


Immune Response and Transplacental Antibody Transfer in Pregnant Women after COVID-19 Vaccination
 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
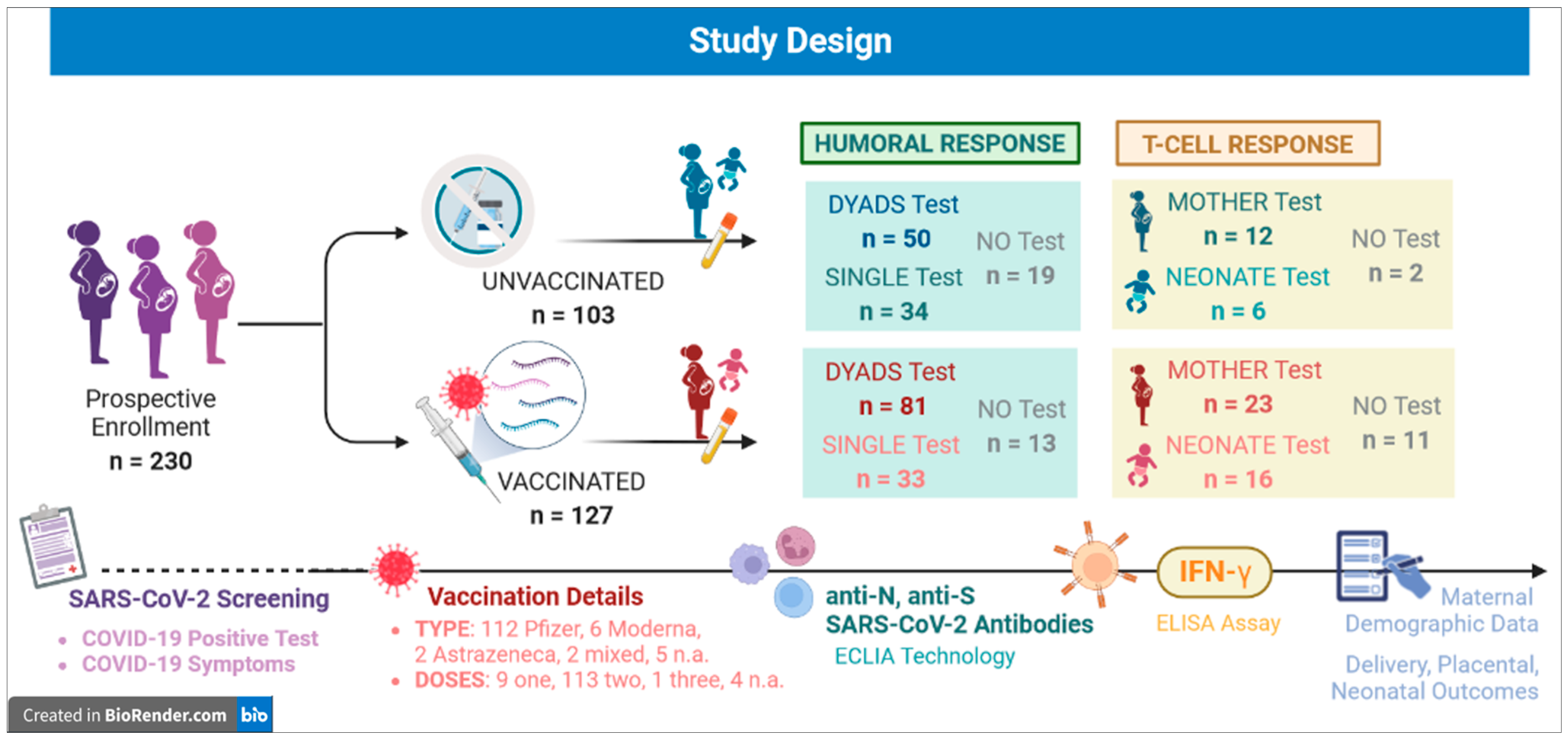
2.1. Study Population
2.2. SARS-CoV-2 Anti-N and Anti-S Antibody Measurement
2.3. Anti-SARS-CoV-2 Evaluation of T-Cell Response
2.4. Statistical Analysis
3. Results
3.1. Study Population
3.2. Serological Screening for Pre-Study Undiagnosed SARS-CoV-2 Infections
3.3. Humoral Response to Anti-SARS-CoV-2 Vaccination
3.4. Anti-SARS-CoV-2 T-Cell Response Evaluation
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Villar, J.; Ariff, S.; Gunier, R.B.; Thiruvengadam, R.; Rauch, S.; Kholin, A.; Roggero, P.; Prefumo, F.; Vale, M.S.D.; Cardona-Perez, J.A.; et al. Maternal and Neonatal Morbidity and Mortality Among Pregnant Women With and Without COVID-19 Infection: The INTERCOVID Multinational Cohort Study. JAMA Pediatr. 2021, 175, 817–826, Erratum in JAMA Pediatr. 2022, 176, 104. [Google Scholar] [CrossRef] [PubMed]
- Allotey, J.; Stallings, E.; Bonet, M.; Yap, M.; Chatterjee, S.; Kew, T.; Debenham, L.; Llavall, A.C.; Dixit, A.; Zhou, D.; et al. Clinical manifestations, risk factors, and maternal and perinatal outcomes of coronavirus disease 2019 in pregnancy: Living systematic review and meta-analysis. BMJ 2020, 370, m3320, Erratum in BMJ 2022, 377, o1205. [Google Scholar] [CrossRef]
- Savasi, V.M.; Parisi, F.; Patanè, L.; Ferrazzi, E.; Frigerio, L.; Pellegrino, A.; Spinillo, A.; Tateo, S.; Ottoboni, M.; Veronese, P.; et al. Clinical Findings and Disease Severity in Hospitalized Pregnant Women With Coronavirus Disease 2019 (COVID-19). Obstet. Gynecol. 2020, 136, 252–258. [Google Scholar] [CrossRef]
- Donati, S.; Corsi, E.; Maraschini, A.; Salvatore, M.A.; Arena, M.G.; Boldrini, R.; Brunelli, R.; Cagnacci, A.; Casucci, P.; Cetin, I.; et al. SARS-CoV-2 infection among hospitalised pregnant women and impact of different viral strains on COVID-19 severity in Italy: A national prospective population-based cohort study. BJOG Int. J. Obstet. Gynaecol. 2022, 129, 221–231. [Google Scholar] [CrossRef] [PubMed]
- Woodworth, K.R.; Olsen, E.O.; Neelam, V.; Lewis, E.L.; Galang, R.R.; Oduyebo, T.; Aveni, K.; Yazdy, M.M.; Harvey, E.; Longcore, N.D.; et al. Birth and Infant Outcomes Following Laboratory-Confirmed SARS-CoV-2 Infection in Pregnancy—SET-NET, 16 Jurisdictions, March 29–October 14, 2020. MMWR. Morb. Mortal. Wkly. Rep. 2020, 69, 1635–1640. [Google Scholar] [CrossRef]
- Swamy, G.K.; Garcia-Putnam, R. Maternal Immunization to Benefit the Mother, Fetus, and Infant. Obstet. Gynecol. Clin. N. Am. 2014, 41, 521–534. [Google Scholar] [CrossRef]
- Fouda, G.G.; Martinez, D.R.; Swamy, G.K.; Permar, S.R. The Impact of IgG Transplacental Transfer on Early Life Immunity. Immunohorizons 2018, 2, 14–25. [Google Scholar] [CrossRef] [PubMed]
- Trostle, M.E.; Aguero-Rosenfeld, M.E.; Roman, A.S.; Lighter, J.L. High antibody levels in cord blood from pregnant women vaccinated against COVID-19. Am. J. Obstet. Gynecol. MFM 2021, 3, 100481. [Google Scholar] [CrossRef]
- Prasad, S.; Kalafat, E.; Blakeway, H.; Townsend, R.; O’brien, P.; Morris, E.; Draycott, T.; Thangaratinam, S.; Le Doare, K.; Ladhani, S.; et al. Systematic review and meta-analysis of the effectiveness and perinatal outcomes of COVID-19 vaccination in pregnancy. Nat. Commun. 2022, 13, 2414. [Google Scholar] [CrossRef]
- Kalafat, E.; Heath, P.; Prasad, S.; Brien, P.O.; Khalil, A. COVID-19 vaccination in pregnancy. Am. J. Obstet. Gynecol. 2022, 227, 136–147. [Google Scholar] [CrossRef]
- Italian Society of Gynecology and Obstetrics (SIGO). Position Paper: Gravidanza e Vaccinazione anti COVID. Rome. 2021. Available online: https://www.sigo.it/wp-content/uploads/2021/05/PositionPaper_Gravidanza_Vaccinazione_anti_COVID_05.05.2021.pdf (accessed on 5 May 2021).
- Centers for Disease Control and Prevention (CDC). Available online: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/recommendations/pregnancy.html (accessed on 22 August 2021).
- The American College of Obstetricians and Gynecologists (ACOG). Available online: https://www.acog.org/clinical/clinical-guidance/practice-advisory/articles/2020/12/covid-19-vaccination-considerations-for-obstetric-gynecologic-care (accessed on 22 August 2021).
- Goldshtein, I.; Nevo, D.; Steinberg, D.M.; Rotem, R.S.; Gorfine, M.; Chodick, G.; Segal, Y. Association Between BNT162b2 Vaccination and Incidence of SARS-CoV-2 Infection in Pregnant Women. JAMA 2021, 12, e2111035. [Google Scholar] [CrossRef] [PubMed]
- Gray, K.J.; Bordt, E.A.; Atyeo, C.; Deriso, E.; Akinwunmi, B.; Young, N.; Baez, A.M.; Shook, L.L.; Cvrk, D.; James, K.; et al. Coronavirus disease 2019 vaccine response in pregnant and lactating women: A cohort study. Am. J. Obstet. Gynecol. 2021, 225, 303.e1–303.e17. [Google Scholar] [CrossRef] [PubMed]
- Cetin, I.; Mandalari, M.; Cesari, E.; Borriello, C.R.; Ercolanoni, M.; Preziosi, G. SARS-CoV-2 Vaccine Uptake during Pregnancy in Regione Lombardia, Italy: A Population-Based Study of 122,942 Pregnant Women. Vaccines 2022, 10, 1369. [Google Scholar] [CrossRef] [PubMed]
- Siegel, M.R.; Lumbreras-Marquez, M.I.; James, K.; McBay, B.R.; Gray, K.J.; Schantz-Dunn, J.; Diouf, K.; Goldfarb, I.T. Perceptions and Attitudes toward COVID-19 Vaccination among Pregnant and Postpartum Individuals. Am. J. Perinatol. 2022, 29, 1489–1495. [Google Scholar] [CrossRef]
- Azami, M.; Nasirkandy, M.P.; Ghaleh, H.E.G.; Ranjbar, R. COVID-19 vaccine acceptance among pregnant women worldwide: A systematic review and meta-analysis. PLoS ONE 2022, 17, e0272273. [Google Scholar] [CrossRef]
- Lubrano, C.; Vilca, L.M.; Coco, C.; Schirripa, I.; Zuliani, P.L.; Corneo, R.; Pavone, G.; Pellegrino, A.; Vignali, M.; Savasi, V.; et al. Pregnant women’s acceptance and views on COVID-19 vaccine in Northern Italy. J. Obstet. Gynaecol. 2022, 43, 2139596. [Google Scholar] [CrossRef]
- Keski-Nisula, L.; Hirvonen, M.-R.; Roponen, M.; Heinonen, S.; Pekkanen, J. Maternal and neonatal IL-4 and IFN-gamma production at delivery and 3 months after birth. J. Reprod. Immunol. 2003, 60, 25–33. [Google Scholar] [CrossRef]
- Molodtsov, I.A.; Kegeles, E.; Mitin, A.N.; Mityaeva, O.; Musatova, O.E.; Panova, A.E.; Pashenkov, M.V.; Peshkova, I.O.; Alsalloum, A.; Asaad, W.; et al. Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2)-Specific T Cells and Antibodies in Coronavirus Disease 2019 (COVID-19) Protection: A Prospective Study. Clin. Infect Dis. 2022, 75, e1–e9. [Google Scholar] [CrossRef]
- Fernández-González, M.; Agulló, V.; Padilla, S.; García, J.A.; García-Abellán, J.; Botella, Á.; Mascarell, P.; Ruiz-García, M.; Masiá, M.; Gutiérrez, F. Clinical Performance of a Standardized Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Interferon-γ Release Assay for Simple Detection of T-Cell Responses After Infection or Vaccination. Clin. Infect Dis. 2022, 75, e338–e346. [Google Scholar] [CrossRef]
- Sauer, K.; Harris, T. An Effective COVID-19 Vaccine Needs to Engage T Cells. Front. Immunol. 2020, 11, 581807. [Google Scholar] [CrossRef]
- McMahan, K.; Yu, J.; Mercado, N.B.; Loos, C.; Tostanoski, L.H.; Chandrashekar, A.; Liu, J.; Peter, L.; Atyeo, C.; Zhu, A.; et al. Correlates of protection against SARS-CoV-2 in rhesus macaques. Nature 2021, 590, 630–634. [Google Scholar] [CrossRef] [PubMed]
- Stephenson, K.E.; Le Gars, M.; Sadoff, J.; de Groot, A.M.; Heerwegh, D.; Truyers, C.; Atyeo, C.; Loos, C.; Chandrashekar, A.; McMahan, K.; et al. Immunogenicity of the Ad26.COV2.S Vaccine for COVID-19. JAMA 2021, 325, 1535–1544. [Google Scholar] [CrossRef] [PubMed]
- Kruse, M.; Dark, C.; Aspden, M.; Cochrane, D.; Competiello, R.; Peltz, M.; Torres, L.; Wrighton-Smith, P.; Dudek, M. Performance of the T-SPOT®.COVID test for detecting SARS-CoV-2-responsive T cells. Int. J. Infect. Dis. 2021, 113, 155–161. [Google Scholar] [CrossRef] [PubMed]
- Jaganathan, S.; Stieber, F.; Rao, S.N.; Nikolayevskyy, V.; Manissero, D.; Allen, N.; Boyle, J.; Howard, J. Preliminary Evaluation of QuantiFERON SARS-CoV-2 and QIAreach Anti-SARS-CoV-2 Total Test in Recently Vaccinated Individuals. Infect. Dis. Ther. 2021, 10, 2765–2776. [Google Scholar] [CrossRef]
- Vogrig, M.; Berger, A.-E.; Bourlet, T.; Waeckel, L.; Haccourt, A.; Chanavat, A.; Hupin, D.; Roche, F.; Botelho-Nevers, E.; Pozzetto, B.; et al. Monitoring of Both Humoral and Cellular Immunities Could Early Predict COVID-19 Vaccine Efficacy Against the Different SARS-CoV-2 Variants. J. Clin. Immunol. 2023, 43, 31–45. [Google Scholar] [CrossRef] [PubMed]
- Mileto, D.; Fenizia, C.; Cutrera, M.; Gagliardi, G.; Gigantiello, A.; De Silvestri, A.; Rizzo, A.; Mancon, A.; Bianchi, M.; De Poli, F.; et al. SARS-CoV-2 mRNA vaccine BNT162b2 triggers a consistent cross-variant humoral and cellular response. Emerg. Microbes Infect. 2021, 10, 2235–2243. [Google Scholar] [CrossRef]
- Ward, H.; Whitaker, M.; Flower, B.; Tang, S.N.; Atchison, C.; Darzi, A.; Donnelly, C.A.; Cann, A.; Diggle, P.J.; Ashby, D.; et al. Population antibody responses following COVID-19 vaccination in 212,102 individuals. Nat. Commun. 2022, 13, 907. [Google Scholar] [CrossRef]
- Wei, J.; Stoesser, N.; Matthews, P.C.; Ayoubkhani, D.; Studley, R.; Bell, I.; Bell, J.I.; Newton, J.N.; Farrar, J.; Diamond, I.; et al. Antibody responses to SARS-CoV-2 vaccines in 45,965 adults from the general population of the United Kingdom. Nat. Microbiol. 2021, 6, 1140–1149. [Google Scholar] [CrossRef]
- Atyeo, C.G.; Shook, L.L.; Brigida, S.; De Guzman, R.M.; Demidkin, S.; Muir, C.; Akinwunmi, B.; Baez, A.M.; Sheehan, M.L.; McSweeney, E.; et al. Maternal immune response and placental antibody transfer after COVID-19 vaccination across trimester and platforms. Nat. Commun. 2022, 13, 3571. [Google Scholar] [CrossRef]
- Prabhu, M.; Yang, Y.J.; Johnston, C.D.; Murphy, E.A.; Ketas, T.J.; Diaz-Tapia, R.; Jurkiewicz, M.; Racine-Brzostek, S.; Mohammed, I.; Sukhu, A.C.; et al. Longitudinal antibody response kinetics following SARS-CoV-2 messenger RNA vaccination in pregnant and nonpregnant persons. Am. J. Obstet. Gynecol. MFM 2022, 5, 100796. [Google Scholar] [CrossRef]
- Nunhofer, V.; Weidner, L.; Hoeggerl, A.D.; Zimmermann, G.; Badstuber, N.; Grabmer, C.; Jungbauer, C.; Lindlbauer, N.; Held, N.; Pascariuc, M.; et al. Persistence of Naturally Acquired and Functional SARS-CoV-2 Antibodies in Blood Donors One Year after Infection. Viruses 2022, 14, 637. [Google Scholar] [CrossRef] [PubMed]
- Korobova, Z.R.; Zueva, E.V.; Arsentieva, N.A.; Batsunov, O.K.; Liubimova, N.E.; Khamitova, I.V.; Kuznetsova, R.N.; Rubinstein, A.A.; Savin, T.V.; Stanevich, O.V.; et al. Changes in Anti-SARS-CoV-2 IgG Subclasses over Time and in Association with Disease Severity. Viruses 2022, 14, 941. [Google Scholar] [CrossRef] [PubMed]
- Van Elslande, J.; Oyaert, M.; Lorent, N.; Weygaerde, Y.V.; Van Pottelbergh, G.; Godderis, L.; Van Ranst, M.; André, E.; Padalko, E.; Lagrou, K.; et al. Lower persistence of anti-nucleocapsid compared to anti-spike antibodies up to one year after SARS-CoV-2 infection. Diagn. Microbiol. Infect. Dis. 2022, 103, 115659. [Google Scholar] [CrossRef]
- Bergeri, I.; Whelan, M.G.; Ware, H.; Subissi, L.; Nardone, A.; Lewis, H.C.; Li, Z.; Ma, X.; Valenciano, M.; Cheng, B.; et al. Global SARS-CoV-2 seroprevalence from January 2020 to April 2022: A systematic review and meta-analysis of standardized population-based studies. PLoS Med. 2022, 19, e1004107. [Google Scholar] [CrossRef] [PubMed]
- Tasca, C.; Rossi, R.S.; Corti, S.; Anelli, G.M.; Savasi, V.; Brunetti, F.; Cardellicchio, M.; Caselli, E.; Tonello, C.; Vergani, P.; et al. Placental pathology in COVID-19 affected pregnant women: A prospective case-control study. Placenta 2021, 110, 9–15. [Google Scholar] [CrossRef]
- Hayward, C.E.; Lean, S.; Sibley, C.P.; Jones, R.L.; Wareing, M.; Greenwood, S.L.; Dilworth, M.R. Placental Adaptation: What Can We Learn from Birthweight:Placental Weight Ratio? Front. Physiol. 2016, 7, 28. [Google Scholar] [CrossRef]
- Bianchi, C.; Taricco, E.; Cardellicchio, M.; Mandò, C.; Massari, M.; Savasi, V.; Cetin, I. The role of obesity and gestational diabetes on placental size and fetal oxygenation. Placenta 2021, 103, 59–63. [Google Scholar] [CrossRef]
- Mandò, C.; Calabrese, S.; Mazzocco, M.I.; Novielli, C.; Anelli, G.M.; Antonazzo, P.; Cetin, I. Sex specific adaptations in placental biometry of overweight and obese women. Placenta 2016, 38, 1–7. [Google Scholar] [CrossRef]
- Salavati, N.; Gordijn, S.; Sovio, U.; Zill-E-Huma, R.; Gebril, A.; Charnock-Jones, D.; Scherjon, S.; Smith, G. Birth weight to placenta weight ratio and its relationship to ultrasonic measurements, maternal and neonatal morbidity: A prospective cohort study of nulliparous women. Placenta 2018, 63, 45–52. [Google Scholar] [CrossRef]
- Decenti, E.C.; Salvatore, M.A.; Mancon, A.; Portella, G.; Rocca, A.; Vocale, C.; Donati, S.; Alberi, I.; Anelli, G.M.; Baltaro, F.; et al. A large series of molecular and serological specimens to evaluate mother-to-child SARS-CoV-2 transmission: A prospective study from the Italian Obstetric Surveillance System. Int. J. Infect. Dis. 2023, 126, 1–9. [Google Scholar] [CrossRef]
- Cinicola, B.; Conti, M.G.; Terrin, G.; Sgrulletti, M.; Elfeky, R.; Carsetti, R.; Salinas, A.F.; Mortari, E.P.; Brindisi, G.; De Curtis, M.; et al. The Protective Role of Maternal Immunization in Early Life. Front. Pediatr. 2021, 9, 638871. [Google Scholar] [CrossRef] [PubMed]
- Kugelman, N.; Nahshon, C.; Shaked-Mishan, P.; Cohen, N.; Sher, M.L.; Gruber, M.; Marom, I.; Zolotarevsky, A.; Lavie, O.; Damti, A.; et al. Maternal and Neonatal SARS-CoV-2 Immunoglobulin G Antibody Levels at Delivery After Receipt of the BNT162b2 Messenger RNA COVID-19 Vaccine During the Second Trimester of Pregnancy. JAMA Pediatr. 2022, 176, 290–295. [Google Scholar] [CrossRef] [PubMed]
- Rottenstreich, A.; Zarbiv, G.; Oiknine-Djian, E.; Vorontsov, O.; Zigron, R.; Kleinstern, G.; Wolf, D.G.; Porat, S. Timing of SARS-CoV-2 vaccination during the third trimester of pregnancy and transplacental antibody transfer: A prospective cohort study. Clin. Microbiol. Infect. 2022, 28, 419–425. [Google Scholar] [CrossRef]
- Faust, J.S.; Rasmussen, S.A.; Jamieson, D.J. Pregnancy should be a condition eligible for additional doses of COVID-19 messenger RNA vaccines. Am. J. Obstet. Gynecol. MFM 2022, 5, 100801. [Google Scholar] [CrossRef]
- Atyeo, C.; Shook, L.L.; Nziza, N.; Deriso, E.A.; Muir, C.; Baez, A.M.; Lima, R.S.; Demidkin, S.; Brigida, S.; De Guzman, R.M.; et al. COVID-19 booster dose induces robust antibody response in pregnant, lactating, and nonpregnant women. Am. J. Obstet. Gynecol. 2023, 228, 68.e1–68.e12. [Google Scholar] [CrossRef] [PubMed]
- Blakeway, H.; Amin-Chowdhury, Z.; Prasad, S.; Kalafat, E.; Ismail, M.; Abdallah, F.N.; Rezvani, A.; Amirthalingam, G.; Brown, K.; Le Doare, K.; et al. Evaluation of immunogenicity and reactogenicity of COVID-19 vaccines in pregnant women. Ultrasound Obstet. Gynecol. 2022, 60, 673–680. [Google Scholar] [CrossRef]
- Rendell, V.; Bath, N.M.; Brennan, T.V. Medawar’s Paradox and Immune Mechanisms of Fetomaternal Tolerance. OBM Transplant. 2020, 4, 104. [Google Scholar] [CrossRef]
- Germain, S.J.; Sacks, G.P.; Soorana, S.R.; Sargent, I.L.; Redman, C.W. Systemic Inflammatory Priming in Normal Pregnancy and Preeclampsia: The Role of Circulating Syncytiotrophoblast Microparticles. J. Immunol. 2007, 178, 5949–5956, Erratum in J. Immunol. 2007, 179, 1390. [Google Scholar] [CrossRef]
- Sahin, U.; Muik, A.; Derhovanessian, E.; Vogler, I.; Kranz, L.M.; Vormehr, M.; Baum, A.; Pascal, K.; Quandt, J.; Maurus, D.; et al. COVID-19 vaccine BNT162b1 elicits human antibody and TH1 T-cell responses. Nature 2020, 586, 594–599, Erratum in Nature 2021, 590, E17. [Google Scholar] [CrossRef]
- Foo, S.-S.; Cambou, M.C.; Mok, T.; Fajardo, V.M.; Jung, K.L.; Fuller, T.; Chen, W.; Kerin, T.; Mei, J.; Bhattacharya, D.; et al. The systemic inflammatory landscape of COVID-19 in pregnancy: Extensive serum proteomic profiling of mother-infant dyads with in utero SARS-CoV-2. Cell Rep. Med. 2021, 2, 100453. [Google Scholar] [CrossRef]
- Rubio, R.; Aguilar, R.; Bustamante, M.; Muñoz, E.; Vázquez-Santiago, M.; Santano, R.; Vidal, M.; Melero, N.R.; Parras, D.; Serra, P.; et al. Maternal and neonatal immune response to SARS-CoV-2, IgG transplacental transfer and cytokine profile. Front. Immunol. 2022, 13, 999136. [Google Scholar] [CrossRef] [PubMed]
- Collier, A.-R.Y.; McMahan, K.; Yu, J.; Tostanoski, L.H.; Aguayo, R.; Ansel, J.; Chandrashekar, A.; Patel, S.; Bondzie, E.A.; Sellers, D.; et al. Immunogenicity of COVID-19 mRNA Vaccines in Pregnant and Lactating Women. JAMA 2021, 325, 2370–2380. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Maternal Variables | Categories | Value n (%) |
|---|---|---|
| Maternal Age | Median age (years) | 34 (range: 20–48) |
| Ethnicity | Caucasian | 191 (83.0%) |
| Non-Caucasian | 39 (17.0%) | |
| Vaccination Status | Vaccinated | 127 (55.2%) |
| Unvaccinated | 103 (44.8%) | |
| Vaccine * | Astrazeneca | 2 (1.6%) |
| Astrazeneca + Pfizer | 2 (1.6%) | |
| Moderna | 6 (4.7%) | |
| Pfizer | 112 (88.2%) | |
| N.A. | 5 (3.9%) | |
| Vaccine Doses * | One | 9 (7.1%) |
| Two | 113 (89.0%) | |
| Three | 1 (0.8%) | |
| N.A. | 4 (3.1%) | |
| Vaccine Side Effects * | None | 23 (18.1%) |
| Pain at injection site | 18 (14.2%) | |
| Fever | 3 (2.3%) | |
| Headache | 2 (1.6%) | |
| N.A. | 81 (63.8%) | |
| Vaccination to Delivery Time Span * | <2 weeks | 12 (9.4%) |
| between 2 and 4 weeks | 18 (14.2%) | |
| >4 weeks | 87 (68.5%) | |
| N.A. | 10 (7.9%) |
| Maternal and Neonatal Variables | UNVACCINATED n = 103 | VACCINATED n = 127 | p-Value | |
|---|---|---|---|---|
| Maternal Age, years | 33.6 ± 5.5 | 34.4 ± 4.9 | ns | |
| Maternal Ethnicity, n- % | Caucasian | 72 (69.9) | 119 (93.7) | p < 0.001 |
| Not Caucasian | 31 (30.1) | 8 (6.3) | ||
| Maternal Pregestational BMI, kg/m2 | 23.5 ± 4.8 | 22.16 ± 3.4 | p = 0.05 | |
| Gestational Age at Delivery, weeks | 39.6 ± 1.1 | 39.6 ± 1.0 | ns | |
| Placental Weight (P), gr | 563.46 ± 91.78 | 535.10 ± 92.16 | p = 0.02 | |
| N/P Weight Ratio | 5.9 ± 1.0 | 6.41 ± 1.3 | p = 0.001 | |
| Neonatal Weight (N), gr | 3279.25 ± 415.07 | 3344.61 ± 388.31 | ns | |
| Neonatal Weight Centiles | 46.7 ± 28.8 | 47.6 ± 26.5 | ns | |
| Neonatal pH | 7.25 ± 0.09 | 7.26 ± 0.09 | ns | |
| Neonatal Apgar, 1 min | 9.16 ± 0.92 | 9.27 ± 0.82 | ns | |
| Neonatal Apgar, 5 min | 9.82 ± 0.72 | 9.93 ± 0.31 | ns | |
| Maternal Positive Anti-N | Maternal Positive Anti-S | Cord Positive Anti-N | Cord Positive Anti-S | Total | |
|---|---|---|---|---|---|
| Unvaccinated | 13 (15.48) | 5 (5.95) | 3 (3.57) | 3 (3.57) | 24 (28.57) |
| Vaccinated | 15 (13.04) | NA | 1 (0.87) | NA | 16 (13.91) |
| Total | 28 (14.07) | 5 (2.51) | 4 (2.01) | 3 (3.57) | 40 (20.10) |
| (a) | ||||
| UNVACCINATED | VACCINATED | p-Value | ||
| Maternal anti-S, % | Positive | 0 (0%) | 89 (96.7%) | p < 0.001 |
| Negative | 49 (100%) | 3 (3.3%) | ||
| Neonatal anti-S, % | Positive | 0 (0%) | 84 (96.6%) | p < 0.001 |
| Negative | 56 (100%) | 3 (3.4%) | ||
| (b) | ||||
| UNVACCINATED | VACCINATED | p-Value | ||
| Maternal anti-S, % | Positive | 0 (0.0%) | 78 (96.3%) | p < 0.001 |
| Negative | 45 (100.0%) | 3 (3.7%) | ||
| Neonatal anti-S, % | Positive | 0 (0.0%) | 79 (97.5%) | |
| Negative | 45 (100.0%) | 2 (2.5%) | ||
| UNVACCINATED | VACCINATED | ||
|---|---|---|---|
| Maternal Interferon γ | indeterminate | 6 (50%) | 9 (39.1%) |
| non-reactive | 6 (50%) | 10 (43.5%) | |
| reactive | 0 | 4 (17.4%) | |
| Neonatal Interferon γ | indeterminate | 6 (100%) | 15 (93.7%) |
| non-reactive | 0 | 1 (6.3%) | |
| reactive | 0 | 0 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lubrano, C.; Mancon, A.; Anelli, G.M.; Gagliardi, G.; Corneo, R.; Bianchi, M.; Coco, C.; Dal Molin, G.; Vignali, M.; Schirripa, I.; et al. Immune Response and Transplacental Antibody Transfer in Pregnant Women after COVID-19 Vaccination. J. Pers. Med. 2023, 13, 689. https://doi.org/10.3390/jpm13040689
Lubrano C, Mancon A, Anelli GM, Gagliardi G, Corneo R, Bianchi M, Coco C, Dal Molin G, Vignali M, Schirripa I, et al. Immune Response and Transplacental Antibody Transfer in Pregnant Women after COVID-19 Vaccination. Journal of Personalized Medicine. 2023; 13(4):689. https://doi.org/10.3390/jpm13040689
Chicago/Turabian StyleLubrano, Chiara, Alessandro Mancon, Gaia Maria Anelli, Gloria Gagliardi, Roberta Corneo, Micol Bianchi, Chiara Coco, Giulia Dal Molin, Michele Vignali, Irene Schirripa, and et al. 2023. "Immune Response and Transplacental Antibody Transfer in Pregnant Women after COVID-19 Vaccination" Journal of Personalized Medicine 13, no. 4: 689. https://doi.org/10.3390/jpm13040689