

Effects of Different Forms of Sensorimotor Training on Postural Control and Functional Status in Patients with Chronic Low Back Pain

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Oswestry Low Back Pain Questionnaire
2.3. Posturography
2.4. Interventions
2.4.1. Sensorimotor Physiotherapy Training
2.4.2. Gallileo® Training
2.4.3. Posturomed® Training
2.5. Statistics
3. Results
3.1. Participants
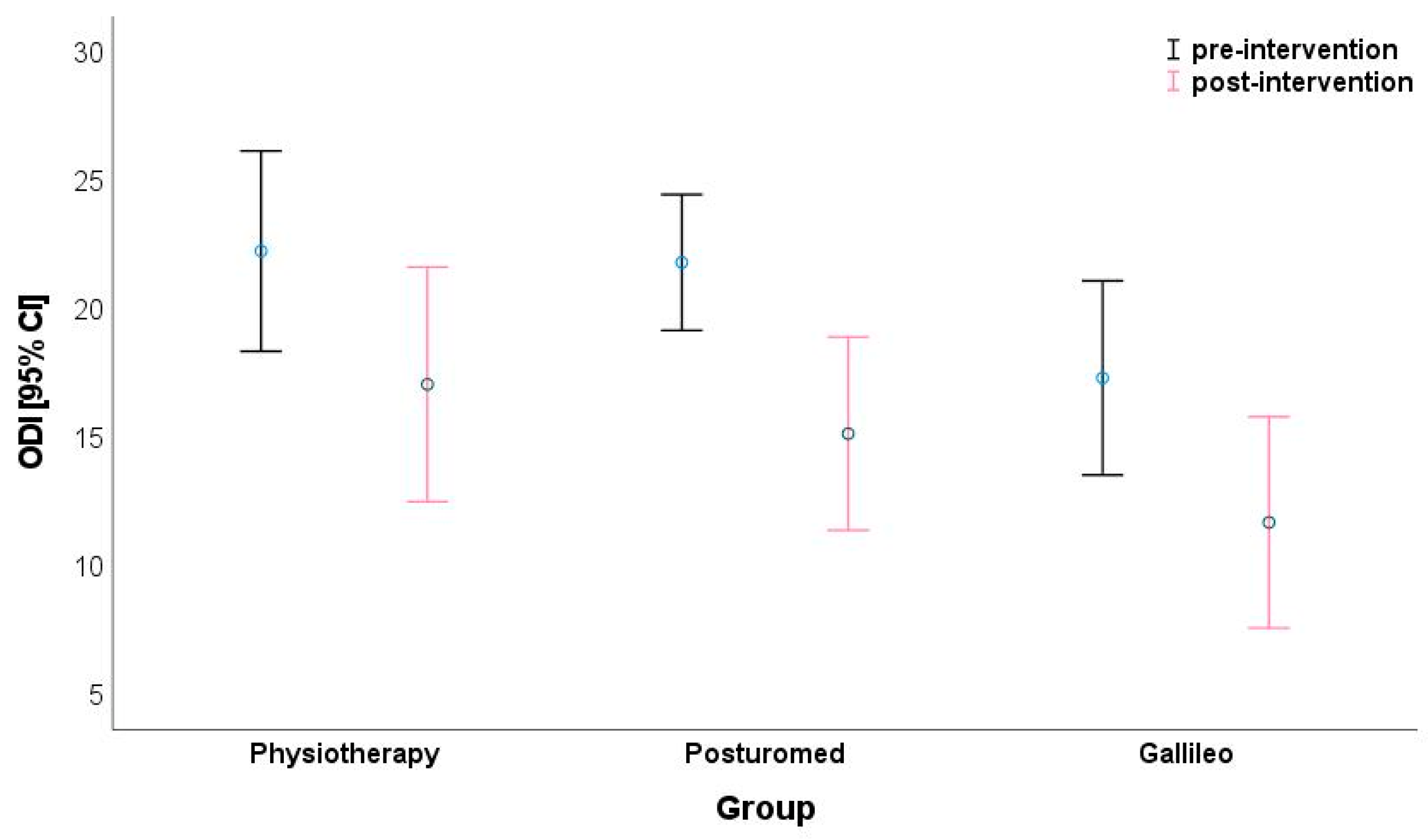
3.2. Oswestry Disability Index (ODI)
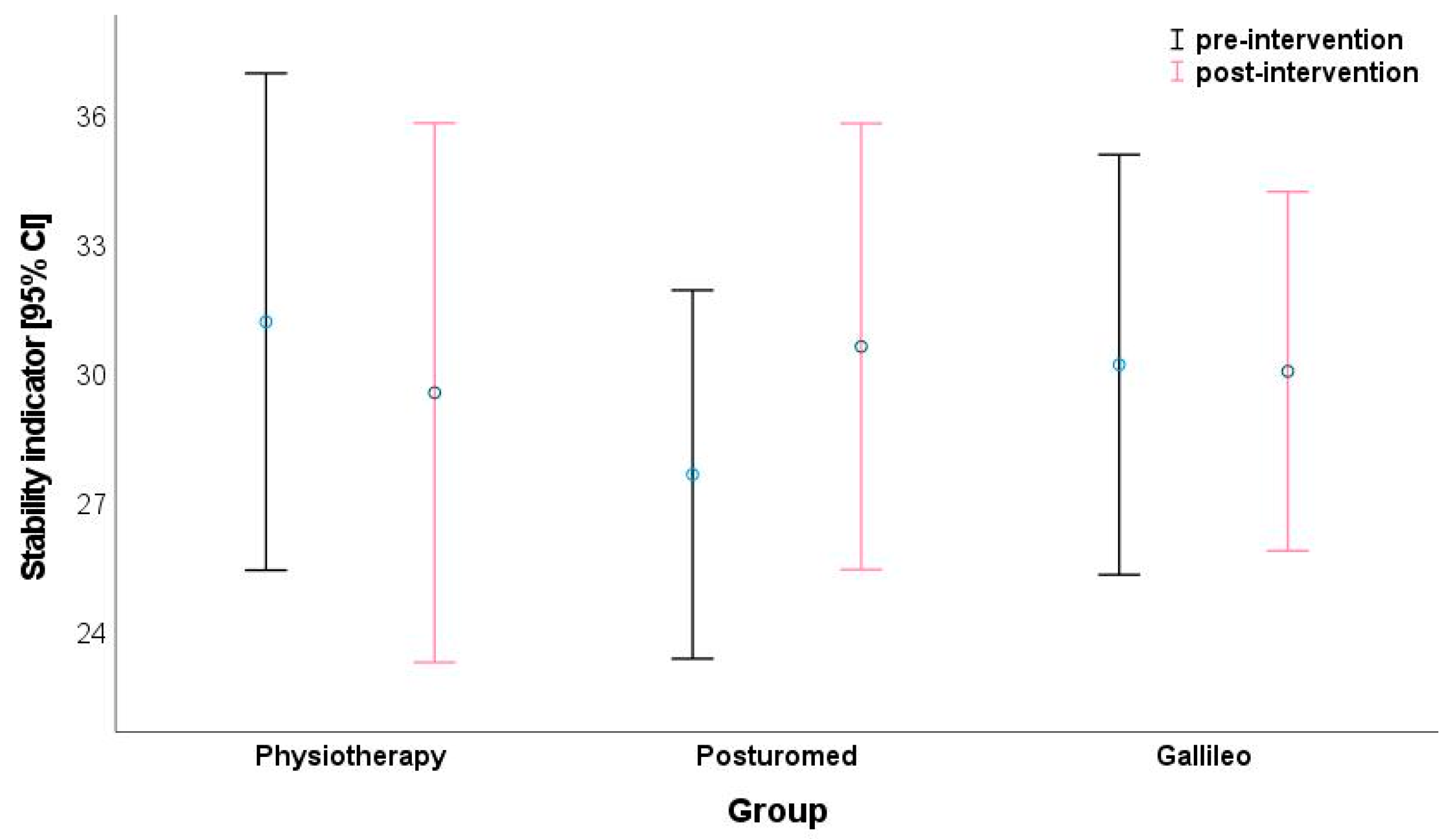
3.3. Posturography
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chenot, J.F.; Greitemann, B.; Kladny, B.; Petzke, F.; Pfingsten, M.; Schorr, S.G. Non-Specific Low Back Pain. Dtsch. Arztebl. Int. 2017, 114, 883–890. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rothman, M.G.; Ortendahl, M.; Rosenblad, A.; Johansson, A.-C. Improved quality of life, working ability, and patient satisfaction after a pretreatment multimodal assessment method in patients with mixed chronic muscular pain: A randomized-controlled study. Clin. J. Pain 2013, 29, 195–204. [Google Scholar] [CrossRef] [PubMed]
- Taube, W. Neuronale Mechanismen der Posturalen Kontrolle und der Einfluss von Gleichgewichtstraining. J. Neurol. Neurochir. Psychiatr. 2012, 14, 55–63. [Google Scholar]
- Otte, C.; Rašev, E. Posturale Aspekte der Schmerztherapie des Bewegungssystems. Man. Med. 2010, 48, 267–274. [Google Scholar] [CrossRef]
- Müller, K.; Schwesig, R.; Leuchte, S.; Riede, D. Coordinative treatment and quality of life—A randomised trial of nurses with back pain. Gesundheitswesen 2001, 63, 609–618. [Google Scholar] [CrossRef] [PubMed]
- Hodges, P.W.; Moseley, G.L. Pain and motor control of the lumbopelvic region: Effect and possible mechanisms. J. Electromyogr. Kinesiol. 2003, 13, 361–370. [Google Scholar] [CrossRef]
- Wilke, H.J.; Wolf, S.; Claes, L.E.; Arand, M.; Wiesend, A. Stability increase of the lumbar spine with different muscle groups. A biomechanical in vitro study. Spine 1995, 20, 192–198. [Google Scholar] [CrossRef]
- Tesh, K.M.; Dunn, J.S.; Evans, J.H. The abdominal muscles and vertebral stability. Spine 1987, 12, 501–508. [Google Scholar] [CrossRef]
- Cresswell, A.G.; Thorstensson, A. Changes in intra-abdominal pressure, trunk muscle activation and force during isokinetic lift ing and lowering. Eur. J. Appl. Physiol. Occup. Physiol. 1994, 68, 315–321. [Google Scholar] [CrossRef]
- Cresswell, A.G.; Oddsson, L.; Thorstensson, A. The influence of sudden perturbations on trunk muscle activity and intra-ab-dominal pressure while standing. Exp. Brain Res. 1994, 98, 336–341. [Google Scholar] [CrossRef]
- Hodges, P.W.; Richardson, C.A. Inefficient muscular stabilization of the lumbar spine associated with low back pain. A motor control evaluation of transversus abdominis. Spine 1996, 21, 2640–2650. [Google Scholar] [CrossRef]
- Hides, J.A.; Stanton, W.R.; McMahon, S.; Sims, K.; Richardson, C.A. Effect of stabilization training on multifidus muscle cross-sectional area among young elite cricketers with low back pain. J. Orthop. Sport. Phys. Ther. 2008, 38, 101–108. [Google Scholar] [CrossRef] [Green Version]
- Sihvonen, T.; Partanen, J. Segmental hypermobility in lumbar spine and entrapment of dorsal rami. Electromyogr. Clin. Neurophysiol. 1990, 30, 175–180. [Google Scholar]
- Lindgren, K.A.; Sihvonen, T.; Leino, E.; Pitkänen, M.; Manninen, H. Exercise therapy effects on functional radiographic findings and segmental electromyographic activity in lumbar spine instability. Arch. Phys. Med. Rehabil. 1993, 74, 933–939. [Google Scholar]
- Smith, D.; Bissell, G.; Bruce-Low, S.; Wakefield, C. The effect of lumbar extension training with and without pelvic stabilization on lumbar strength and low back pain. J. Back Musculoskelet. Rehabil. 2011, 24, 241–249. [Google Scholar] [CrossRef] [Green Version]
- França, F.R.; Burke, T.N.; Caffaro, R.R.; Ramos, L.A.; Marques, A.P. Effects of muscular stretching and segmental stabilization on functional disability and pain in patients with chronic low back pain: A randomized, controlled trial. J. Manip. Physiol. Ther. 2012, 35, 279–285. [Google Scholar] [CrossRef]
- Javadian, Y.; Behtash, H.; Akbari, M.; Taghipour-Darzi, M.; Zekavat, H. The effects of stabilizing exercises on pain and disability of patients with lumbar segmental instability. J. Back Musculoskelet. Rehabil. 2012, 25, 149–155. [Google Scholar] [CrossRef] [Green Version]
- Tsao, H.; Hodges, P.W. Immediate changes in feedforward postural adjustments following voluntary motor training. Exp. Brain Res. 2007, 181, 537–546. [Google Scholar] [CrossRef]
- Tsigkanos, C.; Gaskell, L.; Smirniotou, A.; Tsigkanos, G. Static and dynamic balance deficiencies in chronic low back pain. J. Back Musculoskelet. Rehabil. 2016, 29, 887–893. [Google Scholar] [CrossRef]
- da Silva, R.A.; Vieira, E.R.; Fernandes, K.B.P.; Andraus, R.A.; Oliveira, M.R.; Sturion, L.A.; Calderon, M.G. People with chronic low back pain have poorer balance than controls in challenging tasks. Disabil. Rehabil. 2018, 40, 1294–1300. [Google Scholar] [CrossRef]
- Müller, O.; Günther, M.; Krauß, I.; Horstmann, T. Physical characterization of the therapeutic device Posturomed as a measuring device--presentation of a procedure to characterize balancing ability. Biomed. Tech. 2004, 49, 56–60. [Google Scholar] [CrossRef] [PubMed]
- Bongiovanni, L.G.; Hagbarth, K.E.; Stjernberg, L. Prolonged muscle vibration reducing motor output in maximal voluntary contractions in man. J. Physiol. 1990, 423, 15–26. [Google Scholar] [CrossRef] [PubMed]
- Fontana, T.L.; Richardson, C.A.; Stanton, W.R. The effect of weightbearing exercise with low frequency, whole body vibration on lumbosacral proprioception: A pilot study on normal subjects. Aust. J. Physiother. 2005, 51, 259–263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Del Pozo-Cruz, B.; Hernández-Mocholí, M.A.; Adsuar, J.C.; Parraca, J.A.; Muro, I.; Gusi, N. Effects of whole body vibration therapy on main outcome measures for chronic non-specific low back pain: A single-blind randomized controlled trial. J. Rehabil. Med. 2011, 43, 689–694. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, J.; Seo, D. The effects of whole body vibration on static balance, spinal curvature, pain, and disability of patients with low back pain. J. Phys. Ther. Sci. 2015, 27, 805–808. [Google Scholar] [CrossRef] [Green Version]
- Chow, D.H.K.; Lee, T.Y.; Pope, M.H. Effects of whole body vibration on spinal proprioception in healthy individuals. Work 2018, 61, 403–411. [Google Scholar] [CrossRef] [Green Version]
- Mannion, A.F.; Junge, A.; Fairbank, J.C.T.; Dvorak, J.; Grob, D. Development of a German version of the Oswestry Disability Index. Part 1: Cross-cultural adaptation, reliability, and validity. Eur. Spine J. 2006, 15, 55–65. [Google Scholar] [CrossRef] [Green Version]
- Gaul, C.; Mette, E.; Schmidt, T.; Grond, S. Praxistauglichkeit einer Deutschen Version des Oswestry Low Back Pain Disability Questionnaire. Ein Fragebogen zur Beeinträchtigung durch Rückenschmerzen. Schmerz 2008, 22, 51–58. [Google Scholar] [CrossRef]
- Schwesig, R.; Becker, S.; Fischer, D. Intraobserver reliability of posturography in healthy subjects. Somatosens. Mot. Res. 2014, 31, 16–22. [Google Scholar] [CrossRef]
- Schwesig, R.; Lauenroth, A.; Müller, A.; Becker, S.; Hottenrott, K. Parametrisierung posturaler Subsysteme mit Posturografie. Man. Med. 2006, 44, 376–384. [Google Scholar] [CrossRef]
- Schwesig, R.; Becker, S.; Lauenroth, A.; Kluttig, A.; Leuchte, S.; Esperer, H.D. A novel posturographic method to differentiate sway patterns of patients with Parkinson’s disease from patients with cerebellar ataxia. Biomed. Tech. 2009, 54, 347–356. [Google Scholar] [CrossRef]
- Lauenroth, A.; Reinhardt, L.; Schulze, S.; Laudner, K.G.; Delank, K.S.; Schwesig, R. Does low back pain affect the reliability of postural regulation? Somatosens. Mot. Res. 2019, 36, 116–121. [Google Scholar] [CrossRef]
- Bortz, J. Basic principle of one-factorial analysis of variance. In Statistics for Social Scientists; Springer: New York, NY, USA, 1999; pp. 237–249. [Google Scholar]
- Richardson, J.T.E. Eta squared and partial eta squared as measures of effect size in educational research. Educ. Res. Rev. 2011, 6, 135–147. [Google Scholar] [CrossRef]
- Brooks, C.; Kennedy, S.; Marshall, P.W.M. Specific trunk and general exercise elicit similar changes in anticipatory postural adjustments in patients with chronic low back pain: A randomized controlled trial. Spine 2012, 37, E1543–E1550. [Google Scholar] [CrossRef]
- Kaeding, T.S.; Karch, A.; Schwarz, R.; Flor, T.; Wittke, T.C.; Kück, M.; Böselt, G.; Tegtbur, U.; Stein, L. Whole-body vibration training as a workplace-based sports activity for employees with chronic low-back pain. Scand. J. Med. Sci. Sports 2017, 27, 2027–2039. [Google Scholar] [CrossRef]
- McCaskey, M.A.; Wirth, B.; Schuster-Amft, C.; de Bruin, E.D. Postural sensorimotor training versus sham exercise in physiotherapy of patients with chronic non-specific low back pain: An exploratory randomised controlled trial. PLoS ONE 2018, 13, e0193358. [Google Scholar] [CrossRef] [Green Version]
- Wegener, V.; Rarack, S.; Tiffe, T.; Grill, E.; Melcher, C.; Birkenmaier, C.; Jansson, V.; Wegener, B. Effects of Whole Body Vibration Therapy and Classic Physiotherapy on Postural Stability in People with Back Pain: A Randomized Trial. Clin. Spine Surg. 2019, 32, E214–E220. [Google Scholar] [CrossRef]
- Schwesig, R.; Müller, K.; Becker, S.; Kreutzfeldt, A.; Hottenrott, K. Sensomotorisches Training im Alter und bei Osteoporose. Akt. Rheumatol. 2006, 31, 196–203. [Google Scholar] [CrossRef]
- Granacher, U.; Gollhofer, A.; Strass, D. Training induced adaptations in characteristics of postural reflexes in elderly men. Gait Posture 2006, 24, 459–466. [Google Scholar] [CrossRef]
- Korsten, K.; Mornieux, G.; Walter, N.; Gollhofer, A. Gibt es Alternativen zum Sensomotorischen Training? Schweiz. Z. Sportmed. Sporttraumatol. 2008, 56, 150–155. [Google Scholar]
- Granacher, U.; Gruber, M.; Gollhofer, A. Auswirkungen von Sensomotorischem Training auf die Posturale Kontrolle Älterer Mäner. Deut. Z. Sportmed. 2009, 60, 387–393. [Google Scholar]
- Giboin, L.S.; Gruber, M.; Kramer, A. Task-specificity of balance training. Hum. Mov. Sci. 2015, 44, 22–31. [Google Scholar] [CrossRef] [PubMed]
- Mikó, I.; Szerb, I.; Szerb, A.; Poor, G. Effectiveness of balance training programme in reducing the frequency of falling in estab-lished osteoporotic women: A randomized controlled trial. Clin. Rehabil. 2017, 31, 217–224. [Google Scholar] [CrossRef] [PubMed]
- Jafarzadeh, A.; Ehsani, F.; Yosephi, M.H.; Zoghi, M.; Jaberzadeh, S. Concurrent postural training and M1 anodal transcranial direct current stimulation improve postural impairment in patients with chronic low back pain. J. Clin. Neurosci. 2019, 68, 224–234. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Group | Body Height [m] | Age [Years] | Body Weight [kg] | BMI [kg/m]2 |
|---|---|---|---|---|
| PT | 1.68 ± 0.07 | 59.9 ± 10.7 | 81.7 ± 15.6 | 29.1 ± 5.34 |
| Galileo® | 1.70 ± 0.10 | 58.3 ± 11.6 | 79.6 ± 19.2 | 27.6 ± 5.42 |
| Posturomed® | 1.72 ± 0.12 | 62.0 ± 11.8 | 87.2 ± 15.9 | 29.5 ± 4.76 |
| p | 0.343 | 0.529 | 0.277 | 0.385 |
| ηp2 | 0.029 | 0.018 | 0.035 | 0.026 |
| Oswestry Disability Index | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Parameter | Physiotherapy Group | Galileo® Group | Posturomed® Group | Variance Analyses (ALM) | |||||||||||
| Pre-Score | Post-Score | d | Pre-Score | Post-Score | d | Pre-Score | Post-Score | d | Group | Time | Time × Group | ||||
| p | ηp2 | p | ηp2 | p | ηp2 | ||||||||||
| Pain intensity | 2.44 ± 0.65 | 1.60 ± 0.82 | 1.14 | 2.36 ± 0.76 | 1.80 ± 0.96 | 0.65 | 2.72 ± 0.68 | 1.40 ± 0.96 | 1.61 | 0.937 | 0.002 | <0.001 | 0.415 | 0.053 | 0.078 |
| Body care | 0.92 ± 0.95 | 0.44 ± 0.65 | 0.60 | 0.72 ± 0.74 | 0.52 ± 0.65 | 0.29 | 0.96 ± 0.98 | 0.44 ± 0.65 | 0.63 | 0.910 | 0.003 | <0.001 | 0.212 | 0.298 | 0.033 |
| Gait | 1.28 ± 1.17 | 0.88 ± 0.93 | 0.38 | 1.12 ± 0.83 | 0.76 ± 0.88 | 0.42 | 1.40 ± 1.12 | 1.08 ± 0.99 | 0.32 | 0.492 | 0.020 | 0.001 | 0.141 | 0.953 | 0.001 |
| Sedentary lifestyle | 2.28 ± 1.06 | 2.04 ± 1.17 | 0.21 | 2.04 ± 0.79 | 1.44 ± 1.04 | 0.65 | 2.48 ± 0.92 | 1.76 ± 0.97 | 0.76 | 0.161 | 0.050 | <0.001 | 0.199 | 0.259 | 0.037 |
| stand | 2.80 ± 0.87 | 2.00 ± 1.26 | 0.75 | 2.40 ± 1.04 | 1.60 ± 1.29 | 0.68 | 2.80 ± 1.12 | 2.00 ± 1.38 | 0.64 | 0.287 | 0.034 | <0.001 | 0.338 | 1.000 | 0.000 |
| sleep | 1.68 ± 1.03 | 1.20 ± 0.91 | 0.49 | 1.72 ± 1.02 | 1.40 ± 1.04 | 0.31 | 1.80 ± 0.91 | 1.04 ± 0.68 | 0.95 | 0.798 | 0.006 | <0.001 | 0.219 | 0.297 | 0.033 |
| Sexuality | 2.06 ± 2.08 | 1.69 ± 1.92 | 0.19 | 1.56 ± 1.50 | 0.88 ± 1.46 | 0.46 | 2.19 ± 1.63 | 1.33 ± 1.62 | 0.53 | 0.465 | 0.030 | <0.001 | 0.245 | 0.451 | 0.031 |
| Social life | 2.36 ± 1.25 | 1.64 ± 1.47 | 0.44 | 2.08 ± 1.22 | 1.20 ± 1.32 | 0.69 | 2.16 ± 1.14 | 1.24 ± 1.09 | 0.82 | 0.456 | 0.022 | <0.001 | 0.310 | 0.843 | 0.005 |
| Travel | 2.52 ± 1.33 | 1.40 ± 1.29 | 0.85 | 1.92 ± 1.58 | 1.08 ± 1.12 | 0.62 | 2.48 ± 1.39 | 1.76 ± 1.62 | 0.48 | 0.165 | 0.049 | <0.001 | 0.276 | 0.619 | 0.013 |
| Lifting | 2.76 ± 1.20 | 2.28 ± 1.49 | 0.36 | 1.96 ± 1.24 | 1.72 ± 1.40 | 0.18 | 2.80 ± 1.16 | 2.20 ± 1.53 | 0.45 | 0.084 | 0.066 | 0.002 | 0.128 | 0.545 | 0.017 |
| Sum | 22.3 ± 2.32 | 17.1 ± 8.57 | 0.95 | 17.3 ± 7.10 | 11.7 ± 7.72 | 0.76 | 21.8 ± 5.81 | 15.1 ± 8.27 | 0.95 | 0.086 | 0.094 | <0.001 | 0.470 | 0.763 | 0.011 |
| Posturography | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Parameter | Physiotherapy Group | Galileo® Group | Posturomed® Group | Variance Analyses (ALM) | |||||||||||
| Pre | Post | d | Pre | Post | d | Pre | Post | d | Group | Time | Time × Group | ||||
| p | ηp2 | p | ηp2 | p | ηp2 | ||||||||||
| F 1 | 19.4 ± 9.07 | 18.0 ± 6.59 | 0.17 | 17.7 ± 5.59 | 18.1 ± 5.49 | −0.08 | 18.4 ± 6.61 | 23.6 ± 25.6 | −0.33 | 0.467 | 0.021 | 0.426 | 0.009 | 0.315 | 0.032 |
| F 2–4 | 11.9 ± 3.99 | 10.3 ± 3.41 | 0.42 | 11.6 ± 3.64 | 10.8 ± 2.78 | 0.26 | 11.0 ± 5.15 | 10.1 ± 2.11 | 0.25 | 0.723 | 0.009 | 0.014 | 0.081 | 0.767 | 0.007 |
| F 5–6 | 5.63 ± 2.37 | 5.08 ± 2.30 | 0.24 | 5.29 ± 1.89 | 5.38 ± 1.85 | −0.05 | 4.80 ± 1.69 | 5.17 ± 1.92 | −0.20 | 0.748 | 0.008 | 0.844 | 0.001 | 0.050 | 0.080 |
| F 7–8 | 1.06 ± 0.55 | 1.04 ± 0.55 | 0.04 | 0.96 ± 0.44 | 1.02 ± 0.37 | −0.15 | 0.92 ± 0.37 | 1.07 ± 0.53 | −0.33 | 0.884 | 0.003 | 0.59 | 0.049 | 0.103 | 0.061 |
| ST | 31.2 ± 14.0 | 29.6 ± 15.2 | 0.11 | 30.2 ± 11.8 | 30.1 ± 10.1 | −0.01 | 27.7 ± 10.4 | 30.6 ± 12.6 | −0.26 | 0.927 | 0.002 | 0.666 | 0.003 | 0.109 | 0.060 |
| WDI | 6.27 ± 2.52 | 5.64 ± 2.34 | 0.26 | 5.67 ± 2.27 | 5.32 ± 2.04 | 0.16 | 5.06 ± 1.41 | 5.46 ± 1.75 | −0.25 | 0.424 | 0.024 | 0.341 | 0.013 | 0.103 | 0.061 |
| Synch. | 672 ± 155 | 636 ± 145 | 0.24 | 635 ± 128 | 634 ± 132 | 0.01 | 670 ± 139 | 644 ± 120 | 0.20 | 0.781 | 0.007 | 0.117 | 0.034 | 0.551 | 0.016 |
| Left | 49.6 ± 6.76 | 50.1 ± 4.19 | −0.09 | 51.5 ± 4.74 | 50.9 ± 3.88 | 0.13 | 50.5 ± 4.67 | 49.0 ± 5.48 | 0.30 | 0.468 | 0.021 | 0.226 | 0.020 | 0.174 | 0.047 |
| Heel | 47.9 ± 7.51 | 45.5 ± 7.20 | 0.32 | 47.4 ± 7.73 | 47.2 ± 8.22 | 0.02 | 46.7 ± 5.92 | 48.7 ± 7.35 | −0.30 | 0.886 | 0.003 | 0.781 | 0.001 | 0.014 | 0.111 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rüger, A.; Laudner, K.; Delank, K.-S.; Schwesig, R.; Steinmetz, A. Effects of Different Forms of Sensorimotor Training on Postural Control and Functional Status in Patients with Chronic Low Back Pain. J. Pers. Med. 2023, 13, 634. https://doi.org/10.3390/jpm13040634
Rüger A, Laudner K, Delank K-S, Schwesig R, Steinmetz A. Effects of Different Forms of Sensorimotor Training on Postural Control and Functional Status in Patients with Chronic Low Back Pain. Journal of Personalized Medicine. 2023; 13(4):634. https://doi.org/10.3390/jpm13040634
Chicago/Turabian StyleRüger, Alex, Kevin Laudner, Karl-Stefan Delank, René Schwesig, and Anke Steinmetz. 2023. "Effects of Different Forms of Sensorimotor Training on Postural Control and Functional Status in Patients with Chronic Low Back Pain" Journal of Personalized Medicine 13, no. 4: 634. https://doi.org/10.3390/jpm13040634