
Early Postoperative Recovery after Modified Ultra-Minimally Invasive Sonography-Guided Thread Carpal Tunnel Release
 , and
, and {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. General Introduction
2.2. Surgical Method
2.2.1. Surgical Equipment
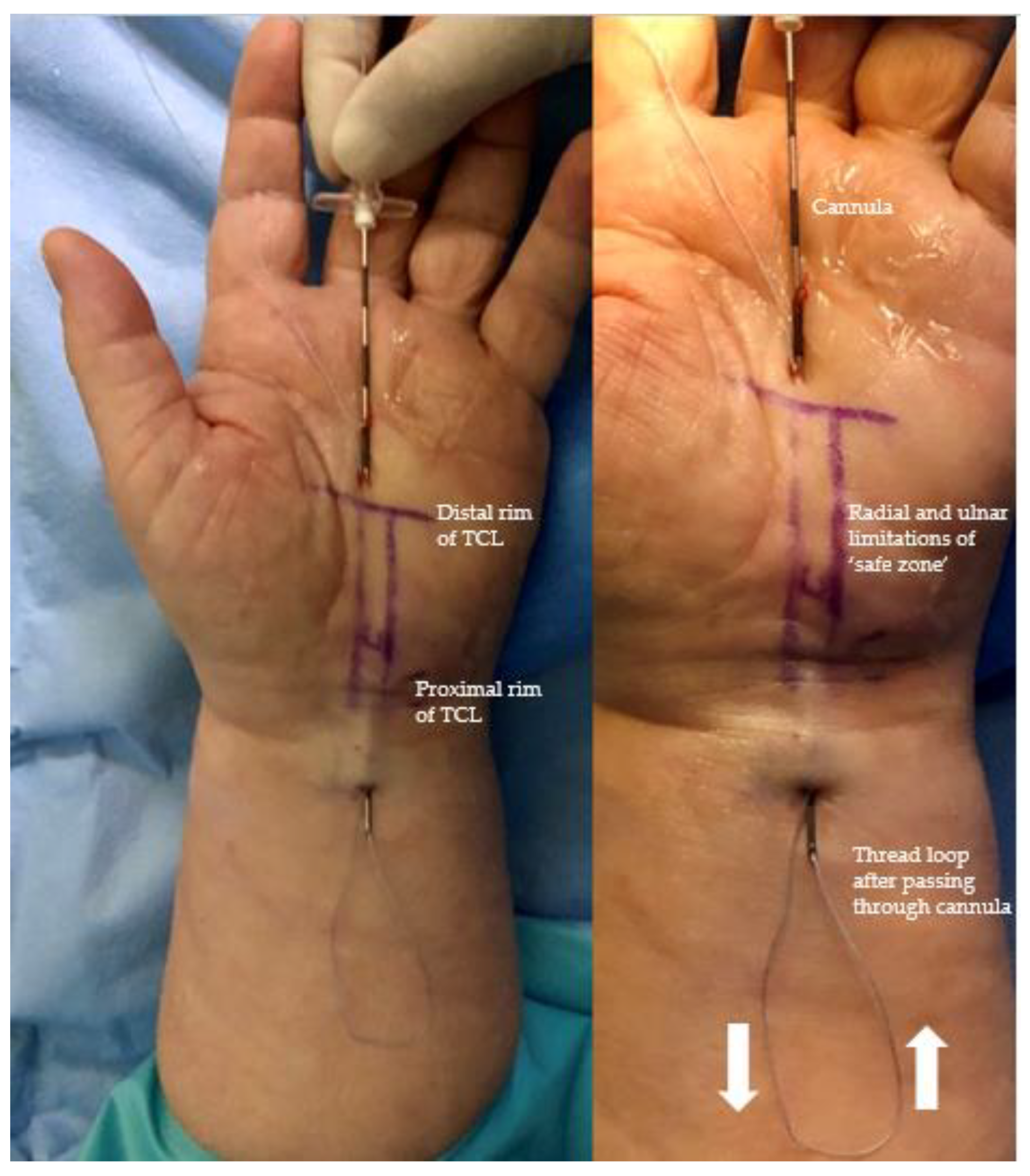
2.2.2. Surgical Procedure
2.3. Statistical Analysis
3. Results
3.1. Demographic Data
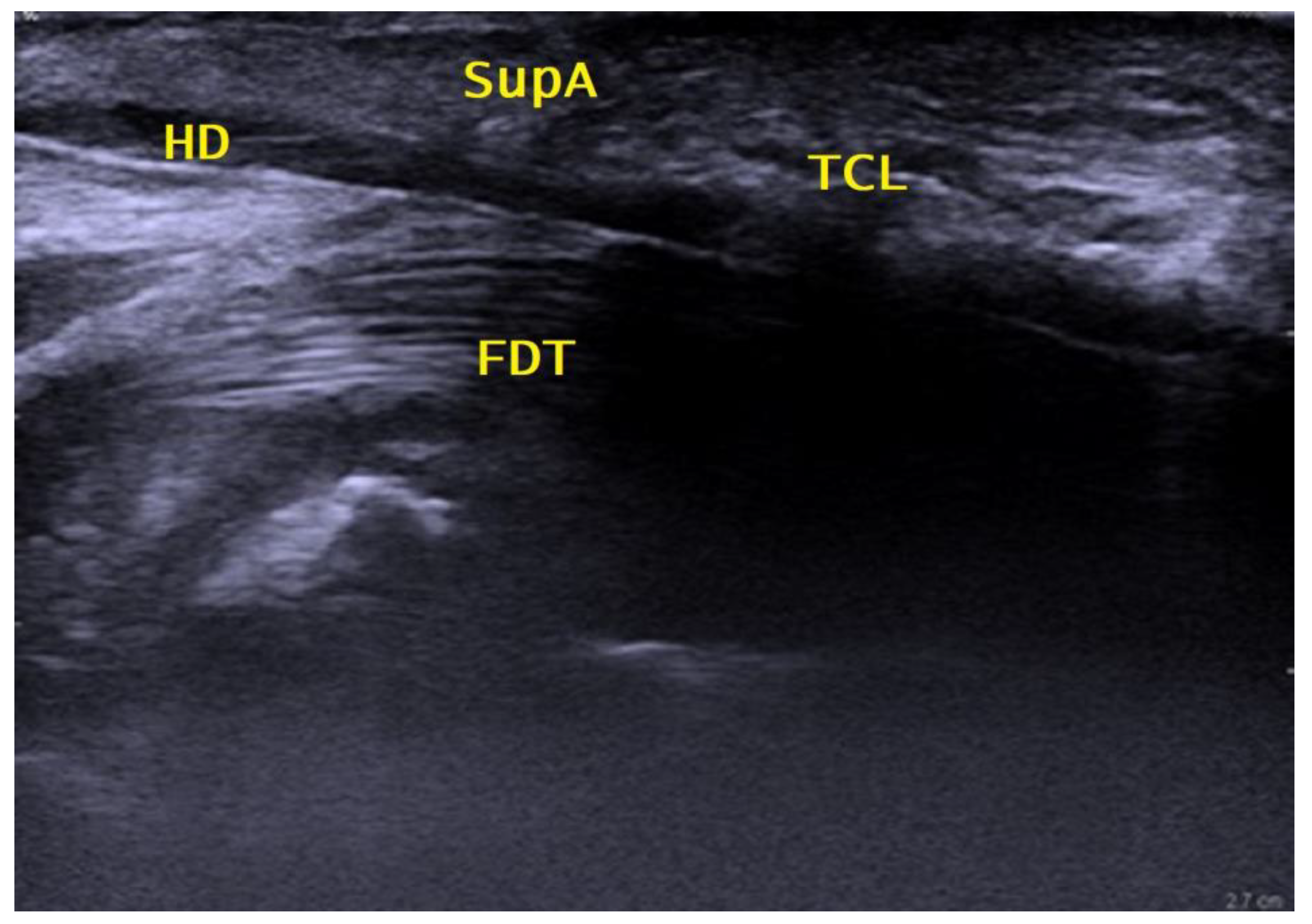
3.2. Ultrasonographic Investigation
3.3. Operating Time and Complications
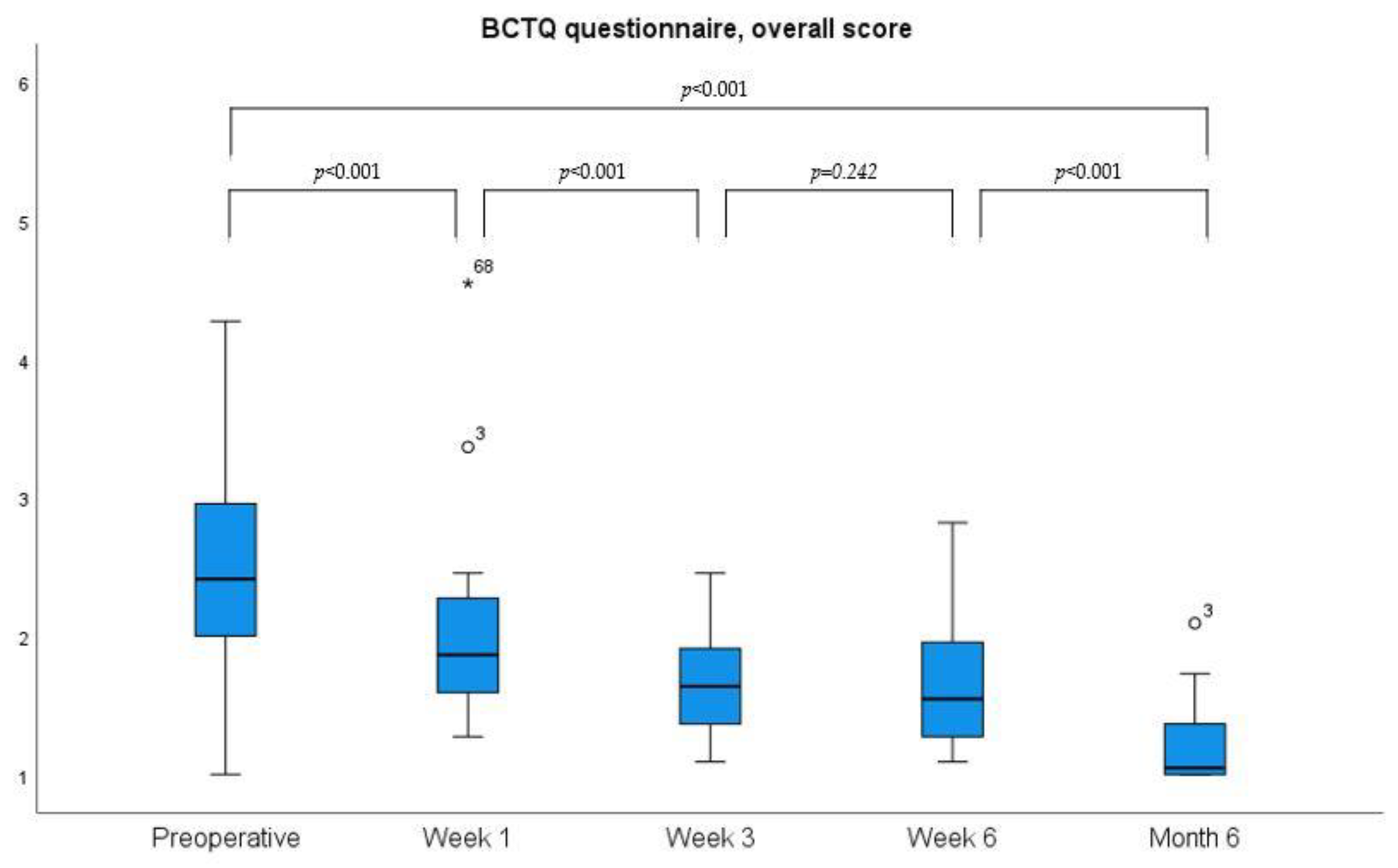
3.4. Grip Strength and PROMs
3.5. Return to Daily Activities, Work, and Satisfaction
4. Discussion
4.1. Safety
4.2. Reoperations for Incomplete Ligament Division
4.3. Postoperative Recovery
4.4. Objective Outcomes and PROMs
4.5. Comparison with UMIUCTR Using a Hook Knife
4.6. Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Scholten, R.J.; van der Molen, A.M.; Uitdehaag, B.M.; Bouter, L.M.; de Vet, H.C. Surgical treatment options for carpal tunnel syndrome. Cochrane Database Syst. Rev. 2007, 2007, Cd003905. [Google Scholar] [CrossRef] [Green Version]
- Aroori, S.; Spence, R.A. Carpal tunnel syndrome. Ulster Med. J. 2008, 77, 6–17. [Google Scholar] [PubMed]
- Bongers, F.J.; Schellevis, F.G.; van den Bosch, W.J.; van der Zee, J. Carpal tunnel syndrome in general practice (1987 and 2001): Incidence and the role of occupational and non-occupational factors. Br. J. Gen. Pract. 2007, 57, 36–39. [Google Scholar] [PubMed]
- Latinovic, R.; Gulliford, M.C.; Hughes, R.A. Incidence of common compressive neuropathies in primary care. J. Neurol. Neurosurg. Psychiatry 2006, 77, 263–265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salaffi, F.; De Angelis, R.; Grassi, W. Prevalence of musculoskeletal conditions in an Italian population sample: Results of a regional community-based study. I. The MAPPING study. Clin. Exp. Rheumatol. 2005, 23, 819–828. [Google Scholar] [PubMed]
- Petrover, D.; Richette, P. Treatment of carpal tunnel syndrome: From ultrasonography to ultrasound guided carpal tunnel release. Jt. Bone Spine 2018, 85, 545–552. [Google Scholar] [CrossRef]
- Karjalainen, T.V.; Lusa, V.; Page, M.J.; O’Connor, D.; Massy-Westropp, N.; Peters, S.E. Splinting for carpal tunnel syndrome. Cochrane Database Syst. Rev. 2023, 2, Cd010003. [Google Scholar]
- Ablove, R.H.; Peimer, C.A.; Diao, E.; Oliverio, R.; Kuhn, J.P. Morphologic changes following endoscopic and two-portal subcutaneous carpal tunnel release. J. Hand Surg. Am. 1994, 19, 821–826. [Google Scholar] [CrossRef]
- Okutsu, I.; Ninomiya, S.; Hamanaka, I.; Kuroshima, N.; Inanami, H. Measurement of pressure in the carpal canal before and after endoscopic management of carpal tunnel syndrome. J. Bone Jt. Surg. Am. 1989, 71, 679–683. [Google Scholar] [CrossRef]
- Wong, K.C.; Hung, L.K.; Ho, P.C.; Wong, J.M. Carpal tunnel release. A prospective, randomised study of endoscopic versus limited-open methods. J. Bone Jt. Surg. Br. 2003, 85, 863–868. [Google Scholar] [CrossRef] [Green Version]
- Bromley, G.S. Minimal-incision open carpal tunnel decompression. J. Hand Surg. Am. 1994, 19, 119–120. [Google Scholar] [CrossRef] [PubMed]
- Worseg, A.P.; Kuzbari, R.; Korak, K.; Höcker, K.; Wiederer, C.; Tschabitscher, M.; Holle, J. Endoscopic carpal tunnel release using a single-portal system. Br. J. Plast. Surg. 1996, 49, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Trumble, T.E.; Diao, E.; Abrams, R.A.; Gilbert-Anderson, M.M. Single-portal endoscopic carpal tunnel release compared with open release: A prospective, randomized trial. J. Bone Jt. Surg. Am. 2002, 84, 1107–1115. [Google Scholar] [CrossRef]
- Guo, D.; Tang, Y.; Ji, Y.; Sun, T.; Guo, J.; Guo, D. A non-scalpel technique for minimally invasive surgery: Percutaneously looped thread transection of the transverse carpal ligament. Hand 2015, 10, 40–48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakamichi, K.; Tachibana, S. Ultrasonographically assisted carpal tunnel release. J. Hand Surg. Am. 1997, 22, 853–862. [Google Scholar] [CrossRef]
- Guo, D.; Guo, D.; Guo, J.; Schmidt, S.C.; Lytie, R.M. A Clinical Study of the Modified Thread Carpal Tunnel Release. Hand 2017, 12, 453–460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Asserson, D.B.; North, T.J.; Rhee, P.C.; Bishop, A.T.; Brault, J.S.; Shin, A.Y. Return to work following ultrasound guided thread carpal tunnel release versus open carpal tunnel release: A comparative study. J. Hand Surg. Eur. Vol. 2022, 47, 359–363. [Google Scholar] [CrossRef]
- Burnham, R.S.; Loh, E.Y.; Rambaransingh, B.; Roberts, S.L.; Agur, A.M.; Playfair, L.D. A Controlled Trial Evaluating the Safety and Effectiveness of Ultrasound-Guided Looped Thread Carpal Tunnel Release. Hand 2021, 16, 73–80. [Google Scholar] [CrossRef]
- Tang, J.B.; Giddins, G. Why and how to report surgeons’ levels of expertise. J. Hand Surg. Eur. Vol. 2016, 41, 365–366. [Google Scholar] [CrossRef] [Green Version]
- Benson, L.S.; Bare, A.A.; Nagle, D.J.; Harder, V.S.; Williams, C.S.; Visotsky, J.L. Complications of endoscopic and open carpal tunnel release. Arthroscopy 2006, 22, 919–924.e2. [Google Scholar] [CrossRef]
- Leite, J.C.; Jerosch-Herold, C.; Song, F. A systematic review of the psychometric properties of the Boston Carpal Tunnel Questionnaire. BMC Musculoskelet Disord. 2006, 7, 78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Franchignoni, F.; Vercelli, S.; Giordano, A.; Sartorio, F.; Bravini, E.; Ferriero, G. Minimal clinically important difference of the disabilities of the arm, shoulder and hand outcome measure (DASH) and its shortened version (QuickDASH). J. Orthop. Sport. Phys. Ther. 2014, 44, 30–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Multanen, J.; Ylinen, J.; Karjalainen, T.; Ikonen, J.; Häkkinen, A.; Repo, J.P. Structural validity of the Boston Carpal Tunnel Questionnaire and its short version, the 6-Item CTS symptoms scale: A Rasch analysis one year after surgery. BMC Musculoskelet Disord. 2020, 21, 609. [Google Scholar] [CrossRef]
- Offenbaecher, M.; Ewert, T.; Sangha, O.; Stucki, G. Validation of a German version of the disabilities of arm, shoulder, and hand questionnaire (DASH-G). J. Rheumatol. 2002, 29, 401–402. [Google Scholar] [PubMed]
- Rojo-Manaute, J.M.; Capa-Grasa, A.; Rodríguez-Maruri, G.E.; Moran, L.M.; Martínez, M.V.; Martín, J.V. Ultra-minimally invasive sonographically guided carpal tunnel release: Anatomic study of a new technique. J. Ultrasound Med. 2013, 32, 131–142. [Google Scholar] [CrossRef] [PubMed]
- Jerosch-Herold, C.; Shepstone, L.; Miller, L.; Chapman, P. The responsiveness of sensibility and strength tests in patients undergoing carpal tunnel decompression. BMC Musculoskelet Disord. 2011, 12, 244. [Google Scholar] [CrossRef]
- Brunetti, S.; Petri, G.J.; Lucchina, S.; Garavaglia, G.; Fusetti, C. Should aspirin be stopped before carpal tunnel surgery? A prospective study. World J. Orthop. 2013, 4, 299–302. [Google Scholar] [CrossRef]
- Wessel, L.E.; Gu, A.; Asadourian, P.A.; Stepan, J.G.; Fufa, D.T.; Osei, D.A. The Epidemiology of Carpal Tunnel Revision over a 1-Year Follow-Up Period. J. Hand Surg. Am. 2021, 46, 758–764. [Google Scholar] [CrossRef]
- Lane, J.C.; Craig, R.S.; Rees, J.L.; Gardiner, M.D.; Green, J.; Prieto-Alhambra, D.; Furniss, D. Serious postoperative complications and reoperation after carpal tunnel decompression surgery in England: A nationwide cohort analysis. Lancet Rheumatol. 2020, 3, 49–57. [Google Scholar] [CrossRef] [PubMed]
- Moungondo, F.; Feipel, V. Percutaneous Sonographically Guided Release of Carpal Tunnel and Trigger Finger: Biomechanics, Clinical Results, Technical Developments. Hand Clin. 2022, 38, 91–100. [Google Scholar] [CrossRef]
- Rojo-Manaute, J.M.; Capa-Grasa, A.; Chana-Rodríguez, F.; Perez-Mañanes, R.; Rodriguez-Maruri, G.; Sanz-Ruiz, P.; Muñoz-Ledesma, J.; Aburto-Bernardo, M.; Esparragoza-Cabrera, L.; Cerro-Gutiérrez, M.D.; et al. Ultra-Minimally Invasive Ultrasound-Guided Carpal Tunnel Release: A Randomized Clinical Trial. J. Ultrasound Med. 2016, 35, 1149–1157. [Google Scholar] [CrossRef] [PubMed]






Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mende, K.; Kamphuis, S.J.M.; Schmid, V.; Schaefer, D.J.; Kaempfen, A.; Gohritz, A. Early Postoperative Recovery after Modified Ultra-Minimally Invasive Sonography-Guided Thread Carpal Tunnel Release. J. Pers. Med. 2023, 13, 610. https://doi.org/10.3390/jpm13040610
Mende K, Kamphuis SJM, Schmid V, Schaefer DJ, Kaempfen A, Gohritz A. Early Postoperative Recovery after Modified Ultra-Minimally Invasive Sonography-Guided Thread Carpal Tunnel Release. Journal of Personalized Medicine. 2023; 13(4):610. https://doi.org/10.3390/jpm13040610
Chicago/Turabian StyleMende, Konrad, Saskia J. M. Kamphuis, Valentin Schmid, Dirk J. Schaefer, Alexandre Kaempfen, and Andreas Gohritz. 2023. "Early Postoperative Recovery after Modified Ultra-Minimally Invasive Sonography-Guided Thread Carpal Tunnel Release" Journal of Personalized Medicine 13, no. 4: 610. https://doi.org/10.3390/jpm13040610