
Management of Patients Affected by Giant Cell Arteritis during the COVID-19 Pandemic: Telemedicine Protocol TELEMACOV

 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Population
2.2. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Buttgereit, F.; Dejaco, C.; Matteson, E.L.; Dasgupta, B. Polymyalgia rheumatica and giant cell arteritis: A systematic review. JAMA 2016, 315, 2442–2458. [Google Scholar] [CrossRef] [PubMed]
- Smeeth, L.; Cook, C.; Hall, A.J. Incidence of diagnosed polymyalgia rheumatica and temporal arteritis in the United Kingdom, 1990–2001. Ann. Rheum. Dis. 2006, 65, 1093–1098. [Google Scholar] [CrossRef] [PubMed]
- Dejaco, C.; Duftner, C.; Buttgereit, F.; Matteson, E.L.; Dasgupta, B. The spectrum of giant cell arteritis and polymyalgia rheumatica: Revisiting the concept of the disease. Rheumatology 2016, 56, 506–515. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hunder, G.G.; Arend, W.P.; Bloch, D.A.; Calabrese, L.H.; Fauci, A.S.; Fries, J.F.; Leavitt, R.Y.; Lie, J.T.; Lightfoot, R.W.; Masi, A.T.; et al. The American College of Rheumatology 1990 criteria for the classification of vasculitis. Introduction. Arthritis Rheum 1990, 33, 1065. [Google Scholar] [CrossRef] [PubMed]
- Chrysidis, S.; Duftner, C.; Dejaco, C.; Schäfer, V.S.; Ramiro, S.; Carrara, G.; Scirè, C.A.; Hocevar, A.; Diamantopoulos, A.P.; Iagnocco, A.; et al. Definitions and reliability assessment of elementary ultrasound lesions in giant cell arteritis: A study from the OMERACT Large Vessel Vasculitis Ultrasound Working Group. RMD Open 2018, 4, e000598. [Google Scholar] [CrossRef] [Green Version]
- Stone, J.H.; Tuckwell, K.; Dimonaco, S.; Klearman, M.; Aringer, M.; Blockmans, D.; Brouwer, E.; Cid, M.C.; Dasgupta, B.; Rech, J.; et al. Trial of Tocilizumab in Giant-Cell Arteritis. N. Engl. J. Med. 2017, 377, 317–328. [Google Scholar] [CrossRef]
- Villiger, P.M.; Adler, S.; Kuchen, S.; Wermelinger, F.; Dan, D.; Fiege, V.; Bütikofer, L.; Seitz, M.; Reichenbach, S. Tocilizumab for induction and maintenance of remission in giant cell arteritis: A phase 2, randomised, double-blind, placebocontrolled trial. Lancet 2016, 387, 1921–1927. [Google Scholar] [CrossRef]
- Dejaco, C.; Brouwer, E.; Mason, J.; Buttgereit, F.; Matteson, E.L.; Dasgupta, B. Giant cell arteritis and polymyalgia rheumatica: Current challenges and opportunities. Nat. Rev. Rheumatol. 2017, 13, 578–592. [Google Scholar] [CrossRef]
- Hellmich, B.; Agueda, A.; Monti, S.; Buttgereit, F.; de Boysson, H.; Brouwer, E.; Cassie, R.; Cid, M.C.; Dasgupta, B.; Dejaco, C.; et al. 2018 Update of the EULAR recommendations for the management of large vessel vasculitis. Ann. Rheum. Dis. 2020, 79, 19–30. [Google Scholar] [CrossRef] [Green Version]
- Ehlers, L.; Askling, J.; Bijlsma, H.W.J.; Cid, M.C.; Cutolo, M.; Dasgupta, B.; Dejaco, C.; Dixon, W.G.; Feltelius, N.; Finckh, A.; et al. EULAR recommendations for a core data set to support observational research and clinical care in giant cell arteritis. Ann. Rheum. Dis. 2019, 78, 1160–1166. [Google Scholar] [CrossRef] [Green Version]
- Consolidated Telemedicine Implementation Guide. Available online: https://www.who.int/publications/i/item/9789240059184 (accessed on 1 February 2020).
- Wagner, E.H.; Coleman, K.; Reid, R.J.; Phillips, K.; Abrams, M.K.; Sugarman, J.R. The Changes Involved in Patient-Centered Medical Home Transformation. Prim. Care 2012, 39, 241–259. [Google Scholar] [CrossRef]
- Wagner, E.H.; Coleman, K.; Reid, R.; Phillips, K.; Sugarman, J.R. Guiding Transformation: How Medical Practices Can Become Patient-Centered Medical Homes; The Commonwealth Fund: New York, NY, USA, 2012. [Google Scholar]
- Polinski, J.M.; Barker, T.; Gagliano, N.; Sussman, A.J.; Brennan, T.A.; Shrank, W.H. Patients’ Satisfaction with and Preference for Telehealth Visits. J. Gen. Intern. Med. 2015, 31, 269–275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thompson, K.; Kulkarni, J.; Sergejew, A.A. Reliability and validity of a new Medication Adherence Rating Scale (MARS) for the psychoses. Schizophr. Res. 2000, 42, 241–247. [Google Scholar] [CrossRef] [PubMed]
- Lam, W.Y.; Fresco, P. Medication Adherence Measures: An Overview. BioMed Res. Int. 2015, 2015, 217047. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Falter, M.; Scherrenberg, M.; Dendale, P. Digital Health in Cardiac Rehabilitation and Secondary Prevention: A Search for the Ideal Tool. Sensors 2020, 21, 12. [Google Scholar] [CrossRef] [PubMed]
- Zedda, A.; Gusai, E.; Caruso, M.; Bertuletti, S.; Baldazzi, G.; Spanu, S.; Riboni, D.; Pibiri, A.; Monticone, M.; Cereatti, A.; et al. DoMoMEA: A Home-Based Telerehabilitation System for Stroke Patients. In Proceedings of the 2020 42nd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Montreal, QC, Canada, 20–24 July 2020; Volume 2020, pp. 5773–5776. [Google Scholar] [CrossRef]
- Wali, S.; Margarido, M.G.; Shah, A.; Ware, P.; McDonald, M.; O’Sullivan, M.; Posada, J.D.; Ross, H.; Seto, E. Expanding Telemonitoring in a Virtual World: A Case Study of the Expansion of a Heart Failure Telemonitoring Program During the COVID-19 Pandemic. J. Med. Internet Res. 2021, 23, e26165. [Google Scholar] [CrossRef] [PubMed]
- Padwal, R.; Wood, P.W. Digital Health Approaches for the Assessment and Optimisation of Hypertension Care Provision. Can. J. Cardiol. 2020, 37, 711–721. [Google Scholar] [CrossRef]
- Mariania, S.; Hanke, J.S.; Dogan, G.; Schmittoa, J.D. Out of hospital management of LVAD patients during COVID-19 outbreak. Artif. Organs 2020, 44, 873–876. [Google Scholar] [CrossRef]
- Matheus, A.S.D.M.; Cabizuca, C.A.; Tannus, L.R.M.; Passos, A.C.; Schmidt, A.C.; de Gouveia, A.T.; Pessoa, B.M.D.A.; Matheus, F.C.; Yang, G.Y.-H.; Divino, J.A.D.S.; et al. Telemonitoring type 1 diabetes patients during the COVID-19 pandemic in Brazil: Was it useful? Arch. Endocrinol. Metab. 2020, 65, 105–111. [Google Scholar] [CrossRef]
- Zabeen, B.; Ahmed, B.; Nahar, J. Young people with type 1 diabetes on insulin pump therapy could fast safely during COVID–19 pandemic Ramadan: A telemonitoring experience in Bangladesh. J. Diabetes Investig. 2020, 12, 1060–1063. [Google Scholar] [CrossRef]
- Sajal, S.R.; Ehsan, T.; Vaidyanathan, R.; Wang, S.; Aziz, T.; Al Mamun, K.A. Telemonitoring Parkinson’s disease using machine learning by combining tremor and voice analysis. Brain Inform. 2020, 7, 12. [Google Scholar] [CrossRef]
- Pinto, S.; Quintarelli, S.; Silani, V. New technologies and Amyotrophic Lateral Sclerosis—Which step forward rushed by the COVID-19 pandemic? J. Neurol. Sci. 2020, 418, 117081. [Google Scholar] [CrossRef] [PubMed]
- Furlanis, G.; Ajčević, M.; Naccarato, M.; Caruso, P.; Scali, I.; Lugnan, C.; Stella, A.B.; Manganotti, P. e-Health vs COVID-19: Home patient telemonitoring to maintain TIA continuum of care. Neurol. Sci. 2020, 41, 2023–2024. [Google Scholar] [CrossRef] [PubMed]
- Mastronardi, M.; Curlo, M.; Polignano, M.; Vena, N.; Rossi, D.; Giannelli, G. Remote Monitoring Empowerment of Patients with IBDs during the SARS-CoV-2 Pandemic. Healthcare 2020, 8, 377. [Google Scholar] [CrossRef] [PubMed]
- Wallis, C.J.; Catto, J.W.; Finelli, A.; Glaser, A.W.; Gore, J.L.; Loeb, S.; Morgan, T.M.; Morgans, A.K.; Mottet, N.; Neal, R.; et al. The Impact of the COVID-19 Pandemic on Genitourinary Cancer Care: Re-envisioning the Future. Eur. Urol. 2020, 78, 731–742. [Google Scholar] [CrossRef] [PubMed]
- Peeters, M.; van Dam, P.; Rasschaert, M.A.; Vulsteke, C.; De Keersmaecker, S.; Croes, L.; Van Brussel, I.; Ravelingien, J.; Janssens, A.; Prenen, H. Prescreening for COVID-19 in patients receiving cancer treatment using a patient-reported outcome platform. ESMO Open 2020, 5, e000817. [Google Scholar] [CrossRef]
- Brunasso, A.M.G.; Massone, C. Teledermatologic monitoring for chronic cutaneous autoimmune diseases with smartworking during COVID-19 emergency in a tertiary center in Italy. Dermatol. Ther. 2020, 33, e13495. [Google Scholar] [CrossRef]
- Dourado, I.; Magno, L.; Soares, F.; Massa, P.; Nunn, A.; Dalal, S.; Grangeiro, A.; The Brazilian PrEP1519 Study Group. Adapting to the COVID-19 Pandemic: Continuing HIV Prevention Services for Adolescents Through Telemonitoring, Brazil. AIDS Behav. 2020, 24, 1994–1999. [Google Scholar] [CrossRef]
- Silven, A.V.; Petrus, A.H.J.; Villalobos-Quesada, M.; Dirikgil, E.; Oerlemans, C.R.; Landstra, C.P.; Boosman, H.; van Os, H.J.A.; Blanker, M.H.; Treskes, R.W.; et al. Telemonitoring for Patients With COVID-19: Recommendations for Design and Implementation. J. Med. Internet Res. 2020, 22, e20953. [Google Scholar] [CrossRef]
- Kavadichanda, C.; Shah, S.; Daber, A.; Bairwa, D.; Mathew, A.; Dunga, S.; Das, A.C.; Gopal, A.; Ravi, K.; Kar, S.S.; et al. Tele-rheumatology for overcoming socioeconomic barriers to healthcare in resource constrained settings: Lessons from COVID-19 pandemic. Rheumatology 2020, 60, 3369–3379. [Google Scholar] [CrossRef]
- Tornero-Molina, J.; Sánchez-Alonso, F.; Fernández-Prada, M.; Bris-Ochaita, M.-L.; Sifuentes-Giraldo, A.; Vidal-Fuentes, J. Telerreumatología en tiempos de crisis durante la pandemia por COVID-19. Reumatol. Clin. 2020, 18, 157–163. [Google Scholar] [CrossRef] [PubMed]
- Naveen, R.; Sundaram, T.G.; Agarwal, V.; Gupta, L. Teleconsultation experience with the idiopathic inflammatory myopathies: A prospective observational cohort study during the COVID-19 pandemic. Rheumatol. Int. 2020, 41, 67–76. [Google Scholar] [CrossRef] [PubMed]
- Azma, K.; Rezasoltani, Z.; Rezaeimoghaddam, F.; Dadarkhah, A.; Mohsenolhosseini, S. Efficacy of tele-rehabilitation compared with office-based physical therapy in patients with knee osteoarthritis: A randomized clinical trial. J. Telemed. Telecare 2017, 24, 560–565. [Google Scholar] [CrossRef] [PubMed]
- De Thurah, A.; Stengaard-Pedersen, K.; Axelsen, M.; Fredberg, U.; Schougaard, L.M.V.; Hjollund, N.H.I.; Pfeiffer-Jensen, M.; Laurberg, T.B.; Tarp, U.; Lomborg, K.; et al. Tele-Health Followup Strategy for Tight Control of Disease Activity in Rheumatoid Arthritis: Results of a Randomized Controlled Trial. Arthritis Rheum. 2017, 70, 353–360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parisi, S.; Ditto, M.C.; Finucci, A.; Fusaro, E. How to manage rheumatic patients during the coronavirus pandemic. Panminerva Med. 2020, 62, 176–177. [Google Scholar] [CrossRef]
- Zuccaro, V.; Celsa, C.; Sambo, M.; Battaglia, S.; Sacchi, P.; Biscarini, S.; Valsecchi, P.; Pieri, T.C.; Gallazzi, I.; Colaneri, M.; et al. Competing-risk analysis of coronavirus disease 2019 in-hospital mortality in a Northern Italian centre from SMAtteo COVID19 REgistry (SMACORE). Sci. Rep. 2021, 11, 1137. [Google Scholar] [CrossRef]
- Stone, J.H.; Tuckwell, K.; Dimonaco, S.; Klearman, M.; Aringer, M.; Blockmans, D.; Brouwer, E.; Cid, M.C.; Dasgupta, B.; Rech, J.; et al. Glucocorticoid Dosages and Acute-Phase Reactant Levels at Giant Cell Arteritis Flare in a Randomized Trial of Tocilizumab. Arthritis Rheumatol. 2019, 71, 1329–1338. [Google Scholar] [CrossRef] [Green Version]
- Conti, M.; Passarella, A.; Das, S.K. The Internet of People (IoP): A new wave in pervasive mobile computing. Pervasive Mob. Comput. 2017, 41, 1–27. [Google Scholar] [CrossRef]
- Jagadeeswari, V.; Vairavasundaram, S.; Logesh, R.; Vijayakumar, V. A study on medical Internet of Things and Big Data in personalized healthcare system. Health Inf. Sci. Syst. 2018, 6, 14. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Domain | New Onset or Description of Concomitant Symptoms | Laboratory Tests | PROs | Therapy | Satisfaction | Compliance to Therapy |
|---|---|---|---|---|---|---|
| Description |
|
|
|
| 0–5 Likert scale evaluating:
| Medication Adherence Rating Scale |
| Parameters | Time at Diagnosis | Pre-Lockdown | First Interview | Second Interview | Visit on Site |
|---|---|---|---|---|---|
| Patients treated with only GC (19 pts) | |||||
| Leukocytes/mm3 | 7330 (±930) | 6820 (±980) | 6700 (±910) | 7640 (±1110) | 8120 (±920) |
| Platelets × 103/mm3 | 291 (±125) | 324 (±111) | 320 (±135) | 330 (±102) | 325 (±105) |
| Creatinine mg/dL | 0.71 (±0.21) | 0.75 (±0.19) | 0.73 (±0.21) | 0.71 (±0.24) | 0.74 (±0.20) |
| ALT U/L | 24.41 (±7.16) | 22.10 (±9.20) | 23.80 (±9.32) | 26.22 (±7.88) | 23.7 (±6.30) |
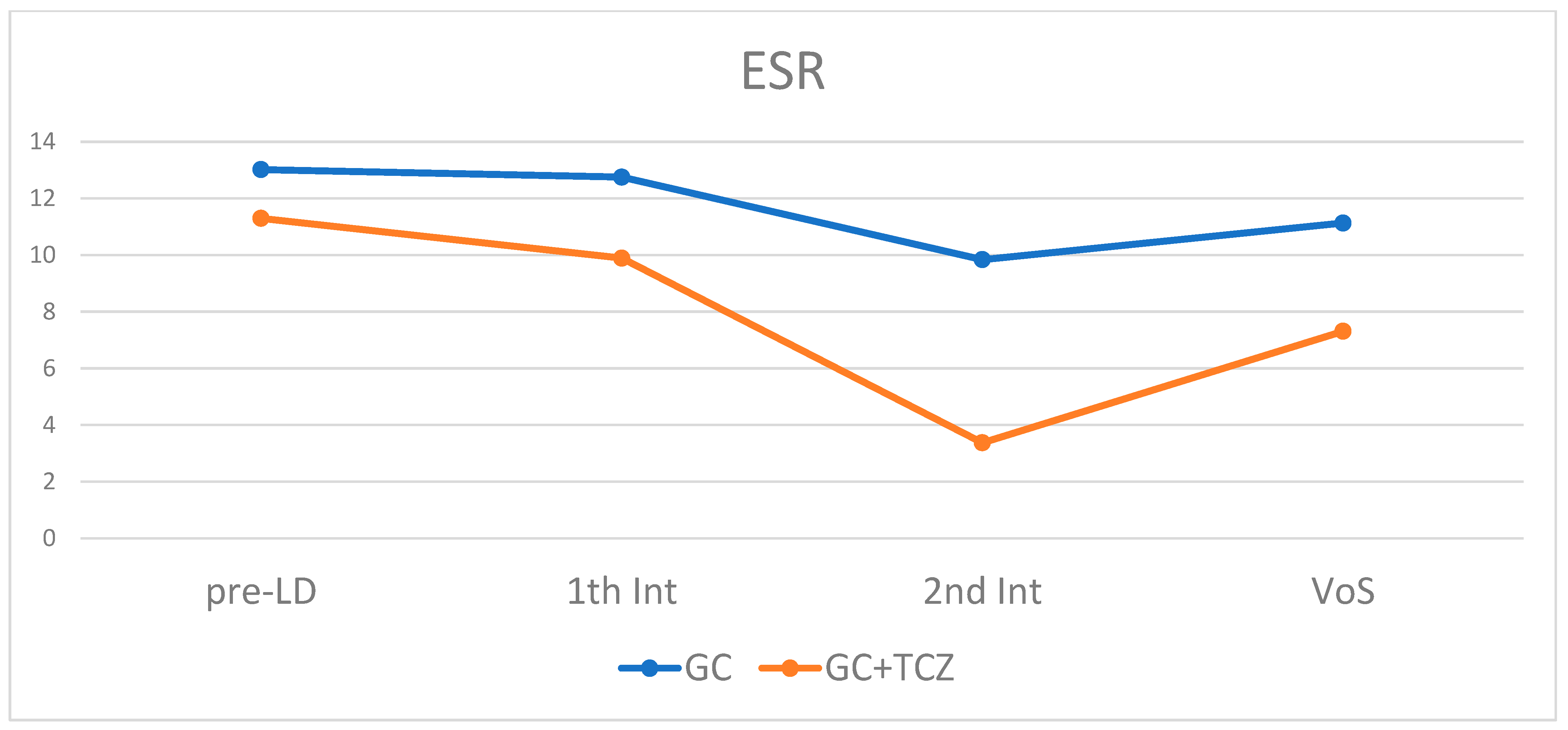
| ESR (mean ± SD) | 74.08 (±23.95) | 13.02 (±8.2) | 12.75 (±6.42) | 9.84 (±6.63) | 11.13 (±7.45) |
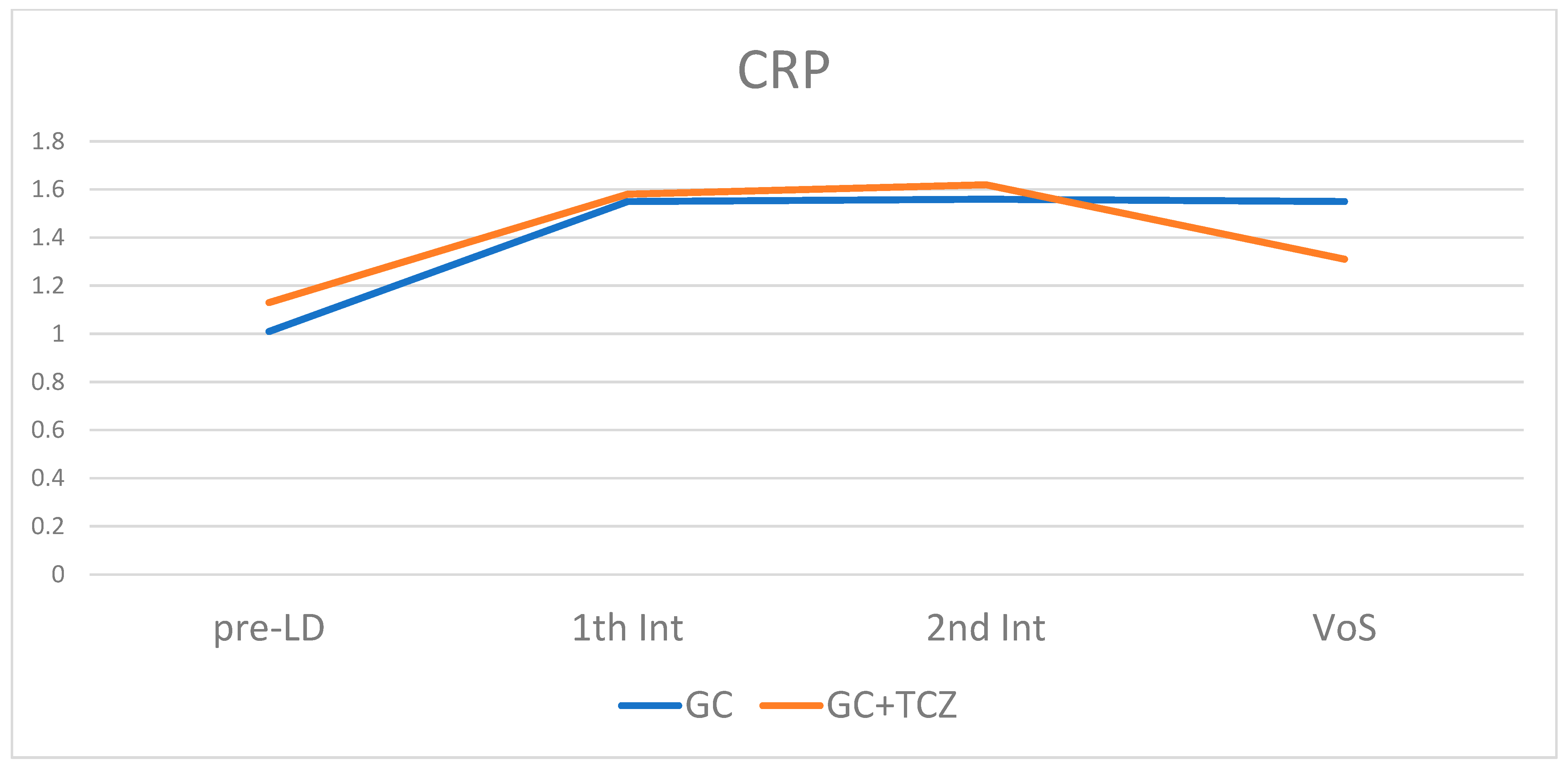
| CRP mg/L (mean ± SD) | 47.4 (±42.2) | 1.01 (±1.1) | 1.55 (±2.29) | 1.5 (±2.24) | 1.55 (±2.05) |
| Hgb mg/dL (mean ± SD) | 11.6 (±2.6) | 13.2 (±2.24) | 12.75 (±3.19) | 13.58 (±2.12) | 13.74 (±0.55) |
| PGA (1–10) median (IQR) | 8.5 (8–9) | 3.5 (1–8) | 3.5 (±1–7) | 2 (1.5–8) | 2 (1.25–4) |
| EGA (1–10) median (IQR) | 7 (6.25–9) | 2.5 (1–6) | 3.5 (0.75–7) | 2 (1–7) | 1.5 (1.25–3) |
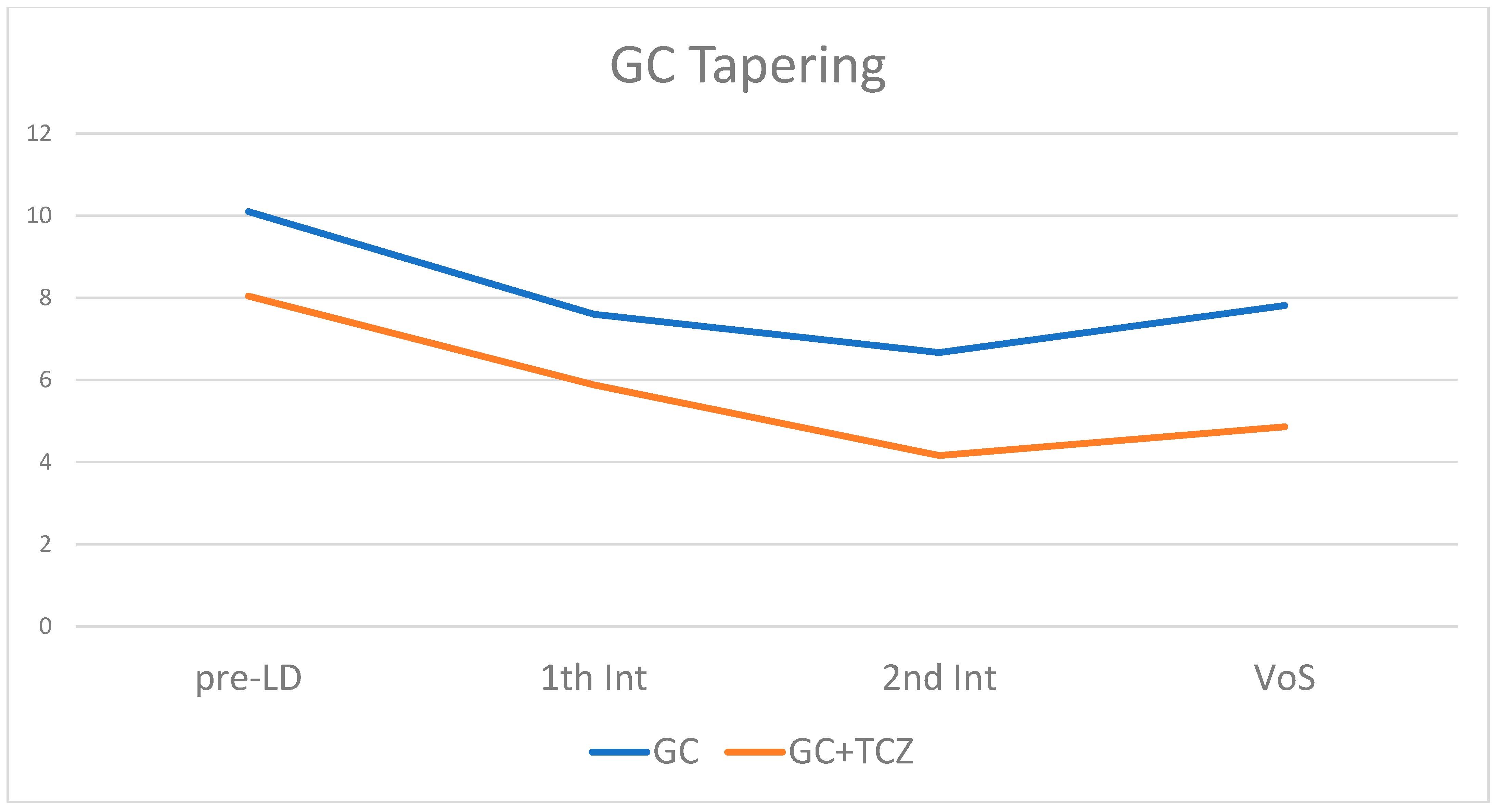
| GC (PDN) mg (mean ± SD) | 52.72 (±18.3) | 10.1 (±6.95) | 7.6 (±4.51) | 6.67 (±3.1) | 7.81 (±4.32) |
| Patients treated with GC and TCZ (18 pt) | |||||
| Leukocytes/mm3 | 6330 (±820) | 7120 (±730) | 6600 (±1115) | 7354 (±1003) | 7120 (±720) |
| Platelets × 103/mm3 | 361 (±135) | 313 (±121) | 330 (±145) | 310 (±98) | 315 (±109) |
| Creatinine mg/dL | 0.74 (±0.22) | 0.74 (±0.19) | 0.81 (±0.31) | 0.79 (±0.23) | 0.76 (±0.30) |
| ALT U/L | 25.11 (±6.22) | 23.10 (±9.20) | 24.82 (±8.18) | 24.33 (±7.89) | 25.51 (±5.20) |
| ESR (mean ± SD) | 74.56 (±36.58) | 11.3 (±3.85) | 9.89 (±4.71) | 3.37 (±4.4) | 7.31 (±6.74) |
| CRP mg/L (mean ± SD) | 47.8 (±41.7) | 1.13 (±0.65) | 1.58 (±0.85) | 1.62 (±0.73) | 1.31 (±1.95) |
| Hgb mg/dL (mean ± SD) | 11.36 (±3.88) | 12.98 (±4.91) | 12.43 (±4.3) | 13.25 (±5.15) | 14.00 (±0.39) |
| PGA (1–10) median (IQR) | 10 (6–10) | 1 (1–7) | 2 (1–4) | 3 (1–4) | 2 (1–3) |
| EGA (1–10) median (IQR) | 9 (6–9) | 1 (1–5) | 1 (0.5–3) | 3 (1–4) | 2 (0–2) |
| GC (PDN) mg (mean ± SD) | 51.76 (±18.85) | 8.04 (±4.38) | 5.88 (±3.92) | 4.16 (±4.32) | 4.46 (±3.56) |
| Group of Patients | Pre-Lockdown | First Interview | Second Interview | Visit on Site |
|---|---|---|---|---|
| Overall, median (IQR) | 8 | 7 | 8 | 7 |
| (6–9) | (6–9) | (6–9) | (6–9) | |
| GC alone, median (IQR) | 7 | 7 | 8 | 7 |
| (6–9) | (6–9) | (6–9) | (6–9) | |
| GC+TCZ, median (IQR) | 8 | 8 | 8 | 7.5 |
| (6–9) | (7–9) | (7–9) | (6–9) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Parisi, S.; Ditto, M.C.; Talotta, R.; Laganà, A.; Peroni, C.L.; Fusaro, E. Management of Patients Affected by Giant Cell Arteritis during the COVID-19 Pandemic: Telemedicine Protocol TELEMACOV. J. Pers. Med. 2023, 13, 620. https://doi.org/10.3390/jpm13040620
Parisi S, Ditto MC, Talotta R, Laganà A, Peroni CL, Fusaro E. Management of Patients Affected by Giant Cell Arteritis during the COVID-19 Pandemic: Telemedicine Protocol TELEMACOV. Journal of Personalized Medicine. 2023; 13(4):620. https://doi.org/10.3390/jpm13040620
Chicago/Turabian StyleParisi, Simone, Maria Chiara Ditto, Rossella Talotta, Angela Laganà, Clara Lisa Peroni, and Enrico Fusaro. 2023. "Management of Patients Affected by Giant Cell Arteritis during the COVID-19 Pandemic: Telemedicine Protocol TELEMACOV" Journal of Personalized Medicine 13, no. 4: 620. https://doi.org/10.3390/jpm13040620