

Psychometric Properties of Suboptimal Health Status Instruments: A Systematic Review

 , , , and
, , , and
Abstract
:1. Introduction
- What instruments are available to measure SHS for different segments of populations?
- What are the key strengths and weaknesses of measures used to assess SHS in target populations?
- To what extent have the psychometric properties of these SHS instruments been evaluated for use in target populations?
- What are the current gaps in generating conclusive evidence about the psychometric properties of these tools in different populations?
2. Materials and Methods
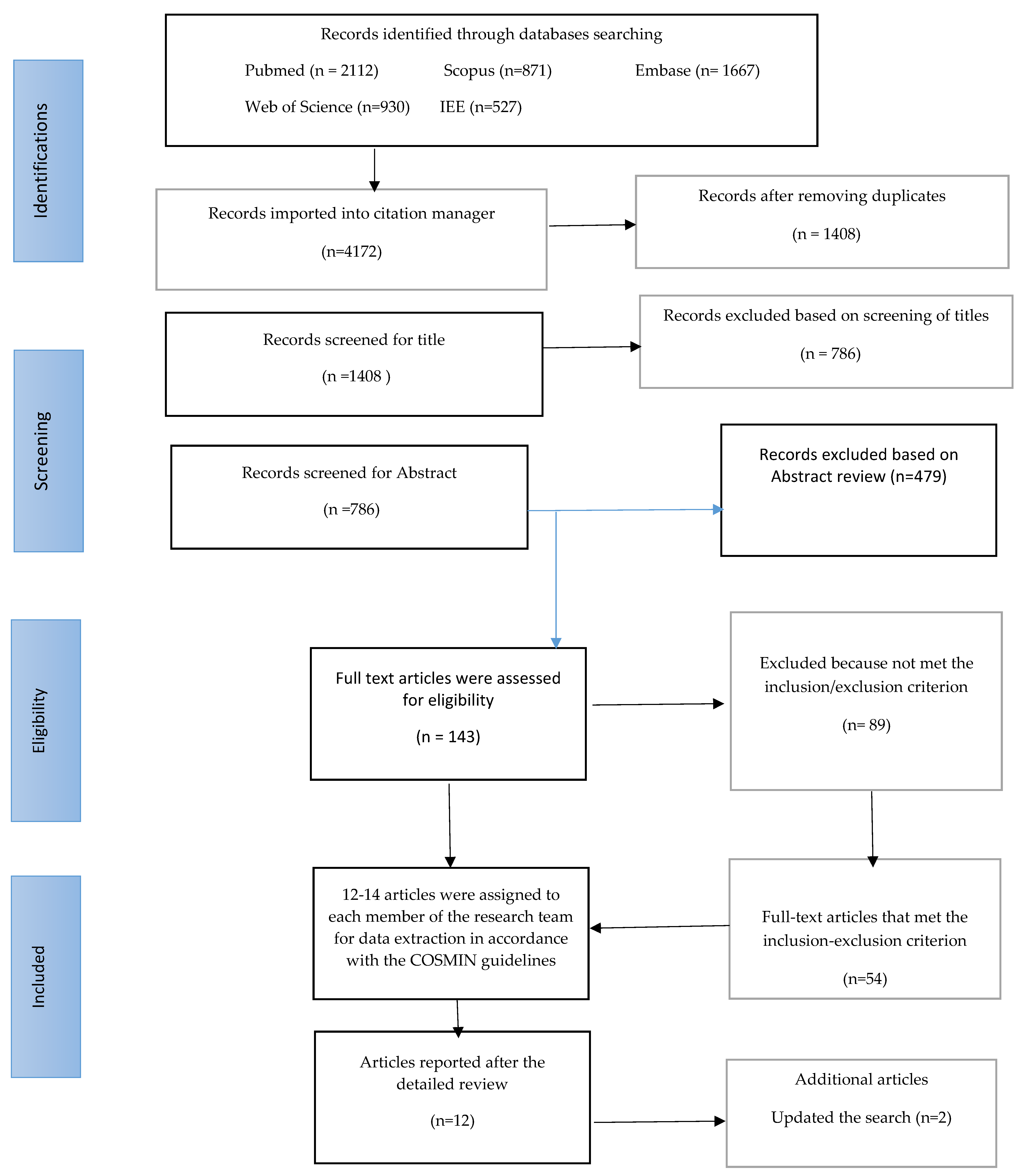
2.1. Search Strategy and Filters
2.2. Evaluation of Articles
2.3. Methodological Quality Assessment
3. Results
3.1. Suboptimal Health Status Questionnaire-25 (SHSQ-25)
3.1.1. Description of the SHSQ-25
3.1.2. Scoring System for the SHSQ-25
3.1.3. Reliability and Validity Indicators of the SHSQ-25
3.2. Sub-Health Measurement Scale V1.0 (SHMS V1.0)
3.2.1. Description of the SHS V1.0
3.2.2. Scoring System for the SHMS V1.0
3.2.3. Reliability and Validity Indicators of the SHMS V 1.0

{kind=link}
| Instrument | Authors and Year | Sample Size | Reliability | Validity | |
|---|---|---|---|---|---|
| Internal Consistency | Test–Retest Reliability | ||||
| SHSQ-25 | Yan et al. (2009) [4] | 3000 adults | Cronbach’s α 0.93, item-sub-scale correlations 0.51–0.72 | Range (0.89–0.98) | Content validity KMO = 0.93 Bartlett test < 0.001 |
| Wang and Yan (2012) [15] | 3405 individuals | Cronbach’s α = 0.91 | Not Reported | Not Reported | |
| Adua, et al. (2021) [28] | 263 healthy adults | Cronbach range 0.7–0.9 Cronbach’s α for sub-scales: Fatigue = 0.846, Immune-cardiovascular = 0.820, Cognitive = 0.846 | Not Reported | Construct validity > 0.7 thresholds Convergent and discriminant validity on sub-scales: Fatigue (AVE = 0.366, MSV = 0.70) Cognitive (AVE = 0.358, MSV = 0.67). Immune-cardiovascular (AVE = 0.537, MSV = 0.185). | |
| Guo, Z. et al. (2022) [30] | 460 healthy adults | Cronbach’s α of 0.953 and Cronbach’s α for each domain ranged from 0.76 to 0.94 | Range (0.88–0.99) | Root mean square error of approximation (RMSEA) = 0.069 < 0.08 Adjusted goodness of fit index (AGFI) = 0.907 > 0.90 | |
| SHMS V 1.0 | Xu et al. (2011) [31] | 2000 individuals | Cronbach α = 0.92, split-half reliability = 0.83 | 0.64 | Correlation coefficient between SHMS V1.0 and SF-36 was 0.664 (p < 0.001). |
| Wu et al. (2016) [38] | 24,475 individuals | Cronbach’s α = 0.91, Cronbach’s α for three dimensions range 0.82–0.85 | Not Reported | Not Reported | |
| Lolokote et al. (2017) [36] | 829 college students | Cronbach’s α = 0.89, sub-scale alpha range 0.71–0.85 | Not Reported | Not Reported | |
| Ma et al. (2020) [41] | 5233 university students | Cronbach’s α = 0.68 | Not Reported | Not Reported | |
| Miao et al. (2021) [40] | 2640 individuals | Cronbach’s α = 0.92, Cronbach’s α on sub-scales: Physical sub-health = 0.85, Psychological sub-health = 0.87, Social adaptation sub-health = 0.89 | 0.67 | Correlation between dimensional range between 0.65 and 0.87 Correlation between SHMS v1.0 and Short Form-36 (SF-36) = 0.67 Correlation between SHMS v1.0 and SF-36 was 0.78 | |
3.3. Multidimensional Sub-Health Questionnaire of Adolescents (MSQA)
3.3.1. Description of the MSQA
3.3.2. Scoring System for the MSQA
3.3.3. Reliability and Validity Indicators of the MSQA
| Instrument | Authors and Year | Sample Size | Reliability | Validity | |
|---|---|---|---|---|---|
| Internal Consistency | Test-Retest Reliability | ||||
| MSQA | Tao et al. (2008) [47] | 7104 middle school student | Cronbach’s α = 0.96, split-half reliability = 0.94 | 0.86 | SCL-90 = 0.63 and CMI the criterion-related validity = 0.64 |
| Yao et al. (2015) [33] | 5249 students from university and high school students | Cronbach’s α = 0.96, split-half reliability coefficient = 0.94 | 0.87 | Not Reported | |
| Huang et al. (2022) [44] | 778 minors (<18 years old) | Cronbach’s α = 0.96 | Not Reported | Not Reported | |
| Tang et al. (2021) [43] | 15,713 students | Cronbach’s α = 0.95 | Not Reported | Not Reported | |
| SSS | [Bi, Jl., 2019] [42] | 6232 students | Cronbach’s α of the total scale = 0.942, Cronbach’s α for sub-scales: Physiological = 0.915, Psychological = 0.856, and Social 0.850 | Not Reported | Correlation between dimension: Physiological = 0.929, Psychological = 0.803, and Social 0.774 Bartlett test < 0.001 KMO = 0.94 |
3.4. Sub-Health Self-Rating Scale (SSS)
3.4.1. Description of the SSS
3.4.2. Scoring System for SSS Measures
3.4.3. Reliability and Validity Indicators of the SSS
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Boorse, C. Health as a Theoretical Concept. Philos. Sci. 1977, 44, 542–573. [Google Scholar]
- Misselbrook, D. W is for Wellbeing and the WHO definition of health. Br. J. Gen. Pract. 2014, 64, 582. [Google Scholar]
- Zhang, Y.; Shao, J. A systemic review of suboptimal health. Glob. J. Public Health 2015, 2, 20. [Google Scholar]
- Yan, Y.-X.; Liu, Y.-Q.; Li, M.; Hu, P.-F.; Guo, A.-M.; Yang, X.-H.; Qiu, J.-J.; Yang, S.-S.; Shen, J.; Zhang, L.-P.; et al. Development and Evaluation of a Questionnaire for Measuring Suboptimal Health Status in Urban Chinese. J. Epidemiol. 2009, 19, 333–341. [Google Scholar]
- Yang, Z.M.; Yang, X.B.; Huang, L. A literature review on the conceptual framework of sub-health. Zhongguo Zhong Xi Yi Jie He Za Zhi 2010, 30, 757–763. (In Chinese) [Google Scholar]
- Ge, S.; Xu, X.; Zhang, J.; Hou, H.; Wang, H.; Liu, D.; Zhang, X.; Song, M.; Li, D.; Zhou, Y.; et al. Suboptimal health status as an independent risk factor for type 2 diabetes mellitus in a community-based cohort: The China suboptimal health cohort study. EPMA J. 2019, 10, 65–72. [Google Scholar] [CrossRef]
- Leonardi, F. The Definition of Health: Towards New Perspectives. Int. J. Health Serv. 2018, 48, 735–748. [Google Scholar]
- Feng, L.Y.; Xu, J.; Luo, R.; Qiu, J.; Zhang, J. Analysis and build-up for sub-health evaluating indicator system. Chin. Gen. Pract. 2011, 14, 37–40. [Google Scholar]
- JChen, J.; Xiang, H.; Jiang, P.; Yu, L.; Jing, Y.; Li, F.; Wu, S.; Fu, X.; Liu, Y.; Kwan, H.; et al. The Role of Healthy Lifestyle in the Implementation of Regressing Suboptimal Health Status among College Students in China: A Nested Case-Control Study. Int. J. Environ. Res. Public Health 2017, 14, 240. [Google Scholar]
- Algahtani, F.D.; Hassan, S.-u.-N.; Alsaif, B.; Zrieq, R. Assessment of the Quality of Life during COVID-19 Pandemic: A Cross-Sectional Survey from the Kingdom of Saudi Arabia. Int. J. Environ. Res. Public Health 2021, 18, 847. [Google Scholar] [CrossRef]
- Kontodimopoulos, N.; Poulaki, E.; Fanourgiakis, J.; Talias, M.A. The Association between Fear of COVID-19 and Health-Related Quality of Life: A Cross-Sectional Study in the Greek General Population. J. Pers. Med. 2022, 12, 1891. [Google Scholar]
- Zhu, R. Clinical guidelines of Chinese medicine on sub-health. Chin. Med. Mod. Distance Educ. China 2009, 7, 5–6. [Google Scholar]
- Wang, Y.; Ge, S.; Yan, Y.; Wang, A.; Zhao, Z.; Yu, X.; Qiu, J.; Alzain, M.A.; Wang, H.; Fang, H.; et al. China suboptimal health cohort study: Rationale, design and baseline characteristics. J. Transl. Med. 2016, 14, 291. [Google Scholar] [CrossRef]
- Peng, N.; Xiao, D. Research state of sub-health diagnosis and assessment methods. Chin. Arch. Tradit. Chin. Med. 2009, 27, 1324–1326. [Google Scholar]
- Wang, W.; Yan, Y. Suboptimal health: A new health dimension for translational medicine. Clin. Transl. Med. 2012, 1, e28. [Google Scholar]
- Hou, H.; Feng, X.; Li, Y.; Meng, Z.; Guo, D.; Wang, F.; Guo, Z.; Zheng, Y.; Peng, Z.; Zhang, W.; et al. Suboptimal health status and psychological symptoms among Chinese college students: A perspective of predictive, preventive and personalised health. EPMA J. 2018, 9, 367–377. [Google Scholar]
- Lu, Y.; Xu, J.; Cai, Y.J.; Xie, J.; Qiu, J.C.; Wei, Q. Reliability and validity of shs measurement scale version 1.0 for measuring the shs of urban residents in three districts. Chin. J. Health Psychol. 2013, 21, 707–708. [Google Scholar]
- Yan, Y.-X.; Dong, J.; Liu, Y.-Q.; Zhang, J.; Song, M.-S.; He, Y.; Wang, W. Association of suboptimal health status with psychosocial stress, plasma cortisol and mRNA expression of glucocorticoid receptor α/β in lymphocyte. Stress 2015, 18, 29–34. [Google Scholar] [CrossRef]
- Kaplan, G.; Baron-Epel, O. What lies behind the subjective evaluation of health status? Soc. Sci. Med. 2003, 56, 1669–1676. [Google Scholar]
- Wang, Y.; Liu, X.; Qiu, J.; Wang, H.; Liu, D.; Zhao, Z.; Song, M.; Song, Q.; Wang, X.; Zhou, Y.; et al. Association between Ideal Cardiovascular Health Metrics and Suboptimal Health Status in Chinese Population. Sci. Rep. 2017, 7, 14975. [Google Scholar]
- Kolokoltsev, M.; Ambartsumyan, R.; Gryaznykh, A.; Kraynik, V.; Makeeva, V.; Tonoyan, K.; Romanova, E.; Savchenkov, A.; Mischenko, N.; Vrachinskaya, T. Physical activity amount influence over suboptimal health status. J. Phys. Educ. Sport 2021, 21, 381–387. [Google Scholar]
- Wang, L.; Zhao, X.; Chen, J.; Guo, X.; Liang, X.; Yi, D.; Cui, H.; Liu, Y. Biological indicators of sub-optimal health status. J. Tradit. Chin. Med. 2013, 33, 647–650. [Google Scholar] [CrossRef]
- Dissemination, C. Systematic reviews: CRD’s guidance for undertaking reviews in healthcare. York Univ. York NHS Cent. Rev. Dissem. 2009. Available online: http://www.york.ac.uk/inst/crd/index_guidance.htm (accessed on 21 October 2021).
- Wang, W.; Yan, Y.; Guo, Z.; Hou, H.; Garcia, M.; Tan, X.; Anto, E.O.; Mahara, G.; Zheng, Y.; Li, B.; et al. All around suboptimal health—A joint position paper of the Suboptimal Health Study Consortium and European Association for Predictive, Preventive and Personalised Medicine. EPMA J. 2021, 12, 403–433. [Google Scholar]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (prisma-p) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef]
- Mokkink, L.B.; de Vet, H.C.W.; Prinsen, C.A.C.; Patrick, D.L.; Alonso, J.; Bouter, L.M.; Terwee, C.B. COSMIN Risk of Bias checklist for systematic reviews of Patient-Reported Outcome Measures. Qual. Life Res. 2018, 27, 1171–1179. [Google Scholar]
- Mokkink, L.B.; Prinsen, C.A.; Terwee, C.B.; de Vet, H.; Bouter, L.; Patrick, D. Consensus-Based Standards for the Selection of Health Measurement Instruments-COSMIN. Amst. Cosm. 2015, 20, 105–113. [Google Scholar]
- Adua, E.; Afrifa-Yamoah, E.; Frimpong, K.; Adama, E.; Karthigesu, S.P.; Anto, E.O.; Aboagye, E.; Yan, Y.; Wang, Y.; Tan, X.; et al. Construct validity of the Suboptimal Health Status Questionnaire-25 in a Ghanaian population. Health Qual. Life Outcomes 2021, 19, 180. [Google Scholar] [CrossRef]
- Anto, E.O.; Roberts, P.; Coall, D.; Turpin, C.A.; Adua, E.; Wang, Y.; Wang, W. Integration of suboptimal health status evaluation as a criterion for prediction of preeclampsia is strongly recommended for healthcare management in pregnancy: A prospective cohort study in a Ghanaian population. EPMA J. 2019, 10, 211–226. [Google Scholar] [CrossRef]
- Guo, Z.; Meng, R.; Zheng, Y.; Li, X.; Zhou, Z.; Yu, L.; Tang, Q.; Zhao, Y.; Garcia, M.; Yan, Y.; et al. Translation and cross-cultural validation of a precision health tool, the Suboptimal Health Status Questionnaire-25, in Korean. J. Glob. Health 2022, 12, 1–9. [Google Scholar] [CrossRef]
- Xu, J.; Feng, L.-Y.; Luo, R.; Qiu, J.-C.; Zhang, J.-H.; Zhao, X.-S.; Lu, Y.; Wei, Q. Assessment of the reliability and validity of the Sub-health Measurement Scale Version1.0. Nan Fang Yi Ke Da Xue Xue Bao = J. South. Med Univ. 2011, 31, 33–38. [Google Scholar]
- Stein, C.; Fisher, L.; Berkey, C.; Colditz, G. Adolescent Physical Activity and Perceived Competence: Does Change in Activity Level Impact Self-Perception? J. Adolesc. Health 2007, 40, 462.e1–462.e8. [Google Scholar]
- Yao, Y.; Wang, L.; Chen, Y.; Kang, Y.; Gu, Q.; Fang, W.; Qing, R.; Lu, W.; Jin, Y.; Ren, X.; et al. Correlation analysis of anxiety status and sub-health status among students of 13-26 years old. Int. J. Clin. Exp. Med. 2015, 8, 9810. [Google Scholar]
- Bi, J.; Huang, Y.; Xiao, Y.; Cheng, J.; Li, F.; Wang, T.; Chen, J.; Wu, L.; Liu, Y.; Luo, R.; et al. Association of lifestyle factors and suboptimal health status: A cross-sectional study of Chinese students. BMJ Open 2014, 4, e005156. [Google Scholar] [CrossRef] [Green Version]
- Wang, T.; Chen, J.; Sun, X.; Xiang, L.; Zhou, L.; Li, F.; Lin, C.; Jiang, P.; Wu, S.; Xiao, Y.; et al. Effects of TCMC on Transformation of Good Health Status to Suboptimal Health Status: A Nested Case-Control Study. Evid.-Based Complement. Altern. Med. 2015, 2015, 259727. [Google Scholar] [CrossRef]
- Lolokote, S.; Hidru, T.H.; Li, X. Do socio-cultural factors influence college students’ self-rated health status and health-promoting lifestyles? A cross-sectional multicenter study in Dalian, China. BMC Public Health 2017, 17, 478. [Google Scholar]
- Liu, Q.; Li, X. The Interactions of Media Use, Obesity, and Suboptimal Health Status: A Nationwide Time-Trend Study in China. Int. J. Environ. Res. Public Health 2021, 18, 13214. [Google Scholar]
- Wu, S.; Xuan, Z.; Li, F.; Xiao, W.; Fu, X.; Jiang, P.; Chen, J.; Xiang, L.; Liu, Y.; Nie, X.; et al. Work-Recreation Balance, Health-Promoting Lifestyles and Suboptimal Health Status in Southern China: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2016, 13, 339. [Google Scholar] [CrossRef]
- Xu, J.; Xue, Y.; Liu, G.; Feng, Y.; Xu, M.; Xie, J.; Wang, X.; Chen, X.; Jiang, L. Establishment of the norms of Sub-Health measurement scale version 1.0 for Chinese urban residents. Nan Fang Yi Ke Da Xue Xue Bao = J. South. Med. Univ. 2019, 39, 271–278. [Google Scholar]
- Miao, J.; Liu, J.; Wang, Y.; Zhang, Y.; Yuan, H. Reliability and validity of SHMS v1. 0 for suboptimal health status assessment of Tianjin residents and factors affecting sub-health: A cross-sectional study. Medicine 2021, 100, e25401. [Google Scholar] [CrossRef]
- Ma, C.; Zhou, L.; Xu, W.; Ma, S.; Wang, Y. Associations of physical activity and screen time with suboptimal health status and sleep quality among Chinese college freshmen: A cross-sectional study. PLoS ONE 2020, 15, e0239429. [Google Scholar]
- Bi, J.-L.; Chen, J.; Sun, X.-M.; Nie, X.-L.; Liu, Y.-Y.; Luo, R.; Zhao, X.-S. The development and evaluation of a sub-health self-rating scale for university students in China. BMC Public Health 2019, 19, 330. [Google Scholar] [CrossRef]
- Tang, Y.; Wan, Y.; Xu, S.; Zhang, S.; Hao, J.; Tao, F. Nonlinear relationship between sleep duration and non-suicidal self-injurious behaviour among Chinese adolescents. BMC Psychiatry 2021, 21, 521. [Google Scholar] [CrossRef]
- Huang, C.; Yuan, Q.; Ge, M.; Sheng, X.; Yang, M.; Shi, S.; Cao, P.; Ye, M.; Peng, R.; Zhou, R.; et al. Childhood trauma and non-suicidal self-injury among Chinese adolescents: The mediating role of psychological sub-health. Front. Psychiatry 2022, 13, 798369. [Google Scholar]
- Cao, H.; Sun, Y.; Wan, Y.; Hao, J.; Tao, F. Problematic Internet use in Chinese adolescents and its relation to psychosomatic symptoms and life satisfaction. BMC Public Health 2011, 11, 802. [Google Scholar]
- Chen, J.; Cheng, J.; Liu, Y.; Tang, Y.; Sun, X.; Wang, T.; Xiao, Y.; Li, F.; Xiang, L.; Jiang, P.; et al. Associations between breakfast eating habits and health-promoting lifestyle, suboptimal health status in Southern China: A population based, cross sectional study. J. Transl. Med. 2014, 12, 348. [Google Scholar]
- Xing, C.; Tao, F. Evaluation of reliability and validity of the multidimensional sub-health ques-tionnaire of adolescents. Chin. J. Public Health 2008, 24, 103–131. [Google Scholar] [CrossRef]
- Alzain, M.A.; Asweto, C.O.; Zhang, J.; Fang, H.; Zhao, Z.; Guo, X.; Song, M.; Zhou, Y.; Chang, N.; Wang, Y.; et al. Telomere Length and Accelerated Biological Aging in the China Suboptimal Health Cohort: A Case–Control Study. OMICS A J. Integr. Biol. 2017, 21, 333–339. [Google Scholar] [CrossRef]

| Authors and Year | Title | Aims | Gap |
|---|---|---|---|
| Zhang Y., et al. (2015) [3] | A systemic review of suboptimal health | Analyze the currently available SHS research and discuss the related issues about its concept and diagnostic criteria. Differentiate between chronic fatigue syndrome and psychosomatic diseases. | Analyzed and discussed the related issues about the concept of SHS and the diagnostic criteria; however, did not focus in the psychometric properties of SHS instruments. |
| Zhong et al. (2010) [5] | A literature review on the conceptual framework of sub-health | Assess conceptual framework, diagnostic criteria, and their operability; foundational support of SHS conditions. | Focused on articulating the conceptual framework of SHS, but never addressed issues related to SHS instruments. |
| Wei Wang (2021) [24] | A joint position paper of the SHS Study Consortium and European Association for PPPM | Demonstrate advanced strategies in bio/medical sciences and healthcare through focused on SHS conditions in PPPM; for potential benefits in healthcare systems, to improved life quality, and advanced professionalism of healthcare givers, and a sustainable healthcare economy. | Focused on the assessment of SHS for PPPM; however, did not adopt a systematic review approach to assess the psychometric properties of tools. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alzain, M.A.; Asweto, C.O.; Hassan, S.-u.-N.; Saeed, M.E.; Kassar, A.; Alsaif, B. Psychometric Properties of Suboptimal Health Status Instruments: A Systematic Review. J. Pers. Med. 2023, 13, 299. https://doi.org/10.3390/jpm13020299
Alzain MA, Asweto CO, Hassan S-u-N, Saeed ME, Kassar A, Alsaif B. Psychometric Properties of Suboptimal Health Status Instruments: A Systematic Review. Journal of Personalized Medicine. 2023; 13(2):299. https://doi.org/10.3390/jpm13020299
Chicago/Turabian StyleAlzain, Mohamed Ali, Collins Otieno Asweto, Sehar-un-Nisa Hassan, Mohammed Elshiekh Saeed, Ahmed Kassar, and Bandar Alsaif. 2023. "Psychometric Properties of Suboptimal Health Status Instruments: A Systematic Review" Journal of Personalized Medicine 13, no. 2: 299. https://doi.org/10.3390/jpm13020299