
Mediation Effects of Social Cognition on the Relationship between Neurocognition and Social Functioning in Major Depressive Disorder and Schizophrenia Spectrum Disorders
 , , , and
, , , and
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Participants
2.2. Measures
2.3. Data Analysis
3. Results
3.1. Demographics and Clinical Characteristics
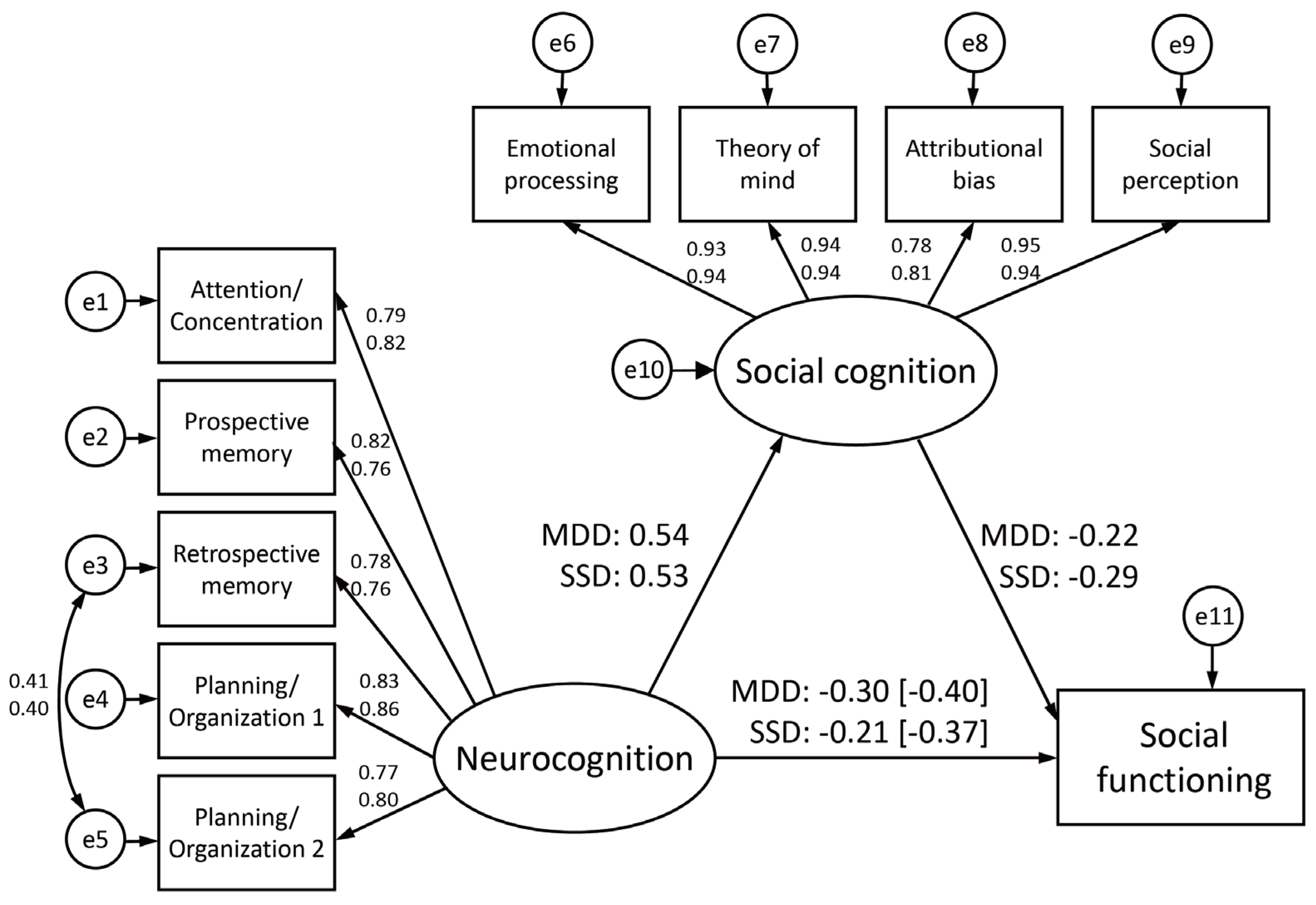
3.2. Mediation Effects of Social Cognition
3.3. Invariances in the Mediation Models across Groups
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Walker, E.R.; McGee, R.E.; Druss, B.G. Mortality in Mental Disorders and Global Disease Burden Implications: A Systematic Review and Meta-Analysis. JAMA Psychiatry 2015, 72, 334–341. [Google Scholar] [CrossRef] [PubMed]
- Whiteford, H.A.; Degenhardt, L.; Rehm, J.; Baxter, A.J.; Ferrari, A.J.; Erskine, H.E.; Charlson, F.J.; Norman, R.E.; Flaxman, A.D.; Johns, N.; et al. Global Burden of Disease Attributable to Mental and Substance Use Disorders: Findings from the Global Burden of Disease Study 2010. Lancet 2013, 382, 1575–1586. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization; World Bank. World Report on Disability 2011; World Health Organization: Geneva, Switzerland, 2011; pp. 55–92. [Google Scholar]
- GBD 2016 Disease and Injury Incidence and Prevalence Collaborators. Global, Regional, and National Incidence, Prevalence, and Years Lived with Disability for 328 Diseases and Injuries for 195 Countries, 1990-2016: A Systematic Analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1211–1259. [Google Scholar] [CrossRef] [PubMed]
- Jääskeläinen, E.; Juola, P.; Hirvonen, N.; McGrath, J.J.; Saha, S.; Isohanni, M.; Veijola, J.; Miettunen, J. A Systematic Review and Meta-Analysis of Recovery in Schizophrenia. Schizophr. Bull. 2013, 39, 1296–1306. [Google Scholar] [CrossRef] [PubMed]
- Green, M.F.; Kern, R.S.; Heaton, R.K. Longitudinal Studies of Cognition and Functional Outcome in Schizophrenia: Implications for MATRICS. Schizophr. Res. 2004, 72, 41–51. [Google Scholar] [CrossRef]
- Cowman, M.; Holleran, L.; Lonergan, E.; O’Connor, K.; Birchwood, M.; Donohoe, G. Cognitive Predictors of Social and Occupational Functioning in Early Psychosis: A Systematic Review and Meta-Analysis of Cross-Sectional and Longitudinal Data. Schizophr. Bull. 2021, 47, 1243–1253. [Google Scholar] [CrossRef]
- Gebreegziabhere, Y.; Habatmu, K.; Mihretu, A.; Cella, M.; Alem, A. Cognitive Impairment in People with Schizophrenia: An Umbrella Review. Eur. Arch. Psychiatry Clin. Neurosci. 2022, 272, 1139–1155. [Google Scholar] [CrossRef]
- Khalil, M.; Hollander, P.; Raucher-Chéné, D.; Lepage, M.; Lavigne, K.M. Structural Brain Correlates of Cognitive Function in Schizophrenia: A Meta-Analysis. Neurosci. Biobehav. Rev. 2022, 132, 37–49. [Google Scholar] [CrossRef]
- Nemoto, T.; Kashima, H.; Mizuno, M. Contribution of Divergent Thinking to Community Functioning in Schizophrenia. Prog. Neuropsychopharmacol. Biol. Psychiatry 2007, 31, 517–524. [Google Scholar] [CrossRef]
- Nemoto, T.; Takeshi, K.; Niimura, H.; Tobe, M.; Ito, R.; Kojima, A.; Saito, H.; Funatogawa, T.; Yamaguchi, T.; Katagiri, N.; et al. Feasibility and Acceptability of Cognitive Rehabilitation during the Acute Phase of Schizophrenia. Early Interv. Psychiatry 2021, 15, 457–462. [Google Scholar] [CrossRef]
- Schmidt, S.J.; Mueller, D.R.; Roder, V. Social Cognition as a Mediator Variable between Neurocognition and Functional Outcome in Schizophrenia: Empirical Review and New Results by Structural Equation Modeling. Schizophr. Bull. 2011, 37 (Suppl. S2), S41–S54. [Google Scholar] [CrossRef] [PubMed]
- Kharawala, S.; Hastedt, C.; Podhorna, J.; Shukla, H.; Kappelhoff, B.; Harvey, P.D. The Relationship between Cognition and Functioning in Schizophrenia: A Semi-Systematic Review. Schizophr. Res. Cogn. 2022, 27, 100217. [Google Scholar] [CrossRef] [PubMed]
- Green, M.F.; Horan, W.P.; Lee, J. Nonsocial and Social Cognition in Schizophrenia: Current Evidence and Future Directions. World Psychiatry 2019, 18, 146–161. [Google Scholar] [CrossRef] [PubMed]
- Green, M.F.; Penn, D.L.; Bentall, R.; Carpenter, W.T.; Gaebel, W.; Gur, R.C.; Kring, A.M.; Park, S.; Silverstein, S.M.; Heinssen, R. Social Cognition in Schizophrenia: An NIMH Workshop on Definitions, Assessment, and Research Opportunities. Schizophr. Bull. 2008, 34, 1211–1220. [Google Scholar] [CrossRef]
- Pinkham, A.E.; Penn, D.L.; Green, M.F.; Buck, B.; Healey, K.; Harvey, P.D. The Social Cognition Psychometric Evaluation Study: Results of the Expert Survey and RAND Panel. Schizophr. Bull. 2014, 40, 813–823. [Google Scholar] [CrossRef]
- Pinkham, A.E.; Harvey, P.D.; Penn, D.L. Social Cognition Psychometric Evaluation: Results of the Final Validation Study. Schizophr. Bull. 2018, 44, 737–748. [Google Scholar] [CrossRef]
- Okano, H.; Kubota, R.; Okubo, R.; Hashimoto, N.; Ikezawa, S.; Toyomaki, A.; Miyazaki, A.; Sasaki, Y.; Yamada, Y.; Nemoto, T.; et al. Evaluation of Social Cognition Measures for Japanese Patients with Schizophrenia Using an Expert Panel and Modified Delphi Method. J. Pers. Med. 2021, 11, 275. [Google Scholar] [CrossRef]
- Lim, K.; Lee, S.-A.; Pinkham, A.E.; Lam, M.; Lee, J. Evaluation of Social Cognitive Measures in an Asian Schizophrenia Sample. Schizophr. Res. Cogn. 2020, 20, 100169. [Google Scholar] [CrossRef]
- Kubota, R.; Okubo, R.; Akiyama, H.; Okano, H.; Ikezawa, S.; Miyazaki, A.; Toyomaki, A.; Sasaki, Y.; Yamada, Y.; Uchino, T.; et al. Study Protocol: The Evaluation Study for Social Cognition Measures in Japan (ESCoM). J. Pers. Med. 2021, 11, 667. [Google Scholar] [CrossRef]
- Pelletier-Baldelli, A.; Holt, D.J. Are Negative Symptoms Merely the “Real World” Consequences of Deficits in Social Cognition? Schizophr. Bull. 2020, 46, 236–241. [Google Scholar] [CrossRef]
- Thibaudeau, E.; Rae, J.; Raucher-Chéné, D.; Bougeard, A.; Lepage, M. Disentangling the Relationships Between the Clinical Symptoms of Schizophrenia Spectrum Disorders and Theory of Mind: A Meta-Analysis. Schizophr. Bull. 2023, 49, 255–274. [Google Scholar] [CrossRef] [PubMed]
- Achim, A.M.; Sutliff, S.; Samson, C.; Montreuil, T.C.; Lecomte, T. Attribution Bias and Social Anxiety in Schizophrenia. Schizophr. Res. Cogn. 2016, 4, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Horan, W.P.; Green, M.F. Treatment of Social Cognition in Schizophrenia: Current Status and Future Directions. Schizophr. Res. 2019, 203, 3–11. [Google Scholar] [CrossRef] [PubMed]
- Nahum, M.; Lee, H.; Fisher, M.; Green, M.F.; Hooker, C.I.; Ventura, J.; Jordan, J.T.; Rose, A.; Kim, S.-J.; Haut, K.M.; et al. Online Social Cognition Training in Schizophrenia: A Double-Blind, Randomized, Controlled Multi-Site Clinical Trial. Schizophr. Bull. 2021, 47, 108–117. [Google Scholar] [CrossRef] [PubMed]
- Halverson, T.F.; Orleans-Pobee, M.; Merritt, C.; Sheeran, P.; Fett, A.-K.; Penn, D.L. Pathways to Functional Outcomes in Schizophrenia Spectrum Disorders: Meta-Analysis of Social Cognitive and Neurocognitive Predictors. Neurosci. Biobehav. Rev. 2019, 105, 212–219. [Google Scholar] [CrossRef]
- Mucci, A.; Galderisi, S.; Gibertoni, D.; Rossi, A.; Rocca, P.; Bertolino, A.; Aguglia, E.; Amore, M.; Bellomo, A.; Biondi, M.; et al. Factors Associated with Real-Life Functioning in Persons With Schizophrenia in a 4-Year Follow-up Study of the Italian Network for Research on Psychoses. JAMA Psychiatry 2021, 78, 550–559. [Google Scholar] [CrossRef]
- Nemoto, T.; Uchino, T.; Aikawa, S.; Matsuo, S.; Mamiya, N.; Shibasaki, Y.; Wada, Y.; Yamaguchi, T.; Katagiri, N.; Tsujino, N.; et al. Impact of Changes in Social Anxiety on Social Functioning and Quality of Life in Outpatients with Schizophrenia: A Naturalistic Longitudinal Study. J. Psychiatr. Res. 2020, 131, 15–21. [Google Scholar] [CrossRef]
- Szmulewicz, A.G.; Valerio, M.P.; Smith, J.M.; Samamé, C.; Martino, D.J.; Strejilevich, S.A. Neuropsychological Profiles of Major Depressive Disorder and Bipolar Disorder during Euthymia. A Systematic Literature Review of Comparative Studies. Psychiatry Res. 2017, 248, 127–133. [Google Scholar] [CrossRef]
- Rock, P.L.; Roiser, J.P.; Riedel, W.J.; Blackwell, A.D. Cognitive Impairment in Depression: A Systematic Review and Meta-Analysis. Psychol. Med. 2014, 44, 2029–2040. [Google Scholar] [CrossRef] [PubMed]
- Knight, M.J.; Baune, B.T. Cognitive Dysfunction in Major Depressive Disorder. Curr. Opin. Psychiatry 2018, 31, 26–31. [Google Scholar] [CrossRef]
- Semkovska, M.; Quinlivan, L.; O’Grady, T.; Johnson, R.; Collins, A.; O’Connor, J.; Knittle, H.; Ahern, E.; Gload, T. Cognitive Function Following a Major Depressive Episode: A Systematic Review and Meta-Analysis. Lancet Psychiatry 2019, 6, 851–861. [Google Scholar] [CrossRef] [PubMed]
- Varghese, S.; Frey, B.N.; Schneider, M.A.; Kapczinski, F.; de Azevedo Cardoso, T. Functional and Cognitive Impairment in the First Episode of Depression: A Systematic Review. Acta Psychiatr. Scand. 2022, 145, 156–185. [Google Scholar] [CrossRef] [PubMed]
- Bora, E.; Yucel, M.; Pantelis, C. Cognitive Endophenotypes of Bipolar Disorder: A Meta-Analysis of Neuropsychological Deficits in Euthymic Patients and Their First-Degree Relatives. J. Affect. Disord. 2009, 113, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Christensen, M.V.; Kyvik, K.O.; Kessing, L.V. Cognitive Function in Unaffected Twins Discordant for Affective Disorder. Psychol. Med. 2006, 36, 1119–1129. [Google Scholar] [CrossRef] [PubMed]
- Ladegaard, N.; Videbech, P.; Lysaker, P.H.; Larsen, E.R. The Course of Social Cognitive and Metacognitive Ability in Depression: Deficit Are Only Partially Normalized after Full Remission of First Episode Major Depression. Br. J. Clin. Psychol. 2016, 55, 269–286. [Google Scholar] [CrossRef]
- Ladegaard, N.; Lysaker, P.H.; Larsen, E.R.; Videbech, P. A Comparison of Capacities for Social Cognition and Metacognition in First Episode and Prolonged Depression. Psychiatry Res. 2014, 220, 883–889. [Google Scholar] [CrossRef]
- Bora, E.; Berk, M. Theory of Mind in Major Depressive Disorder: A Meta-Analysis. J. Affect. Disord. 2016, 191, 49–55. [Google Scholar] [CrossRef]
- Weightman, M.J.; Air, T.M.; Baune, B.T. A Review of the Role of Social Cognition in Major Depressive Disorder. Front. Psychiatry 2014, 5, 179. [Google Scholar] [CrossRef]
- Weightman, M.J.; Knight, M.J.; Baune, B.T. A Systematic Review of the Impact of Social Cognitive Deficits on Psychosocial Functioning in Major Depressive Disorder and Opportunities for Therapeutic Intervention. Psychiatry Res. 2019, 274, 195–212. [Google Scholar] [CrossRef]
- Nuechterlein, K.H.; Green, M.F.; Kern, R.S.; Baade, L.E.; Barch, D.M.; Cohen, J.D.; Essock, S.; Fenton, W.S.; Frese, F.J., 3rd; Gold, J.M.; et al. The MATRICS Consensus Cognitive Battery, Part 1: Test Selection, Reliability, and Validity. Am. J. Psychiatry 2008, 165, 203–213. [Google Scholar] [CrossRef]
- Keefe, R.S.E.; Harvey, P.D.; Goldberg, T.E.; Gold, J.M.; Walker, T.M.; Kennel, C.; Hawkins, K. Norms and Standardization of the Brief Assessment of Cognition in Schizophrenia (BACS). Schizophr. Res. 2008, 102, 108–115. [Google Scholar] [CrossRef]
- Bell, M.; Bryson, G.; Lysaker, P. Positive and Negative Affect Recognition in Schizophrenia: A Comparison with Substance Abuse and Normal Control Subjects. Psychiatry Res. 1997, 73, 73–82. [Google Scholar] [CrossRef] [PubMed]
- Kohler, C.G.; Turner, T.H.; Bilker, W.B.; Brensinger, C.M.; Siegel, S.J.; Kanes, S.J.; Gur, R.E.; Gur, R.C. Facial Emotion Recognition in Schizophrenia: Intensity Effects and Error Pattern. Am. J. Psychiatry 2003, 160, 1768–1774. [Google Scholar] [CrossRef] [PubMed]
- Corcoran, R.; Mercer, G.; Frith, C.D. Schizophrenia, Symptomatology and Social Inference: Investigating “Theory of Mind” in People with Schizophrenia. Schizophr. Res. 1995, 17, 5–13. [Google Scholar] [CrossRef]
- McDonald, S.; Flanagan, S.; Rollins, J.; Kinch, J. TASIT: A New Clinical Tool for Assessing Social Perception after Traumatic Brain Injury. J. Head Trauma Rehabil. 2003, 18, 219–238. [Google Scholar] [CrossRef] [PubMed]
- Halverson, T.F.; Hajdúk, M.; Pinkham, A.E.; Harvey, P.D.; Jarskog, L.F.; Nye, L.; Penn, D.L. Psychometric Properties of the Observable Social Cognition Rating Scale (OSCARS): Self-Report and Informant-Rated Social Cognitive Abilities in Schizophrenia. Psychiatry Res. 2020, 286, 112891. [Google Scholar] [CrossRef] [PubMed]
- Graux, J.; Thillay, A.; Morlec, V.; Sarron, P.-Y.; Roux, S.; Gaudelus, B.; Prost, Z.; Brénugat-Herné, L.; Amado, I.; Morel-Kohlmeyer, S.; et al. A Transnosographic Self-Assessment of Social Cognitive Impairments (ACSO): First Data. Front. Psychiatry 2019, 10, 847. [Google Scholar] [CrossRef] [PubMed]
- Morel-Kohlmeyer, S.; Thillay, A.; Roux, S.; Amado, I.; Brenugat, L.; Carteau-Martin, I.; Danset-Alexandre, C.; Gaudelus, B.; Graux, J.; Peyroux, E.; et al. When Alterations in Social Cognition Meet Subjective Complaints in Autism Spectrum Disorder: Evaluation With the “ClaCoS” Battery. Front. Psychiatry 2021, 12, 643551. [Google Scholar] [CrossRef]
- Haddad, C.; Salameh, P.; Hallit, S.; Sacre, H.; Clément, J.-P.; Calvet, B. Self-Assessment of Social Cognition in a Sample of Lebanese in-Patients with Schizophrenia. Schizophr. Res. Cogn. 2021, 26, 100207. [Google Scholar] [CrossRef]
- Dubreucq, J.; Gabayet, F.; Ycart, B.; Faraldo, M.; Melis, F.; Lucas, T.; Arnaud, B.; Bacconnier, M.; Bakri, M.; Cambier, G.; et al. Improving Social Function with Real-World Social-Cognitive Remediation in Schizophrenia: Results from the RemedRugby Quasi-Experimental Trial. Eur. Psychiatry 2020, 63, e41. [Google Scholar] [CrossRef]
- Sullivan, M.J.; Edgley, K.; Dehoux, E. A Survey of Multiple Sclerosis: I. Perceived Cognitive Problems and Compensatory Strategy Use. Can. J. Rehabil. 1990, 4, 99–105. [Google Scholar]
- Sumiyoshi, T.; Uchida, H.; Watanabe, K.; Oosawa, M.; Ren, H.; Moriguchi, Y.; Fujikawa, K.; Fernandez, J. Validation and Functional Relevance of the Short Form of the Perceived Deficits Questionnaire for Depression for Japanese Patients with Major Depressive Disorder. Neuropsychiatr. Dis. Treat. 2022, 18, 2507–2517. [Google Scholar] [CrossRef]
- Shi, C.; Wang, G.; Tian, F.; Han, X.; Sha, S.; Xing, X.; Yu, X. Reliability and Validity of Chinese Version of Perceived Deficits Questionnaire for Depression in Patients with MDD. Psychiatry Res. 2017, 252, 319–324. [Google Scholar] [CrossRef] [PubMed]
- Inoue, T.; Sasai, K.; Kitagawa, T.; Nishimura, A.; Inada, I. Randomized, Double-Blind, Placebo-Controlled Study to Assess the Efficacy and Safety of Vortioxetine in Japanese Patients with Major Depressive Disorder. Psychiatry Clin. Neurosci. 2020, 74, 140–148. [Google Scholar] [CrossRef] [PubMed]
- Uchino, T.; Okubo, R.; Takubo, Y.; Aoki, A.; Wada, I.; Hashimoto, N.; Ikezawa, S.; Nemoto, T. Perceptions of and Subjective Difficulties with Social Cognition in Schizophrenia from an Internet Survey: Knowledge, Clinical Experiences, and Awareness of Association with Social Functioning. Psychiatry Clin. Neurosci. 2022, 76, 429–436. [Google Scholar] [CrossRef] [PubMed]
- Okubo, R.; Yoshioka, T.; Ohfuji, S.; Matsuo, T.; Tabuchi, T. COVID-19 Vaccine Hesitancy and Its Associated Factors in Japan. Vaccines 2021, 9, 662. [Google Scholar] [CrossRef]
- Rosenbaum, P.R.; Rubin, D.B. The Central Role of the Propensity Score in Observational Studies for Causal Effects. Biometrika 1983, 70, 41–55. [Google Scholar] [CrossRef]
- Birchwood, M.; Smith, J.; Cochrane, R.; Wetton, S.; Copestake, S. The Social Functioning Scale. The Development and Validation of a New Scale of Social Adjustment for Use in Family Intervention Programmes with Schizophrenic Patients. Br. J. Psychiatry 1990, 157, 853–859. [Google Scholar] [CrossRef]
- Uchino, T.; Nemoto, T.; Kojima, A.; Takubo, Y.; Kotsuji, Y.; Yamaguchi, E.; Yamaguchi, T.; Katagiri, N.; Tsujino, N.; Tanaka, K.; et al. Effects of Motivation Domains on Social Functioning in Schizophrenia with Consideration of the Factor Structure and Confounding Influences. J. Psychiatr. Res. 2021, 133, 106–112. [Google Scholar] [CrossRef]
- Nemoto, T.; Fujii, C.; Miura, Y.; Chino, B.; Kobayashi, H.; Yamazawa, R.; Murakami, M.; Kashima, H.; Mizuno, M. Reliability and Validity of the Social Functioning Scale Japanese Version (SFS-J). Jpn. Bull. Soc. Psychiatry 2008, 17, 188–195. [Google Scholar]
- Jackson, D.L.; Gillaspy, J.A.; Purc-Stephenson, R. Reporting Practices in Confirmatory Factor Analysis: An Overview and Some Recommendations. Psychol. Methods 2009, 14, 6–23. [Google Scholar] [CrossRef]
- Schermelleh-Engell, K.; Moosbrugger, H.; Müller, H.; Engell, K. Evaluating the Fit of Structural Equation Models: Tests of Significance and Descriptive Goodness-of Fit Measures. Methods Psychol. Res. Online 2003, 8, 23–74. [Google Scholar]
- Rossier, J.; Zecca, G.; Stauffer, S.D.; Maggiori, C.; Dauwalder, J.-P. Career Adapt-Abilities Scale in a French-Speaking Swiss Sample: Psychometric Properties and Relationships to Personality and Work Engagement. J. Vocat. Behav. 2012, 80, 734–743. [Google Scholar] [CrossRef]
- Cheung, G.W.; Rensvold, R.B. Evaluating Goodness-of-Fit Indexes for Testing Measurement Invariance. Struct. Equ. Model. A Multidiscip. J. 2002, 9, 233–255. [Google Scholar] [CrossRef]
- Millsap, R.E.; Yun-Tein, J. Assessing Factorial Invariance in Ordered-Categorical Measures. Multivariate Behav. Res. 2004, 39, 479–515. [Google Scholar] [CrossRef]
- Krabbendam, L.; Arts, B.; van Os, J.; Aleman, A. Cognitive Functioning in Patients with Schizophrenia and Bipolar Disorder: A Quantitative Review. Schizophr. Res. 2005, 80, 137–149. [Google Scholar] [CrossRef]
- Schaub, A.; Goerigk, S.; Kim, T.M.; Hautzinger, M.; Roth, E.; Goldmann, U.; Charypar, M.; Engel, R.; Möller, H.-J.; Falkai, P. A 2-Year Longitudinal Study of Neuropsychological Functioning, Psychosocial Adjustment and Rehospitalisation in Schizophrenia and Major Depression. Eur. Arch. Psychiatry Clin. Neurosci. 2020, 270, 699–708. [Google Scholar] [CrossRef]
- Schaub, A.; Neubauer, N.; Mueser, K.T.; Engel, R.; Möller, H.-J. Neuropsychological Functioning in Inpatients with Major Depression or Schizophrenia. BMC Psychiatry 2013, 13, 203. [Google Scholar] [CrossRef]
- Lee, J.; Altshuler, L.; Glahn, D.C.; Miklowitz, D.J.; Ochsner, K.; Green, M.F. Social and Nonsocial Cognition in Bipolar Disorder and Schizophrenia: Relative Levels of Impairment. Am. J. Psychiatry 2013, 170, 334–341. [Google Scholar] [CrossRef]
- Kriesche, D.; Woll, C.F.J.; Tschentscher, N.; Engel, R.R.; Karch, S. Neurocognitive Deficits in Depression: A Systematic Review of Cognitive Impairment in the Acute and Remitted State. Eur. Arch. Psychiatry Clin. Neurosci. 2022, 1–24. [Google Scholar] [CrossRef]
- van Neerven, T.; Bos, D.J.; van Haren, N.E. Deficiencies in Theory of Mind in Patients with Schizophrenia, Bipolar Disorder, and Major Depressive Disorder: A Systematic Review of Secondary Literature. Neurosci. Biobehav. Rev. 2021, 120, 249–261. [Google Scholar] [CrossRef] [PubMed]
- Weiss, E.M.; Deisenhammer, E.A.; Fink, A.; Marksteiner, J.; Canazei, M.; Papousek, I. Disorder-Specific Profiles of Self-Perceived Emotional Abilities in Schizophrenia and Major Depressive Disorder. Brain Sci. 2022, 12, 356. [Google Scholar] [CrossRef] [PubMed]
- Upthegrove, R.; Marwaha, S.; Birchwood, M. Depression and Schizophrenia: Cause, Consequence, or Trans-Diagnostic Issue? Schizophr. Bull. 2017, 43, 240–244. [Google Scholar] [CrossRef] [PubMed]
- Sönmez, N.; Romm, K.L.; Andreasssen, O.A.; Melle, I.; Røssberg, J.I. Depressive Symptoms in First Episode Psychosis: A One-Year Follow-up Study. BMC Psychiatry 2013, 13, 106. [Google Scholar] [CrossRef] [PubMed]
- Michelini, G.; Palumbo, I.M.; DeYoung, C.G.; Latzman, R.D.; Kotov, R. Linking RDoC and HiTOP: A New Interface for Advancing Psychiatric Nosology and Neuroscience. Clin. Psychol. Rev. 2021, 86, 102025. [Google Scholar] [CrossRef] [PubMed]
- Shah, J.L.; Scott, J.; McGorry, P.D.; Cross, S.P.M.; Keshavan, M.S.; Nelson, B.; Wood, S.J.; Marwaha, S.; Yung, A.R.; Scott, E.M.; et al. Transdiagnostic Clinical Staging in Youth Mental Health: A First International Consensus Statement. World Psychiatry 2020, 19, 233–242. [Google Scholar] [CrossRef] [PubMed]
- Machlitt-Northen, S.; Keers, R.; Munroe, P.B.; Howard, D.M.; Pluess, M. Gene-Environment Correlation over Time: A Longitudinal Analysis of Polygenic Risk Scores for Schizophrenia and Major Depression in Three British Cohorts Studies. Genes 2022, 13, 1136. [Google Scholar] [CrossRef]
- Cross-Disorder Group of the Psychiatric Genomics Consortium Identification of Risk Loci with Shared Effects on Five Major Psychiatric Disorders: A Genome-Wide Analysis. Lancet 2013, 381, 1371–1379. [CrossRef]
- Schulze, T.G.; Akula, N.; Breuer, R.; Steele, J.; Nalls, M.A.; Singleton, A.B.; Degenhardt, F.A.; Nöthen, M.M.; Cichon, S.; Rietschel, M.; et al. Molecular Genetic Overlap in Bipolar Disorder, Schizophrenia, and Major Depressive Disorder. World J. Biol. Psychiatry 2014, 15, 200–208. [Google Scholar] [CrossRef]
- Ma, M.; Zhang, Y.; Zhang, X.; Yan, H.; Zhang, D.; Yue, W. Common and Distinct Alterations of Cognitive Function and Brain Structure in Schizophrenia and Major Depressive Disorder: A Pilot Study. Front. Psychiatry 2021, 12, 705998. [Google Scholar] [CrossRef]
- Freeman, D.; Gittins, M.; Pugh, K.; Antley, A.; Slater, M.; Dunn, G. What Makes One Person Paranoid and Another Person Anxious? The Differential Prediction of Social Anxiety and Persecutory Ideation in an Experimental Situation. Psychol. Med. 2008, 38, 1121–1132. [Google Scholar] [CrossRef] [PubMed]
- Oliveri, L.N.; Awerbuch, A.W.; Jarskog, L.F.; Penn, D.L.; Pinkham, A.; Harvey, P.D. Depression Predicts Self Assessment of Social Function in Both Patients with Schizophrenia and Healthy People. Psychiatry Res. 2020, 284, 112681. [Google Scholar] [CrossRef]
- Ermel, J.; Carter, C.S.; Gold, J.M.; MacDonald, A.W., 3rd; Daniel Ragland, J.; Silverstein, S.M.; Strauss, M.E.; Barch, D.M. Self versus Informant Reports on the Specific Levels of Functioning Scale: Relationships to Depression and Cognition in Schizophrenia and Schizoaffective Disorder. Schizophr. Res. Cogn. 2017, 9, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Belvederi Murri, M.; Respino, M.; Innamorati, M.; Cervetti, A.; Calcagno, P.; Pompili, M.; Lamis, D.A.; Ghio, L.; Amore, M. Is Good Insight Associated with Depression among Patients with Schizophrenia? Systematic Review and Meta-Analysis. Schizophr. Res. 2015, 162, 234–247. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| SSD (N = 210) Mean (SD) or % | MDD (N = 210) Mean (SD) or % | p Value | |
|---|---|---|---|
| Age | 44.49 (8.27) | 45.35 (9.10) | 0.31 |
| Sex (male/female) | 58.0/42.0 | 57.2/42.8 | 0.84 |
| Duration of illness | 10.76 (8.90) | 10.45 (8.53) | 0.71 |
| PDQ-5 Attention/concentration | 2.47 (1.34) | 2.51 (1.27) | 0.74 |
| PDQ-5 Prospective memory | 2.37 (1.25) | 2.10 (1.23) | 0.03 * |
| PDQ-5 Retrospective memory | 1.98 (1.18) | 1.81 (1.15) | 0.14 |
| PDQ-5 Planning/organization 1 | 2.39 (1.25) | 2.40 (1.23) | 0.91 |
| PDQ-5 Planning/organization 2 | 2.03 (1.21) | 1.87 (1.16) | 0.15 |
| ACSo Emotional processes | 3.67 (3.05) | 3.10 (2.73) | 0.05 * |
| ACSo Theory of mind | 4.45 (3.15) | 3.86 (3.00) | 0.05 * |
| ACSo Attributional bias | 4.07 (3.32) | 3.70 (2.87) | 0.23 |
| ACSo Social perception | 3.77 (3.02) | 3.18 (2.79) | 0.04 * |
| SFS total score | 102.31 (25.14) | 106.90 (24.22) | 0.06 |
| X2 (df) | X2/df | ΔX2 (df) | CFI | ΔCFI | RMSEA | ΔRMSEA | Judgment | |
|---|---|---|---|---|---|---|---|---|
| Configural invariance | 138.816 (65) | 2.136 | Ref | 0.978 | Ref | 0.052 | Ref | ACCEPT |
| Metric invariance | 144.458 (72) | 2.006 | 5.642 (7) | 0.978 | <0.001 | 0.049 | −0.003 | ACCEPT |
| Scalar invariance | 164.690 (82) | 2.008 | 20.232 (10) * | 0.975 | −0.003 | 0.049 | <0.001 | ACCEPT |
| Residual invariance | 184.019 (93) | 1.979 | 19.329 (11) | 0.973 | −0.002 | 0.048 | −0.001 | ACCEPT |
| Structural invariance | 184.615 (97) | 1.903 | 0.596 (4) | 0.974 | 0.001 | 0.046 | −0.002 | ACCEPT |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Uchino, T.; Okubo, R.; Takubo, Y.; Aoki, A.; Wada, I.; Hashimoto, N.; Ikezawa, S.; Nemoto, T. Mediation Effects of Social Cognition on the Relationship between Neurocognition and Social Functioning in Major Depressive Disorder and Schizophrenia Spectrum Disorders. J. Pers. Med. 2023, 13, 683. https://doi.org/10.3390/jpm13040683
Uchino T, Okubo R, Takubo Y, Aoki A, Wada I, Hashimoto N, Ikezawa S, Nemoto T. Mediation Effects of Social Cognition on the Relationship between Neurocognition and Social Functioning in Major Depressive Disorder and Schizophrenia Spectrum Disorders. Journal of Personalized Medicine. 2023; 13(4):683. https://doi.org/10.3390/jpm13040683
Chicago/Turabian StyleUchino, Takashi, Ryo Okubo, Youji Takubo, Akiko Aoki, Izumi Wada, Naoki Hashimoto, Satoru Ikezawa, and Takahiro Nemoto. 2023. "Mediation Effects of Social Cognition on the Relationship between Neurocognition and Social Functioning in Major Depressive Disorder and Schizophrenia Spectrum Disorders" Journal of Personalized Medicine 13, no. 4: 683. https://doi.org/10.3390/jpm13040683