
Posttraumatic Osteomyelitis Risks Associated with NLRP3 Gene Polymorphisms in the Chinese Population
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Controls
2.2. Determination of NLRP3 Polymorphisms
2.3. Outcome Parameters
2.4. Statistical Analysis
3. Results
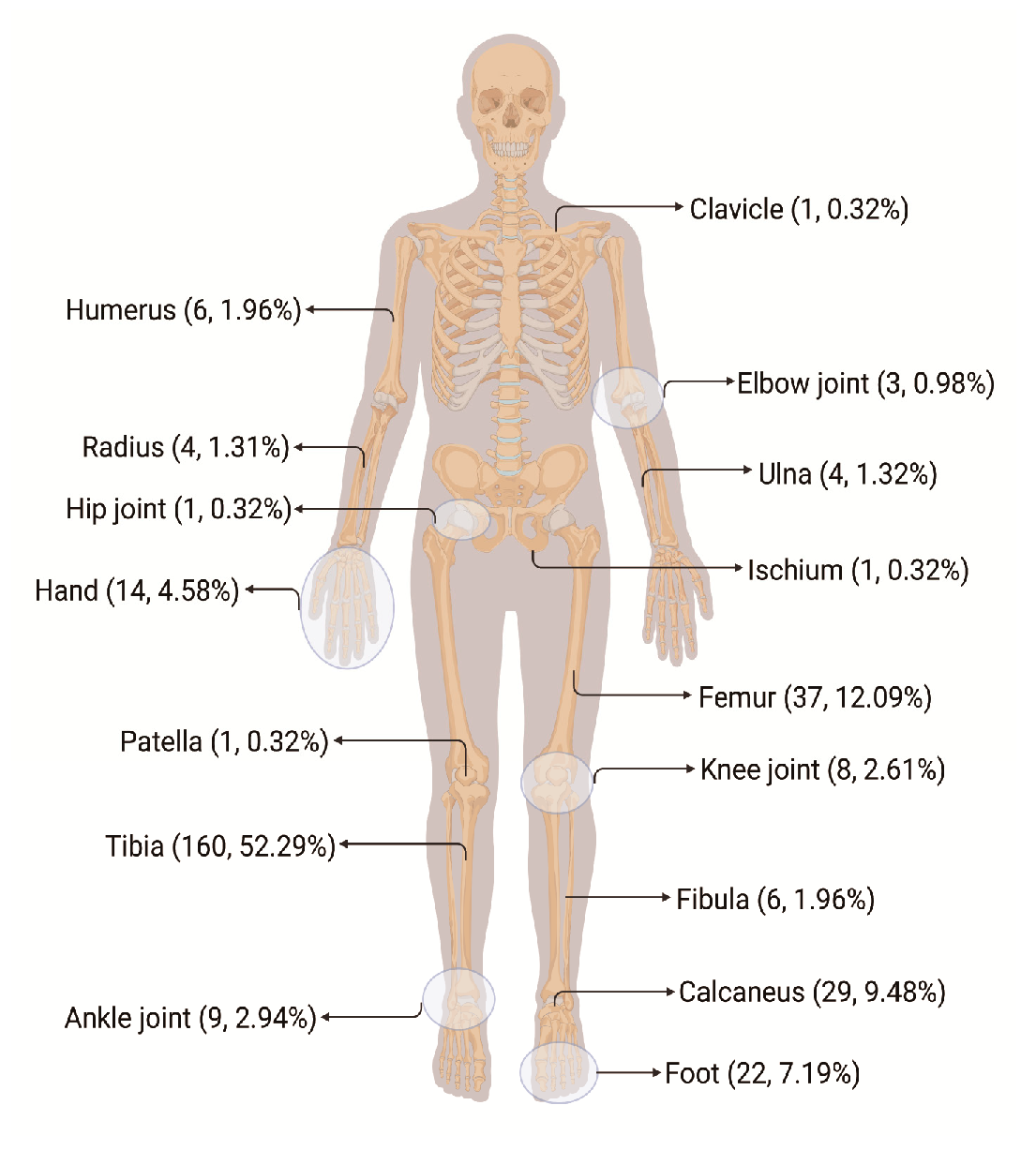
3.1. Clinical Characteristics of Patients with PTOM
3.2. Results of HWE Tests
3.3. Relationship between 25 SNPs and PTOM Susceptibility
3.3.1. NLRP3 rs10754558 and rs7525979
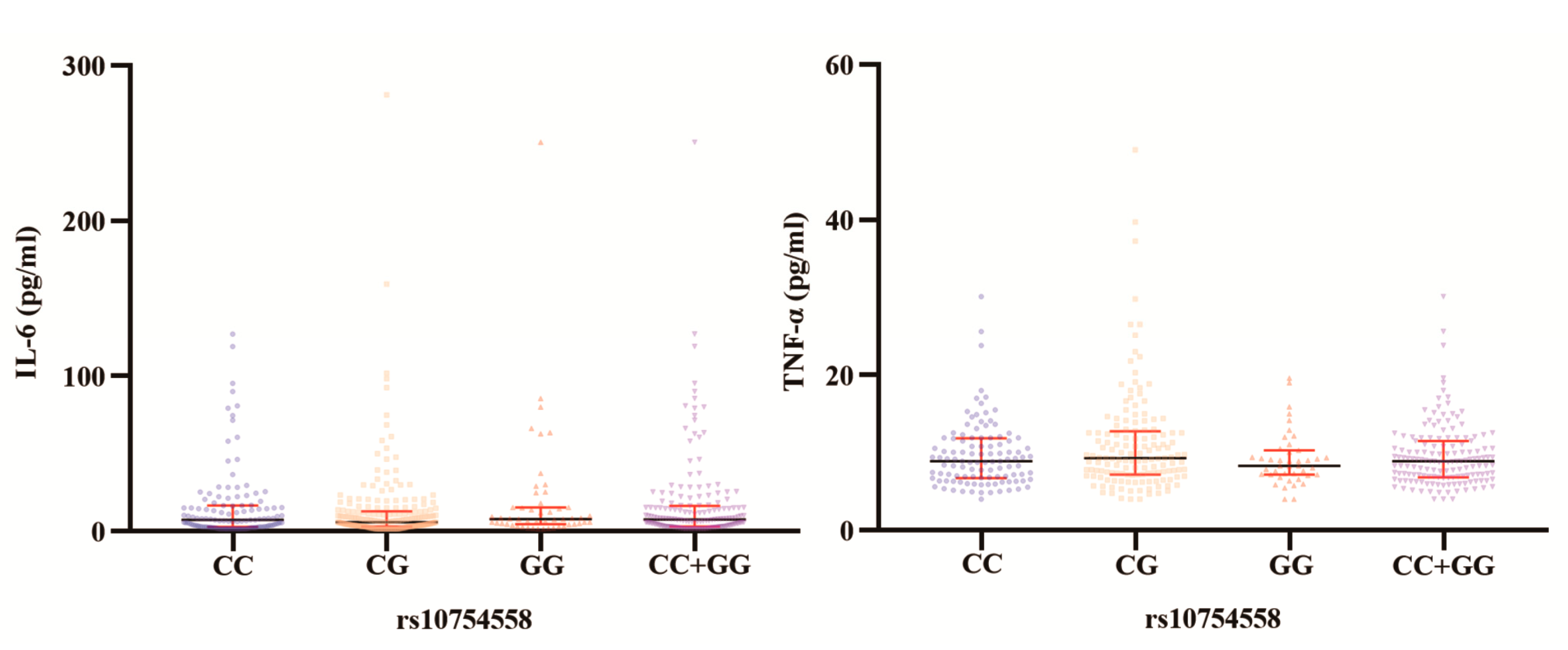
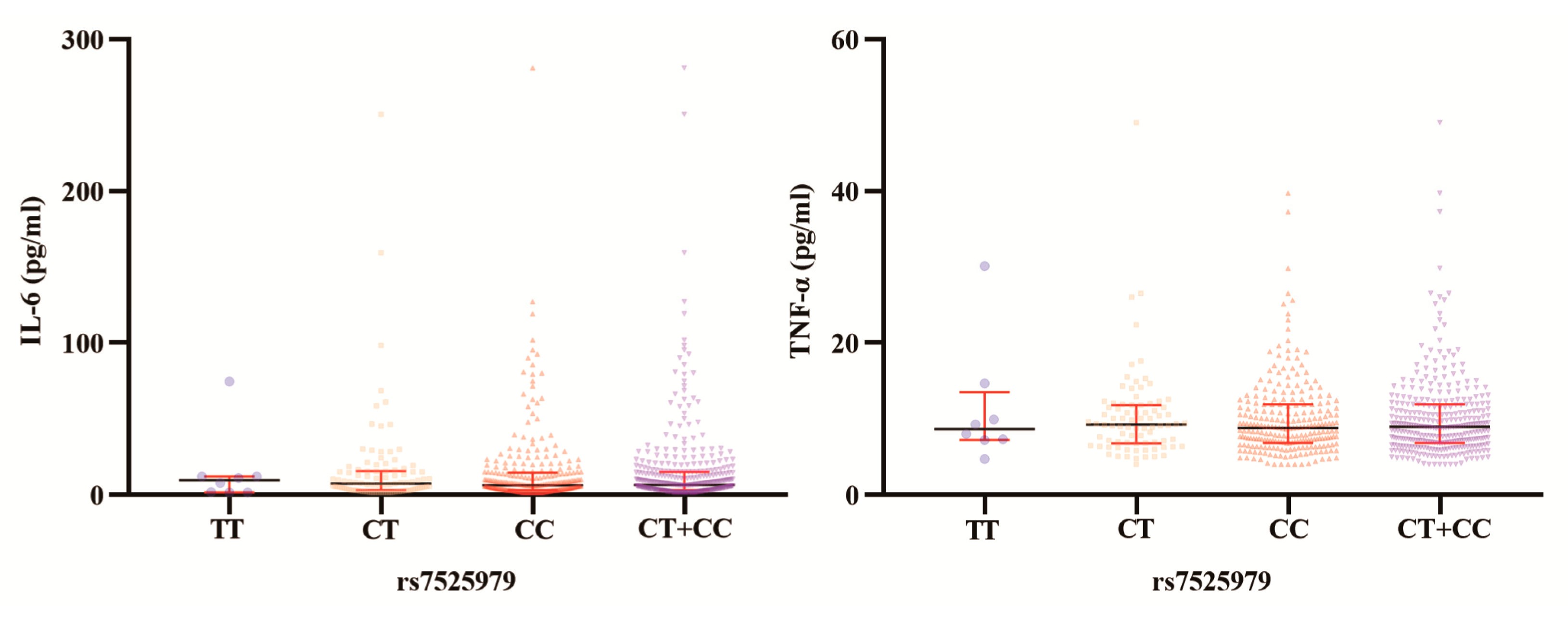
3.3.2. Serological IL-6 and TNF-α Levels in Various NLRP3 rs10754558 and rs7525979 Patient Genotypes
3.3.3. Lack of Association between the Other 21 SNPs with PTOM Susceptibility
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zimmerli, W. Clinical presentation and treatment of orthopaedic implant-associated infection. J. Intern. Med. 2014, 276, 111–119. [Google Scholar] [CrossRef] [PubMed]
- Trampuz, A.; Zimmerli, W. Diagnosis and treatment of infections associated with fracture-fixation devices. Injury 2006, 37, S59–S66. [Google Scholar] [CrossRef] [PubMed]
- Hogan, A.; Heppert, V.G.; Suda, A.J. Osteomyelitis. Arch. Orthop. Trauma Surg. 2013, 133, 1183–1196. [Google Scholar] [CrossRef] [PubMed]
- Tseng, C.H.; Huang, W.S.; Muo, C.H.; Chang, Y.J.; Kao, C.H. Increased depression risk among patients with chronic osteomyelitis. J. Psychosom. Res. 2014, 77, 535–540. [Google Scholar] [CrossRef]
- Jiang, N.; Wu, H.T.; Lin, Q.R.; Hu, Y.J.; Yu, B. Health Care Costs of Post-traumatic Osteomyelitis in China: Current Situation and Influencing Factors. J. Surg. Res. 2020, 247, 356–363. [Google Scholar] [CrossRef]
- Tschudin-Sutter, S.; Frei, R.; Dangel, M.; Jakob, M.; Balmelli, C.; Schaefer, D.J.; Weisser, M.; Elzi, L.; Battegay, M.; Widmer, A.F. Validation of a treatment algorithm for orthopaedic implant-related infections with device-retention-results from a prospective observational cohort study. Clin. Microbiol. Infect. 2016, 22, 457.e1–457.e9. [Google Scholar] [CrossRef]
- Wang, L.; Jiang, N.; Lin, Q.R.; Qin, C.H.; Hu, Y.J.; Yu, B. Cyclooxygenase-2 (COX-2) polymorphism rs689466 may contribute to the increased susceptibility to post-traumatic osteomyelitis in Chinese population. Infect. Dis. 2017, 49, 817–823. [Google Scholar] [CrossRef]
- Alves De Souza, C.; Queiroz Alves De Souza, A.; Queiroz Alves De Souza, M.D.S.; Dias Leite, J.A.; Silva De Morais, M.; Barem Rabenhorst, S.H. A link between osteomyelitis and IL1RN and IL1B polymorphisms-a study in patients from Northeast Brazil. Acta Orthop. 2017, 88, 556–561. [Google Scholar] [CrossRef] [Green Version]
- McCall, S.H.; Sahraei, M.; Young, A.B.; Worley, C.S.; Duncan, J.A.; Ting, J.P.; Marriott, I. Osteoblasts express NLRP3, a nucleotide-binding domain and leucine-rich repeat region containing receptor implicated in bacterially induced cell death. J. Bone Miner. Res. 2008, 23, 30–40. [Google Scholar] [CrossRef] [Green Version]
- Kummer, J.A.; Broekhuizen, R.; Everett, H.; Agostini, L.; Kuijk, L.; Martinon, F.; van Bruggen, R.; Tschopp, J. Inflammasome components NALP 1 and 3 show distinct but separate expression profiles in human tissues suggesting a site-specific role in the inflammatory response. J. Histochem. Cytochem. 2007, 55, 443–452. [Google Scholar] [CrossRef]
- Gross, O.; Thomas, C.J.; Guarda, G.; Tschopp, J. The inflammasome: An integrated view. Immunol. Rev. 2011, 243, 136–151. [Google Scholar] [CrossRef]
- Xian, H.; Watari, K.; Sanchez-Lopez, E.; Offenberger, J.; Onyuru, J.; Sampath, H.; Ying, W.; Hoffman, H.M.; Shadel, G.S.; Karin, M. Oxidized DNA fragments exit mitochondria via mPTP- and VDAC-dependent channels to activate NLRP3 inflammasome and interferon signaling. Immunity 2022, 55, 1370–1385.8. [Google Scholar] [CrossRef]
- Jiang, N.; Wang, B.W.; Chai, Y.M.; Wu, X.B.; Tang, P.F.; Zhang, Y.Z.; Yu, B. Chinese expert consensus on diagnosis and treatment of infection after fracture fixation. Injury 2019, 50, 1952–1958. [Google Scholar] [CrossRef]
- Jiang, N.; Li, S.Y.; Ma, Y.F.; Hu, Y.J.; Lin, Q.R.; Yu, B. Associations between Interleukin Gene Polymorphisms and Risks of Developing Extremity Posttraumatic Osteomyelitis in Chinese Han Population. Mediat. Inflamm. 2020, 2020, 3278081. [Google Scholar] [CrossRef]
- Miller, S.A.; Dykes, D.D.; Polesky, H.F. A simple salting out procedure for extracting DNA from human nucleated cells. Nucleic Acids Res. 1988, 16, 1215. [Google Scholar] [CrossRef] [Green Version]
- Ben, S.; Cooper-DeHoff, R.M.; Flaten, H.K.; Evero, O.; Ferrara, T.M.; Spritz, R.A.; Monte, A.A. Multiplex SNaPshot-a new simple and efficient CYP2D6 and ADRB1 genotyping method. Hum. Genom. 2016, 10, 11. [Google Scholar] [CrossRef] [Green Version]
- Jiang, N.; Zhao, X.Q.; Qin, C.H.; Hu, Y.J.; Wang, L.; Xie, G.P.; Wang, S.N.; Chen, L.G.; Yu, B. Association of vitamin D receptor gene TaqI, BsmI, FokI and ApaI polymorphisms and susceptibility to extremity chronic osteomyelitis in Chinese population. Injury 2016, 47, 1655–1660. [Google Scholar] [CrossRef]
- Marais, L.C.; Ferreira, N.; Aldous, C.; Sartorius, B.; Le Roux, T. A modified staging system for chronic osteomyelitis. J. Orthop. 2015, 12, 184–192. [Google Scholar] [CrossRef] [Green Version]
- Lu, K.; Zhang, J.; Cheng, J.; Liu, H.; Yang, C.; Yin, L.; Wang, H.; You, X.; Qu, Q. Incidence and risk factors for surgical site infection after open reduction and internal fixation of intra-articular fractures of distal femur: A multicentre study. Int. Wound J. 2019, 16, 473–478. [Google Scholar] [CrossRef]
- Chan, G.; Iliopoulos, E.; Jain, A.; Turki, M.; Trompeter, A. Infection after operative fixation of tibia plateau fractures. A risk factor analysis. Injury 2019, 50, 2089–2092. [Google Scholar] [CrossRef]
- Zhou, D.; Wang, X.; Chen, T.; Wen, W.; Liu, Y.; Wu, Y.; Yuan, Z. The NLRP3 rs10754558 Polymorphism Is Associated with the Occurrence and Prognosis of Coronary Artery Disease in the Chinese Han Population. BioMed Res. Int. 2016, 2016, 3185397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hanaei, S.; Sadr, M.; Rezaei, A.; Shahkarami, S.; Ebrahimi Daryani, N.; Bidoki, A.Z.; Rezaei, N. Association of NLRP3 single nucleotide polymorphisms with ulcerative colitis: A case-control study. Clin. Res. Hepatol. Gastroenterol. 2018, 42, 269–275. [Google Scholar] [CrossRef] [PubMed]
- Meliț, L.E.; Mărginean, C.O.; Săsăran, M.O.; Mocanu, S.; Ghiga, D.V.; Crișan, A.; Bănescu, C. Innate Immune Responses in Pediatric Patients with Gastritis-A Trademark of Infection or Chronic Inflammation? Children 2022, 9, 121. [Google Scholar] [CrossRef] [PubMed]
- Addobbati, C.; da Cruz, H.L.A.; Adelino, J.E.; Melo Tavares Ramos, A.L.; Fragoso, T.S.; Domingues, A.; Branco Pinto Duarte, Â.L.; Oliveira, R.D.R.; Louzada-Júnior, P.; Donadi, E.A.; et al. Polymorphisms and expression of inflammasome genes are associated with the development and severity of rheumatoid arthritis in Brazilian patients. Inflamm. Res. 2018, 67, 255–264. [Google Scholar] [CrossRef]
- Lazzarini, L.; Mader, J.T.; Calhoun, J.H. Osteomyelitis in long bones. J. Bone Jt. Surg. 2004, 86, 2305–2318. [Google Scholar] [CrossRef]
- Mathews, J.A.; Ward, J.; Chapman, T.W.; Khan, U.M.; Kelly, M.B. Single-stage orthoplastic reconstruction of Gustilo-Anderson Grade III open tibial fractures greatly reduces infection rates. Injury 2015, 46, 2263–2266. [Google Scholar] [CrossRef]
- Yoshimoto, T.; Kittaka, M.; Doan, A.A.P.; Urata, R.; Prideaux, M.; Rojas, R.E.; Harding, C.V.; Henry Boom, W.; Bonewald, L.F.; Greenfield, E.M.; et al. Osteocytes directly regulate osteolysis via MYD88 signaling in bacterial bone infection. Nat. Commun. 2022, 13, 6648. [Google Scholar] [CrossRef]
- Scianaro, R.; Insalaco, A.; Bracci Laudiero, L.; De Vito, R.; Pezzullo, M.; Teti, A.; De Benedetti, F.; Prencipe, G. Deregulation of the IL-1β axis in chronic recurrent multifocal osteomyelitis. Pediatr. Rheumatol. Online J. 2014, 12, 30. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| SNP | Item | Allele or Genotype | Patients | Controls | p-Values | OR (95% CI) |
|---|---|---|---|---|---|---|
| rs35829419 | Genotype (n, %) | AA | 0 (0.0) | 0 (0.0) | NA | NA |
| AC | 2 (0.65) | 1 (0.27) | ||||
| CC | 304 (99.35) | 367 (99.73) | ||||
| Allele frequency | A vs. C | 2/610 | 1/735 | 0.873 | 2.410 (0.218, 26.640) | |
| Dominant model | AA + AC vs. CC | 2/304 | 1/367 | 0.873 | 2.414 (0.218, 26.756) | |
| Recessive model | AA vs. AC + CC | 0/306 | 0/368 | NA | NA | |
| Homozygous model | AA vs. CC | 0/304 | 0/367 | NA | NA | |
| Heterozygous model | AC vs. CC | 2/304 | 1/367 | 0.873 | 2.414 (0.218, 26.756) | |
| rs10754558 | Genotype (n, %) | CC | 97 (31.70) | 135 (36.68) | 0.047 | NA |
| CG | 169 (55.23) | 169 (45.92) | ||||
| GG | 40 (13.07) | 64 (17.39) | ||||
| Allele frequency | C vs. G | 363/249 | 439/297 | 0.901 | 0.986 (0.793, 1.227) | |
| Dominant model | CC + CG vs. GG | 266/40 | 304/64 | 0.122 | 1.400 (0.913, 2.148) | |
| Recessive model | CC vs. CG + GG | 97/209 | 135/233 | 0.175 | 0.801 (0.581, 1.104) | |
| Homozygous model | CC vs.GG | 97/40 | 135/64 | 0.564 | 1.150 (0.716, 1.846) | |
| Heterozygous model | CG vs.GG | 169/40 | 169/64 | 0.039 | 1.600 (1.021, 2.507) | |
| rs7525979 | Genotype (n, %) | TT | 3 (0.98) | 14 (3.84) | 0.048 | NA |
| CT | 80 (26.14) | 102 (27.95) | ||||
| CC | 223 (72.88) | 249 (68.22) | ||||
| Allele frequency | T vs. C | 86/526 | 130/600 | 0.062 | 0.755 (0.561, 1.015) | |
| Dominant model | TT + CT vs. CC | 83/223 | 116/249 | 0.188 | 0.799 (0.572, 1.117) | |
| Recessive model | TT vs. CT + CC | 3/303 | 14/351 | 0.019 | 0.248 (0.071, 0.872) | |
| Homozygous model | TT vs. CC | 3/223 | 14/249 | 0.016 | 0.239 (0.068, 0.844) | |
| Heterozygous model | CT vs. CC | 80/223 | 102/249 | 0.450 | 0.876 (0.621, 1.235) | |
| rs4612666 | Genotype (n, %) | CC | 73 (23.86) | 98 (26.63) | 0.265 | NA |
| CT | 168 (54.90) | 179 (48.64) | ||||
| TT | 65 (21.24) | 91 (24.73) | ||||
| Allele frequency | C vs. T | 314/298 | 375/361 | 0.896 | 1.014 (0.819, 1.257) | |
| Dominant model | CC + CT vs. TT | 241/65 | 277/91 | 0.285 | 1.218 (0.848, 1.750) | |
| Recessive model | CC vs. CT + TT | 73/233 | 98/270 | 0.401 | 0.863 (0.608, 1.225) | |
| Homozygous model | CC vs. TT | 73/65 | 98/91 | 0.852 | 1.043 (0.672, 1.618) | |
| Heterozygous model | CT vs. TT | 168/65 | 179/91 | 0.160 | 1.314 (0.897, 1.925) |
| Items | rs35829419 | rs10754558 | rs7525979 | rs4612666 | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| AA | AC | CC | p Value | CC | CG | GG | p Value | TT | CT | CC | p Value | CC | CT | TT | p Value | |
| WBC (×10/L)9 Median (IQR) | NA | 6.065 (5.460, 6.065) | 6.980 (5.720, 8.320) | 0.365 | 7.03 (5.72, 8.61) | 6.96 (5.63, 8.25) | 6.82 (5.62, 8.30) | 0.917 | 6.35 (5.88, 6.35) | 7.44 (5.75, 8.23) | 6.81 (5.66, 8.37) | 0.711 | 6.79 (5.52, 8.82) | 6.99 (5.86, 8.34) | 6.86 (5.68, 8.00) | 0.624 |
| CRP (mg/L) Median (IQR) | NA | 5.840 (2.100, 5.840) | 4.345 (1.485, 11.920) | 0.870 | 5.61 (1.73, 15.24) | 4.09 (1.40, 9.83) | 3.25 (1.42, 8.10) | 0.282 | 8.70 (7.10, 8.70) | 5.30 (1.67, 15.24) | 4.05 (1.42, 9.98) | 0.160 | 3.00 (0.98, 8.61) | 4.58 (1.99, 12.47) | 4.03 (1.55, 16.42) | 0.129 |
| ESR (mm/h) Median (IQR) | NA | 7.000 (1.000, 7.000) | 15.000 (7.000, 36.000) | 0.184 | 20.00 (7.75, 42.50) | 14.00 (7.00, 32.00) | 13.00 (4.25, 28.25) | 0.399 | 36.00 (5.00, 36.00) | 14.00 (6.00, 43.00) | 16.00 (7.00, 32.00) | 0.698 | 13.00 (5.00, 22.75) | 16.00 (7.00, 39.50) | 15.00 (7.75, 44.00) | 0.257 |
| PCT (ng/mL) Median (IQR) | NA | NA | 0.037 (0.021, 0.060) | NA | 0.03 (0.02, 0.05) | 0.04 (0.03, 0.07) | 0.03 (0.02, 0.04) | 0.258 | 0.03 (0.03, 0.03) | 0.04 (0.03, 0.05) | 0.03 (0.02, 0.06) | 0.488 | 0.03 (0.02, 0.06) | 0.04 (0.02, 0.07) | 0.03 (0.02, 0.05) | 0.585 |
| IL-6 (pg/mL) Median (IQR) | NA | 7.660 (6.010, 7.660) | 5.270 (2.895, 10.930)) | 0.518 | 6.83 (2.81, 14.49) | 4.67 (2.75, 9.65) | 5.86 (3.18, 8.51) | 0.217 | 12.16 (1.54, 12.16) | 5.71 (2.50, 11.76) | 5.05 (3.00, 9.89) | 0.879 | 4.72 (2.98, 8.32) | 5.61 (2.94, 11.19) | 5.60 (2.39, 14.41) | 0.455 |
| TNF-α (pg/mL) Median (IQR) | NA | 7.015 (6.150, 7.015) | 8.320 (6.570, 10.800) | 0.394 | 8.55 (6.43, 10.80) | 8.31 (6.50, 11.05) | 8.06 (6.93, 9.77) | 0.855 | 8.02 (7.23, 8.02) | 9.08 (6.78, 11.33) | 8.08 (6.49, 10.73) | 0.679 | 7.71 (6.71, 10.10) | 8.88 (6.74, 11.50) | 7.38 (6.29, 10.70) | 0.526 |
| SAA (mg/L) Median (IQR) | NA | 12.750 (6.800, 12.750) | 11.400 (6.400, 35.900) | 0.880 | 12.70 (6.70, 51.55) | 10.90 (6.20, 33.18) | 10.90 (6.85, 24.30) | 0.818 | 35.90 (12.70, 35.90) | 12.65 (7.38, 56.70) | 10.95 (6.20, 32.70) | 0.296 | 8.85 (5.88, 23.75) | 12.10 (6.70, 36.10) | 13.05 (6.95, 67.28) | 0.174 |
| Number | PubMed ID | SNP | Related Diseases |
|---|---|---|---|
| 1 | 33848452 30658261 | Q705K | Cystic fibrosis Multiple sclerosis |
| 2 | 31978095 28116820 | rs4612666 | Periodontitis Ankylosing spondylitis |
| 3 | 33533549 | rs3806265 | Myasthenia gravis |
| 4 | 29888470 26689701 | rs10754558 | Acne vulgaris Ischemic stroke |
| 5 | 30131971 | rs7525979 | Parkinson’s disease |
| 6 | 23588528 | rs7512998 | Primary gouty arthritis |
| 7 | 29850521 | rs3806265, rs10754557 | Psoriasis vulgaris |
| 8 | 21621776 | rs35829419 | Abdominal aortic aneurysms |
| 9 | 22112657 | rs2027432, rs12048215 | MOD syndrome |
| The present study | NA | Rs10754558, rs7525979 | PTOM |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Qu, Y.; Li, J.; Zhang, W.; Xia, C.; Ou, S.; Yang, Y.; Jiang, N.; Ma, Y.; Qi, Y.; Xu, C. Posttraumatic Osteomyelitis Risks Associated with NLRP3 Gene Polymorphisms in the Chinese Population. J. Pers. Med. 2023, 13, 253. https://doi.org/10.3390/jpm13020253
Qu Y, Li J, Zhang W, Xia C, Ou S, Yang Y, Jiang N, Ma Y, Qi Y, Xu C. Posttraumatic Osteomyelitis Risks Associated with NLRP3 Gene Polymorphisms in the Chinese Population. Journal of Personalized Medicine. 2023; 13(2):253. https://doi.org/10.3390/jpm13020253
Chicago/Turabian StyleQu, Yudun, Jiaxuan Li, Wei Zhang, Changliang Xia, Shuanji Ou, Yang Yang, Nan Jiang, Yunfei Ma, Yong Qi, and Changpeng Xu. 2023. "Posttraumatic Osteomyelitis Risks Associated with NLRP3 Gene Polymorphisms in the Chinese Population" Journal of Personalized Medicine 13, no. 2: 253. https://doi.org/10.3390/jpm13020253