
Effects and Safety of Wearable Exoskeleton for Robot-Assisted Gait Training: A Retrospective Preliminary Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Study Design
2.2. Wearable RAGT
2.3. Clinical Evaluation
2.4. Statistics
3. Results
3.1. Patient Characteristics
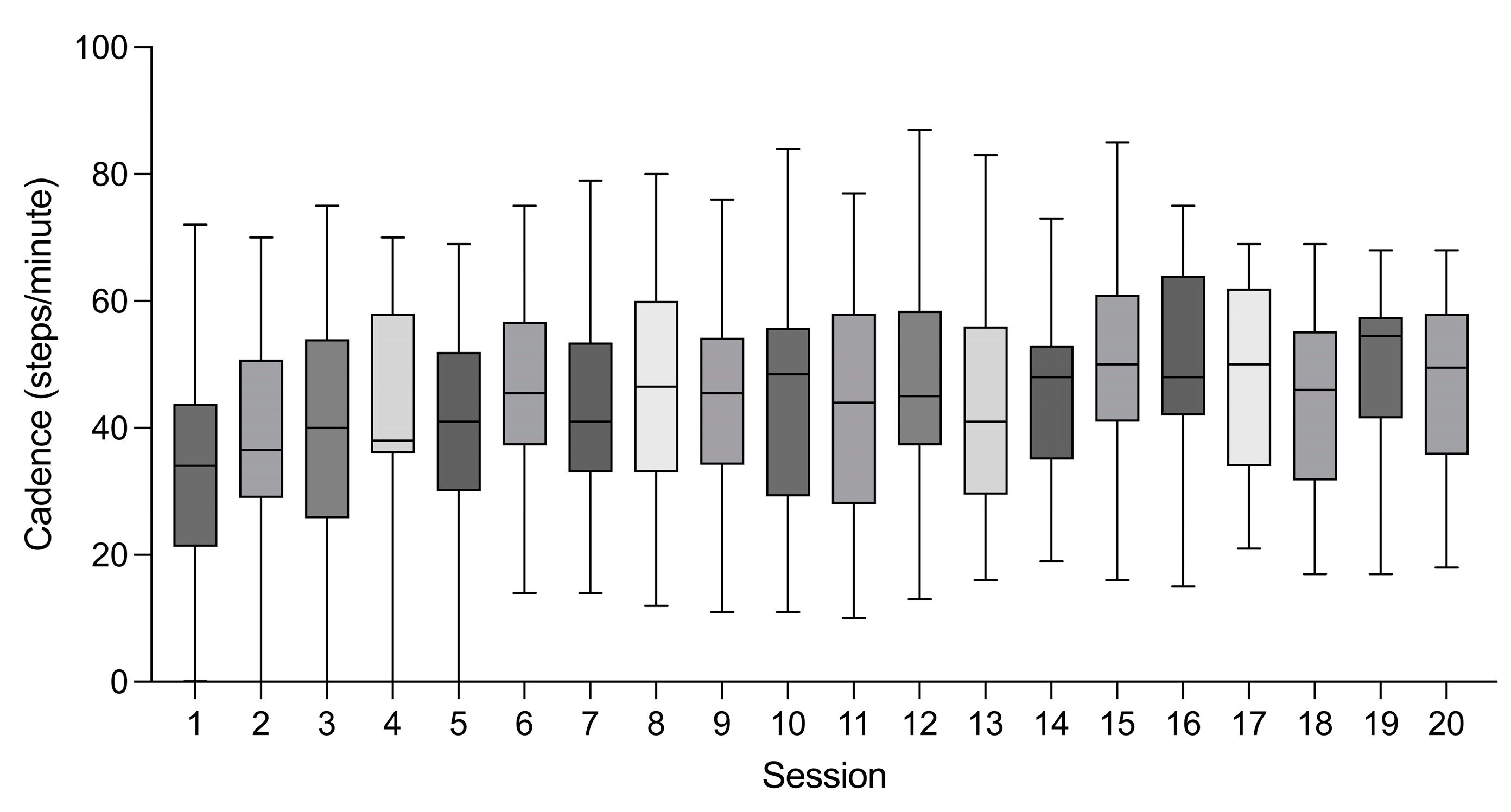
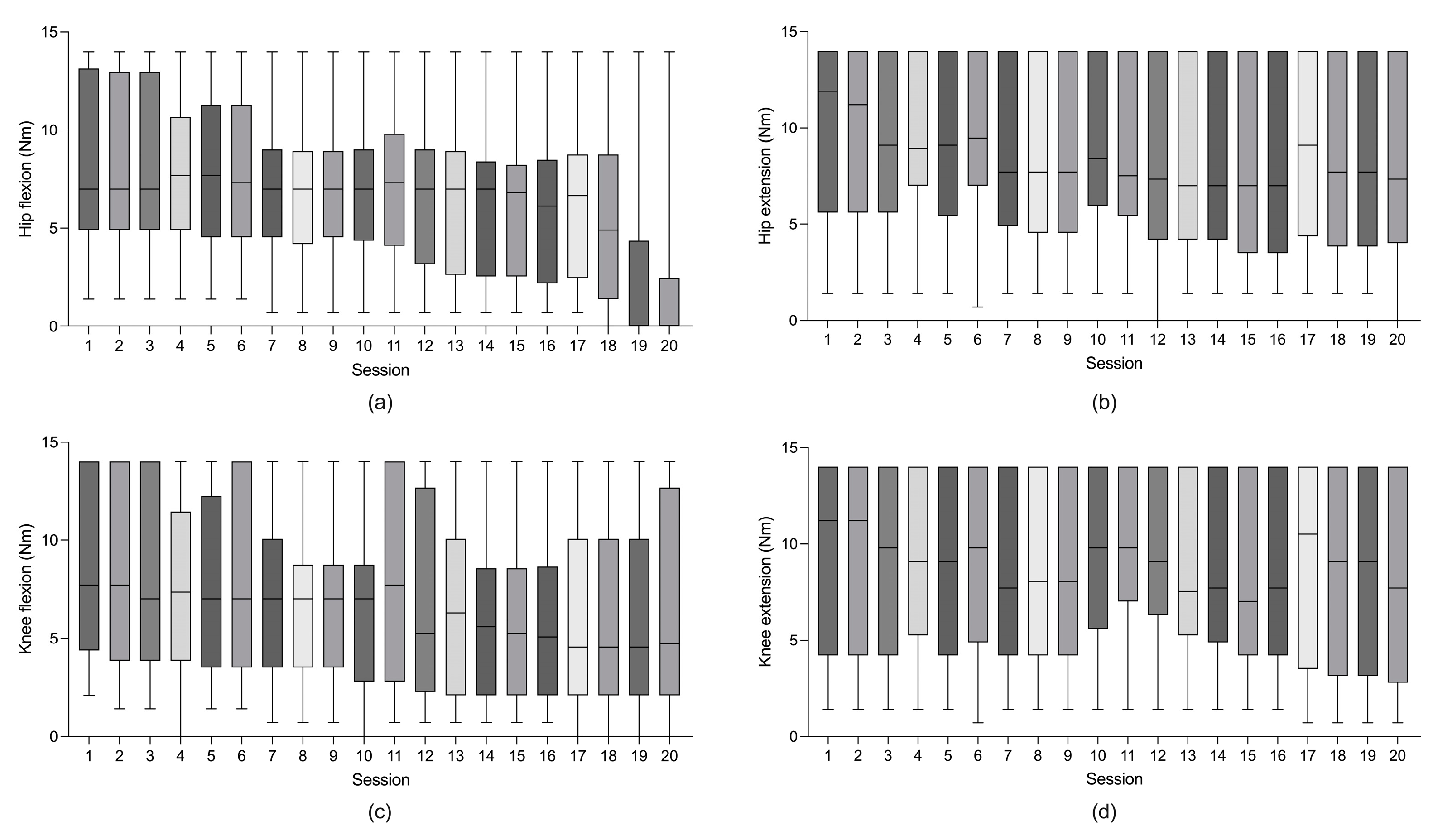
3.2. Parameters for Wearable RAGT
3.3. Changes in Clinical Outcome after RAGT
3.4. Feasibility of Wearable RAGT
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nam, K.Y.; Kim, H.J.; Kwon, B.S.; Park, J.W.; Lee, H.J.; Yoo, A. Robot-assisted gait training (Lokomat) improves walking function and activity in people with spinal cord injury: A systematic review. J. Neuroeng. Rehabil. 2017, 14, 24. [Google Scholar] [CrossRef] [PubMed]
- Booth, F.W.; Roberts, C.K.; Laye, M.J. Lack of exercise is a major cause of chronic diseases. Compr. Physiol. 2012, 2, 1143–1211. [Google Scholar] [CrossRef]
- Knight, J.A. Physical inactivity: Associated diseases and disorders. Ann. Clin. Lab. Sci. 2012, 42, 320–337. [Google Scholar] [PubMed]
- Baylor, C.; Yorkston, K.M.; Jensen, M.P.; Truitt, A.R.; Molton, I.R. Scoping review of common secondary conditions after stroke and their associations with age and time post stroke. Top. Stroke Rehabil. 2014, 21, 371–382. [Google Scholar] [CrossRef]
- Sezer, N.; Akkuş, S.; Uğurlu, F.G. Chronic complications of spinal cord injury. World J. Orthop. 2015, 6, 24–33. [Google Scholar] [CrossRef] [PubMed]
- Jensen, M.P.; Truitt, A.R.; Schomer, K.G.; Yorkston, K.M.; Baylor, C.; Molton, I.R. Frequency and age effects of secondary health conditions in individuals with spinal cord injury: A scoping review. Spinal Cord 2013, 51, 882–892. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.A.; Kim, D.H. Brain Connectivity Affecting Gait Function after Unilateral Supratentorial Stroke. Brain Sci. 2021, 11, 870. [Google Scholar] [CrossRef]
- Yang, H.E.; Kyeong, S.; Lee, S.H.; Lee, W.J.; Ha, S.W.; Kim, S.M.; Kang, H.; Lee, W.M.; Kang, C.S.; Kim, D.H. Structural and functional improvements due to robot-assisted gait training in the stroke-injured brain. Neurosci. Lett. 2017, 637, 114–119. [Google Scholar] [CrossRef]
- Hong, J.; Lee, J.; Choi, T.; Choi, W.; Kim, T.; Kwak, K.; Kim, S.; Kim, K.; Kim, D. Feasibility of Overground Gait Training Using a Joint-Torque-Assisting Wearable Exoskeletal Robot in Children with Static Brain Injury. Sensors 2022, 22, 3870. [Google Scholar] [CrossRef]
- Mehrholz, J.; Thomas, S.; Kugler, J.; Pohl, M.; Elsner, B. Electromechanical-assisted training for walking after stroke. Cochrane Database Syst. Rev. 2020, 10, 1–203. [Google Scholar] [CrossRef]
- Hornby, T.G.; Reisman, D.S.; Ward, I.G.; Scheets, P.L.; Miller, A.; Haddad, D.; Fox, E.J.; Fritz, N.E.; Hawkins, K.; Henderson, C.E.; et al. Clinical Practice Guideline to Improve Locomotor Function Following Chronic Stroke, Incomplete Spinal Cord Injury, and Brain Injury. J. Neurol. Phys. Ther. 2020, 44, 49–100. [Google Scholar] [CrossRef] [PubMed]
- Winstein, C.J.; Stein, J.; Arena, R.; Bates, B.; Cherney, L.R.; Cramer, S.C.; Deruyter, F.; Eng, J.J.; Fisher, B.; Harvey, R.L.; et al. Guidelines for Adult Stroke Rehabilitation and Recovery: A Guideline for Healthcare Professionals from the American Heart Association/American Stroke Association. Stroke 2016, 47, e98–e169. [Google Scholar] [CrossRef]
- Hesse, S.; Tomelleri, C.; Bardeleben, A.; Werner, C.; Waldner, A. Robot-assisted practice of gait and stair climbing in nonambulatory stroke patients. J. Rehabil. Res. Dev. 2012, 49, 613–622. [Google Scholar] [CrossRef]
- Stroppa, F.; Loconsole, C.; Marcheschi, S.; Frisoli, A. A robot-assisted neuro-rehabilitation system for post-stroke patients’ motor skill evaluation with ALEx exoskeleton. In Converging Clinical and Engineering Research on Neurorehabilitation II, Proceedings of the 3rd International Conference on NeuroRehabilitation (ICNR2016), Segovia, Spain, 18–21 October 2016; Springer: Cham, Switzerland, 2017; pp. 501–505. [Google Scholar]
- Mazzoleni, S.; Focacci, A.; Franceschini, M.; Waldner, A.; Spagnuolo, C.; Battini, E.; Bonaiuti, D. Robot-assisted end-effector-based gait training in chronic stroke patients: A multicentric uncontrolled observational retrospective clinical study. NeuroRehabilitation 2017, 40, 483–492. [Google Scholar] [CrossRef] [PubMed]
- Mehrholz, J.; Thomas, S.; Werner, C.; Kugler, J.; Pohl, M.; Elsner, B. Electromechanical-assisted training for walking after stroke. Cochrane Database Syst. Rev. 2017, 5, 1–125. [Google Scholar] [CrossRef]
- Mehrholz, J.; Elsner, B.; Werner, C.; Kugler, J.; Pohl, M. Electromechanical-assisted training for walking after stroke. Cochrane Database Syst. Rev. 2013, 7, 1–97. [Google Scholar] [CrossRef]
- Mehrholz, J.; Werner, C.; Kugler, J.; Pohl, M. Electromechanical-assisted training for walking after stroke. Cochrane Database Syst. Rev. 2007, 4, 1–49. [Google Scholar] [CrossRef]
- Zhang, L.; Lin, F.; Sun, L.; Chen, C. Comparison of Efficacy of Lokomat and Wearable Exoskeleton-Assisted Gait Training in People with Spinal Cord Injury: A Systematic Review and Network Meta-Analysis. Front. Neurol. 2022, 13, 772660. [Google Scholar] [CrossRef] [PubMed]
- Peri, E.; Turconi, A.C.; Biffi, E.; Maghini, C.; Panzeri, D.; Morganti, R.; Pedrocchi, A.; Gagliardi, C. Effects of dose and duration of Robot-Assisted Gait Training on walking ability of children affected by cerebral palsy. Technol. Health Care 2017, 25, 671–681. [Google Scholar] [CrossRef]
- Jin, L.H.; Yang, S.S.; Choi, J.Y.; Sohn, M.K. The Effect of Robot-Assisted Gait Training on Locomotor Function and Functional Capability for Daily Activities in Children with Cerebral Palsy: A Single-Blinded, Randomized Cross-Over Trial. Brain Sci. 2020, 10, 801. [Google Scholar] [CrossRef]
- Tedla, J.S.; Dixit, S.; Gular, K.; Abohashrh, M. Robotic-Assisted Gait Training Effect on Function and Gait Speed in Subacute and Chronic Stroke Population: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Eur. Neurol. 2019, 81, 103–111. [Google Scholar] [CrossRef] [PubMed]
- Beretta, E.; Storm, F.A.; Strazzer, S.; Frascarelli, F.; Petrarca, M.; Colazza, A.; Cordone, G.; Biffi, E.; Morganti, R.; Maghini, C.; et al. Effect of Robot-Assisted Gait Training in a Large Population of Children with Motor Impairment due to Cerebral Palsy or Acquired Brain Injury. Arch. Phys. Med. Rehabil. 2020, 101, 106–112. [Google Scholar] [CrossRef]
- Kim, D.H.; Kang, C.S.; Kyeong, S. Robot-assisted gait training promotes brain reorganization after stroke: A randomized controlled pilot study. NeuroRehabilitation 2020, 46, 483–489. [Google Scholar] [CrossRef]
- Colombo, R.; Sanguineti, V. Rehabilitation Robotics: Technology and Application; Academic Press: Cambridge, USA, 2018. [Google Scholar]
- Zhu, J.; Wen, H.; Zhang, H.; Huang, P.; Liu, L.; Hu, H. Recent advances in biodegradable electronics-from fundament to the next-generation multi-functional, medical and environmental device. Sustain. Mater. Technol. 2022, 35, e00530. [Google Scholar] [CrossRef]
- Cho, D.Y.; Park, S.W.; Lee, M.J.; Park, D.S.; Kim, E.J. Effects of robot-assisted gait training on the balance and gait of chronic stroke patients: Focus on dependent ambulators. J. Phys. Ther. Sci. 2015, 27, 3053–3057. [Google Scholar] [CrossRef]
- Calafiore, D.; Negrini, F.; Tottoli, N.; Ferraro, F.; Ozyemisci-Taskiran, O.; de Sire, A. Efficacy of robotic exoskeleton for gait rehabilitation in patients with subacute stroke: A systematic review. Eur. J. Phys. Rehabil. Med. 2022, 58, 1–8. [Google Scholar] [CrossRef]
- Rodríguez-Fernández, A.; Lobo-Prat, J.; Font-Llagunes, J.M. Systematic review on wearable lower-limb exoskeletons for gait training in neuromuscular impairments. J. Neuroeng. Rehabil. 2021, 18, 22. [Google Scholar] [CrossRef]
- Molteni, F.; Guanziroli, E.; Goffredo, M.; Calabrò, R.S.; Pournajaf, S.; Gaffuri, M.; Gasperini, G.; Filoni, S.; Baratta, S.; Galafate, D.; et al. Gait Recovery with an Overground Powered Exoskeleton: A Randomized Controlled Trial on Subacute Stroke Subjects. Brain Sci. 2021, 11, 104. [Google Scholar] [CrossRef]
- Holden, M.K.; Gill, K.M.; Magliozzi, M.R.; Nathan, J.; Piehl-Baker, L. Clinical gait assessment in the neurologically impaired. Reliability and meaningfulness. Phys. Ther. 1984, 64, 35–40. [Google Scholar] [CrossRef] [PubMed]
- Collin, C.; Wade, D. Assessing motor impairment after stroke: A pilot reliability study. J. Neurol. Neurosurg. Psychiatry 1990, 53, 576–579. [Google Scholar] [CrossRef] [PubMed]
- Berg, K.; Wood-Dauphinee, S.; Williams, J.I. The Balance Scale: Reliability assessment with elderly residents and patients with an acute stroke. Scand. J. Rehabil. Med. 1995, 27, 27–36. [Google Scholar] [PubMed]
- Gladstone, D.J.; Danells, C.J.; Black, S.E. The fugl-meyer assessment of motor recovery after stroke: A critical review of its measurement properties. Neurorehabil. Neural Repair 2002, 16, 232–240. [Google Scholar] [CrossRef] [PubMed]
- Kleyweg, R.P.; van der Meché, F.G.; Schmitz, P.I. Interobserver agreement in the assessment of muscle strength and functional abilities in Guillain-Barré syndrome. Muscle Nerve 1991, 14, 1103–1109. [Google Scholar] [CrossRef] [PubMed]
- Colombo, G.; Joerg, M.; Schreier, R.; Dietz, V. Treadmill training of paraplegic patients using a robotic orthosis. J. Rehabil. Res. Dev. 2000, 37, 693–700. [Google Scholar]
- Seo, J.S.; Yang, H.S.; Jung, S.; Kang, C.S.; Jang, S.; Kim, D.H. Effect of reducing assistance during robot-assisted gait training on step length asymmetry in patients with hemiplegic stroke: A randomized controlled pilot trial. Medicine 2018, 97, e11792. [Google Scholar] [CrossRef]
- Chisholm, A.E.; Alamro, R.A.; Williams, A.M.; Lam, T. Overground vs. treadmill-based robotic gait training to improve seated balance in people with motor-complete spinal cord injury: A case report. J. Neuroeng. Rehabil. 2017, 14, 27. [Google Scholar] [CrossRef] [PubMed]
- Zeilig, G.; Weingarden, H.; Zwecker, M.; Dudkiewicz, I.; Bloch, A.; Esquenazi, A. Safety and tolerance of the ReWalk™ exoskeleton suit for ambulation by people with complete spinal cord injury: A pilot study. J. Spinal Cord Med. 2012, 35, 96–101. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | Values |
|---|---|
| Demographics | |
| Mean age (years, mean ± SD) | 43.9 ± 22.4 |
| Male:Female (n, %) | 17 (60.7):11 (39.3) |
| Height (cm, mean ± SD) | 167.1 ± 10.5 |
| Weight (kg, mean ± SD) | 64.4 ± 12.4 |
| Diagnosis (n, percentage) | |
| Brain injury | 19 (68.0) |
| Stroke | 7 (25.0) |
| Cerebral palsy | 9 (32.1) |
| etc. | 3 (10.7) |
| Spinal cord injury | 7 (25.0) |
| Trauma | 2 (7.1) |
| Tumor | 3 (10.7) |
| etc. | 2 (7.1) |
| Peripheral nerve injury | 2 (7.1) |
| CIDP | 2 (7.1) |
| Clinical Measure | Values | p-Value | |
|---|---|---|---|
| Before RAGT | After RAGT | ||
| All patients | |||
| MRC * | 36.6 ± 2.1 | 37.8 ± 2.4 | 0.012 † |
| BBS ** | 24.9 ± 3.3 | 32.2 ± 3.2 | 0.001 † |
| FAC * | 1.8 ± 0.4 | 2.7 ± 0.3 | 0.030 |
| TCT | 59.4 ± 4.0 | 79.4 ± 5.8 | 0.057 |
| Brain injury | |||
| MRC * | 39.4 ± 1.5 | 40.8 ± 1.5 | 0.017 † |
| BBS ** | 23.5 ± 3.6 | 30.6 ± 3.2 | 0.001 † |
| FAC | 1.8 ± 0.5 | 2.6 ± 0.4 | 0.053 |
| TCT | 59.4 ± 4.0 | 79.4 ± 5.8 | 0.057 |
| FMLL | 13.0 ± 3.8 | 22.6 ± 3.4 | 0.062 |
| Spinal cord injury | |||
| MRC | 22.2 ± 6.6 | 24.6 ± 8.3 | 0.586 |
| BBS | 25.3 ± 7.5 | 34.0 ± 11.2 | 0.371 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, G.-M.; Cho, S.-H.; Hong, J.-T.; Kim, D.-H.; Shin, J.-C. Effects and Safety of Wearable Exoskeleton for Robot-Assisted Gait Training: A Retrospective Preliminary Study. J. Pers. Med. 2023, 13, 676. https://doi.org/10.3390/jpm13040676
Park G-M, Cho S-H, Hong J-T, Kim D-H, Shin J-C. Effects and Safety of Wearable Exoskeleton for Robot-Assisted Gait Training: A Retrospective Preliminary Study. Journal of Personalized Medicine. 2023; 13(4):676. https://doi.org/10.3390/jpm13040676
Chicago/Turabian StylePark, Gwang-Min, Su-Hyun Cho, Jun-Taek Hong, Dae-Hyun Kim, and Ji-Cheol Shin. 2023. "Effects and Safety of Wearable Exoskeleton for Robot-Assisted Gait Training: A Retrospective Preliminary Study" Journal of Personalized Medicine 13, no. 4: 676. https://doi.org/10.3390/jpm13040676