
Soluble Urokinase Plasminogen Activator Receptor (suPAR) in Autoimmune Rheumatic and Non Rheumatic Diseases
 ,
,  , and
, and 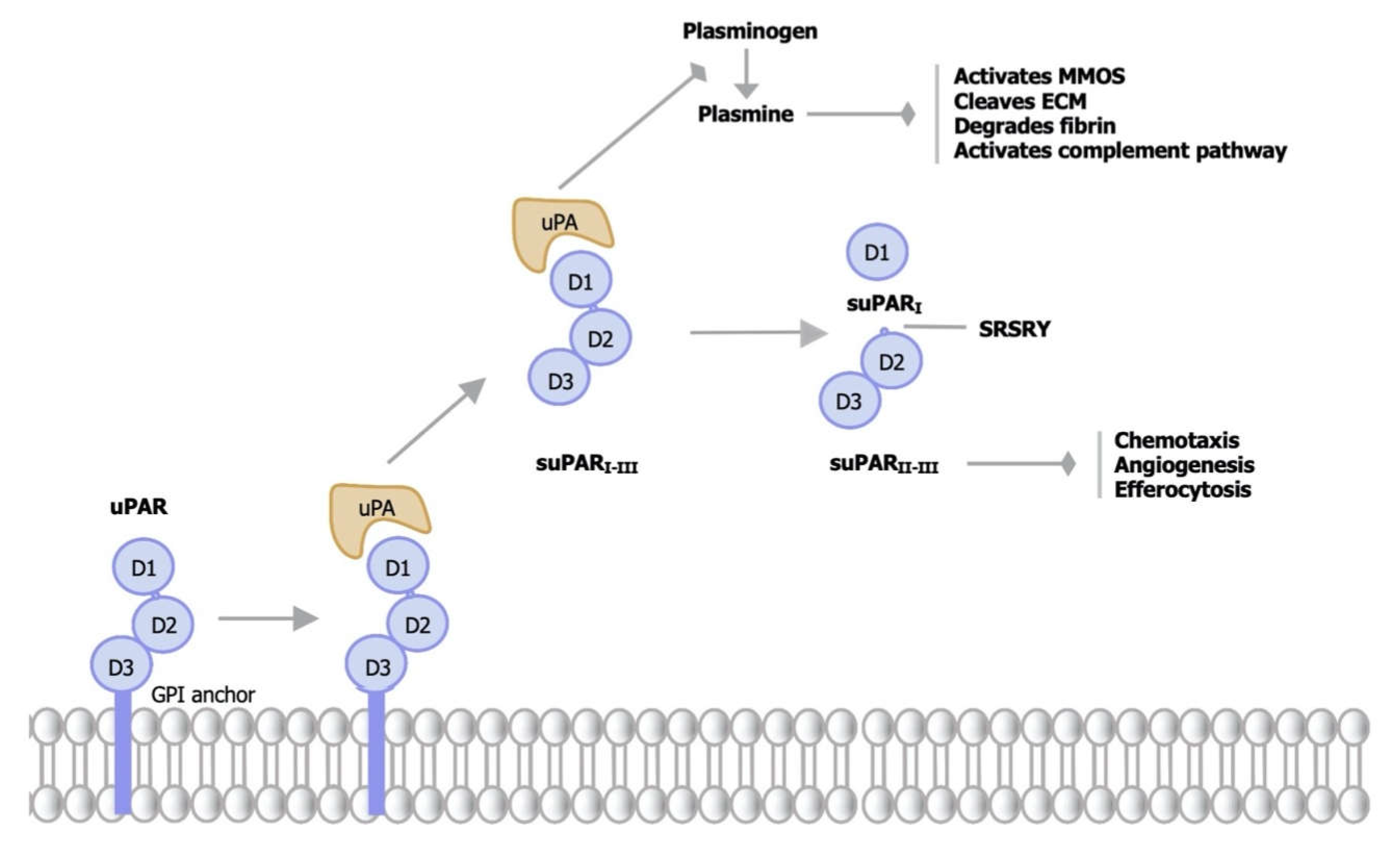{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Methods
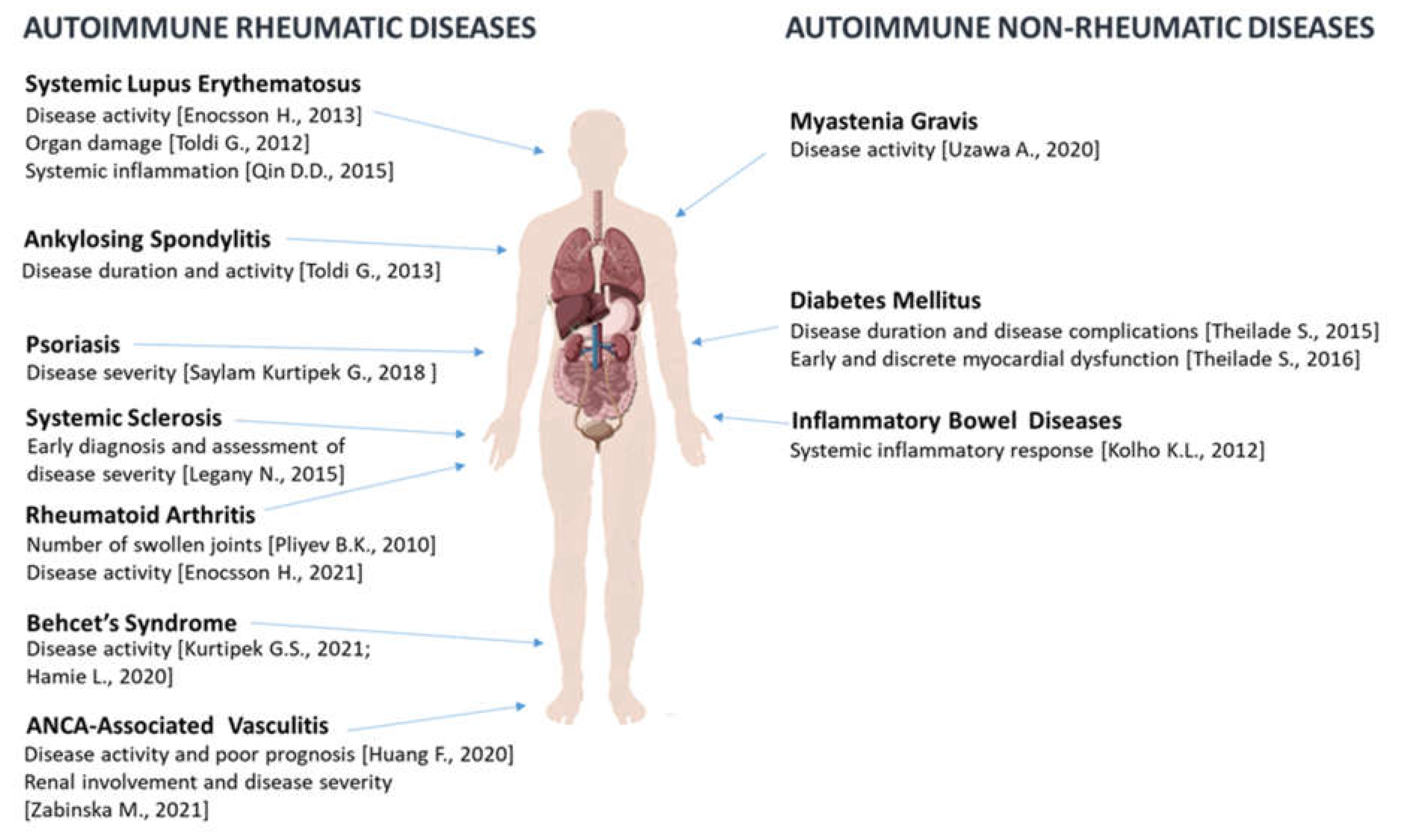
3. suPAR in Autoimmune Rheumatic Diseases
3.1. Rheumatoid Arthritis (RA)
3.2. Systemic Lupus Erythematosus (SLE)
3.3. Systemic Sclerosis (SSc)
3.4. Behcet’s Syndrome
3.5. Psoriasis
3.6. Ankylosing Spondylitis (AS)
3.7. ANCA-Associated Vasculitis (AAV)
3.8. Key Messages
4. suPAR in Autoimmune Non-Rheumatic Diseases
4.1. Type 1 Diabetes Mellitus (T1DM)
4.2. Inflammatory Bowel Diseases (IBD)
4.3. Myasthenia Gravis (MG)
4.4. Key Messages
5. Conclusions and Perspective
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Thuno, M.; Macho, B.; Eugen-Olsen, J. suPAR: The molecular crystal ball. Dis. Markers 2009, 27, 157–172. [Google Scholar] [CrossRef]
- Rasmussen, L.J.H.; Petersen, J.E.V.; Eugen-Olsen, J. Soluble Urokinase Plasminogen Activator Receptor (suPAR) as a Biomarker of Systemic Chronic Inflammation. Front. Immunol. 2021, 12, 780641. [Google Scholar] [CrossRef]
- Danø, K.B.N.; Brünner, N.; Ellis, V.; Ploug, M.; Pyke, C. The urokinase receptor. Protein structure and role in plasminogen activation and cancer invasion. Fibrinolysis 1994, 8, 189–203. [Google Scholar] [CrossRef]
- Behrendt N, S.R. The urokinase receptor. Fibrinolysis Proteol. 1998, 12, 191–204. [Google Scholar] [CrossRef]
- Smith, H.W.; Marshall, C.J. Regulation of cell signalling by uPAR. Nat. Rev. Mol. Cell. Biol. 2010, 11, 23–36. [Google Scholar] [CrossRef]
- Donadello, K.; Scolletta, S.; Covajes, C.; Vincent, J.L. suPAR as a prognostic biomarker in sepsis. BMC Med. 2012, 10, 2. [Google Scholar] [CrossRef]
- Choi, H.M.; Lee, Y.A.; Yang, H.I.; Yoo, M.C.; Kim, K.S. Increased levels of thymosin beta4 in synovial fluid of patients with rheumatoid arthritis: Association of thymosin beta4 with other factors that are involved in inflammation and bone erosion in joints. Int. J. Rheum. Dis. 2011, 14, 320–324. [Google Scholar] [CrossRef] [PubMed]
- Koshelnick, Y.; Ehart, M.; Stockinger, H.; Binder, B.R. Mechanisms of signaling through urokinase receptor and the cellular response. Thromb. Haemost. 1999, 82, 305–311. [Google Scholar] [CrossRef] [PubMed]
- Plesner, T.; Behrendt, N.; Ploug, M. Structure, function and expression on blood and bone marrow cells of the urokinase-type plasminogen activator receptor, uPAR. Stem Cells 1997, 15, 398–408. [Google Scholar] [CrossRef]
- Plesner, T.; Ralfkiaer, E.; Wittrup, M.; Johnsen, H.; Pyke, C.; Pedersen, T.L.; Hansen, N.E.; Dano, K. Expression of the receptor for urokinase-type plasminogen activator in normal and neoplastic blood cells and hematopoietic tissue. Am. J. Clin. Pathol. 1994, 102, 835–841. [Google Scholar] [CrossRef]
- Del Rosso, M.; Margheri, F.; Serrati, S.; Chilla, A.; Laurenzana, A.; Fibbi, G. The urokinase receptor system, a key regulator at the intersection between inflammation, immunity, and coagulation. Curr. Pharm. Des. 2011, 17, 1924–1943. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.S.; Lee, Y.A.; Choi, H.M.; Yoo, M.C.; Yang, H.I. Implication of MMP-9 and urokinase plasminogen activator (uPA) in the activation of pro-matrix metalloproteinase (MMP)-13. Rheumatol. Int. 2012, 32, 3069–3075. [Google Scholar] [CrossRef]
- Pavon, M.A.; Arroyo-Solera, I.; Cespedes, M.V.; Casanova, I.; Leon, X.; Mangues, R. uPA/uPAR and SERPINE1 in head and neck cancer: Role in tumor resistance, metastasis, prognosis and therapy. Oncotarget 2016, 7, 57351–57366. [Google Scholar] [CrossRef]
- Stephens, R.W.; Pedersen, A.N.; Nielsen, H.J.; Hamers, M.J.; Hoyer-Hansen, G.; Ronne, E.; Dybkjaer, E.; Dano, K.; Brunner, N. ELISA determination of soluble urokinase receptor in blood from healthy donors and cancer patients. Clin. Chem. 1997, 43, 1868–1876. [Google Scholar] [CrossRef]
- Ronne, E.; Pappot, H.; Grondahl-Hansen, J.; Hoyer-Hansen, G.; Plesner, T.; Hansen, N.E.; Dano, K. The receptor for urokinase plasminogen activator is present in plasma from healthy donors and elevated in patients with paroxysmal nocturnal haemoglobinuria. Br. J. Haematol. 1995, 89, 576–581. [Google Scholar] [CrossRef]
- Haastrup, E.; Grau, K.; Eugen-Olsen, J.; Thorball, C.; Kessing, L.V.; Ullum, H. Soluble urokinase plasminogen activator receptor as a marker for use of antidepressants. PLoS ONE 2014, 9, e110555. [Google Scholar] [CrossRef]
- Eugen-Olsen, J.; Andersen, O.; Linneberg, A.; Ladelund, S.; Hansen, T.W.; Langkilde, A.; Petersen, J.; Pielak, T.; Moller, L.N.; Jeppesen, J.; et al. Circulating soluble urokinase plasminogen activator receptor predicts cancer, cardiovascular disease, diabetes and mortality in the general population. J. Intern. Med. 2010, 268, 296–308. [Google Scholar] [CrossRef]
- Cerinic, M.M.; Generini, S.; Partsch, G.; Pignone, A.; Dini, G.; Konttinen, Y.T.; Del Rosso, M. Synoviocytes from osteoarthritis and rheumatoid arthritis produce plasminogen activators and plasminogen activator inhibitor-1 and display u-PA receptors on their surface. Life Sci. 1998, 63, 441–453. [Google Scholar] [CrossRef] [PubMed]
- Riisbro, R.; Christensen, I.J.; Hogdall, C.; Brunner, N.; Hogdall, E. Soluble urokinase plasminogen activator receptor measurements: Influence of sample handling. Int. J. Biol. Markers 2001, 16, 233–239. [Google Scholar] [CrossRef] [PubMed]
- Pillinger, M.H.; Abramson, S.B. The neutrophil in rheumatoid arthritis. Rheum. Dis. Clin. N. Am. 1995, 21, 691–714. [Google Scholar] [CrossRef]
- Edwards, S.W.; Hallett, M.B. Seeing the wood for the trees: The forgotten role of neutrophils in rheumatoid arthritis. Immunol. Today 1997, 18, 320–324. [Google Scholar] [CrossRef]
- Pliyev, B.K.; Menshikov, M.Y. Release of the soluble urokinase-type plasminogen activator receptor (suPAR) by activated neutrophils in rheumatoid arthritis. Inflammation 2010, 33, 1–9. [Google Scholar] [CrossRef]
- Enocsson, H.; Lukic, T.; Ziegelasch, M.; Kastbom, A. Serum levels of the soluble urokinase plasminogen activator receptor (suPAR) correlates with disease activity in early rheumatoid arthritis and reflects joint damage over time. Transl. Res. 2021, 232, 142–149. [Google Scholar] [CrossRef]
- Toldi, G.; Beko, G.; Kadar, G.; Macsai, E.; Kovacs, L.; Vasarhelyi, B.; Balog, A. Soluble urokinase plasminogen activator receptor (suPAR) in the assessment of inflammatory activity of rheumatoid arthritis patients in remission. Clin. Chem. Lab. Med. 2013, 51, 327–332. [Google Scholar] [CrossRef]
- Slot, O.; Brunner, N.; Locht, H.; Oxholm, P.; Stephens, R.W. Soluble urokinase plasminogen activator receptor in plasma of patients with inflammatory rheumatic disorders: Increased concentrations in rheumatoid arthritis. Ann. Rheum. Dis. 1999, 58, 488–492. [Google Scholar] [CrossRef] [PubMed]
- Ugarte-Gil, M.F.; Gonzalez, L.A.; Alarcon, G.S. Lupus: The new epidemic. Lupus 2019, 28, 1031–1050. [Google Scholar] [CrossRef]
- Burcsar, S.; Toldi, G.; Kovacs, L.; Szalay, B.; Vasarhelyi, B.; Balog, A. Urine soluble urokinase plasminogen activator receptor as a potential biomarker of lupus nephritis activity. Biomarkers 2021, 26, 443–449. [Google Scholar] [CrossRef] [PubMed]
- Enocsson, H.; Wettero, J.; Skogh, T.; Sjowall, C. Soluble urokinase plasminogen activator receptor levels reflect organ damage in systemic lupus erythematosus. Transl. Res. 2013, 162, 287–296. [Google Scholar] [CrossRef] [PubMed]
- Toldi, G.; Szalay, B.; Beko, G.; Bocskai, M.; Deak, M.; Kovacs, L.; Vasarhelyi, B.; Balog, A. Plasma soluble urokinase plasminogen activator receptor (suPAR) levels in systemic lupus erythematosus. Biomarkers 2012, 17, 758–763. [Google Scholar] [CrossRef]
- Enocsson, H.; Wirestam, L.; Dahle, C.; Padyukov, L.; Jonsen, A.; Urowitz, M.B.; Gladman, D.D.; Romero-Diaz, J.; Bae, S.C.; Fortin, P.R.; et al. Soluble urokinase plasminogen activator receptor (suPAR) levels predict damage accrual in patients with recent-onset systemic lupus erythematosus. J. Autoimmun. 2020, 106, 102340. [Google Scholar] [CrossRef] [PubMed]
- Qin, D.D.; Song, D.; Huang, J.; Yu, F.; Zhao, M.H. Plasma-soluble urokinase-type plasminogen activator receptor levels are associated with clinical and pathological activities in lupus nephritis: A large cohort study from China. Lupus 2015, 24, 546–557. [Google Scholar] [CrossRef]
- Soltysiak, J.; Zachwieja, J.; Benedyk, A.; Lewandowska-Stachowiak, M.; Nowicki, M.; Ostalska-Nowicka, D. Circulating suPAR as a biomarker of disease severity in children with proteinuric glomerulonephritis. Minerva Pediatr. 2019, 71, 4–11. [Google Scholar] [CrossRef] [PubMed]
- Manetti, M. Emerging biomarkers in systemic sclerosis. Curr. Opin. Rheumatol. 2016, 28, 606–612. [Google Scholar] [CrossRef]
- Muangchan, C.; Harding, S.; Khimdas, S.; Bonner, A.; Canadian Scleroderma Research Group; Baron, M.; Pope, J. Association of C-reactive protein with high disease activity in systemic sclerosis: Results from the Canadian Scleroderma Research Group. Arthritis Care Res. 2012, 64, 1405–1414. [Google Scholar] [CrossRef]
- Legany, N.; Toldi, G.; Distler, J.H.; Beyer, C.; Szalay, B.; Kovacs, L.; Vasarhelyi, B.; Balog, A. Increased plasma soluble urokinase plasminogen activator receptor levels in systemic sclerosis: Possible association with microvascular abnormalities and extent of fibrosis. Clin. Chem. Lab. Med. 2015, 53, 1799–1805. [Google Scholar] [CrossRef] [PubMed]
- Butt, S.; Jeppesen, J.L.; Iversen, L.V.; Fenger, M.; Eugen-Olsen, J.; Andersson, C.; Jacobsen, S. Association of soluble urokinase plasminogen activator receptor levels with fibrotic and vascular manifestations in systemic sclerosis. PLoS ONE 2021, 16, e0247256. [Google Scholar] [CrossRef]
- Karadag, O.; Bolek, E.C. Management of Behcet’s syndrome. Rheumatology 2020, 59, iii108–iii117. [Google Scholar] [CrossRef] [PubMed]
- Saylam Kurtipek, G.; Kesli, R.; Tuncez Akyurek, F.; Akyurek, F.; Ataseven, A.; Terzi, Y. Plasma-soluble urokinase plasminogen activator receptor (suPAR) levels in Behcet’s disease and correlation with disease activity. Int. J. Rheum. Dis. 2018, 21, 866–870. [Google Scholar] [CrossRef]
- Parisi, R.; Iskandar, I.Y.K.; Kontopantelis, E.; Augustin, M.; Griffiths, C.E.M.; Ashcroft, D.M.; Global Psoriasis, A. National, regional, and worldwide epidemiology of psoriasis: Systematic analysis and modelling study. BMJ 2020, 369, m1590. [Google Scholar] [CrossRef]
- Kurtipek, G.S.; Kesli, R.; Tuncez Akyurek, F.; Akyuret, F.; Terzi, Y. Plasma-soluble urokinase plasminogen activator receptor (suPAR) levels in psoriasis patients and correlation with disease severity. Acta Dermatovenerol. Alp. Pannonica Adriat. 2015, 24, 73–75. [Google Scholar] [CrossRef]
- Hamie, L.; Eid, E.; Abbas, O.; Safi, R.; Nammour, T.; Tamim, H.; Makki, M.; Stephan, C.; Hasbani, D.; Wehbe, H.; et al. SuPAR, a potential inflammatory mediator in psoriasis pathogenesis. Clin. Exp. Pharmacol. Physiol. 2020, 47, 1705–1712. [Google Scholar] [CrossRef]
- Braun, J.; Sieper, J. Ankylosing spondylitis. Lancet 2007, 369, 1379–1390. [Google Scholar] [CrossRef] [PubMed]
- Toldi, G.; Szalay, B.; Beko, G.; Kovacs, L.; Vasarhelyi, B.; Balog, A. Plasma soluble urokinase plasminogen activator receptor (suPAR) levels in ankylosing spondylitis. Jt. Bone Spine 2013, 80, 96–98. [Google Scholar] [CrossRef] [PubMed]
- Zabinska, M.; Koscielska-Kasprzak, K.; Krajewska, J.; Bartoszek, D.; Augustyniak-Bartosik, H.; Krajewska, M. Immune Cells Profiling in ANCA-Associated Vasculitis Patients-Relation to Disease Activity. Cells 2021, 10, 1773. [Google Scholar] [CrossRef] [PubMed]
- Huang, F.; Li, Y.; Xu, R.; Cheng, A.; Lv, Y.; Liu, Q. The Plasma Soluble Urokinase Plasminogen Activator Receptor Is Related to Disease Activity of Patients with ANCA-Associated Vasculitis. Mediat. Inflamm. 2020, 2020, 7850179. [Google Scholar] [CrossRef] [PubMed]
- Chawla, A.; Chawla, R.; Jaggi, S. Microvasular and macrovascular complications in diabetes mellitus: Distinct or continuum? Indian J. Endocrinol. Metab. 2016, 20, 546–551. [Google Scholar] [CrossRef]
- Theilade, S.; Lyngbaek, S.; Hansen, T.W.; Eugen-Olsen, J.; Fenger, M.; Rossing, P.; Jeppesen, J.L. Soluble urokinase plasminogen activator receptor levels are elevated and associated with complications in patients with type 1 diabetes. J. Intern. Med. 2015, 277, 362–371. [Google Scholar] [CrossRef]
- Theilade, S.; Rossing, P.; Eugen-Olsen, J.; Jensen, J.S.; Jensen, M.T. suPAR level is associated with myocardial impairment assessed with advanced echocardiography in patients with type 1 diabetes with normal ejection fraction and without known heart disease or end-stage renal disease. Eur. J. Endocrinol. 2016, 174, 745–753. [Google Scholar] [CrossRef]
- Fukunaga, S.; Kuwaki, K.; Mitsuyama, K.; Takedatsu, H.; Yoshioka, S.; Yamasaki, H.; Yamauchi, R.; Mori, A.; Kakuma, T.; Tsuruta, O.; et al. Detection of calprotectin in inflammatory bowel disease: Fecal and serum levels and immunohistochemical localization. Int. J. Mol. Med. 2018, 41, 107–118. [Google Scholar] [CrossRef]
- Canani, R.B.; Terrin, G.; Rapacciuolo, L.; Miele, E.; Siani, M.C.; Puzone, C.; Cosenza, L.; Staiano, A.; Troncone, R. Faecal calprotectin as reliable non-invasive marker to assess the severity of mucosal inflammation in children with inflammatory bowel disease. Dig. Liver Dis. 2008, 40, 547–553. [Google Scholar] [CrossRef]
- Lasson, A.; Stotzer, P.O.; Ohman, L.; Isaksson, S.; Sapnara, M.; Strid, H. The intra-individual variability of faecal calprotectin: A prospective study in patients with active ulcerative colitis. J. Crohns Colitis 2015, 9, 26–32. [Google Scholar] [CrossRef]
- Turner, D.; Mack, D.R.; Hyams, J.; LeLeiko, N.; Otley, A.; Markowitz, J.; Kasirer, Y.; Muise, A.; Seow, C.H.; Silverberg, M.S.; et al. C-reactive protein (CRP), erythrocyte sedimentation rate (ESR) or both? A systematic evaluation in pediatric ulcerative colitis. J. Crohns Colitis 2011, 5, 423–429. [Google Scholar] [CrossRef]
- Kolho, K.L.; Valtonen, E.; Rintamaki, H.; Savilahti, E. Soluble urokinase plasminogen activator receptor suPAR as a marker for inflammation in pediatric inflammatory bowel disease. Scand. J. Gastroenterol. 2012, 47, 951–955. [Google Scholar] [CrossRef] [PubMed]
- Meriggioli, M.N.; Sanders, D.B. Autoimmune myasthenia gravis: Emerging clinical and biological heterogeneity. Lancet Neurol. 2009, 8, 475–490. [Google Scholar] [CrossRef] [PubMed]
- Uzawa, A.; Kojima, Y.; Ozawa, Y.; Yasuda, M.; Onishi, Y.; Akamine, H.; Kawaguchi, N.; Himuro, K.; Kuwabara, S. Serum level of soluble urokinase plasminogen activator receptor (suPAR) as a disease severity marker of myasthenia gravis: A pilot study. Clin. Exp. Immunol. 2020, 202, 321–324. [Google Scholar] [CrossRef] [PubMed]
- Savva, A.; Raftogiannis, M.; Baziaka, F.; Routsi, C.; Antonopoulou, A.; Koutoukas, P.; Tsaganos, T.; Kotanidou, A.; Apostolidou, E.; Giamarellos-Bourboulis, E.J.; et al. Soluble urokinase plasminogen activator receptor (suPAR) for assessment of disease severity in ventilator-associated pneumonia and sepsis. J. Infect. 2011, 63, 344–350. [Google Scholar] [CrossRef]
- Nilsonne, G.; Lekander, M.; Akerstedt, T.; Axelsson, J.; Ingre, M. Diurnal Variation of Circulating Interleukin-6 in Humans: A Meta-Analysis. PLoS ONE 2016, 11, e0165799. [Google Scholar] [CrossRef]
- Desmedt, S.; Desmedt, V.; Delanghe, J.R.; Speeckaert, R.; Speeckaert, M.M. The intriguing role of soluble urokinase receptor in inflammatory diseases. Crit. Rev. Clin. Lab. Sci. 2017, 54, 117–133. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Manfredi, M.; Van Hoovels, L.; Benucci, M.; De Luca, R.; Coccia, C.; Bernardini, P.; Russo, E.; Amedei, A.; Guiducci, S.; Grossi, V.; et al. Soluble Urokinase Plasminogen Activator Receptor (suPAR) in Autoimmune Rheumatic and Non Rheumatic Diseases. J. Pers. Med. 2023, 13, 688. https://doi.org/10.3390/jpm13040688
Manfredi M, Van Hoovels L, Benucci M, De Luca R, Coccia C, Bernardini P, Russo E, Amedei A, Guiducci S, Grossi V, et al. Soluble Urokinase Plasminogen Activator Receptor (suPAR) in Autoimmune Rheumatic and Non Rheumatic Diseases. Journal of Personalized Medicine. 2023; 13(4):688. https://doi.org/10.3390/jpm13040688
Chicago/Turabian StyleManfredi, Mariangela, Lieve Van Hoovels, Maurizio Benucci, Riccardo De Luca, Carmela Coccia, Pamela Bernardini, Edda Russo, Amedeo Amedei, Serena Guiducci, Valentina Grossi, and et al. 2023. "Soluble Urokinase Plasminogen Activator Receptor (suPAR) in Autoimmune Rheumatic and Non Rheumatic Diseases" Journal of Personalized Medicine 13, no. 4: 688. https://doi.org/10.3390/jpm13040688