
The Association of Intravitreal Injections of Different Anti-Vascular Endothelial Growth Factor with Systemic Outcomes in Diabetic Patients

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Patient Inclusion
2.3. Covariates
2.4. Outcomes
2.5. Statistical Analysis
3. Results
3.1. Patient Enrollment
3.2. Baseline Characteristics
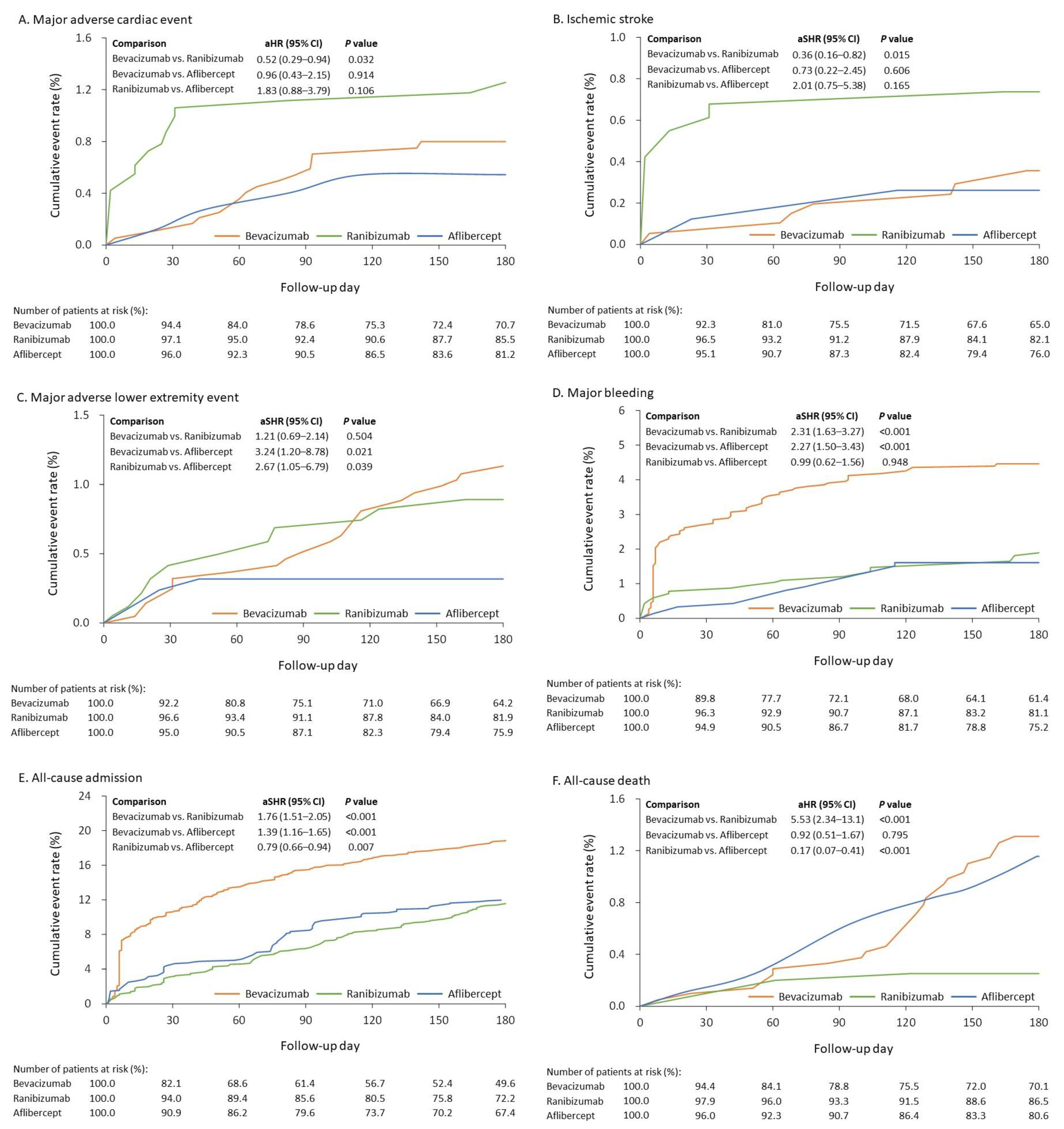
3.3. Clinical Events
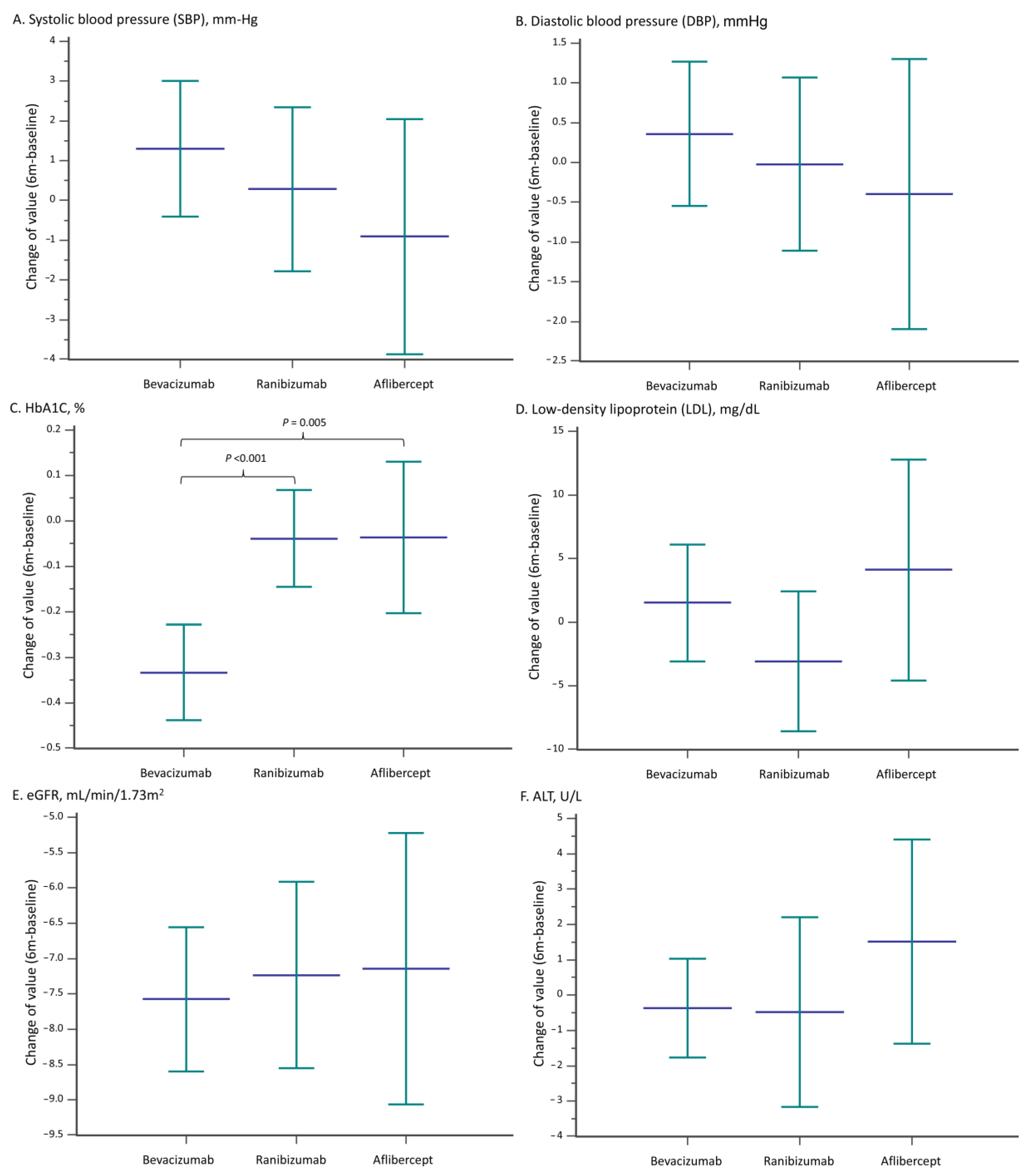
3.4. Laboratory Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Liu, J.; Ren, Z.-H.; Qiang, H.; Wu, J.; Shen, M.; Zhang, L.; Lyu, J. Trends in the incidence of diabetes mellitus: Results from the Global Burden of Disease Study 2017 and implications for diabetes mellitus prevention. BMC Public Health 2020, 20, 1415. [Google Scholar] [CrossRef]
- Williams, R.; Karuranga, S.; Malanda, B.; Saeedi, P.; Basit, A.; Besançon, S.; Bommer, C.; Esteghamati, A.; Ogurtsova, K.; Zhang, P.; et al. Global and regional estimates and projections of diabetes-related health ex-penditure: Results from the International Diabetes Federation Diabetes Atlas. Diabetes Res. Clin. Pract. 2020, 162, 108072. [Google Scholar] [CrossRef] [Green Version]
- Capitão, M.; Soares, R. Angiogenesis and inflammation crosstalk in diabetic retinopathy. J. Cell. Biochem. 2016, 117, 2443–2453. [Google Scholar] [CrossRef] [PubMed]
- Lee, R.; Wong, T.Y.; Sabanayagam, C. Epidemiology of Diabetic Retinopathy, Diabetic Macular Edema and Related Vision Loss. Eye Vis. 2015, 2, 17. [Google Scholar] [CrossRef] [Green Version]
- Rittiphairoj, T.; Mir, T.A.; Li, T.; Virgili, G. Intravitreal steroids for macular edema in diabetes. Cochrane Database Syst. Rev. 2020, 2020, CD005656. [Google Scholar] [CrossRef]
- Jorge, E.C.; Jorge, E.N.; Botelho, M.; Farat, J.G.; Virgili, G.; El Dib, R. Monotherapy laser photocoagulation for diabetic macular oedema. Cochrane Database Syst. Rev. 2018, 10, CD010859. [Google Scholar] [CrossRef] [PubMed]
- Virgili, G.; Parravano, M.; Evans, J.R.; Gordon, I.; Lucenteforte, E. Anti-vascular endothelial growth factor for diabetic macular oedema: A network meta-analysis. Cochrane Database Syst. Rev. 2017, 6, CD007419. [Google Scholar] [CrossRef]
- Simó, R.; Sundstrom, J.M.; Antonetti, D.A. Ocular Anti-VEGF Therapy for Diabetic Retinopathy: The Role of VEGF in the Pathogenesis of Diabetic Retinopathy. Diabetes Care 2014, 37, 893–899. [Google Scholar] [CrossRef] [Green Version]
- Wu, S.; Kim, C.; Baer, L.; Zhu, X. Bevacizumab Increases Risk for Severe Proteinuria in Cancer Patients. J. Am. Soc. Nephrol. 2010, 21, 1381–1389. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, M.; Kroetz, D.L. Bevacizumab-induced hypertension: Clinical presentation and molecular understanding. Pharmacol. Ther. 2017, 182, 152–160. [Google Scholar] [CrossRef] [Green Version]
- Totzeck, M.; Mincu, R.I.; Rassaf, T. Cardiovascular Adverse Events in Patients With Cancer Treated With Bevacizumab: A Meta-Analysis of More Than 20,000 Patients. J. Am. Heart Assoc. 2017, 6, e006278. [Google Scholar] [CrossRef] [Green Version]
- Ranpura, V.; Hapani, S.; Wu, S. Treatment-Related Mortality With Bevacizumab in Cancer Patients: A meta-analysis. JAMA 2011, 305, 487–494. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Avery, R.L.; Castellarin, A.A.; Steinle, N.C.; Dhoot, D.S.; Pieramici, D.J.; See, R.; Couvillion, S.; Nasir, M.A.; Rabena, M.D.; Maia, M.; et al. Systemic pharmacokinetics and pharmacodynamics of intravitreal aflibercept, bevacizumab, and ranibizumab. Retina 2017, 37, 1847–1858. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Avery, R.L.; Castellarin, A.A.; Steinle, N.C.; Dhoot, D.S.; Pieramici, D.J.; See, R.; Couvillion, S.A.; Nasir, M.; Rabena, M.D.; Le, K.; et al. Systemic pharmacokinetics following intravitreal injections of ranibizumab, bevacizumab or aflibercept in patients with neovascular AMD. Br. J. Ophthalmol. 2014, 98, 1636–1641. [Google Scholar] [CrossRef] [PubMed]
- Hirano, T.; Toriyama, Y.; Iesato, Y.; Imai, A.; Murata, T. Changes in plasma vascular endothelial growth factor level after intravitreal injection of bevacizumab, aflibercept, or ranibizumab for diabetic macular edema. Retina 2018, 38, 1801–1808. [Google Scholar] [CrossRef]
- Avery, R.L. What is the evidence for systemic effects of intravitreal anti-VEGF agents, and should we be concerned? Br. J. Ophthalmol. 2013, 98, i7–i10. [Google Scholar] [CrossRef]
- Wells, J.A.; Glassman, A.R.; Ayala, A.R.; Jampol, L.M.; Bressler, N.M.; Bressler, S.B.; Brucker, A.J.; Ferris, F.L.; Hampton, G.R.; Jhaveri, C.; et al. Aflibercept, Bevacizumab, or Ranibizumab for Diabetic Macular Edema: Two-year results from a comparative effectiveness randomized clinical trial. Ophthalmology 2016, 123, 1351–1359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hykin, P.; Prevost, T.; Vasconcelos, J.C.; Murphy, C.; Kelly, J.; Ramu, J.; Hounsome, B.; Yang, Y.; Harding, S.P.; Lotery, A.; et al. Clinical Effectiveness of Intravitreal Therapy With Ranibizumab vs Aflibercept vs Bevacizumab for Macular Edema Secondary to Central Retinal Vein Occlusion. JAMA Ophthalmol. 2019, 137, 1256–1264. [Google Scholar] [CrossRef]
- Berg, K.; Hadzalic, E.; Gjertsen, I.; Forsaa, V.; Berger, L.H.; Kinge, B.; Henschien, H.; Fossen, K.; Markovic, S.; Pedersen, T.R.; et al. Ranibizumab or Bevacizumab for Neovascular Age-Related Macular Degeneration According to the Lucentis Compared to Avastin Study Treat-and-Extend Protocol. Ophthalmology 2016, 123, 51–59. [Google Scholar] [CrossRef]
- Sangroongruangsri, S.; Chaikledkaew, U.; Kumluang, S.; Wu, O.; Geue, C.; Ratanapakorn, T.; Leelahavarong, P.; Ingsrisawang, L.; Ruamviboonsuk, P.; Taweebanjongsin, W.; et al. Real-World Safety of Intravitreal Bevacizumab and Ranibizumab Treatments for Retinal Diseases in Thailand: A Prospective Observational Study. Clin. Drug Investig. 2018, 38, 853–865. [Google Scholar] [CrossRef] [Green Version]
- Chen, S.-N.; Lian, I.; Hwang, Y.-C.; Chen, Y.-H.; Chang, Y.-C.; Lee, K.-H.; Chuang, C.-C.; Wu, W.-C. Intravitreal anti-vascular endothelial growth factor treatment for retinopathy of prematurity: Comparison between ranibizumab and bevacizumab. Retina 2015, 35, 667–674. [Google Scholar] [CrossRef] [Green Version]
- Hanhart, J.; Comaneshter, D.S.; Vinker, S. Mortality after a cerebrovascular event in age-related macular degeneration patients treated with bevacizumab ocular injections. Acta Ophthalmol. 2018, 96, e732–e739. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maloney, M.H.; Schilz, S.R.; Herrin, J.; Sangaralingham, L.R.; Shah, N.D.; Barkmeier, A.J. Risk of Systemic Adverse Events Associated with Intravitreal Anti–VEGF Therapy for Diabetic Macular Edema in Routine Clinical Practice. Ophthalmology 2018, 126, 1007–1015. [Google Scholar] [CrossRef] [PubMed]
- Dalvin, L.A.; Starr, M.R.; AbouChehade, J.E.; Damento, G.M.; Garcia, M.; Shah, S.M.; Hodge, D.O.; Meissner, I.; Bakri, S.J.; Iezzi, R. Association of Intravitreal Anti–Vascular Endothelial Growth Factor Therapy With Risk of Stroke, Myocardial Infarction, and Death in Patients With Exudative Age-Related Macular Degeneration. JAMA Ophthalmol. 2019, 137, 483–490. [Google Scholar] [CrossRef] [PubMed]
- Hsiao, F.-C.; Lin, C.-P.; Tung, Y.-C.; Wu, C.-T.; Chu, P.-H. Major adverse limb events in type 2 diabetes patients receiving glucagon-like peptide-1 receptor agonists versus sodium-glucose cotransporter 2 inhibitors: A retrospective multi-institutional study. Diabetes Res. Clin. Pract. 2021, 180, 109076. [Google Scholar] [CrossRef]
- Shao, S.; Chan, Y.; Yang, Y.K.; Lin, S.; Hung, M.; Chien, R.; Lai, C.; Lai, E.C. The Chang Gung Research Database—A multi-institutional electronic medical records database for real-world epidemiological studies in Taiwan. Pharmacoepidemiol. Drug Saf. 2019, 28, 593–600. [Google Scholar] [CrossRef]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- McCaffrey, D.F.; Griffin, B.A.; Almirall, D.; Slaughter, M.E.; Ramchand, R.; Burgette, L.F. A tutorial on propensity score estimation for multiple treatments using generalized boosted models. Stat. Med. 2013, 32, 3388–3414. [Google Scholar] [CrossRef] [Green Version]
- Chung, Y.-R.; Kim, Y.H.; Byeon, H.-E.; Jo, D.H.; Kim, J.H.; Lee, K. Effect of a Single Intravitreal Bevacizumab Injection on Proteinuria in Patients With Diabetes. Transl. Vis. Sci. Technol. 2020, 9, 4. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, M.; Alouch, N.; Ahmed, A.; Jagadesh, S.K. Worsening of renal function and uncontrolled hypertension from intravitreal bevacizumab injections. Bayl. Univ. Med. Cent. Proc. 2021, 34, 527–529. [Google Scholar] [CrossRef]
- Glassman, A.R.; Liu, D.; Jampol, L.M.; Sun, J.K.; and Diabetic Retinopathy Clinical Research Network. Changes in Blood Pressure and Urine Albumin-Creatinine Ratio in a Randomized Clinical Trial Comparing Aflibercept, Bevacizumab, and Ranibizumab for Diabetic Macular Edema. Investig. Opthalmol. Vis. Sci. 2018, 59, 1199–1205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shye, M.; Hanna, R.M.; Patel, S.S.; Tram-Tran, N.; Hou, J.; McCannel, C.; Khalid, M.; Hanna, M.; Abdelnour, L.; Kurtz, I. Worsening proteinuria and renal function after intravitreal vascular endothelial growth factor blockade for diabetic proliferative retinopathy. Clin. Kidney J. 2020, 13, 969–980. [Google Scholar] [CrossRef] [PubMed]
- International Diabetes Federation. IDF Diabetes Atlas Eighth Edition 2017; International Diabetes Federation: Brussels, Belgium, 2017. [Google Scholar]
- Modjtahedi, B.S.; Wu, J.; Luong, T.Q.; Gandhi, N.K.; Fong, D.S.; Chen, W. Severity of Diabetic Retinopathy and the Risk of Future Cerebrovascular Disease, Cardiovascular Disease, and All-Cause Mortality. Ophthalmology 2020, 128, 1169–1179. [Google Scholar] [CrossRef] [PubMed]
- Austin, P.C.; Lee, D.S.; Fine, J.P. Introduction to the Analysis of Survival Data in the Presence of Competing Risks. Circulation 2016, 133, 601–609. [Google Scholar] [CrossRef]
- Berry, S.D.; Ngo, L.; Samelson, E.J.; Kiel, D.P. Competing Risk of Death: An Important Consideration in Studies of Older Adults. J. Am. Geriatr. Soc. 2010, 58, 783–787. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hurwitz, H.; Fehrenbacher, L.; Novotny, W.; Cartwright, T.; Hainsworth, J.; Heim, W.; Berlin, J.; Baron, A.; Griffing, S.; Holmgren, E.; et al. Bevacizumab plus Irinotecan, Fluorouracil, and Leucovorin for Metastatic Colorectal Cancer. N. Engl. J. Med. 2004, 350, 2335–2342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maloney, M.H.; Payne, S.R.; Herrin, J.; Sangaralingham, L.R.; Shah, N.D.; Barkmeier, A.J. Risk of Systemic Adverse Events after Intravitreal Bevacizumab, Ranibizumab, and Aflibercept in Routine Clinical Practice. Ophthalmology 2020, 128, 417–424. [Google Scholar] [CrossRef]
- Ntjam, N.N.; Thulliez, M.; Paintaud, G.; Salvo, F.; Angoulvant, D.; Pisella, P.-J.; Bejan-Angoulvant, T. Cardiovascular Adverse Events With Intravitreal Anti–Vascular Endothelial Growth Factor Drugs: A Systematic Review and Meta-analysis of Randomized Clinical Trials. JAMA Ophthalmol. 2021, 139, 610. [Google Scholar] [CrossRef]
- Amoaku, W.M.; Chakravarthy, U.; Gale, R.; Gavin, M.; Ghanchi, F.; Gibson, J.M.; Harding, S.P.; Johnston, R.L.; Kelly, S.P.; Lotery, A.J.; et al. Defining response to anti-VEGF therapies in neovascular AMD. Eye 2015, 29, 721–731. [Google Scholar] [CrossRef]
- Reibaldi, M.; Fallico, M.; Avitabile, T.; Marolo, P.; Parisi, G.; Cennamo, G.; Furino, C.; Lucenteforte, E.; Virgili, G. Frequency of Intravitreal Anti-Vascular Endothelial Growth Factor Injections and Risk of Death: A systematic review with meta-analysis. Ophthalmol. Retin. 2021, 6, 369–376. [Google Scholar] [CrossRef] [PubMed]
- Sheu, S.-J.; Cheng, C.-K.; Kuo, H.-K.; Tsai, C.-Y.; Lin, T.-C.; Tan, J.; Chandwani, H.; Adena, M.; Chen, S.-J. Treatment patterns in diabetic macular edema in Taiwan: A retrospective chart review. Clin. Ophthalmol. 2018, 12, 2189–2198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chou, Y.-B.; Chen, M.-J.; Lin, T.-C.; Chen, S.-J.; Hwang, D.-K. Priority options of anti-vascular endothelial growth factor agents in wet age-related macular degeneration under the National Health Insurance Program. J. Chin. Med. Assoc. 2019, 82, 659–664. [Google Scholar] [CrossRef]
- Ramachandran, A. Know the signs and symptoms of diabetes. Indian J. Med. Res. 2014, 140, 579–581. [Google Scholar] [PubMed]
- Shah, A.R.; Van Horn, A.N.; Verchinina, L.; Wichorek, M.; Su, L.; Markel, D.; Gardner, T.W. Blood Pressure Is Associated with Receiving Intravitreal Anti–Vascular Endothelial Growth Factor Treatment in Patients with Diabetes. Ophthalmol. Retin. 2019, 3, 410–416. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | Total (n = 3040) | Bevacizumab (n = 1477) | Ranibizumab (n = 1056) | Aflibercept (n = 507) | MASD |
|---|---|---|---|---|---|
| Male | 57.4 | 57.6 | 59.1 | 54.6 | 0.09 |
| Age, years | 62.2 ± 11.8 | 61.4 ± 12.3 | 62.2 ± 11.6 | 63.2 ± 11.3 | 0.15 |
| Age ≥ 65 years | 41.1 | 38.1 | 42.0 | 44.0 | 0.12 |
| Number of injections during 6 month follow up | 3.1 ± 2.3 | 1.7 ± 1.1 | 4.2 ± 2.4 | 3.6 ± 2.2 | 0.90 |
| BMI, kg/m2 * | 25.8 ± 4.1 | 25.8 ± 4.1 | 25.8 ± 4.1 | 25.8 ± 3.9 | 0.01 |
| Diabetes severity | |||||
| HbA1c,% | 7.7 ± 1.6 | 7.8 ± 1.8 | 7.6 ± 1.5 | 7.6 ± 1.5 | 0.12 |
| Diabetic duration, years | 6.6 ± 5.7 | 6.8 ± 5.7 | 6.4 ± 5.7 | 6.7 ± 5.8 | 0.07 |
| Diabetic duration grouping | 0.04 | ||||
| <5 years | 47.7 | 47.1 | 49.0 | 46.8 | |
| 5–10 years | 21.1 | 20.9 | 19.7 | 23.1 | |
| >10 years | 31.2 | 32.0 | 31.2 | 30.0 | |
| Diabetic neuropathy | 33.3 | 36.0 | 32.5 | 30.8 | 0.05 |
| Diabetic foot ulcer | 3.9 | 4.2 | 3.4 | 4.3 | 0.11 |
| Type of diabetes | 0.10 | ||||
| Type 1 | 3.9 | 4.8 | 4.0 | 2.7 | |
| Type 2 | 96.1 | 95.2 | 96.0 | 97.3 | |
| Comorbidity | |||||
| Dyslipidemia | 51.7 | 52.4 | 50.3 | 52.5 | 0.05 |
| Hypertension | 60.6 | 64.0 | 59.8 | 57.0 | 0.14 |
| Ischemic heart disease | 15.3 | 17.4 | 14.7 | 13.3 | 0.11 |
| Chronic kidney disease | 42.2 | 47.0 | 42.2 | 35.7 | 0.23 |
| Stroke | 6.4 | 8.0 | 6.2 | 4.6 | 0.13 |
| Heart failure hospitalization | 3.4 | 4.5 | 3.1 | 2.5 | 0.10 |
| Myocardial infarction | 3.4 | 3.6 | 3.6 | 2.8 | 0.05 |
| Atrial fibrillation | 2.8 | 3.2 | 2.1 | 3.2 | 0.07 |
| Chronic obstructive pulmonary disease | 8.1 | 8.9 | 6.8 | 9.0 | 0.08 |
| Obstructive sleep apnea | 4.6 | 4.4 | 3.7 | 6.1 | 0.12 |
| Charlson’s Comorbidity Index score | 3.6 ± 1.9 | 3.8 ± 2.0 | 3.6 ± 1.9 | 3.5 ± 1.7 | 0.12 |
| Medication use | |||||
| Anti-platelet | 23.7 | 25.4 | 22.0 | 23.8 | 0.08 |
| Anti-coagulant | 1.7 | 1.9 | 1.3 | 2.1 | 0.06 |
| Statins | 36.5 | 37.7 | 36.2 | 35.4 | 0.05 |
| Fibrates | 3.4 | 3.6 | 3.0 | 3.5 | 0.03 |
| Ocular history | |||||
| Glaucoma | 4.0 | 4.7 | 3.0 | 4.6 | 0.08 |
| Age-related macular degeneration | 26.8 | 23.4 | 25.2 | 33.8 | 0.24 |
| Diabetic macular edema | 43.3 | 39.7 | 45.3 | 45.4 | 0.12 |
| Retinal vascular occlusion | 6.7 | 6.5 | 7.1 | 6.6 | 0.03 |
| Vitreous hemorrhage | 20.3 | 25.0 | 18.7 | 16.0 | 0.22 |
| Myopic choroidal neovascularization | 1.9 | 1.3 | 2.2 | 2.2 | 0.07 |
| All grade diabetic retinopathy | 71.6 | 72.4 | 76.1 | 64.4 | 0.27 |
| Received retinal laser | 38.6 | 40.6 | 41.5 | 31.7 | 0.20 |
| Received vitrectomy | 6.3 | 6.5 | 6.5 | 5.6 | 0.04 |
| No. of outpatient visits at ophthalmology in the previous year | 3.9 ± 3.5 | 3.6 ± 3.5 | 4.1 ± 3.6 | 3.9 ± 3.3 | 0.14 |
| Incidence (95% CI) * | aHR (95%CI)/aSHR (95%CI) | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Outcome | Bevacizumab | Ranibizumab | Aflibercept | Bevacizumab vs. Ranibizumab | p | Bevacizumab vs. Aflibercept | p | Ranibizumab vs. Aflibercept | p |
| Major adverse cardiac event | 1.99 (1.11–2.86) | 2.76 (1.80–3.71) | 1.23 (0.46–1.99) | 0.52 (0.29–0.94) | 0.032 | 0.96 (0.43–2.15) | 0.914 | 1.83 (0.88–3.79) | 0.106 |
| Myocardial infarction | 0.53 (0.07–0.99) | 0.71 (0.22–1.20) | 0.31 (−0.08–0.70) | 0.41 (0.11–1.63) | 0.208 | 0.58 (0.14–2.45) | 0.460 | 1.41 (0.53–3.73) | 0.495 |
| Ischemic stroke | 0.92 (0.32–1.53) | 1.65 (0.91–2.40) | 0.61 (0.06–1.16) | 0.36 (0.16–0.82) | 0.015 | 0.73 (0.22–2.45) | 0.606 | 2.01 (0.75–5.38) | 0.165 |
| Cardiovascular death | 0.86 (0.29–1.44) | 0.44 (0.06–0.81) | 0.34 (−0.06–0.73) | 1.48 (0.47–4.66) | 0.508 | 1.89 (0.41–8.80) | 0.415 | 1.29 (0.26–6.31) | 0.758 |
| MALE outcome † | 2.95 (1.86–4.04) | 2.00 (1.18–2.82) | 0.74 (0.14–1.34) | 1.21 (0.69–2.14) | 0.504 | 3.24 (1.20–8.78) | 0.021 | 2.67 (1.05–6.79) | 0.039 |
| Composite thromboembolic events ‡ | 2.16 (1.23–3.09) | 2.53 (1.60–3.45) | 1.48 (0.63–2.33) | 0.65 (0.34–1.24) | 0.190 | 0.84 (0.38–1.88) | 0.678 | 1.30 (0.66–2.59) | 0.450 |
| Major bleeding | 12.1 (9.8–14.3) | 4.3 (3.1–5.5) | 3.8 (2.4–5.1) | 2.31 (1.63–3.27) | <0.001 | 2.27 (1.50–3.43) | <0.001 | 0.99 (0.62–1.56) | 0.948 |
| All-cause admission | 58.6 (53.3–63.9) | 27.6 (24.4–30.7) | 30.2 (26.2–34.2) | 1.76 (1.51–2.05) | <0.001 | 1.39 (1.16–1.65) | <0.001 | 0.79 (0.66–0.94) | 0.007 |
| All-cause death | 3.26 (2.14–4.37) | 0.55 (0.13–0.97) | 2.61 (1.50–3.72) | 5.53 (2.34–13.08) | <0.001 | 0.92 (0.51–1.67) | 0.795 | 0.17 (0.07–0.41) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kang, E.Y.-C.; Lin, T.-Y.; Garg, S.J.; Wang, N.-K.; Chen, L.-J.; Huang, P.-W.; Chan, M.-J.; Chen, K.-J.; Wu, W.-C.; Lai, C.-C.; et al. The Association of Intravitreal Injections of Different Anti-Vascular Endothelial Growth Factor with Systemic Outcomes in Diabetic Patients. J. Pers. Med. 2023, 13, 544. https://doi.org/10.3390/jpm13030544
Kang EY-C, Lin T-Y, Garg SJ, Wang N-K, Chen L-J, Huang P-W, Chan M-J, Chen K-J, Wu W-C, Lai C-C, et al. The Association of Intravitreal Injections of Different Anti-Vascular Endothelial Growth Factor with Systemic Outcomes in Diabetic Patients. Journal of Personalized Medicine. 2023; 13(3):544. https://doi.org/10.3390/jpm13030544
Chicago/Turabian StyleKang, Eugene Yu-Chuan, Tzu-Yi Lin, Sunir J. Garg, Nan-Kai Wang, Lee-Jen Chen, Pei-Wei Huang, Ming-Jen Chan, Kuan-Jen Chen, Wei-Chi Wu, Chi-Chun Lai, and et al. 2023. "The Association of Intravitreal Injections of Different Anti-Vascular Endothelial Growth Factor with Systemic Outcomes in Diabetic Patients" Journal of Personalized Medicine 13, no. 3: 544. https://doi.org/10.3390/jpm13030544