
The Severity of Pain in Prostate Biopsy Depends on the Biopsy Sector
 , , ,
, , ,
Abstract
:1. Introduction
2. Material and Methods
2.1. Study Design
2.2. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Carlsson, S.V.; Vickers, A.J. Screening for Prostate Cancer. Med. Clin. N. Am. 2020, 104, 1051–1062. [Google Scholar] [CrossRef]
- Culp, M.B.B.; Soerjomataram, I.; Efstathiou, J.A.; Bray, F.; Jemal, A. Recent Global Patterns in Prostate Cancer Incidence and Mortality Rates. Eur. Urol. 2020, 77, 38–52. [Google Scholar] [CrossRef]
- Kohaar, I.; Petrovics, G.; Srivastava, S. A rich array of prostate cancer molecular biomarkers: Opportunities and challenges. Int. J. Mol. Sci. 2019, 20, 1813. [Google Scholar] [CrossRef] [Green Version]
- Merriel, S.W.D.; Funston, G.; Hamilton, W. Prostate Cancer in Primary Care. Adv. Ther. 2018, 35, 1285–1294. [Google Scholar] [CrossRef] [Green Version]
- Rajwa, P.; Sprenkle, P.C.; Leapman, M.S. When and How Should Active Surveillance for Prostate Cancer Be De-Escalated? Eur. Urol. Focus 2021, 7, 297–300. [Google Scholar] [CrossRef] [PubMed]
- Weinreb, J.C.; Barentsz, J.O.; Choyke, P.L.; Cornud, F.; Haider, M.A.; Macura, K.J.; Margolis, D.; Schnall, M.D.; Shtern, F.; Tempany, C.M.; et al. PI-RADS Prostate Imaging—Reporting and Data System: 2015, Version 2. Eur. Urol. 2016, 69, 16–40. [Google Scholar] [CrossRef] [PubMed]
- Prostate Cancer between Prognosis and Adequate/Proper Therapy—PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/28255369/ (accessed on 11 November 2022).
- Jones, D.; Friend, C.; Dreher, A.; Allgar, V.; Macleod, U. The diagnostic test accuracy of rectal examination for prostate cancer diagnosis in symptomatic patients: A systematic review. BMC Fam. Pract. 2018, 19, 79. [Google Scholar] [CrossRef] [Green Version]
- Chuang, R.J.; Marks, L.S. Targeted and Systematic Biopsy for Diagnosis and Management of Prostate Cancer. Clin. Oncol. 2020, 32, 144–148. [Google Scholar] [CrossRef] [PubMed]
- Eldred-Evans, D.; Burak, P.; Connor, M.J.; Day, E.; Evans, M.; Fiorentino, F.; Gammon, M.; Hosking-Jervis, F.; Klimowska-Nassar, N.; McGuire, W.; et al. Population-Based Prostate Cancer Screening with Magnetic Resonance Imaging or Ultrasonography: The IP1-PROSTAGRAM Study. JAMA Oncol. 2021, 7, 395–402. [Google Scholar] [CrossRef] [PubMed]
- Kryvenko, O.N.; Epstein, J.I. Prostate cancer grading: A decade after the 2005 modified gleason grading system. Arch. Pathol. Lab. Med. 2016, 140, 1153–1156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Omer, A.; Lamb, A.D. Optimizing prostate biopsy techniques. Curr. Opin. Urol. 2019, 29, 578–586. [Google Scholar] [CrossRef] [PubMed]
- Eklund, M.; Jäderling, F.; Discacciati, A.; Bergman, M.; Annerstedt, M.; Aly, M.; Glaessgen, A.; Carlsson, S.; Grönberg, H.; Nordström, T. MRI-Targeted or Standard Biopsy in Prostate Cancer Screening. N. Engl. J. Med. 2021, 385, 908–920. [Google Scholar] [CrossRef] [PubMed]
- Giannarini, G.; Autorino, R.; Valent, F.; Mogorovich, A.; Manassero, F.; De Maria, M.; Morelli, G.; Barbone, F.; Di Lorenzo, G.; Selli, C. Combination of Perianal-Intrarectal Lidocaine-Prilocaine Cream and Periprostatic Nerve Block for Pain Control During Transrectal Ultrasound Guided Prostate Biopsy: A Randomized, Controlled Trial. J. Urol. 2009, 181, 585–593. [Google Scholar] [CrossRef]
- Nazir, B. Pain during transrectal ultrasound-guided prostate biopsy and the role of periprostatic nerve block: What radiologists should know. Korean J. Radiol. 2014, 15, 543–553. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garcia-Perdomo, H.A.; Mejia, N.G.; Fernandez, L.; Carbonell, J. Effectiveness of periprostatic block to prevent pain in transrectal prostate biopsy: A systematic review and a network meta-analysis. Cent. Eur. J. Urol. 2019, 72, 121–133. [Google Scholar] [CrossRef]
- Schober, P.; Schwarte, L.A. Correlation coefficients: Appropriate use and interpretation. Anesth. Analg. 2018, 126, 1763–1768. [Google Scholar] [CrossRef] [PubMed]
- Aus, G.; Hermansson, C.G.; Hugosson, J.; Pedersen, K.V. Transrectal Ultrasound Examination of the Prostate: Complications and Acceptance by Patients. Br. J. Urol. 1993, 71, 457–459. [Google Scholar] [CrossRef]
- Hiroš, M.; Selimović, M.; Spahović, H.; Sadović, S.; Spužic-Čelić, E. Transrectal ultrasound-guided prostate biopsy, periprostatic local anesthesia and pain tolerance. Bosn. J. Basic Med. Sci. 2010, 10, 68–72. [Google Scholar] [CrossRef] [Green Version]
- Inal, G.; Yazici, S.; Adsan, Ö.; Özturk, B.; Çetinkaya, M. Periprostatic nerve blockade before transrectal ultrasound-guided prostate biopsy: The Ankara numune experience. Urol. Int. 2003, 71, 165–167. [Google Scholar] [CrossRef]
- Vaidya, A.; Soloway, M.S. Periprostatic local anesthesia before ultrasound-guided prostate biopsy: An update of the Miami experience. Eur. Urol. 2001, 40, 135–138. [Google Scholar] [CrossRef]
- Nakai, Y.; Tanaka, N.; Matsubara, T.; Anai, S.; Miyake, M.; Hori, S.; Fujii, T.; Ohbayashi, C.; Fujimoto, K. Effect of prolonged duration of transrectal ultrasound-guided biopsy of the prostate and pre-procedure anxiety on pain in patients without anesthesia. Res. Rep. Urol. 2021, 13, 111–120. [Google Scholar] [CrossRef]
- Bastide, C.; Lechevallier, E.; Eghazarian, C.; Ortega, J.C.; Coulange, C. Tolerance of pain during transrectal ultrasound-guided biopsy of the prostate: Risk factors. Prostate Cancer Prostatic Dis. 2003, 6, 239–241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, S.J.; Lee, J.; An, D.H.; Park, C.H.; Lim, J.H.; Kim, H.G.; Park, J.Y. A randomized controlled comparison between periprostatic nerve block and pelvic plexus block at the base and apex of 14-core prostate biopsies. World J. Urol. 2019, 37, 2663–2669. [Google Scholar] [CrossRef]
- Moussa, A.S.; Meshref, A.; Schoenfield, L.; Masoud, A.; Abdel-Rahman, S.; Li, J.; Flazoura, S.; Magi-Galluzzi, C.; Fergany, A.; Fareed, K.; et al. Importance of Additional “Extreme” Anterior Apical Needle Biopsies in the Initial Detection of Prostate Cancer. Urology 2010, 75, 1034–1039. [Google Scholar] [CrossRef] [PubMed]
- Yoo, J.W.; Koo, K.C.; Chung, B.H.; Lee, K.S. Efficacy of additional periprostatic apex nerve block on pain in each of 12 transrectal prostate core biopsies: A retrospective study. BMC Urol. 2021, 21, 132. [Google Scholar] [CrossRef] [PubMed]
- Yoo, J.W.; Koo, K.C.; Chung, B.H.; Lee, K.S. Pain control according to the periprostatic nerve block site in magnetic resonance imaging/transrectal targeted prostate biopsy. Sci. Rep. 2022, 12, 772. [Google Scholar] [CrossRef]
- Meng, M.V.; Franks, J.H.; Presti, J.C.; Shinohara, K. The utility of apical anterior horn biopsies in prostate cancer detection. Urol. Oncol. Semin. Orig. Investig. 2003, 21, 361–365. [Google Scholar] [CrossRef]
- Chesnut, G.T.; Zareba, P.; Sjoberg, D.D.; Mamoor, M.; Carlsson, S.; Lee, T.; Fainberg, J.; Vertosick, E.; Manasia, M.; Schoen, M.; et al. Patient-reported pain, discomfort, and anxiety during magnetic resonance imaging-targeted prostate biopsy. Can. Urol. Assoc. J. 2019, 14, E202–E208. [Google Scholar] [CrossRef]
- Urologia Polska 2006/59/3—Ocena Nasilenia Bólu Występującego We Wczesnym Okresie Po Biopsji Rdzeniowej Stercza, Wykonanej Pod Kontrolą Ultrasonografii Przezodbytniczej. Available online: http://www.urologiapolska.pl/artykul.php?3032 (accessed on 11 September 2022).
- Saraçǧlu, T.; Ünsal, A.; Taşkin, F.; Sevinçok, L.; Karaman, C.Z. The impact of pre-procedural waiting period and anxiety level on pain perception in patients undergoing transrectal ultrasound-guided prostate biopsy. Diagn. Interv. Radiol. 2012, 18, 195–199. [Google Scholar] [CrossRef] [Green Version]
- Rodriguez, A.; Kyriakou, G.; Leray, E.; Lobel, B.; Guillé, F. Prospective study comparing two methods of anaesthesia for prostate biopsies: Apex periprostatic nerve block versus intrarectal lidocaine gel: Review of the literature. Eur. Urol. 2003, 44, 195–200. [Google Scholar] [CrossRef]
- Leibovici, D.; Zisman, A.; Siegel, Y.I.; Sella, A.; Kleinmann, J.; Lindner, A. Local anesthesia for prostate biopsy by periprostatic lidocaine injection: A double-blind placebo controlled study. J. Urol. 2002, 167, 563–565. [Google Scholar] [CrossRef] [PubMed]
- Han, K.S.; Lee, K.H. Factors influencing pain during transrectal ultrasonography-guided prostate biopsy. Prostate Cancer Prostatic Dis. 2008, 11, 139–142. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Median | Mean | SD |
|---|---|---|---|
| Age (years) | 66.4 | 65.6 | 7.4 |
| Prostate volume (mL) | 50.0 | 52.7 | 24.9 |
| PSA (ng/mL) | 7.6 | 9.7 | 10.1 |
| PSAD (ng/mL2) | 0.16 | 0.23 | 0.24 |
| Biopsy time (min) | 30.0 | 31.3 | 18.8 |
| Target diameter (mm) | 14.0 | 13.5 | 6.0 |
| Number of cores | 14.0 | 13.7 | 3.0 |
| Variable | n | Median | IQR | p |
|---|---|---|---|---|
| Prostate area | ||||
| posterior | 81 | 2.00 | 1.00–4.00 | 0.099 a |
| anterior | 62 | 1.00 | 1.00–2.00 | |
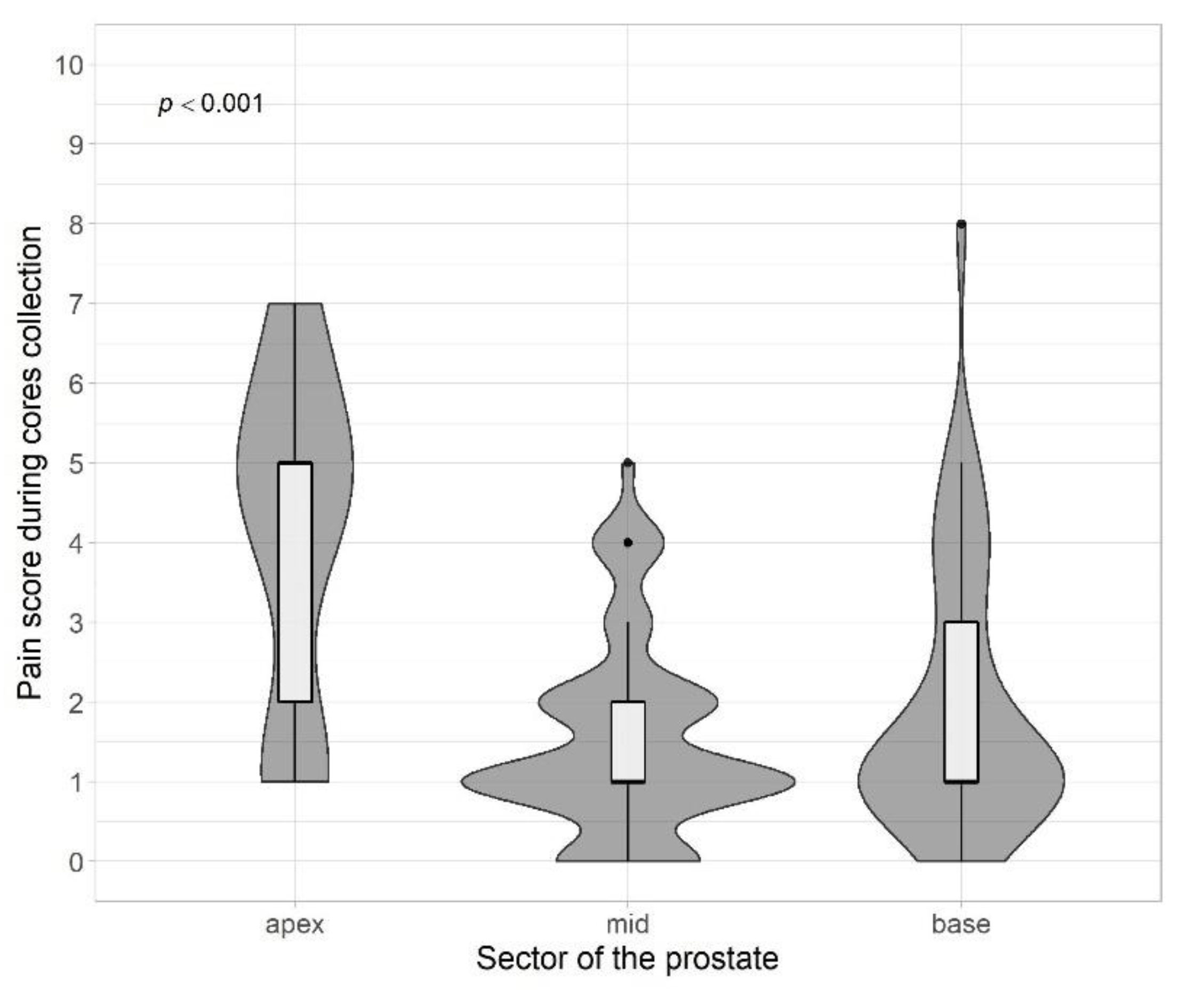
| Target localisation level | ||||
| Apex | 34 | 5.00 | 2.00–5.00 | <0.001 b |
| Mid | 66 | 1.00 | 1.00–2.00 | |
| Base | 43 | 1.00 | 1.00–3.00 | |
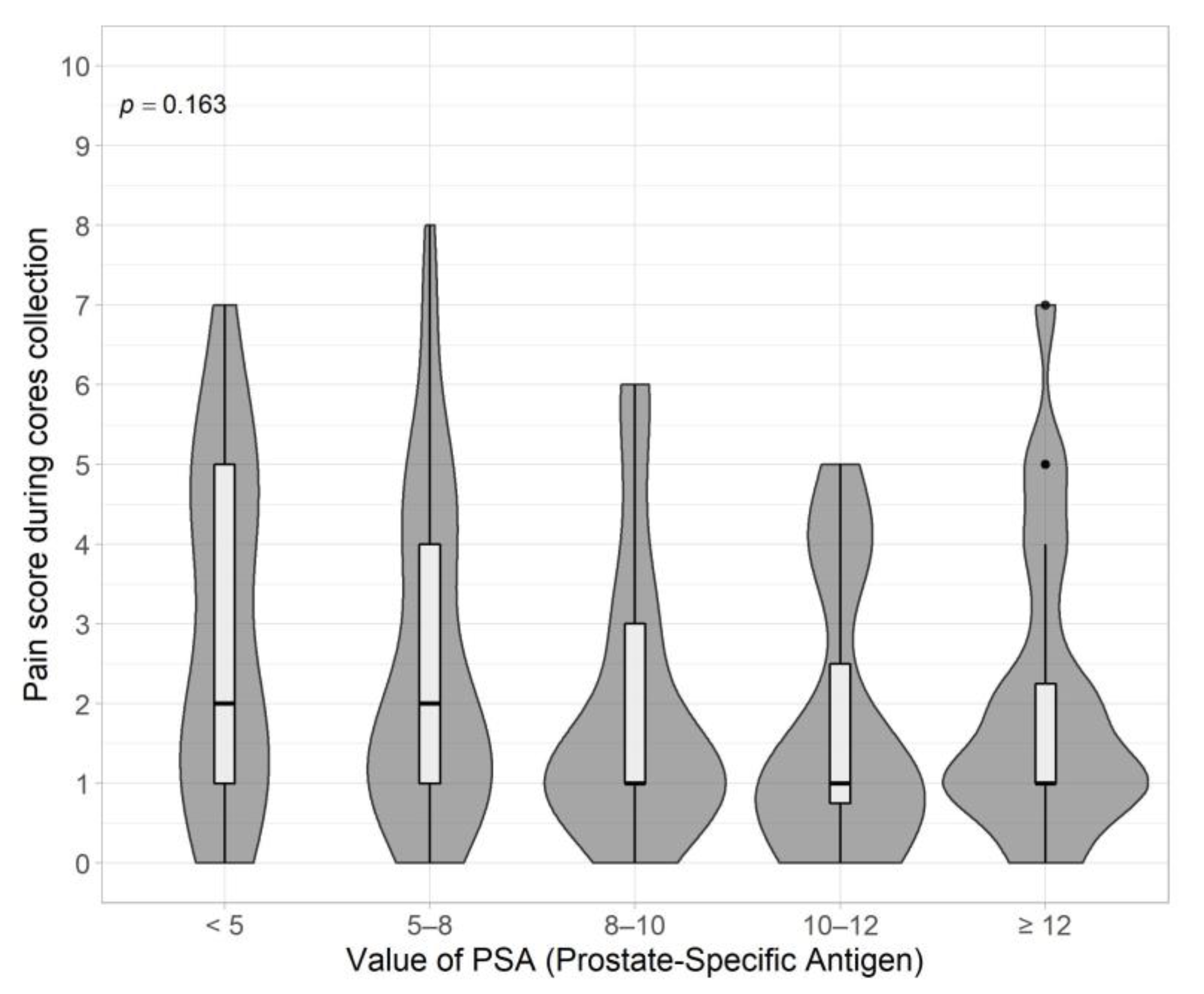
| PSA | ||||
| <5 | 20 | 2.00 | 1.00–5.00 | 0.163 b |
| 5–8 | 54 | 2.00 | 1.00–4.00 | |
| 8–10 | 25 | 1.00 | 1.00–3.00 | |
| 10–12 | 16 | 1.00 | 0.75–2.50 | |
| ≥12 | 24 | 1.00 | 1.00–2.25 | |
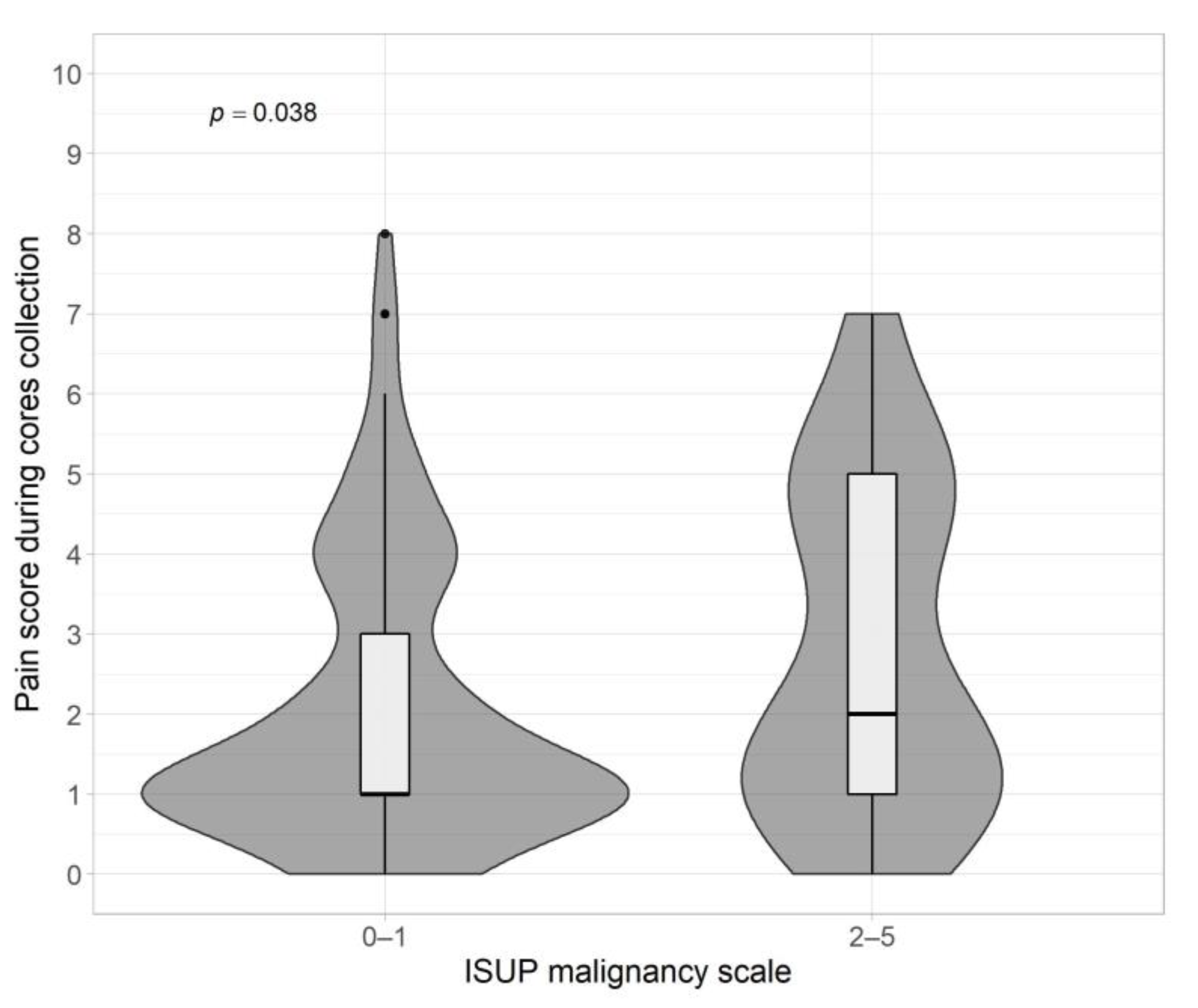
| ISUP | ||||
| 0–1 | 102 | 1.00 | 1.00–3.00 | 0.038 a |
| 2–5 | 41 | 2.00 | 1.00–5.00 | |
| PI-RADS | ||||
| 2 | 9 | 2.00 | 1.00–5.00 | 0.42 b |
| 3 | 22 | 1.00 | 1.00–2.00 | |
| 4 | 69 | 1.00 | 1.00–4.00 | |
| 5 | 42 | 1.50 | 1.00–4.00 | |
| Number of cores | ||||
| <10 | 12 | 1.00 | 0.00–4.25 | 0.74 b |
| 10–15 | 74 | 2.00 | 1.00–4.00 | |
| >15 | 57 | 1.00 | 1.00–4.00 | |
| Prostate volume | ||||
| <30 | 21 | 2.00 | 1.00–5.00 | 0.47 b |
| 30–60 | 59 | 2.00 | 1.00–4.00 | |
| 60–100 | 37 | 1.00 | 1.00–4.00 | |
| ≥100 | 5 | 1.00 | 1.00–1.00 |
| Variable | p-Value | r |
|---|---|---|
| Age | 0.65 | −0.04 |
| Time of biopsy (affect the feeling of discomfort) | 0.038 | 0.19 |
| Target diameter | 0.29 | −0.10 |
| PI-RADS | 0.86 | −0.02 |
| ISUP (2–5) | 0.29 | 0.09 |
| PSA | 0.046 | −0.17 |
| Number of cores | 0.56 | 0.05 |
| Prostate volume | 0.22 | −0.11 |
| Anxiety | 0.38 | 0.07 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rempega, G.; Rajwa, P.; Kępiński, M.; Ryszawy, J.; Wojnarowicz, J.; Kowalik, M.; Krzempek, M.; Krzywon, A.; Dobrakowski, M.; Paradysz, A.; et al. The Severity of Pain in Prostate Biopsy Depends on the Biopsy Sector. J. Pers. Med. 2023, 13, 431. https://doi.org/10.3390/jpm13030431
Rempega G, Rajwa P, Kępiński M, Ryszawy J, Wojnarowicz J, Kowalik M, Krzempek M, Krzywon A, Dobrakowski M, Paradysz A, et al. The Severity of Pain in Prostate Biopsy Depends on the Biopsy Sector. Journal of Personalized Medicine. 2023; 13(3):431. https://doi.org/10.3390/jpm13030431
Chicago/Turabian StyleRempega, Grzegorz, Paweł Rajwa, Michał Kępiński, Jakub Ryszawy, Jakub Wojnarowicz, Maksymilian Kowalik, Marcela Krzempek, Aleksandra Krzywon, Michał Dobrakowski, Andrzej Paradysz, and et al. 2023. "The Severity of Pain in Prostate Biopsy Depends on the Biopsy Sector" Journal of Personalized Medicine 13, no. 3: 431. https://doi.org/10.3390/jpm13030431