
A Multi-Institutional Informed Consent Proposal as a Prevention Tool for Combined Oral Contraceptive Intake and Thrombotic Risk
 , , , , , ,
, , , , , ,  , , ,
, , ,  ,
,  , , and
, , and {kind=link}
{kind=link}
Abstract
:1. Introduction
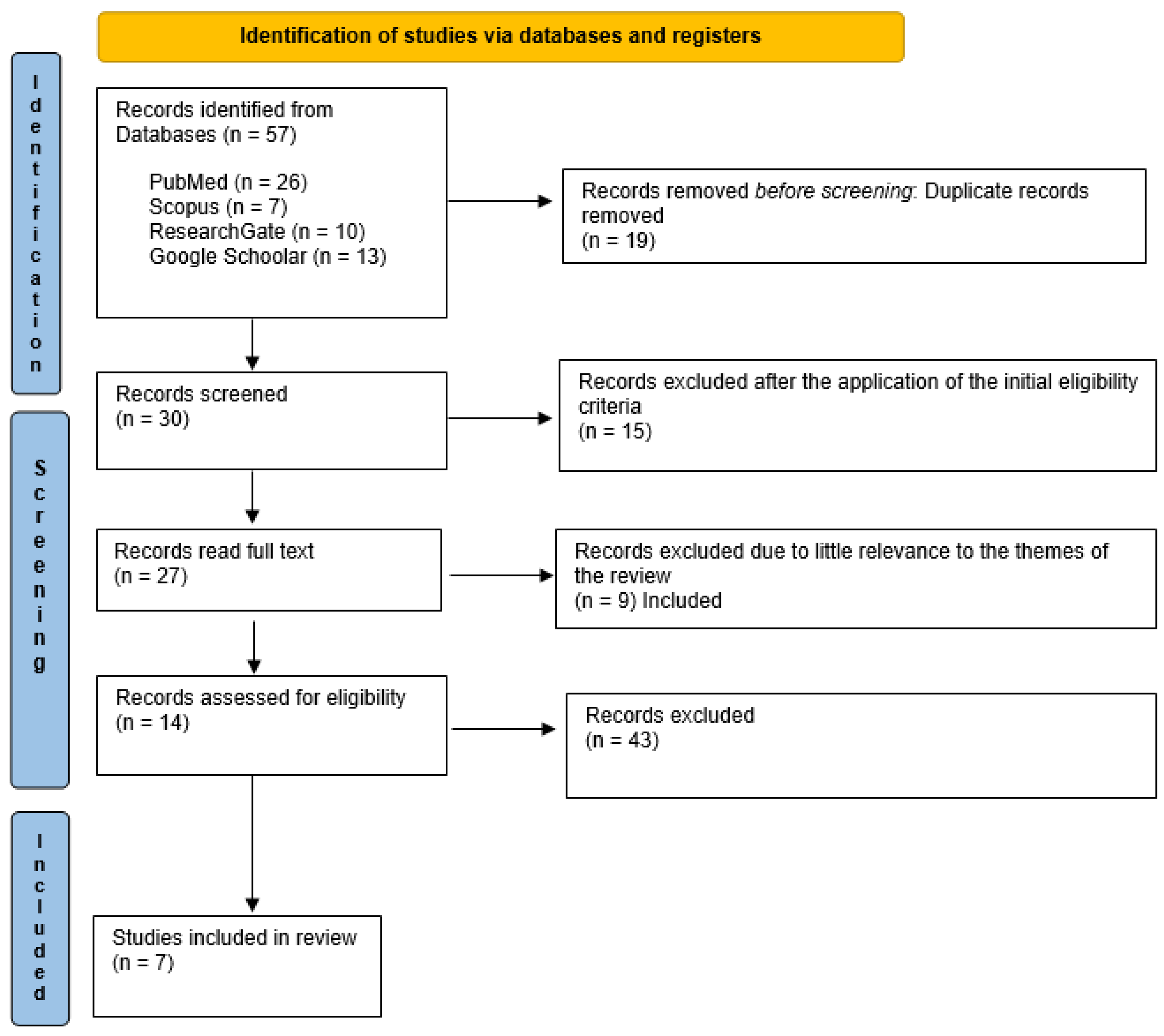
2. Materials and Methods
3. Results
The Informed Consent for Combined Oral Contraceptive: Our Proposal
- (I)
- How to take It: The use of COC from the first day of the menstrual cycle, guarantees an intermediate efficacy. If one wants to start taking COC at any time of the cycle, it is recommended to use an additional contraception for 7 days and only with pills containing estradiol valerate (EV) +dienogest (DNG) in the formulation 26 + 2, for 9 days.
- (II)
- Warnings: The first week of contraceptive use, either combined estrogen-progestin oral contraceptive pills (OCPs) or progestogen-only pills (POPs), inhibits ovulation. Delays or forgetting to take pills greatly increase the chances of pregnancy in the first week of the package. The allowed admission time is 12 h; after 24 h, it is advisable to take two tablets together. Risk of inefficiency in case of vomiting within 3 h or excessive diarrhea after 4–6 h of consumption. First clinical examination within 12 months of starting treatment, blood pressure control within six months of starting treatment. COC use should be discontinued 4 weeks before major surgery.
- (III)
- Side effects: The COC is associated with an increased risk of VTE, but it should be considered that in most women, the benefits associated with using COC far outweigh the risk of serious side effects. There is the possibility of water retention, which may cause a weight increase of no more than 2 kg completely reversible upon the suspension of the method. However, the available literature does not identify the effect of COC on weight. Sensations of heavy legs, headache during taking or pause, mastodynia, nausea, rare vomiting, or changes in sexual desire may occur. Most side effects are reduced from the second cycle, often resolving spontaneously within 5 months. Occasional bleeding may occur. Have a specialized medical assessment for side effects from any entity. Please note: COC causes an increased risk of venous and arterial thrombosis ranging from 5 to 12 per 10,000 women each year depending on the type of COC taken. Therefore, it is recommended to alert the doctor and to go to the emergency department if there are signs or symptoms attributable to this event (swollen arms or ankles, legs tingling, lower extremity edema, erythromelalgia, dyspnea, etc.). In this regard, it is recommended to periodically reassess individual risk factors, such as age, tobacco use, obesity, etc.
- (IV)
- Symptoms Or Diagnoses Requiring Clinical Assessment During COC.
- (a)
- Urgent action: chest pain, shortness of breath, hemoptysis, pain in one leg (usually the calf or inner thigh), swelling in the leg or arm, numbness or weakness on one side of the body, sudden change in your mental state.
- (b)
- Outpatient care: breast node, secretion from the nipple, nipple inversion, changes in the breast skin; new onset migraine, new sensory or motor symptoms in the hour preceding the onset of migraine; persistent atypical vaginal bleeding; arterial hypertension, increase in BMI >35 kg/m2, migraine or migraine with aura, deep venous thrombosis or pulmonary embolism, blood clotting abnormality, antiphospholipid antibodies positivity; angina, heart attack, stroke or peripheral vascular disease, atrial fibrillation, cardiomyopathy; mutation of the gene BRCA1-2 or breast cancer, liver tumor, gallbladder calculus.
- (V)
- Extracontraceptive Benefits: Hormonal contraception has a protective effect on genital integrity and fertility, resulting in an overall benefit in terms of reproductive health. Reduction of dysmenorrhea and heavy menstrual bleeding, menstrual headaches, hyperandrogenic symptoms, endometriosis, ectopic pregnancy, prevention of ovarian, and endometrial and colon cancers.
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- McLure, Z. Failure rates of contraceptive methods. Fam. Plan. Inf. Serv. 1981, 1, 59–61. [Google Scholar]
- Fu, H.; Darroch, J.E.; Haas, T.; Ranjit, N. Contraceptive failure rates: New estimates from the 1995 National Survey of Family Growth. Fam. Plan. Perspect. 1999, 31, 56–63. [Google Scholar] [CrossRef]
- Christin-Maitre, S. Worldwide contraception. Med. Sci. 2022, 38, 457–463. [Google Scholar] [CrossRef]
- United Nations Department of Economic; Social Affairs/Population Division. World Population Ageing; United Nations Department of Economic and Social Affairs: New York, NY, USA, 2015. [Google Scholar]
- United Nations Department of Economic; Social Affairs/Population Division. Contraceptive Use by Method 2019: Data Booklet (ST/ESA/SER. A/435); United Nations Department of Economic and Social Affairs: New York, NY, USA, 2019. [Google Scholar]
- DI Carlo, C.; Abbondanza, M.; Agnello, A.; Cavalli, G.; Driul, L.; Petriglia, M.; Tinelli, A.; Tirelli, A.; Tusei, A.; Grandi, G. Current and future hormonal contraception in Italy: Results from an Italian consensus expert meeting. Minerva Obstet. Gynecol. 2021, 73, 614–620. [Google Scholar] [CrossRef]
- Vimercati, A.; Dellino, M.; Suma, C.; Damiani, G.R.; Malvasi, A.; Cazzato, G.; Cascardi, E.; Resta, L.; Cicinelli, E. Spontaneous Uterine Rupture and Adenomyosis, a Rare but Possible Correlation: Case Report and Literature Review. Diagnostics 2022, 12, 1574. [Google Scholar] [CrossRef] [PubMed]
- Schindler, A.E. Non-contraceptive benefits of oral hormonal contraceptives. Int. J. Endocrinol. Metab. 2013, 11, 41–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dellino, M.; Silvestris, E.; Loizzi, V.; Paradiso, A.; Loiacono, R.; Minoia, C.; Daniele, A.; Cormio, G. Germinal ovarian tumors in reproductive age women: Fertility-sparing and outcome. Medicine 2020, 99, e22146. [Google Scholar] [CrossRef]
- Cascardi, E.; Cazzato, G.; Daniele, A.; Silvestris, E.; Cormio, G.; Di Vagno, G.; Malvasi, A.; Loizzi, V.; Scacco, S.; Pinto, V. Association between Cervical Microbiota and HPV: Could This Be the Key to Complete Cervical Cancer Eradication? Biology 2022, 11, 1114. [Google Scholar] [CrossRef]
- Morimont, L.; Haguet, H.; Dogne, J.M.; Gaspard, U.; Douxfils, J. Combined Oral Contraceptives and Venous Thromboembolism: Review and Perspective to Mitigate the Risk. Front. Endocrinol. 2021, 12, 769187. [Google Scholar] [CrossRef]
- Practice Committee of the American Society for Reproductive Medicine; American Society for Reproductive Medicine. Combined hormonal contraception and the risk of venous thromboembolism: A guideline. Fertil. Steril. 2017, 107, 43–51. [Google Scholar] [CrossRef] [Green Version]
- Buonomo, B.; Massarotti, C.; Dellino, M.; Anserini, P.; Ferrari, A.; Campanella, M.; Magnotti, M.; De Stefano, C.; Peccatori, F.A.; Lambertini, M. Reproductive issues in carriers of germline pathogenic variants in the BRCA1/2 genes: An expert meeting. BMC Med. 2021, 19, 205. [Google Scholar] [CrossRef] [PubMed]
- Lidegaard, Ø.; Milsom, I.; Geirsson, R.T.; Skjeldestad, F.E. Hormonal contraception and venous thromboembolism. Acta Obstet. Gynecol. Scand. 2012, 91, 769–778. [Google Scholar] [CrossRef] [PubMed]
- Brynhildsen, J. Combined hormonal contraceptives: Prescribing patterns, compliance, and benefits versus risks. Ther. Adv. Drug Saf. 2014, 5, 201–213. [Google Scholar] [CrossRef] [Green Version]
- Agency, E.M. Benefits of Combined Hormonal Contraceptives (CHCs) Continue to Outweigh Risks—CHMP Endorses PRAC Recommendation. 2021. Available online: https://www.ema.europa.eu/en/news/benefits-combined-hormonal-contraceptives-chcs-continue-outweigh-risks-chmp-endorses-prac (accessed on 30 November 2022).
- FDA. FDA Drug Safety Communication: Updated Information about the Risk of Blood Clots in Women Taking Birth Control Pills Containing Drospirenone. 2012. Available online: https://www.fda.gov/drugs/drug-safety-and-availability/fda-drug-safety-communication-updated-information-about-risk-blood-clots-women-taking-birth-control-:~:text=Based%20on%20this%20review%2C%20FDA,drospirenone%2Dcontaining%20birth%20control%20pills (accessed on 7 December 2022).
- Heit, J.A.; Spencer, F.A.; White, R.H. The epidemiology of venous thromboembolism. J Thromb. Thrombolysis 2016, 41, 3–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lidegaard, O.; Nielsen, L.H.; Skovlund, C.W.; Lokkegaard, E. Venous thrombosis in users of non-oral hormonal contraception: Follow-up study, Denmark 2001–10. BMJ 2012, 344, e2990. [Google Scholar] [CrossRef] [Green Version]
- Medical Eligibility Criteria for Contraceptive Use, 5th ed.; WHO Guidelines Approved by the Guidelines Review Committee; WHO: Geneva, Switzerland, 2015.
- NICE. Long-Acting Reversible Contraception. 2005. Available online: https://www.nice.org.uk/guidance/cg30 (accessed on 7 December 2022).
- AIFA. Nota Informativa Importante sui Contraccettivi Ormonali Combinati. 2019. Available online: https://www.aifa.gov.it/-/nota-informativa-importante-sui-contraccettivi-ormonali-combina-2 (accessed on 13 December 2022).
- Dellino, M.; Carriero, C.; Silvestris, E.; Capursi, T.; Paradiso, A.; Cormio, G. Primary Vaginal Carcinoma Arising on Cystocele Mimicking Vulvar Cancer. J. Obstet. Gynaecol. Can. 2020, 42, 1543–1545. [Google Scholar] [CrossRef] [PubMed]
- Silvestris, E.; Cormio, G.; Skrypets, T.; Dellino, M.; Paradiso, A.V.; Guarini, A.; Minoia, C. Novel aspects on gonadotoxicity and fertility preservation in lymphoproliferative neoplasms. Crit. Rev. Oncol. Hematol. 2020, 151, 102981. [Google Scholar] [CrossRef] [PubMed]
- Gast, K.; Snyder, T. Combination oral contraceptives and cancer risk. Kans. Med. 1990, 91, 201–208. [Google Scholar]
- Iversen, L.; Sivasubramaniam, S.; Lee, A.J.; Fielding, S.; Hannaford, P.C. Lifetime cancer risk and combined oral contraceptives: The Royal College of General Practitioners’ Oral Contraception Study. Am. J. Obstet. Gynecol. 2017, 216, 580.e1–580.e9. [Google Scholar] [CrossRef]
- Fruzzetti, F.; Cagnacci, A. Venous thrombosis and hormonal contraception: What’s new with estradiol-based hormonal contraceptives? Open. Access J. Contracept. 2018, 9, 75–79. [Google Scholar] [CrossRef] [Green Version]
- Peragallo Urrutia, R.; Coeytaux, R.R.; McBroom, A.J.; Gierisch, J.M.; Havrilesky, L.J.; Moorman, P.G.; Lowery, W.J.; Dinan, M.; Hasselblad, V.; Sanders, G.D.; et al. Risk of acute thromboembolic events with oral contraceptive use: A systematic review and meta-analysis. Obstet. Gynecol. 2013, 122, 380–389. [Google Scholar] [CrossRef]
- Roach, R.E.; Helmerhorst, F.M.; Lijfering, W.M.; Stijnen, T.; Algra, A.; Dekkers, O.M. Combined oral contraceptives: The risk of myocardial infarction and ischemic stroke. Cochrane Database Syst. Rev. 2015, 2015, CD011054. [Google Scholar] [CrossRef] [Green Version]
- de Bastos, M.; Stegeman, B.H.; Rosendaal, F.R.; Van Hylckama Vlieg, A.; Helmerhorst, F.M.; Stijnen, T.; Dekkers, O.M. Combined oral contraceptives: Venous thrombosis. Cochrane Database Syst. Rev. 2014, 3, CD010813. [Google Scholar] [CrossRef] [PubMed]
- Assiri, G.A.; Bannan, D.F.; Alshehri, G.H.; Alshyhani, M.; Almatri, W.; Mahmoud, M.A. The Contraindications to Combined Oral Contraceptives among Reproductive-Aged Women in an Obstetrics and Gynaecology Clinic: A Single-Centre Cross-Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 1567. [Google Scholar] [CrossRef] [PubMed]
- Williams, R.; Hensel, D.; Lehmann, A.; Sarin, T.; Shew, M.; Ott, M. Adolescent self-screening for contraindications to combined oral contraceptive pills. Contraception 2015, 92, 380. [Google Scholar] [CrossRef]
- Wilkinson, T.A.; Meredith, A.H.; Rafie, S.; Katz, A.J.; Vielott, T.L.; Meagher, C.G.; Ott, M.A. Adolescents’ and Young Adults’ Ability to Self-Screen for Contraindications to Hormonal Contraception and the Role of Chronic Illness. J. Adolesc. Health 2021, 69, 566–573. [Google Scholar] [CrossRef] [PubMed]
- Ballini, A.; Cantore, S.; Fatone, L.; Montenegro, V.; De Vito, D.; Pettini, F.; Crincoli, V.; Antelmi, A.; Romita, P.; Rapone, B.; et al. Transmission of nonviral sexually transmitted infections and oral sex. J. Sex. Med. 2012, 9, 372–384. [Google Scholar] [CrossRef]
- Cicinelli, E.; Ballini, A.; Marinaccio, M.; Poliseno, A.; Coscia, M.F.; Monno, R.; De Vito, D. Microbiological findings in endometrial specimen: Our experience. Arch. Gynecol. Obstet. 2012, 285, 1325–1329. [Google Scholar] [CrossRef]
- Di Cosola, M.; Cazzolla, A.P.; Charitos, I.A.; Ballini, A.; Inchingolo, F.; Santacroce, L. Candida albicans and Oral Carcinogenesis. A Brief Review. J. Fungi 2021, 7, 476. [Google Scholar] [CrossRef]
- Coscia, M.F.; Monno, R.; Ballini, A.; Mirgaldi, R.; Dipalma, G.; Pettini, F.; Cristallo, V.; Inchingolo, F.; Foti, C.; de Vito, D. Human papilloma virus (HPV) genotypes prevalence in a region of South Italy (Apulia). Ann. Ist Super. Sanit. 2015, 51, 248–251. [Google Scholar] [CrossRef]
- Dellino, M.; Cascardi, E.; Laganà, A.S.; Di Vagno, G.; Malvasi, A.; Zaccaro, R.; Maggipinto, K.; Cazzato, G.; Scacco, S.; Tinelli, R.; et al. Lactobacillus crispatus M247 oral administration: Is it really an effective strategy in the management of papillomavirus-infected women? Infect. Agent Cancer 2022, 17, 53. [Google Scholar] [CrossRef]
- Dellino, M.; Cascardi, E.; Tomasone, V.; Zaccaro, R.; Maggipinto, K.; Giacomino, M.E.; De Nicolò, M.; De Summa, S.; Cazzato, G.; Scacco, S.; et al. Communications Is Time for Care: An Italian Monocentric Survey on Human Papillomavirus (HPV) Risk Information as Part of Cervical Cancer Screening. J. Pers. Med. 2022, 12, 1387. [Google Scholar] [CrossRef]
- Muzio, L.L.; Ballini, A.; Cantore, S.; Bottalico, L.; Charitos, I.A.; Ambrosino, M.; Nocini, R.; Malcangi, A.; Dioguardi, M.; Cazzolla, A.P.; et al. Overview of Candida albicans and Human Papillomavirus (HPV) Infection Agents and their Biomolecular Mechanisms in Promoting Oral Cancer in Pediatric Patients. BioMed Res. Int. 2021, 2021, 7312611. [Google Scholar] [CrossRef]
- Dellino, M.; Lamanna, B.; Vinciguerra, M.; Tafuri, S.; Stefanizzi, P.; Malvasi, A.; Di Vagno, G.; Cormio, G.; Loizzi, V.; Cazzato, G.; et al. SARS-CoV-2 Vaccines and Adverse Effects in Gynecology and Obstetrics: The First Italian Retrospective Study. Int. J. Environ. Res. Public Health 2022, 19, 13167. [Google Scholar] [CrossRef]
- Dellino, M.; Cascardi, E.; Vinciguerra, M.; Lamanna, B.; Malvasi, A.; Scacco, S.; Acquaviva, S.; Pinto, V.; Di Vagno, G.; Cormio, G.; et al. Nutrition as Personalized Medicine against SARS-CoV-2 Infections: Clinical and Oncological Options with a Specific Female Groups Overview. Int. J. Mol. Sci. 2022, 23, 9136. [Google Scholar] [CrossRef]
- Dellino, M.; Vimercati, A.; D’Amato, A.; Damiani, G.R.; Laganà, A.S.; Cicinelli, E.; Pinto, V.; Malvasi, A.; Scacco, S.; Ballini, A.; et al. “GONE WITH THE WIND”: The Transitory Effects of COVID-19 on the Gynecological System. J. Pers. Med. 2023, 13, 312. [Google Scholar] [CrossRef]
- Charitos, I.A.; Ballini, A.; Lovero, R.; Castellaneta, F.; Colella, M.; Scacco, S.; Cantore, S.; Arrigoni, R.; Mastrangelo, F.; Dioguardi, M. Update on COVID-19 and Effectiveness of a Vaccination Campaign in a Global Context. Int. J. Environ. Res. Public Health 2022, 19, 10712. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vinciguerra, M.; Cascardi, E.; Lamanna, B.; Marrone, M.; Pititto, F.; Macorano, E.; Sciorio, R.; Baldini, G.M.; Malvasi, A.; Ballini, A.; et al. A Multi-Institutional Informed Consent Proposal as a Prevention Tool for Combined Oral Contraceptive Intake and Thrombotic Risk. J. Pers. Med. 2023, 13, 584. https://doi.org/10.3390/jpm13040584
Vinciguerra M, Cascardi E, Lamanna B, Marrone M, Pititto F, Macorano E, Sciorio R, Baldini GM, Malvasi A, Ballini A, et al. A Multi-Institutional Informed Consent Proposal as a Prevention Tool for Combined Oral Contraceptive Intake and Thrombotic Risk. Journal of Personalized Medicine. 2023; 13(4):584. https://doi.org/10.3390/jpm13040584
Chicago/Turabian StyleVinciguerra, Marina, Eliano Cascardi, Bruno Lamanna, Maricla Marrone, Fortunato Pititto, Enrica Macorano, Romualdo Sciorio, Giorgio Maria Baldini, Antonio Malvasi, Andrea Ballini, and et al. 2023. "A Multi-Institutional Informed Consent Proposal as a Prevention Tool for Combined Oral Contraceptive Intake and Thrombotic Risk" Journal of Personalized Medicine 13, no. 4: 584. https://doi.org/10.3390/jpm13040584