
Evolution in Endoscopic Sinus Surgery: The Adjuvant Role of Reboot Surgery in Patients with Uncontrolled Nasal Symptoms of Eosinophilic Granulomatosis with Polyangiitis

 , , , , , , and
, , , , , , and 
Abstract
:1. Introduction
2. Patients and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jennette, J.C.; Falk, R.J.; Bacon, P.A.; Basu, N.; Cid, M.C.; Ferrario, F.; Flores-Suarez, L.F.; Gross, W.L.; Guillevin, L.; Hagen, E.C.; et al. 2012 Revised International Chapel Hill Consensus Conference Nomenclature of Vasculitides. Arthritis Rheum 2013, 65, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Cottin, V.; Khouatra, C.; Dubost, R.; Glérant, J.-C.; Cordier, J.-F. Persistent Airflow Obstruction in Asthma of Patients with Churg-Strauss Syndrome and Long-Term Follow-Up. Allergy 2009, 64, 589–595. [Google Scholar] [CrossRef] [PubMed]
- Guillevin, L.; Cohen, P.; Gayraud, M.; Lhote, F.; Jarrousse, B.; Casassus, P. Churg-Strauss Syndrome. Clinical Study and Long-Term Follow-up of 96 Patients. Medicine 1999, 78, 26–37. [Google Scholar] [CrossRef] [PubMed]
- Comarmond, C.; Pagnoux, C.; Khellaf, M.; Cordier, J.-F.; Hamidou, M.; Viallard, J.-F.; Maurier, F.; Jouneau, S.; Bienvenu, B.; Puéchal, X.; et al. Eosinophilic Granulomatosis with Polyangiitis (Churg-Strauss): Clinical Characteristics and Long-Term Followup of the 383 Patients Enrolled in the French Vasculitis Study Group Cohort. Arthritis Rheum 2013, 65, 270–281. [Google Scholar] [CrossRef] [PubMed]
- Bacciu, A.; Buzio, C.; Giordano, D.; Pasanisi, E.; Vincenti, V.; Mercante, G.; Grasselli, C.; Bacciu, S. Nasal Polyposis in Churg-Strauss Syndrome. Laryngoscope 2008, 118, 325–329. [Google Scholar] [CrossRef] [PubMed]
- Cottin, V.; Bel, E.; Bottero, P.; Dalhoff, K.; Humbert, M.; Lazor, R.; Sinico, R.A.; Sivasothy, P.; Wechsler, M.E.; Groh, M.; et al. Respiratory Manifestations of Eosinophilic Granulomatosis with Polyangiitis (Churg-Strauss). Eur. Respir. J. 2016, 48, 1429–1441. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chung, S.A.; Langford, C.A.; Maz, M.; Abril, A.; Gorelik, M.; Guyatt, G.; Archer, A.M.; Conn, D.L.; Full, K.A.; Grayson, P.C.; et al. 2021 American College of Rheumatology/Vasculitis Foundation Guideline for the Management of Antineutrophil Cytoplasmic Antibody–Associated Vasculitis. Arthritis Rheumatol. 2021, 73, 1366–1383. [Google Scholar] [CrossRef] [PubMed]
- Wechsler, M.E.; Akuthota, P.; Jayne, D.; Khoury, P.; Klion, A.; Langford, C.A.; Merkel, P.A.; Moosig, F.; Specks, U.; Cid, M.C.; et al. Mepolizumab or Placebo for Eosinophilic Granulomatosis with Polyangiitis. N. Engl. J. Med. 2017, 376, 1921–1932. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raffray, L.; Guillevin, L. Updates for the Treatment of EGPA. Presse. Med. 2020, 49, 104036. [Google Scholar] [CrossRef] [PubMed]
- Seccia, V.; Baldini, C.; Latorre, M.; Gelardi, M.; Dallan, I.; Cristofani-Mencacci, L.; Sellari-Franceschini, S.; Bartoli, M.L.; Bacci, E.; Paggiaro, P. Focus on the Involvement of the Nose and Paranasal Sinuses in Eosinophilic Granulomatosis with Polyangiitis (Churg-Strauss Syndrome): Nasal Cytology Reveals Infiltration of Eosinophils as a Very Common Feature. Int. Arch. Allergy Immunol. 2018, 175, 61–69. [Google Scholar] [CrossRef] [PubMed]
- Alsharif, S.; Jonstam, K.; van Zele, T.; Gevaert, P.; Holtappels, G.; Bachert, C. Endoscopic Sinus Surgery for Type-2 CRS WNP: An Endotype-Based Retrospective Study. Laryngoscope 2019, 129, 1286–1292. [Google Scholar] [CrossRef] [PubMed]
- Malvezzi, L.; Pirola, F.; De Virgilio, A.; Heffler, E. Long-Lasting Clinical, Radiological and Immunological Remission of Severe Nasal Polyposis by Means of ‘Reboot’ Surgery. BMJ Case Rep. 2020, 13, e233726. [Google Scholar] [CrossRef] [PubMed]
- Pirola, F.; Pace, G.M.; Giombi, F.; Heffler, E.; Paoletti, G.; Nappi, E.; Sanità, W.; Giulietti, G.; Giunta, G.; Ferreli, F.; et al. Outcomes of Non-Mucosa Sparing Endoscopic Sinus Surgery (Partial Reboot) in Refractory Chronic Rhinosinusitis with Nasal Polyposis: An Academic Hospital Experience. Laryngoscope 2022. epub ahead of print. [Google Scholar] [CrossRef]
- Jayne, D.R.W.; Merkel, P.A.; Schall, T.J.; Bekker, P.; ADVOCATE Study Group. Avacopan for the treatment of ANCA-associated vasculitis. N. Engl. J. Med. 2021, 384, 599–609. [Google Scholar] [CrossRef] [PubMed]
- Walsh, M.; Merkel, P.A.; Peh, C.-A.; Szpirt, W.M.; Puéchal, X.; Fujimoto, S.; Hawley, C.M.; Khalidi, N.; Floßmann, O.; Wald, R.; et al. Plasma Exchange and Glucocorticoids in Severe ANCA-Associated Vasculitis. N. Engl. J. Med. 2020, 382, 622–631. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Patient #1 | Patient #2 | |||
|---|---|---|---|---|
| PRE | POST | PRE | POST | |
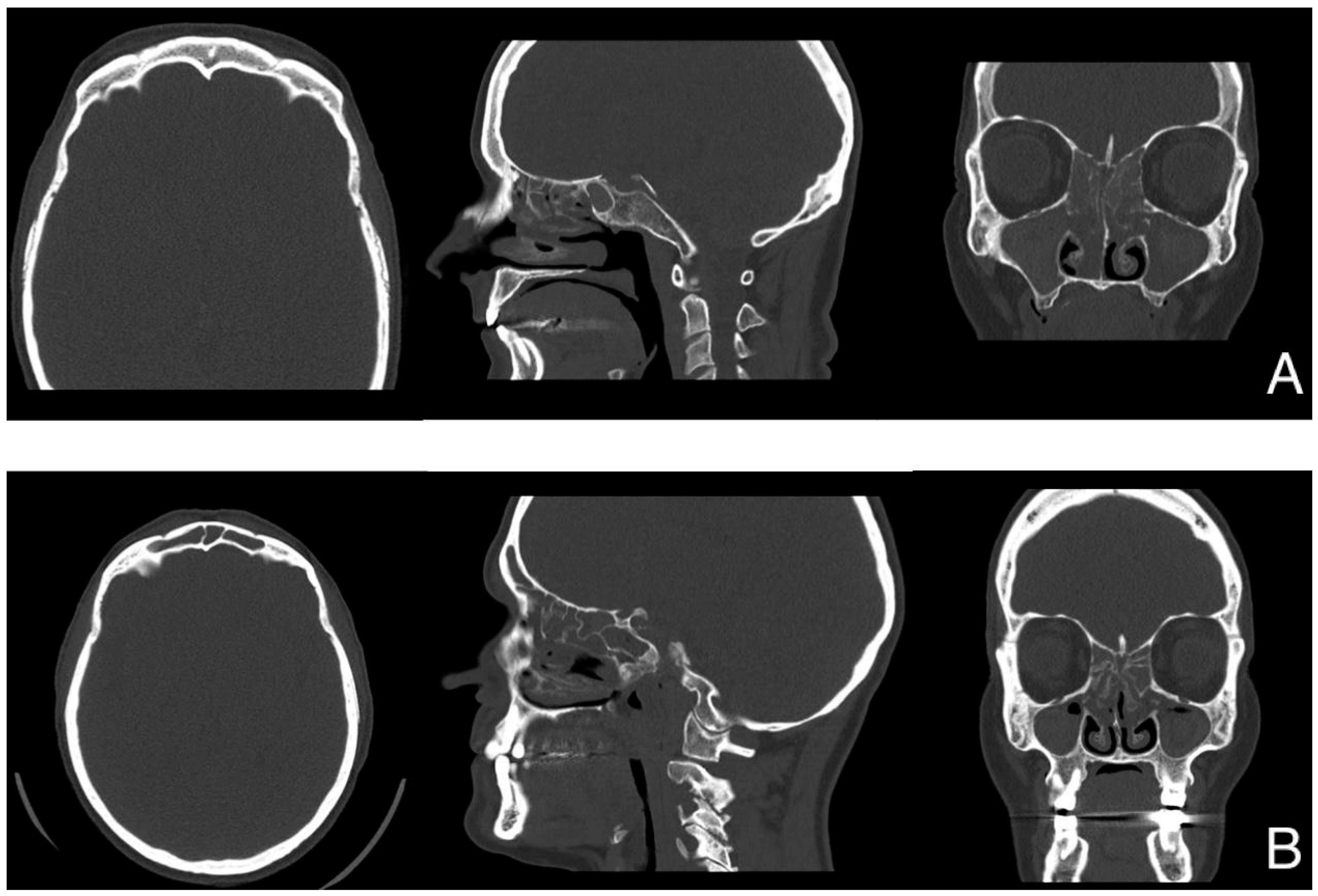
| Lund-Mackay score | 18/20 * | n.a. | 22/24 | n.a. |
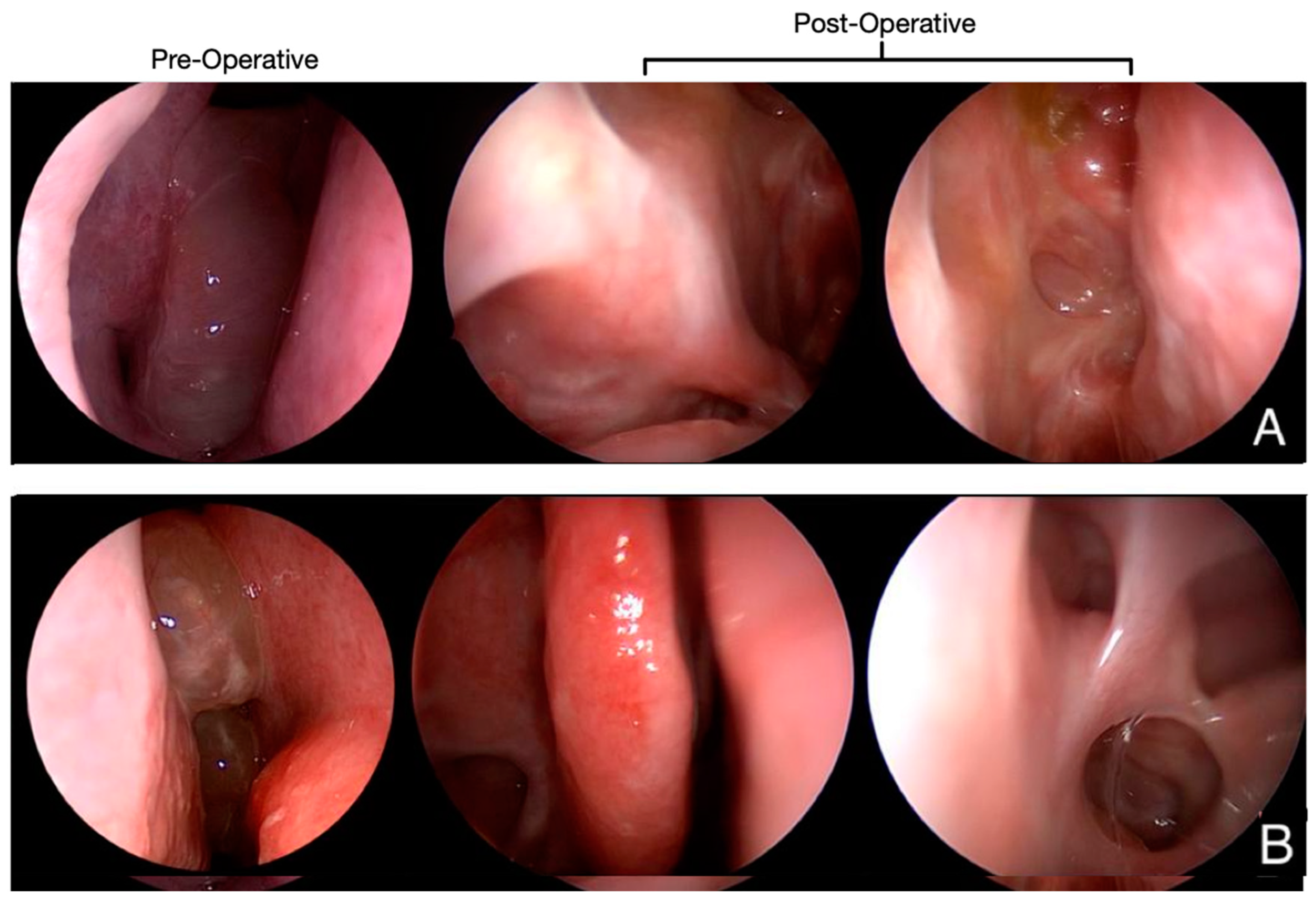
| Nasal endoscopy | NPS 3 (L) | NPS 0 (L) | NPS 3 (L) | NPS 0 (L) |
| NPS 4 (R) | NPS 0 (R) | NPS 3 (R) | NPS 0 (R) | |
| SNOT-22 | 56 | 11 | 104 | 21 |
| VAS (out of 10) | ||||
| Nasal obstruction | 7 | 0 | 9 | 0 |
| Hyposmia | 10 | 0 | 9 | 3 |
| Dysgeusia | 10 | 0 | 7 | 3 |
| Headache or facial pain/pressure | 0 | 0 | 9 | 0 |
| Anterior rhinorrhea | 7 | 0 | 5 | 1 |
| Posterior rhinorrhea | 6 | 1 | 5 | 2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pirola, F.; Giunta, G.; Muci, G.; Giombi, F.; Nappi, E.; Grizzi, F.; Heffler, E.; Paoletti, G.; Canonica, G.W.; Mercante, G.; et al. Evolution in Endoscopic Sinus Surgery: The Adjuvant Role of Reboot Surgery in Patients with Uncontrolled Nasal Symptoms of Eosinophilic Granulomatosis with Polyangiitis. J. Pers. Med. 2023, 13, 647. https://doi.org/10.3390/jpm13040647
Pirola F, Giunta G, Muci G, Giombi F, Nappi E, Grizzi F, Heffler E, Paoletti G, Canonica GW, Mercante G, et al. Evolution in Endoscopic Sinus Surgery: The Adjuvant Role of Reboot Surgery in Patients with Uncontrolled Nasal Symptoms of Eosinophilic Granulomatosis with Polyangiitis. Journal of Personalized Medicine. 2023; 13(4):647. https://doi.org/10.3390/jpm13040647
Chicago/Turabian StylePirola, Francesca, Gianmarco Giunta, Giovanna Muci, Francesco Giombi, Emanuele Nappi, Fabio Grizzi, Enrico Heffler, Giovanni Paoletti, Giorgio Walter Canonica, Giuseppe Mercante, and et al. 2023. "Evolution in Endoscopic Sinus Surgery: The Adjuvant Role of Reboot Surgery in Patients with Uncontrolled Nasal Symptoms of Eosinophilic Granulomatosis with Polyangiitis" Journal of Personalized Medicine 13, no. 4: 647. https://doi.org/10.3390/jpm13040647