
Association of Diabetes Mellitus with All-Cause and Cause-Specific Mortality among Patients with Metabolic-Dysfunction-Associated Fatty Liver Disease: A Longitudinal Cohort Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection and Study Setting
2.2. Study Variable Measurement
2.3. Clinical and Laboratory Assessments
3. Results
3.1. Baseline Characteristics of the Included Population
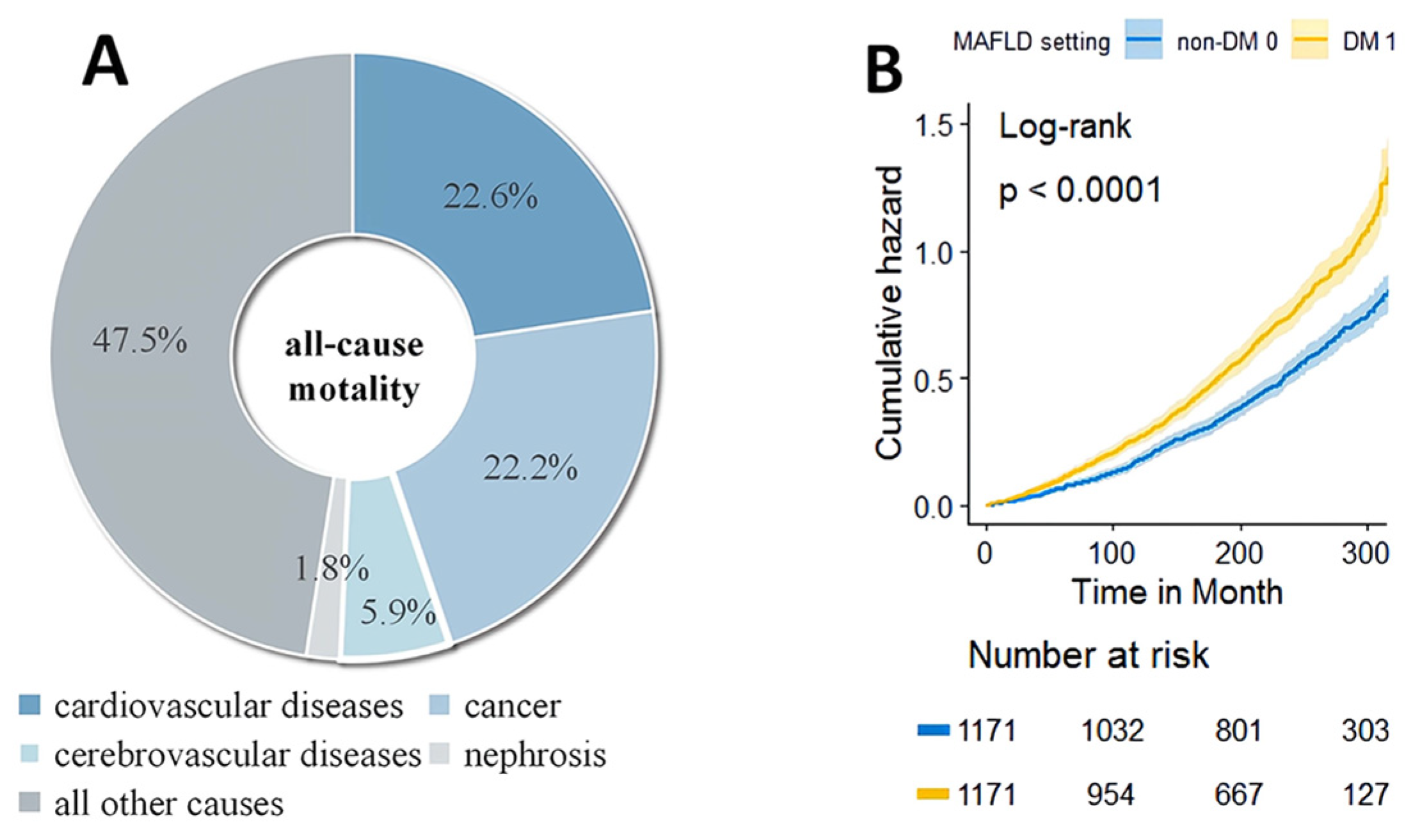
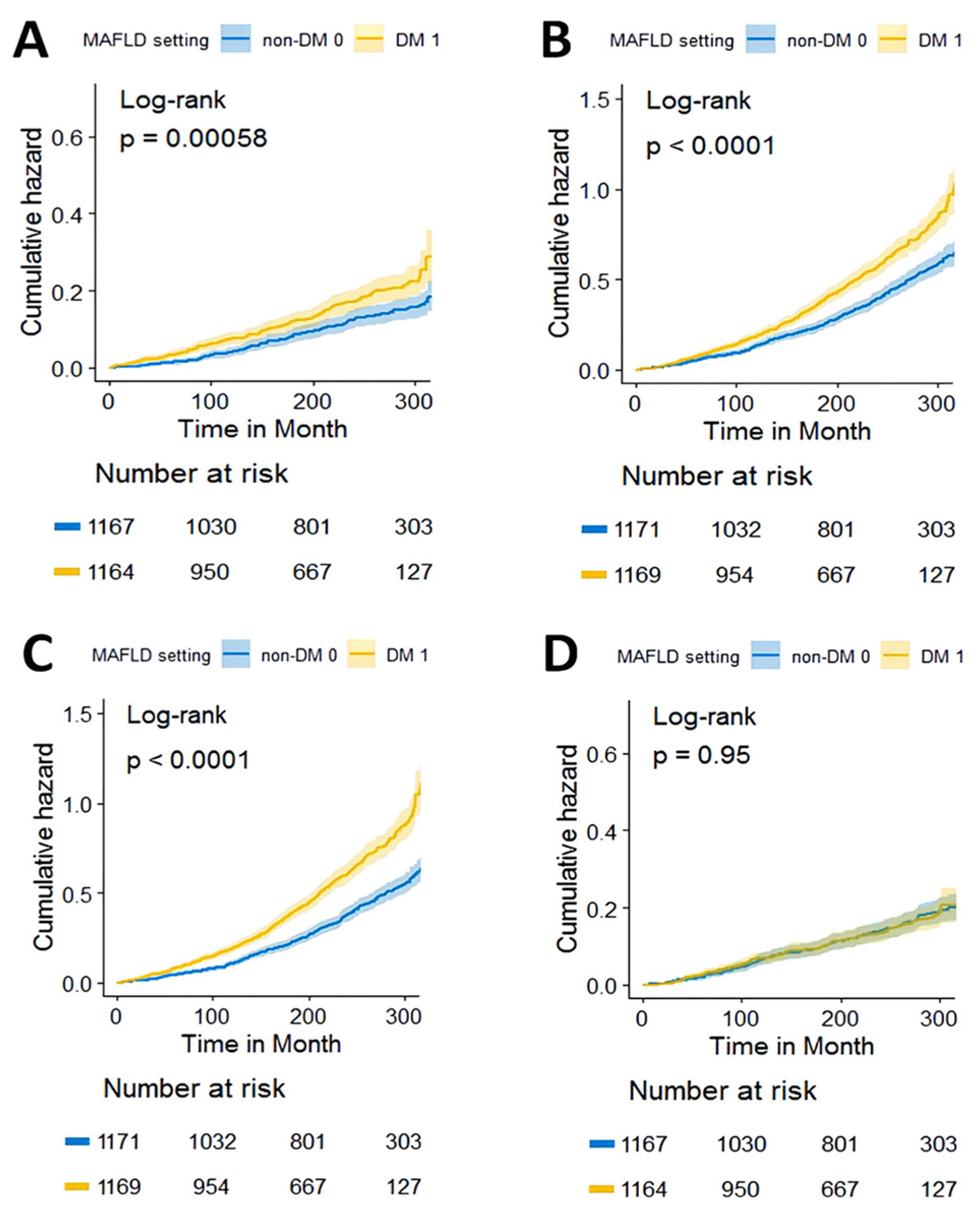
3.2. Relationship between DM and Overall and Specific Causes of Mortality in MAFLD Patients
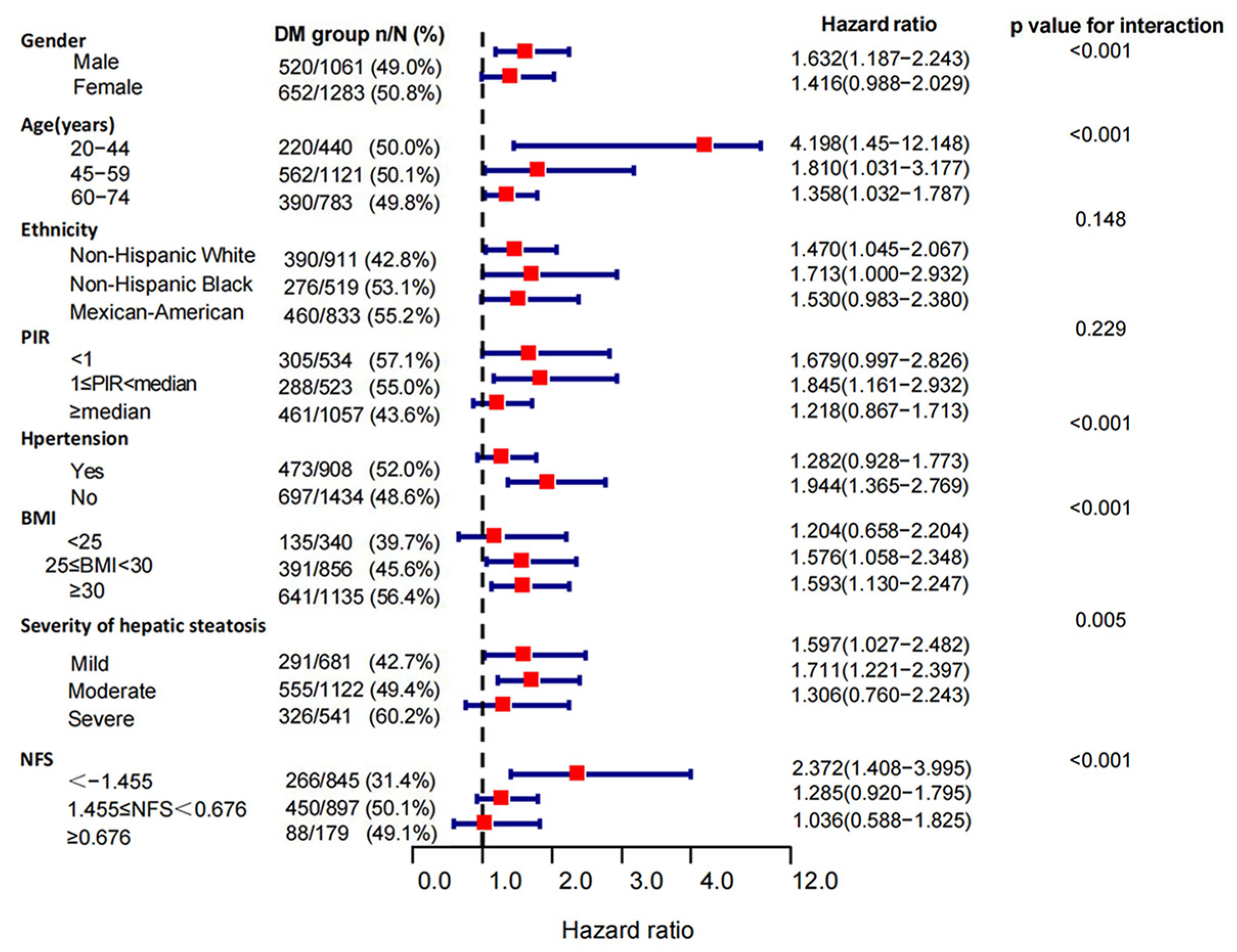
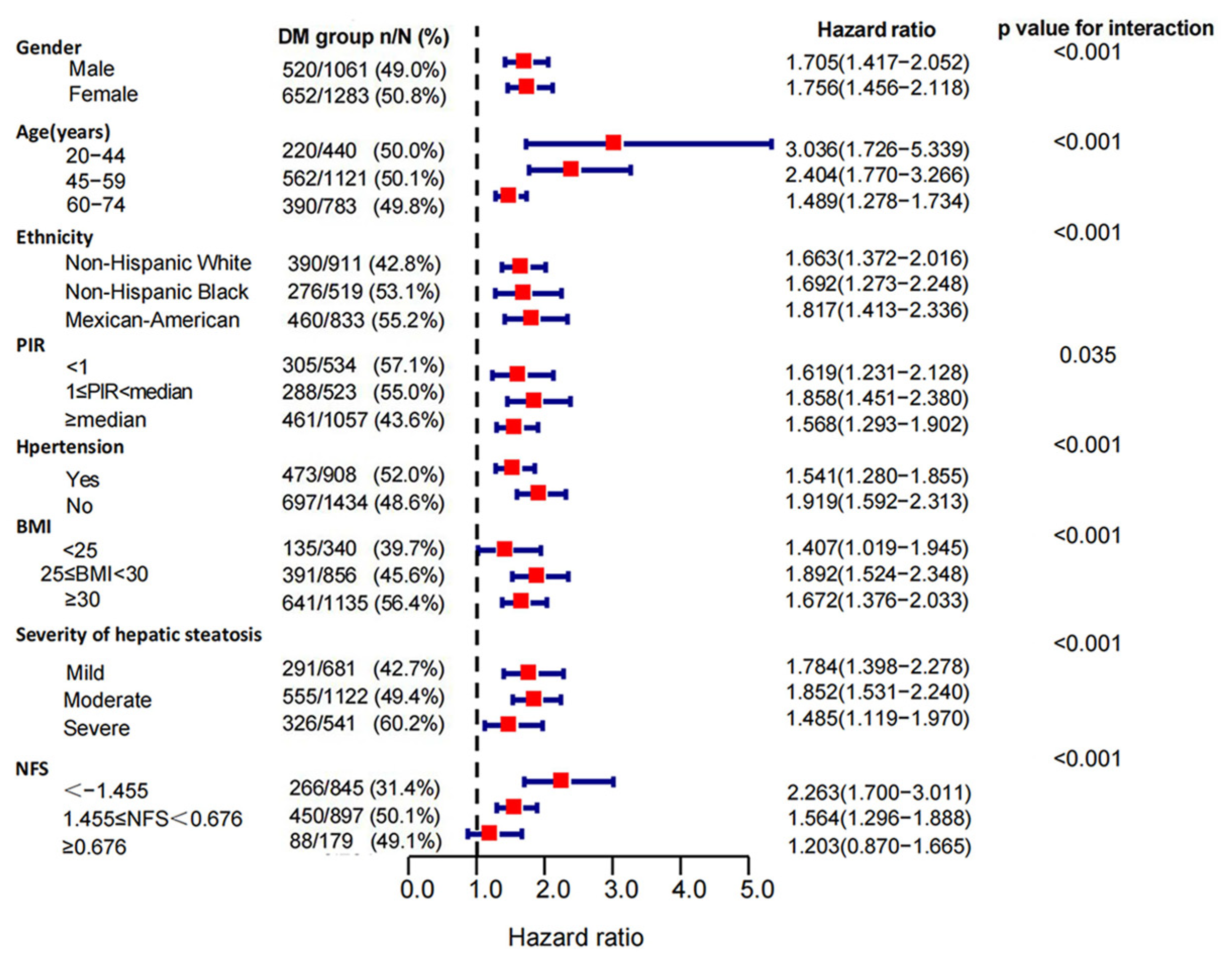
3.3. Subgroup Analysis of the Association of DM with Mortality in MAFLD Patients
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Le, M.H.; Yeo, Y.H.; Li, X.; Li, J.; Zou, B.; Wu, Y.; Ye, Q.; Huang, D.Q.; Zhao, C.; Zhang, J.; et al. 2019 Global NAFLD Prevalence: A Systematic Review and Meta-analysis. Clin. Gastroenterol. Hepatol. 2021, 20, 2809–2817.e28. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Zou, B.; Yeo, Y.H.; Feng, Y.; Xie, X.; Lee, D.H.; Fujii, H.; Wu, Y.; Kam, L.Y.; Ji, F.; et al. Prevalence, incidence, and outcome of non-alcoholic fatty liver disease in Asia, 1999-2019: A systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 2019, 4, 389–398. [Google Scholar] [CrossRef] [PubMed]
- Rui, F.; Yang, H.; Hu, X.; Xue, Q.; Xu, Y.; Shi, J.; Li, J. Renaming NAFLD to MAFLD: Advantages and Potential Changes in Diagnosis, Pathophysiology, Treatment, and Management. Infect. Microbes Dis. 2022, 4, 49–55. [Google Scholar] [CrossRef]
- Nguyen, V.H.; Le, M.H.; Cheung, R.C.; Nguyen, M.H. Differential Clinical Characteristics and Mortality Outcomes in Persons With NAFLD and/or MAFLD. Clin. Gastroenterol. Hepatol. 2021, 19, 2172–2181.e2176. [Google Scholar] [CrossRef]
- Matteoni, C.A.; Younossi, Z.M.; Gramlich, T.; Boparai, N.; Liu, Y.C.; McCullough, A.J. Nonalcoholic fatty liver disease: A spectrum of clinical and pathological severity. Gastroenterology 1999, 116, 1413–1419. [Google Scholar] [CrossRef]
- Margini, C.; Dufour, J.F. The story of HCC in NAFLD: From epidemiology, across pathogenesis, to prevention and treatment. Liver Int. 2016, 36, 317–324. [Google Scholar] [CrossRef] [Green Version]
- Byrne, C.D.; Targher, G. NAFLD: A multisystem disease. J. Hepatol. 2015, 62, S47–S64. [Google Scholar] [CrossRef] [Green Version]
- Sun, H.; Saeedi, P.; Karuranga, S.; Pinkepank, M.; Ogurtsova, K.; Duncan, B.B.; Stein, C.; Basit, A.; Chan, J.C.N.; Mbanya, J.C.; et al. IDF Diabetes Atlas: Global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res. Clin. Pract. 2022, 183, 109119. [Google Scholar] [CrossRef]
- Younossi, Z.M.; Golabi, P.; de Avila, L.; Paik, J.M.; Srishord, M.; Fukui, N.; Qiu, Y.; Burns, L.; Afendy, A.; Nader, F. The global epidemiology of NAFLD and NASH in patients with type 2 diabetes: A systematic review and meta-analysis. J. Hepatol. 2019, 71, 793–801. [Google Scholar] [CrossRef]
- Jarvis, H.; Craig, D.; Barker, R.; Spiers, G.; Stow, D.; Anstee, Q.M.; Hanratty, B. Metabolic risk factors and incident advanced liver disease in non-alcoholic fatty liver disease (NAFLD): A systematic review and meta-analysis of population-based observational studies. PLoS Med. 2020, 17, e1003100. [Google Scholar] [CrossRef]
- Suzuki, A.; Angulo, P.; Lymp, J.; St Sauver, J.; Muto, A.; Okada, T.; Lindor, K. Chronological development of elevated aminotransferases in a nonalcoholic population. Hepatology 2005, 41, 64–71. [Google Scholar] [CrossRef] [PubMed]
- Stepanova, M.; Rafiq, N.; Makhlouf, H.; Agrawal, R.; Kaur, I.; Younoszai, Z.; McCullough, A.; Goodman, Z.; Younossi, Z.M. Predictors of all-cause mortality and liver-related mortality in patients with non-alcoholic fatty liver disease (NAFLD). Dig. Dis. Sci. 2013, 58, 3017–3023. [Google Scholar] [CrossRef] [PubMed]
- Fracanzani, A.L.; Valenti, L.; Bugianesi, E.; Andreoletti, M.; Colli, A.; Vanni, E.; Bertelli, C.; Fatta, E.; Bignamini, D.; Marchesini, G.; et al. Risk of severe liver disease in nonalcoholic fatty liver disease with normal aminotransferase levels: A role for insulin resistance and diabetes. Hepatology 2008, 48, 792–798. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.; Huang, J.; Wang, M.; Kumar, R.; Liu, Y.; Liu, S.; Wu, Y.; Wang, X.; Zhu, Y. Comparison of MAFLD and NAFLD diagnostic criteria in real world. Liver Int. 2020, 40, 2082–2089. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes-2020. Diabetes Care 2020, 43, S14–S31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eslam, M.; Newsome, P.N.; Sarin, S.K.; Anstee, Q.M.; Targher, G.; Romero-Gomez, M.; Zelber-Sagi, S.; Wai-Sun Wong, V.; Dufour, J.F.; Schattenberg, J.M.; et al. A new definition for metabolic dysfunction-associated fatty liver disease: An international expert consensus statement. J. Hepatol. 2020, 73, 202–209. [Google Scholar] [CrossRef]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension: The Task Force for the management of arterial hypertension of the European Society of Cardiology and the European Society of Hypertension: The Task Force for the management of arterial hypertension of the European Society of Cardiology and the European Society of Hypertension. J. Hypertens. 2018, 36, 1953–2041. [Google Scholar] [CrossRef] [Green Version]
- Xiao, G.; Zhu, S.; Xiao, X.; Yan, L.; Yang, J.; Wu, G. Comparison of laboratory tests, ultrasound, or magnetic resonance elastography to detect fibrosis in patients with nonalcoholic fatty liver disease: A meta-analysis. Hepatology 2017, 66, 1486–1501. [Google Scholar] [CrossRef] [Green Version]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., 3rd; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- Angulo, P.; Hui, J.M.; Marchesini, G.; Bugianesi, E.; George, J.; Farrell, G.C.; Enders, F.; Saksena, S.; Burt, A.D.; Bida, J.P.; et al. The NAFLD fibrosis score: A noninvasive system that identifies liver fibrosis in patients with NAFLD. Hepatology 2007, 45, 846–854. [Google Scholar] [CrossRef]
- Sterling, R.K.; Lissen, E.; Clumeck, N.; Sola, R.; Correa, M.C.; Montaner, J.; Sulkowski, M.S.; Torriani, F.J.; Dieterich, D.T.; Thomas, D.L.; et al. Development of a simple noninvasive index to predict significant fibrosis in patients with HIV/HCV coinfection. Hepatology 2006, 43, 1317–1325. [Google Scholar] [CrossRef]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: Insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mantovani, A.; Petracca, G.; Beatrice, G.; Tilg, H.; Byrne, C.D.; Targher, G. Non-alcoholic fatty liver disease and risk of incident diabetes mellitus: An updated meta-analysis of 501 022 adult individuals. Gut 2021, 70, 962–969. [Google Scholar] [CrossRef] [PubMed]
- Arrese, M.; Barrera, F.; Triantafilo, N.; Arab, J.P. Concurrent nonalcoholic fatty liver disease and type 2 diabetes: Diagnostic and therapeutic considerations. Expert Rev. Gastroenterol. Hepatol. 2019, 13, 849–866. [Google Scholar] [CrossRef] [PubMed]
- Lonardo, A.; Nascimbeni, F.; Mantovani, A.; Targher, G. Hypertension, diabetes, atherosclerosis and NASH: Cause or consequence? J. Hepatol. 2018, 68, 335–352. [Google Scholar] [CrossRef] [PubMed]
- Stefan, N.; Häring, H.U.; Cusi, K. Non-alcoholic fatty liver disease: Causes, diagnosis, cardiometabolic consequences, and treatment strategies. Lancet Diabetes Endocrinol. 2019, 7, 313–324. [Google Scholar] [CrossRef]
- Strain, W.D.; Paldánius, P.M. Diabetes, cardiovascular disease and the microcirculation. Cardiovasc. Diabetol. 2018, 17, 57. [Google Scholar] [CrossRef] [Green Version]
- Adams, L.A.; Anstee, Q.M.; Tilg, H.; Targher, G. Non-alcoholic fatty liver disease and its relationship with cardiovascular disease and other extrahepatic diseases. Gut 2017, 66, 1138–1153. [Google Scholar] [CrossRef] [Green Version]
- Armstrong, M.J.; Haydon, G.; Syn, W.K. Beyond the liver in patients with non-alcoholic fatty liver disease (NAFLD)-cause for concern? Hepatobiliary Surg. Nutr. 2018, 7, 138–142. [Google Scholar] [CrossRef] [Green Version]
- Shlomai, G.; Neel, B.; LeRoith, D.; Gallagher, E.J. Type 2 Diabetes Mellitus and Cancer: The Role of Pharmacotherapy. J. Clin. Oncol. 2016, 34, 4261–4269. [Google Scholar] [CrossRef] [Green Version]
- Huang, D.Q.; El-Serag, H.B.; Loomba, R. Global epidemiology of NAFLD-related HCC: Trends, predictions, risk factors and prevention. Nat. Rev. Gastroenterol. Hepatol. 2021, 18, 223–238. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.D.; Ahmed, F.; Mara, K.C.; Addissie, B.D.; Allen, A.M.; Gores, G.J.; Roberts, L.R. Diabetes Is Associated With Increased Risk of Hepatocellular Carcinoma in Patients With Cirrhosis From Nonalcoholic Fatty Liver Disease. Hepatology 2020, 71, 907–916. [Google Scholar] [CrossRef] [PubMed]
- Johnston, M.P.; Patel, J.; Byrne, C.D. Diabetes is associated with increased risk of hepatocellular carcinoma in non-alcoholic steatohepatitis with cirrhosis-implications for surveillance and future pharmacotherapy. Hepatobiliary Surg. Nutr. 2020, 9, 230–234. [Google Scholar] [CrossRef] [PubMed]
- Taylor, R.S.; Taylor, R.J.; Bayliss, S.; Hagström, H.; Nasr, P.; Schattenberg, J.M.; Ishigami, M.; Toyoda, H.; Wai-Sun Wong, V.; Peleg, N.; et al. Association Between Fibrosis Stage and Outcomes of Patients With Nonalcoholic Fatty Liver Disease: A Systematic Review and Meta-Analysis. Gastroenterology 2020, 158, 1611–1625.e1612. [Google Scholar] [CrossRef] [Green Version]
- Hopkins, B.D.; Goncalves, M.D.; Cantley, L.C. Obesity and Cancer Mechanisms: Cancer Metabolism. J. Clin. Oncol. 2016, 34, 4277–4283. [Google Scholar] [CrossRef] [Green Version]
- Kautzky-Willer, A.; Harreiter, J.; Pacini, G. Sex and Gender Differences in Risk, Pathophysiology and Complications of Type 2 Diabetes Mellitus. Endocr. Rev. 2016, 37, 278–316. [Google Scholar] [CrossRef] [Green Version]
- Spanakis, E.K.; Golden, S.H. Race/ethnic difference in diabetes and diabetic complications. Curr. Diab. Rep. 2013, 13, 814–823. [Google Scholar] [CrossRef] [Green Version]
- Levi, F.; Lucchini, F.; Negri, E.; La Vecchia, C. Trends in mortality from cardiovascular and cerebrovascular diseases in Europe and other areas of the world. Heart 2002, 88, 119–124. [Google Scholar] [CrossRef]
- Harding, J.L.; Pavkov, M.E.; Magliano, D.J.; Shaw, J.E.; Gregg, E.W. Global trends in diabetes complications: A review of current evidence. Diabetologia 2019, 62, 3–16. [Google Scholar] [CrossRef] [Green Version]
- Gregg, E.W.; Cheng, Y.J.; Srinivasan, M.; Lin, J.; Geiss, L.S.; Albright, A.L.; Imperatore, G. Trends in cause-specific mortality among adults with and without diagnosed diabetes in the USA: An epidemiological analysis of linked national survey and vital statistics data. Lancet 2018, 391, 2430–2440. [Google Scholar] [CrossRef]
- Huo, L.; Magliano, D.J.; Rancière, F.; Harding, J.L.; Nanayakkara, N.; Shaw, J.E.; Carstensen, B. Impact of age at diagnosis and duration of type 2 diabetes on mortality in Australia 1997–2011. Diabetologia 2018, 61, 1055–1063. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Færch, K.; Carstensen, B.; Almdal, T.P.; Jørgensen, M.E. Improved survival among patients with complicated type 2 diabetes in Denmark: A prospective study (2002–2010). J. Clin. Endocrinol. Metab. 2014, 99, E642–E646. [Google Scholar] [CrossRef] [Green Version]
- Viner, R.; White, B.; Christie, D. Type 2 diabetes in adolescents: A severe phenotype posing major clinical challenges and public health burden. Lancet 2017, 389, 2252–2260. [Google Scholar] [CrossRef] [PubMed]
- Magliano, D.J.; Sacre, J.W.; Harding, J.L.; Gregg, E.W.; Zimmet, P.Z.; Shaw, J.E. Young-onset type 2 diabetes mellitus—Implications for morbidity and mortality. Nat. Rev. Endocrinol. 2020, 16, 321–331. [Google Scholar] [CrossRef] [PubMed]
- Bhaskaran, K.; Dos-Santos-Silva, I.; Leon, D.A.; Douglas, I.J.; Smeeth, L. Association of BMI with overall and cause-specific mortality: A population-based cohort study of 3·6 million adults in the UK. Lancet Diabetes Endocrinol. 2018, 6, 944–953. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aune, D.; Sen, A.; Prasad, M.; Norat, T.; Janszky, I.; Tonstad, S.; Romundstad, P.; Vatten, L.J. BMI and all cause mortality: Systematic review and non-linear dose-response meta-analysis of 230 cohort studies with 3.74 million deaths among 30.3 million participants. BMJ 2016, 353, i2156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zaccardi, F.; Dhalwani, N.N.; Papamargaritis, D.; Webb, D.R.; Murphy, G.J.; Davies, M.J.; Khunti, K. Nonlinear association of BMI with all-cause and cardiovascular mortality in type 2 diabetes mellitus: A systematic review and meta-analysis of 414,587 participants in prospective studies. Diabetologia 2017, 60, 240–248. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Overall Cohort (n = 2344) | Non-DM Cohort (n = 1172) | DM Cohort (n = 1172) | p-Value | |
|---|---|---|---|---|
| Male, gender (%) | 1061 (45.3) | 541 (46.2) | 520 (44.4) | 0.384 |
| Age, years. | 60 (48.67) | 60 (48.67) | 60 (48.67) | 0.995 |
| Ethnicity (%) | <0.001 | |||
| Non-Hispanic White | 911 (38.9) | 521 (44.5) | 390 (33.3) | |
| Non-Hispanic Black | 519 (22.1) | 243 (20.7) | 276 (23.5) | |
| Mexican American | 833 (35.5) | 373 (31.9) | 460 (39.2) | |
| Other | 81 (3.5) | 35 (3.0) | 46 (3.9) | |
| PIR | <0.001 | |||
| <1 | 533 (25.2) | 228 (21.5) | 305 (28.9) | |
| 1 ≤ PIR < median | 523 (24.7) | 235 (22.2) | 288 (27.3) | |
| ≥median | 1058 (50.0) | 597 (56.3) | 461 (43.7) | |
| Hypertension (%) | 908 (38.8) | 435 (37.1) | 473 (40.4) | 0.1 |
| BMI | <0.001 | |||
| <25 | 341 (14.6) | 206 (17.7) | 135 (11.6) | |
| 25 ≤ BMI < 30 | 856 (36.7) | 465 (39.9) | 391 (33.5) | |
| ≥30 | 1134 (48.6) | 493 (42.4) | 641 (54.9) | |
| ALT (U/L) | 16 (12, 24) | 15 (11, 21) | 18 (13, 27) | <0.001 |
| AST (U/L) | 20 (17, 27) | 20 (17, 26) | 20 (17, 27) | 0.45 |
| ALP (U/L) | 90 (74, 110) | 86 (71, 103) | 95 (77, 117) | <0.001 |
| CRP (mg/dL) | 0.3 (0.2, 0.7) | 0.2 (0.2, 0.6) | 0.4 (0.2, 0.9) | <0.001 |
| FRP (ng/mL) | 127 (65, 243) | 110 (55, 196) | 153 (77, 285) | <0.001 |
| Vitamin A (umol/L) | 2.0 (1.7, 2.4) | 2.1 (1.8, 2.5) | 2.0 (1.6, 2.4) | <0.001 |
| Vitamin C (umol/L) | 36.9 (18.2, 53.4) | 38.0 (17.0, 55.6) | 35.8 (18.7, 51.7) | 0.105 |
| Vitamin E (umol/L) | 26.8 (21.6, 33.6) | 26.5 (21.5, 32.6) | 27.17 (21.6, 35.0) | 0.011 |
| Serum selenium (nmol/L) | 1.6 (1.4, 1.7) | 1.6 (1.4, 1.7) | 1.6 (1.5, 1.7) | <0.001 |
| PLT (* 109/L) | 267.0 (224.5, 318.3) | 271.0 (228.0, 320.5) | 263.0 (220.0, 315.5) | 0.023 |
| TC (mmol/L) | 5.6 (4.9, 6.4) | 5.6 (4.9, 6.27) | 5.6 (4.9, 6.5) | 0.078 |
| TG (mmol/L) | 1.9 (1.3, 2.7) | 1.6 (1.15, 2.36) | 2.1 (1.5, 3.1) | <0.001 |
| HDL-C (mmol/L) | 1.2 (1.0, 1.4) | 1.2 (1.0, 1.5) | 1.1 (0.9, 1.3) | <0.001 |
| Total protein (g/L) | 74 (71, 77) | 73 (71, 77) | 75 (72, 78) | <0.001 |
| Albumin (g/L) | 41 (39, 43) | 41 (39, 44) | 41 (38, 43) | <0.001 |
| UA (umol/L) | 333.1 (273.6, 392.6) | 339 (284.0, 398.5) | 327.1 (261.7, 392.6) | 0.001 |
| Scr (mg/dL) | 1.0 (0.9, 1.2) | 1.1 (0.9, 1.2) | 1.0 (0.9, 1.2) | 0.008 |
| eGFR category (%) | <0.001 | |||
| ≥90 (Stage 1 CKD) | 337 (14.9) | 135 (12.1) | 202 (17.7) | |
| 60 ≤ eGFR < 90 (Stage 2 CKD) | 1349 (59.8) | 693 (62.0) | 656 (57.6) | |
| 30 ≤ eGFR < 60 (Stage 3 CKD) | 550 (24.4) | 283 (25.3) | 267 (23.4) | |
| <30 (Stage 4–5 CKD) | 20 (0.9) | 6 (0.5) | 14 (1.2) | |
| FIB-4 category (%) | 0.042 | |||
| <1.3 | 1394 (62.7) | 666 (60.7) | 728 (64.6) | |
| 1.3 ≤ FIB-4 < 2.67 | 742 (33.3) | 393 (35.8) | 349 (31.0) | |
| ≥2.67 | 89 (4.0) | 39 (3.6) | 50 (4.4) | |
| NFS category (%) | <0.001 | |||
| <−1.455 | 846 (37.5) | 580 (51.9) | 266 (23.4) | |
| −1.455 ≤ NFS < 0.676 | 1090 (48.3) | 447 (40.0) | 643 (56.5) | |
| ≥0.676 | 321 (14.2) | 91 (8.1) | 230 (20.2) | |
| Severity of hepatic steatosis (%) | <0.001 | |||
| Mild | 681 (29.1) | 390 (33.3) | 291 (24.8) | |
| Moderate | 1122 (47.9) | 567 (48.4) | 555 (47.4) | |
| Severe | 541 (23.1) | 215 (18.3) | 326 (27.8) | 0.384 |
| Model 1 | Model 2 | Model 3 | |||||
|---|---|---|---|---|---|---|---|
| Unadjusted HR | HR (95% Cl) | p-Value | HR (95% Cl) | p-Value | HR (95% Cl) | p-Value | |
| All-cause mortality | 1.459 (1.310, 1.623) | 1.546 (1.381, 1.732) | <0.001 | 1.564 (1.395, 1.753) | <0.001 | 1.428 (1.257, 1.623) | <0.001 |
| Cardiovascular mortality | 1.482 (1.183, 1.858) | 1.546 (1.221, 2.230) | <0.001 | 1.526 (1.204, 1.935) | <0.001 | 1.464 (1.122, 1.909) | 0.005 |
| Cancer mortality | 0.993 (0.791, 1.246) | 1.143 (0.903, 1.447) | 0.267 | 1.173 (0.924, 1.489) | 0.189 | 1.026 (0.787, 1.336) | 0.851 |
| Non-cardiovascular-related mortality | 1.448 (1.282, 1.637) | 1.546 (1.358, 1.760) | <0.001 | 1.575 (1.382, 1.796) | <0.001 | 1.423 (1.229, 1.647) | <0.001 |
| Non-cancer-related mortality | 1.627 (1.439, 1.840) | 1.696 (1.489, 1.932) | <0.001 | 1.709 (1.499, 1.948) | <0.001 | 1.587 (1.370, 1.838) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhu, Y.; Liu, C.; Xu, X.; Ma, X.; Liu, J.; Zhang, Z.; Li, F.; Wong, D.K.-H.; Fan, Z.; Wu, C.; et al. Association of Diabetes Mellitus with All-Cause and Cause-Specific Mortality among Patients with Metabolic-Dysfunction-Associated Fatty Liver Disease: A Longitudinal Cohort Study. J. Pers. Med. 2023, 13, 554. https://doi.org/10.3390/jpm13030554
Zhu Y, Liu C, Xu X, Ma X, Liu J, Zhang Z, Li F, Wong DK-H, Fan Z, Wu C, et al. Association of Diabetes Mellitus with All-Cause and Cause-Specific Mortality among Patients with Metabolic-Dysfunction-Associated Fatty Liver Disease: A Longitudinal Cohort Study. Journal of Personalized Medicine. 2023; 13(3):554. https://doi.org/10.3390/jpm13030554
Chicago/Turabian StyleZhu, Yixuan, Chuan Liu, Xiaoming Xu, Xiaoyan Ma, Jiacheng Liu, Zhiyi Zhang, Fuchao Li, Danny Ka-Ho Wong, Zhiwen Fan, Chao Wu, and et al. 2023. "Association of Diabetes Mellitus with All-Cause and Cause-Specific Mortality among Patients with Metabolic-Dysfunction-Associated Fatty Liver Disease: A Longitudinal Cohort Study" Journal of Personalized Medicine 13, no. 3: 554. https://doi.org/10.3390/jpm13030554