimumab in Real Life Setting Study—Joint and Skin (BeRLiSS-JS). J. Pers. Med. 2023, 13, 691. https://doi.org/10.3390/jpm13040691
Zen M, Gatto M, Depascale R, Regola F, Fredi M, Andreoli L, Franceschini F, Urban ML, Emmi G, Ceccarelli F, et al. Early and Late Response and Glucocorticoid-Sparing Effect of Belimumab in Patients with Systemic Lupus Erythematosus with Joint and Skin Manifestations: Results from the Belimumab in Real Life Setting Study—Joint and Skin (BeRLiSS-JS). Journal of Personalized Medicine. 2023; 13(4):691. https://doi.org/10.3390/jpm13040691
Chicago/Turabian StyleZen, Margherita, Mariele Gatto, Roberto Depascale, Francesca Regola, Micaela Fredi, Laura Andreoli, Franco Franceschini, Maria Letizia Urban, Giacomo Emmi, Fulvia Ceccarelli, and et al. 2023. "Early and Late Response and Glucocorticoid-Sparing Effect of Belimumab in Patients with Systemic Lupus Erythematosus with Joint and Skin Manifestations: Results from the Belimumab in Real Life Setting Study—Joint and Skin (BeRLiSS-JS)" Journal of Personalized Medicine 13, no. 4: 691. https://doi.org/10.3390/jpm13040691