

Personalized Brain–Computer Interface and Its Applications
Abstract
:1. Introduction
2. Personalized BCI
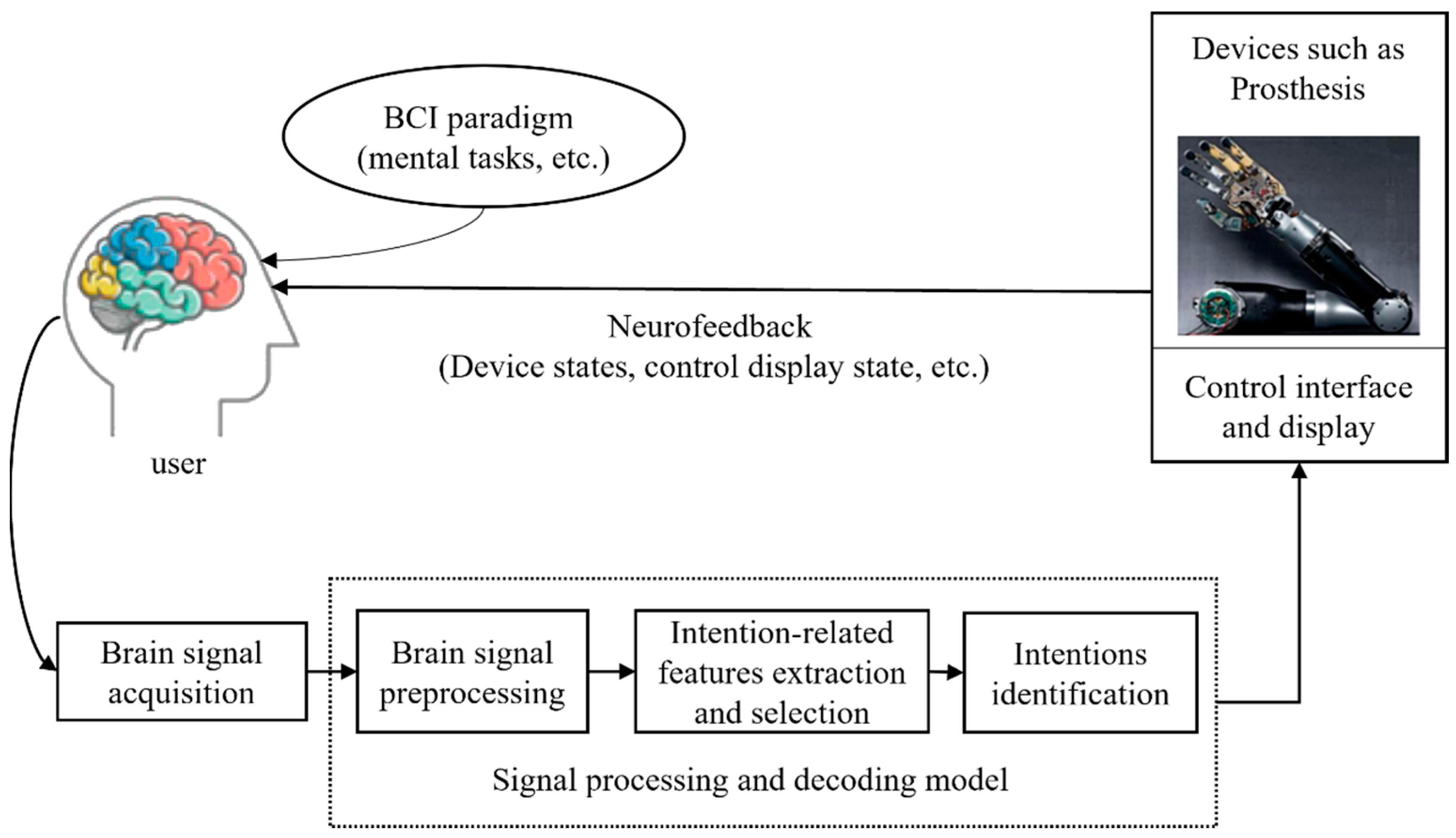
2.1. General BCI
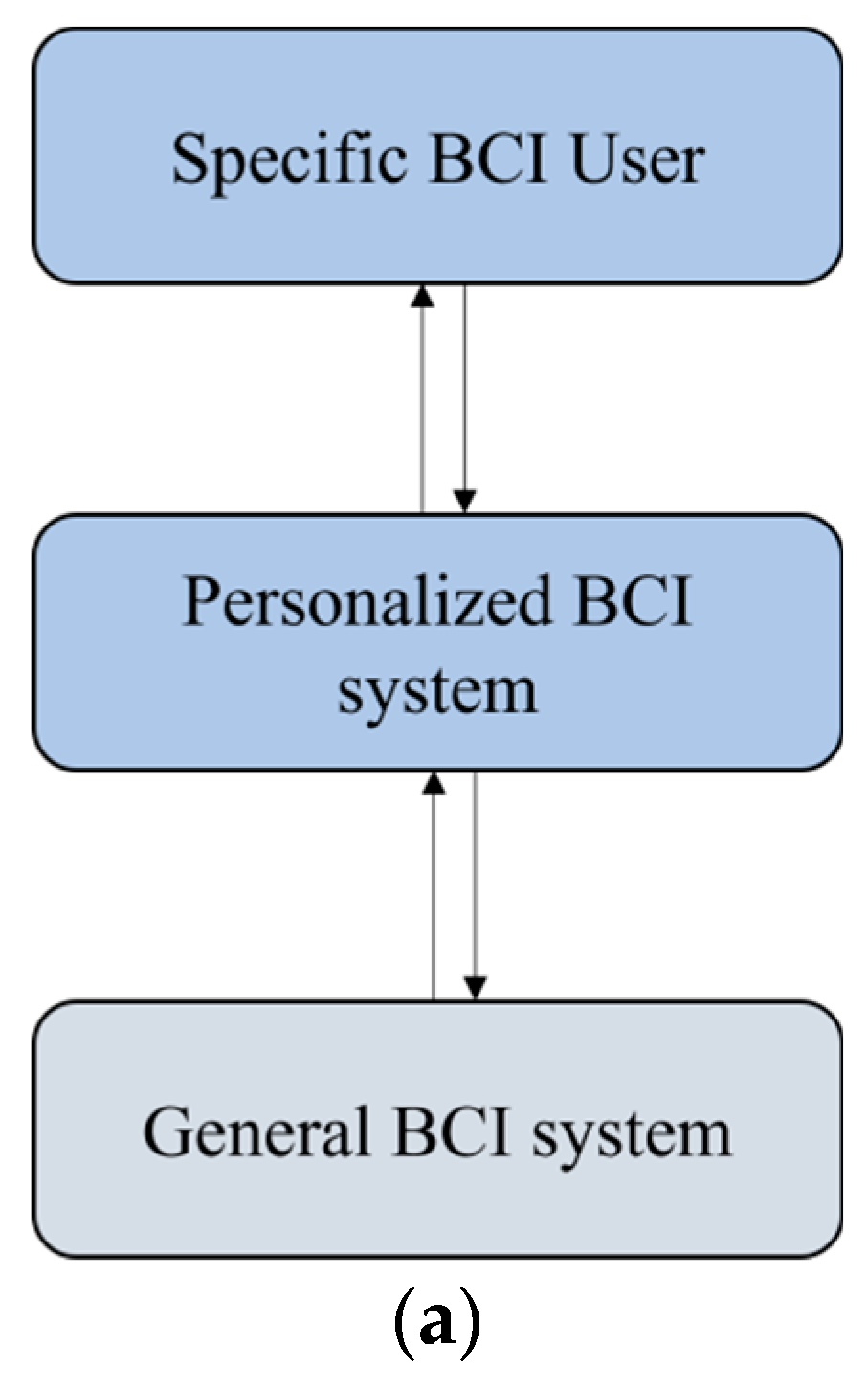
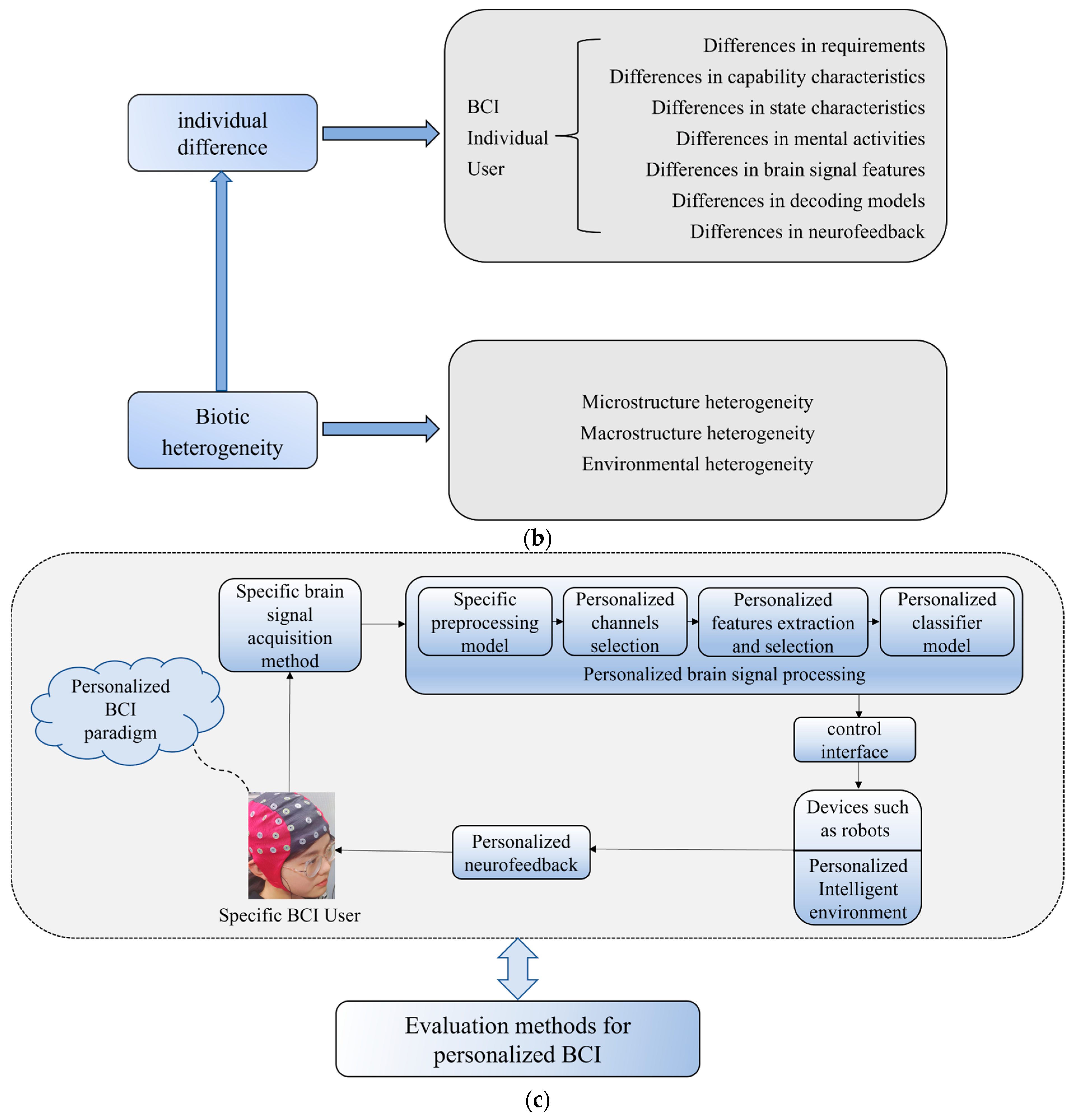
2.2. Personalized BCI
3. Personalized BCI Design, Research, and Development
3.1. Personalized BCI Paradigm Design
3.2. Brain Signal Acquisition Scheme for a Specific User
3.3. Personalized Processing of Brain Signals
3.3.1. Specific Preprocessing Model
3.3.2. Personalized Channel Selection
3.3.3. Personalized Feature Extraction and Selection
3.3.4. Personalized Classification Model
3.3.5. Personalization Algorithm Design Based on the Overall BCI System
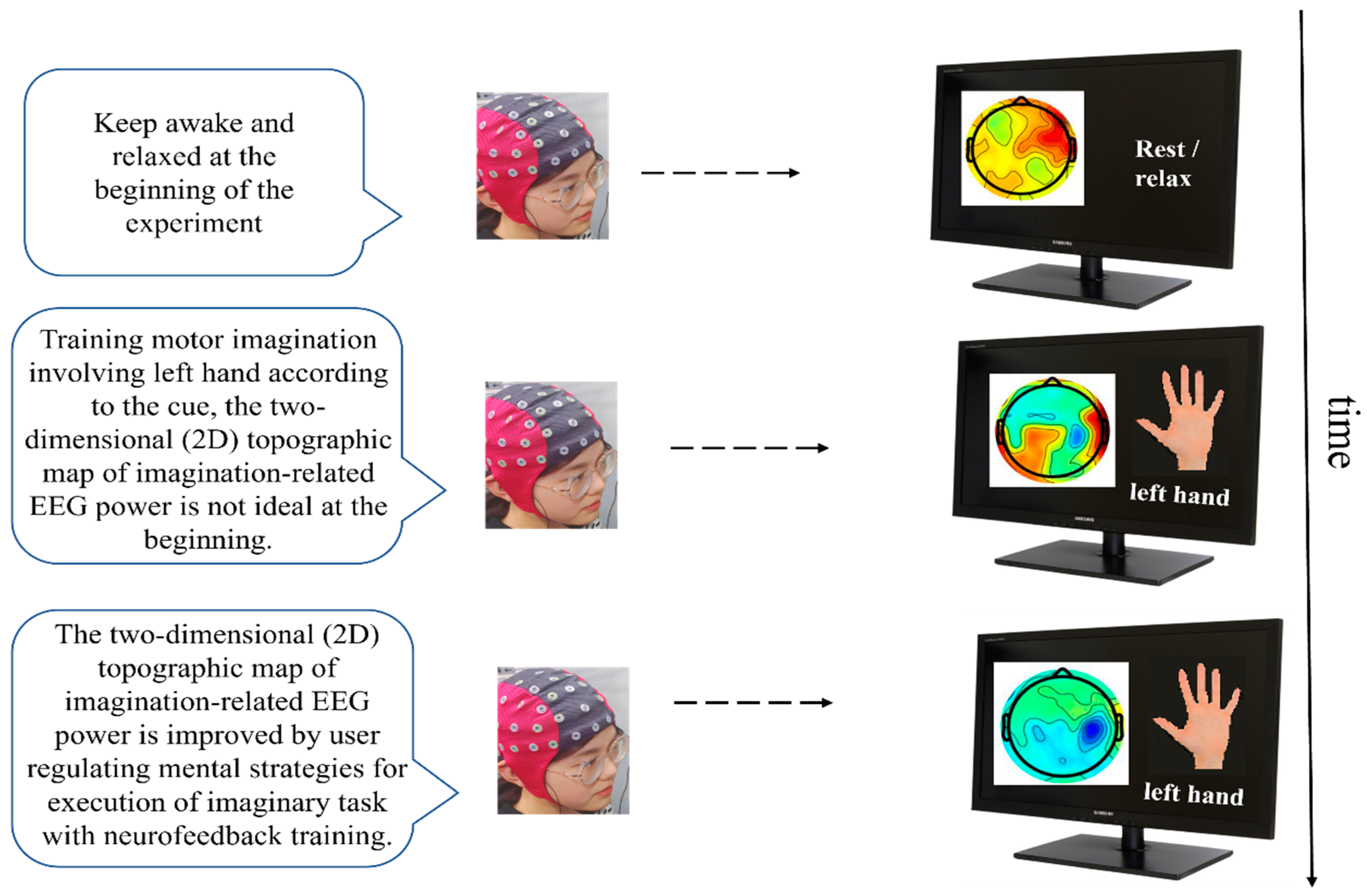
3.4. Personalized Neurofeedback
3.5. Personalized Intelligent Environment
4. Evaluation of Personalized BCI Performance
4.1. Performance Evaluation Methods for General BCI System
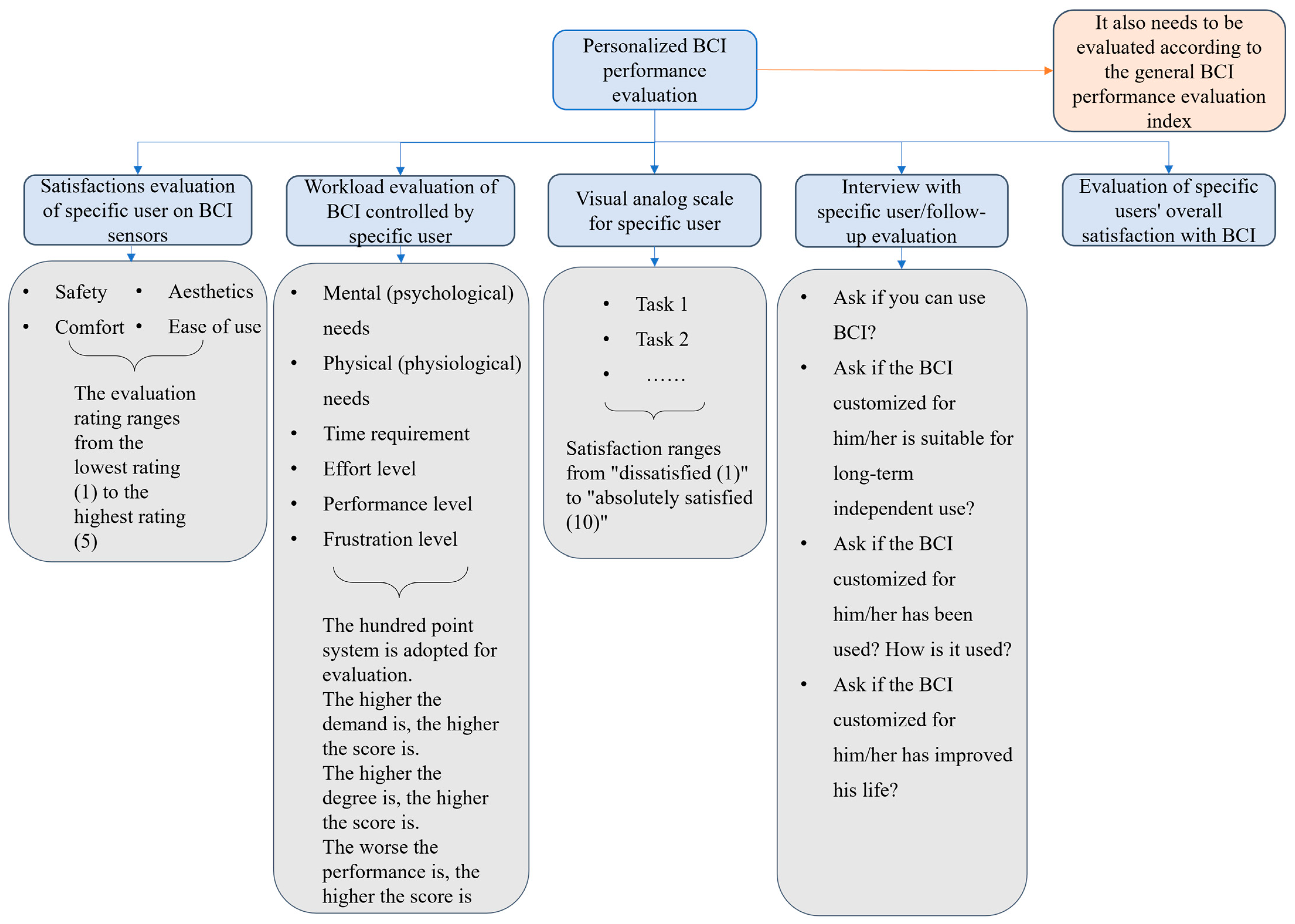
4.2. Evaluation Method of Personalized BCI Performance
5. Personalized BCI Application
5.1. Application of Personalized BCI in Auxiliary Control
- (1)
- Communication and control
- (2)
- Motion replacement
5.2. Application of Individualized BCI in the Rehabilitation of Neurological Diseases
- (1)
- Treatment and rehabilitation of Parkinson’s disease
- (2)
- Rehabilitation after stroke
- (a)
- Rehabilitation of cognitive impairment
- (b)
- Rehabilitation of dyskinesia
5.3. Application of Individualized BCI in the Rehabilitation of Mental Disorders
5.4. Application of Individualized BCI in the Rehabilitation of Mental Disorders
5.5. BCI-Related Research Considering Specific Users
6. Challenges and Prospects of Personalized BCI
6.1. Challenges Faced by Personalized BCI
- (1)
- How to personalize the general BCI to suit specific users
- (2)
- Which BCI paradigm suits or satisfies a specific user
- (3)
- Which brain signal acquisition sensor is suitable for satisfying a specific BCI user
- (4)
- Which brain signal characteristics of a specific user are suitable for driving a BCI
- (5)
- What kind of neural feedback can improve BCI performance and satisfy specific users
- (6)
- How to evaluate the performance of BCI customized for specific users
6.2. Limitations of Personalized BCI
6.3. Future of Personalized BCI
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| Term | Abbreviations |
| Brain-computer Interface | BCI |
| Personalized brain-computer interface | pBCI |
| Customized brain-computer interface | cBCI |
| General brain-computer interface | gBCI |
| User-selected weighted slope scores | WS-US |
| User-selected pair-wise accuracy rankings | PWAR–US |
| Repeatable Battery for the Assessment of Neuropsychological Status | RBANS |
| Sparse common spatial pattern | SCSP |
| Electroencephalogram | EEG |
| Near infrared spectroscopy | NIRS |
| Motor imagery | MI |
| Self-organizing map | SOM |
| Electrocorticography | ECoG |
| Local field potential | LFP |
| Event-related desynchronization | ERD |
| Event related synchronization | ERS |
| Select distribution estimation | EDA |
| Deep Belief Network | DBN |
| Filter Bank Common Spatial Pattern | FBCSP |
| Weighted discriminator | WD |
| Neurofeedback | NF |
| Receiver operating characteristic curve | ROC |
| Area Under Curve | AUC |
| Deep brain computer interface | DBCI |
| Subthalamic nucleus–deep brain stimulation | STN-DBS |
| Parkinson disease | PD |
| BCI transcranial Direct Current Stimulation coupled BCI | TDCS-BCI |
| Power ratio index | PRI |
| Deep brain stimulation | DBS |
| Transcranial direct/alternating current stimulation | tDCS/tACS |
| Transcranial Magnetic Stimulation | TMS |
| Transcranial ultrasound stimulation | TUS |
| Explainable Artifificial Intelligence | XAI |
| Event-related Potentials | ERPs |
| Affective BCI | aBCI |
| Brain-computer music interfaces | BCMI |
| Affective algorithm composition | AAC |
| Steady-state visual evoked potentials | SSVEP |
| Discriminative and multi-scale filter bank tangent space mapping | DMFBTSM |
| Inter stimulus interval | ISI |
| Multiscale-CNN | MS-CNN |
| TrAdaBoost based on cross-validation and an adaptive threshold | CV-T-TAB |
| Canonical correlation analysis | CCA |
| Wavelet Transform | WT |
| Brain/neural exoskeleton | B/NE |
References
- Ramsey, N.F.; Millán, J.D.R. Brain-Computer Interfaces; Elsevier: Amsterdam, The Netherlands, 2020; ISBN 978-0-444-63934-9. [Google Scholar]
- Allison, B.Z.; Dunne, S.; Leeb, R.; Millán, J.D.R.; Nijholt, A. Towards Practical Brain-Computer Interfaces: Bridging the Gap from Research to Real-World Applications; Springer: Berlin/Heidelberg, Germany, 2012. [Google Scholar]
- Mason, S.G.; Birch, G.E. A general framework for brain-computer interface design. IEEE Trans. Neural Syst. Rehabil. Eng. 2003, 11, 70–85. [Google Scholar] [CrossRef] [PubMed]
- Kawala-Sterniuk, A.; Browarska, N.; Al-Bakri, A.; Pelc, M.; Zygarlicki, J.; Sidikova, M.; Martinek, R.; Gorzelanczyk, E.J. Summary of over Fifty Years with Brain-Computer Interfaces—A Review. Brain Sci. 2021, 11, 43. [Google Scholar] [CrossRef] [PubMed]
- Kübler, A. The history of BCI: From a vision for the future to real support for personhood in people with locked-in syndrome. Neuroethics 2019, 13, 163–180. [Google Scholar] [CrossRef]
- Bamdad, M.; Zarshenas, H.; Auais, M.A. Application of BCI systems in neurorehabilitation: A scoping review. Disabil. Rehabilitation Assist. Technol. 2015, 10, 355–364. [Google Scholar] [CrossRef]
- Kingwell, K. Neurally controlled robotic arm enables tetraplegic patient to drink coffee of her own volition. Nat. Rev. Neurol. 2012, 8, 353. [Google Scholar] [CrossRef]
- Ethier, C.; Oby, E.R.; Bauman, M.J.; Miller, L.E. Restoration of grasp following paralysis through brain-controlled stimulation of muscles. Nature 2012, 485, 368–371. [Google Scholar] [CrossRef] [Green Version]
- Hochberg, L.R.; Bacher, D.; Jarosiewicz, B.; Masse, N.Y.; Simeral, J.D.; Vogel, J.; Haddadin, S.; Liu, J.; Cash, S.S.; Van Der Smagt, P.; et al. Reach and grasp by people with tetraplegia using a neurally controlled robotic arm. Nature 2012, 485, 372–375. [Google Scholar] [CrossRef] [Green Version]
- Ajiboye, A.B.; Willett, F.R.; Young, D.R.; Memberg, W.D.; Murphy, B.A.; Miller, J.P.; Walter, B.L.; Sweet, J.; Hoyen, H.A.; Keith, M.W.; et al. Restoration of reaching and grasping movements through brain-controlled muscle stimulation in a person with tetraplegia: A proof-of-concept demonstration. Lancet 2017, 389, 1821–1830. [Google Scholar] [CrossRef] [Green Version]
- Weyand, S.; Schudlo, L.; Takehara-Nishiuchi, K.; Chau, T. Usability and performance-informed selection of personalized mental tasks for an online near-infrared spectroscopy brain-computer interface. Neurophotonics 2015, 2, 025001. [Google Scholar] [CrossRef] [Green Version]
- McConnell, A.; Moioli, R.; Brasil, F.; Vallejo, M.; Corne, D.; Vargas, P.; Stokes, A. Robotic devices and brain-machine interfaces for hand rehabilitation post-stroke. J. Rehabil. Med. 2017, 49, 449–460. [Google Scholar] [CrossRef]
- Bormane, D.S.; Patil, S.T.; Ingole, D.T.; Mahajan, A. High performance EEG analysis for brain interface. In Proceedings of the 13th International Conference on Biomedical Engineering, Singapore, 3–6 December 2008; pp. 69–72. [Google Scholar]
- Arvaneh, M.; Guan, C.; Ang, K.K.; Quek, C. Optimizing the Channel Selection and Classification Accuracy in EEG-Based BCI. IEEE Trans. Biomed. Eng. 2011, 58, 1865–1873. [Google Scholar] [CrossRef] [PubMed]
- Weyand, S.; Takehara-Nishiuchi, K.; Chau, T. Exploring Methodological Frameworks for A Mental Task-Based Near-Infrared Spectroscopy Brain-Computer Interface. J. Neurosci. Methods 2015, 254, 36–45. [Google Scholar] [CrossRef] [PubMed]
- Mastakouri, A.A.; Weichwald, S.; Özdenizci, O.; Meyer, T.; Schölkopf, B.; Grosse-Wentrup, M. Personalized brain-computer interface models for motor rehabilitation. In Proceedings of the 2017 IEEE International Conference on Systems, Man, and Cybernetics (SMC), Banff, AB, Canada, 5–8 October 2017; pp. 3024–3029. [Google Scholar]
- Qi, W.; Aliverti, A. A Multimodal Wearable System for Continuous and Real-Time Breathing Pattern Monitoring During Daily Activity. IEEE J. Biomed. Health Inform. 2019, 24, 2199–2207. [Google Scholar] [CrossRef] [PubMed]
- Lotte, F.; Congedo, M.; Lécuyer, A.; Lamarche, F.; Arnaldi, B. A review of classification algorithms for EEG-based brain–computer interfaces. J. Neural Eng. 2007, 4, R1. [Google Scholar] [CrossRef] [Green Version]
- Astigarraga, A.; Arruti, A.; Muguerza, J.; Santana, R.; Martin, J.I.; Sierra, B. User adapted motor-imaginary brain-computer interface by means of EEG channel selection based on estimation of distributed algorithms. Math. Probl. Eng. 2016, 2016, 1435321. [Google Scholar] [CrossRef] [Green Version]
- Yun-Fa, F.; Yue-Chao, W.; Hong-Yi, L.; Bao-Lei, X.; Yong-Cheng, L. Direct brain-controlled robot interface technology. Acta Autom. Sin. 2012, 38, 1229–1246. [Google Scholar]
- Aswinseshadri, K. Evaluation of feature selection in Brain Computer Interface. In Proceedings of the 2nd International Conference on Advances in Electrical, Electronics, Information, Communication and Bio-Informatics (AEEICB), Chennai, India, 27–28 February 2016; pp. 93–97. [Google Scholar]
- Li, Y.; Koike, Y.; Sugiyama, M. A Framework of Adaptive Brain Computer Interfaces. In Proceedings of the International Conference on Biomedical Engineering & Informatics, Tianjin, China, 17–19 October 2009. [Google Scholar]
- Stieglitz, T.; Rubehn, B.; Henle, C.; Kisban, S.; Herwik, S.; Ruther, P.; Schuettler, M. Brain–computer interfaces: An overview of the hardware to record neural signals from the cortex. Prog. Brain Res. 2009, 175, 297–315. [Google Scholar] [CrossRef]
- Dangi, S.; Gowda, S.; Heliot, R.; Carmena, J.M. Adaptive Kalman filtering for closed-loop Brain-Machine Interface systems. In Proceedings of the 5th International IEEE/EMBS Conference on Neural Engineering, Cancun, Mexico, 27 April–1 May 2011; pp. 609–612. [Google Scholar] [CrossRef]
- Rejer, I.; Górski, P. Independent Component Analysis for EEG data preprocessing-algorithms comparison. In Proceedings of the IFIP International Conference on Computer Information Systems and Industrial Management, Krakow, Poland, 25–27 September 2013; pp. 108–119. [Google Scholar]
- Shin, H.; Chung, W. Brain computer interface approach using sensor covariance matrix with forced whitening. In Proceedings of the 2017 5th International Winter Conference on Brain-Computer Interface (BCI), Gangwon, Korea, 9–11 January 2017; pp. 66–68. [Google Scholar]
- Sun, H.; Zhang, L.; Li, J.; Zhao, Q. EEG Based Brain-Computer Interface System for Remote Vehicle Controlling. In Advances in Cognitive Neurodynamics (II); Springer: Dordrecht, The Netherlands, 2011; pp. 695–699. [Google Scholar]
- Chen, X.; Li, C.; Liu, A.; McKeown, M.J.; Qian, R.; Wang, Z.J. Toward Open-World Electroencephalogram Decoding Via Deep Learning: A comprehensive survey. IEEE Signal Process. Mag. 2022, 39, 117–134. [Google Scholar] [CrossRef]
- Naseer, N.; Hong, K.-S. fNIRS-based brain-computer interfaces: A review. Front. Hum. Neurosci. 2015, 9, 3. [Google Scholar] [CrossRef] [Green Version]
- Lyu, X.; Ding, P.; Li, S.; Dong, Y.; Su, L.; Zhao, L.; Gong, A.; Fu, Y. Human factors engineering of BCI: An evaluation for satisfaction of BCI based on motor imagery. Cogn. Neurodyn. 2022. [Google Scholar] [CrossRef]
- Wang, J.G.; Shao, H.M.; Yao, Y.; Liu, J.L.; Ma, S.W. A Personalized Feature Extraction and Classification Method for Motor Imagery Recognition. Mob. Netw. Appl. 2021, 26, 1359–1371. [Google Scholar] [CrossRef]
- Hamburg, M.A.; Collins, F.S. The path to personalized medicine. New Engl. J. Med. 2010, 363, 301–304. [Google Scholar] [CrossRef] [PubMed]
- Yeo, S.N.; Lee, T.S.; Sng, W.T.; Heo, M.Q.; Bautista, D.; Cheung, Y.B.; Zhang, H.H.; Wang, C.; Chin, Z.Y.; Feng, L.; et al. Effectiveness of a Personalized Brain-Computer Interface System for Cognitive Training in Healthy Elderly: A Randomized Controlled Trial. J. Alzheimer’s Dis. 2018, 66, 127–138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuzovkin, I.; Tretyakov, K.; Uusberg, A.; Vicente, R. Mental state space visualization for interactive modeling of personalized BCI control strategies. J. Neural Eng. 2020, 17, 016059. [Google Scholar] [CrossRef]
- Rodríguez-Ugarte, M.; Iáñez, E.; Ortíz, M.; Azorín, J.M. Personalized offline and pseudo-online BCI models to detect pedaling intent. Front. Neuroinformatic 2017, 11, 45. [Google Scholar] [CrossRef] [Green Version]
- Kalaganis, F.P.; Laskaris, N.A.; Chatzilari, E.; Nikolopoulos, S.; Kompatsiaris, I. A Data Augmentation Scheme for Geometric Deep Learning in Personalized Brain–Computer Interfaces. IEEE Access 2020, 8, 162218–162229. [Google Scholar] [CrossRef]
- Bashashati, H.; Ward, R.K.; Bashashati, A. User-customized brain computer interfaces using Bayesian optimiza-tion. J. Neural Eng. 2016, 13, 026001. [Google Scholar] [CrossRef]
- Jia, C.; Gao, X.; Hong, B.; Gao, S. Frequency and Phase Mixed Coding in SSVEP-Based Brain—Computer Interface. IEEE Trans. Biomed. Eng. 2010, 58, 200–206. [Google Scholar] [CrossRef]
- Tanji, Y.; Nakanishi, M.; Suefusa, K.; Tanaka, T. Waveform-Based Multi-Stimulus Coding for Brain-Computer Interfaces Based on Steady-State Visual Evoked Potentials. In Proceedings of the 2018 IEEE International Conference on Acoustics, Speech and Signal Processing (ICASSP), Calgary, AB, Canada, 15–20 April 2018; pp. 821–825. [Google Scholar] [CrossRef]
- Abiri, R.; Borhani, S.; Sellers, E.W.; Jiang, Y.; Zhao, X. A comprehensive review of EEG-based brain–computer interface paradigms. J. Neural Eng. 2018, 16, 011001. [Google Scholar] [CrossRef]
- Rezeika, A.; Benda, M.; Stawicki, P.; Gembler, F.; Saboor, A.; Volosyak, I. Brain–Computer Interface Spellers: A Review. Brain Sci. 2018, 8, 57. [Google Scholar] [CrossRef] [Green Version]
- Kaski, S.; Joutsiniemi, S.L. Monitoring EEG signal with the self-organizing map. In Proceedings of the International Conference on Artificial Neural Networks, San Francisco, CA, USA, 28 March–1 April 1993; pp. 974–977. [Google Scholar]
- Uma, M.; Sheela, T. Analysis of Collaborative Brain Computer Interface (BCI) based Personalized GUI for Differently Abled. Intell. Autom. Soft Comput. 2018, 24, 747–757. [Google Scholar] [CrossRef]
- Wu, X.; Zheng, L.; Jiang, L.; Huang, X.; Liu, Y.; Xing, L.; Xing, X.; Wang, Y.; Pei, W.; Yang, X.; et al. A Dry Electrode Cap and Its Application in a Steady-State Visual Evoked Potential-Based Brain–Computer Interface. Electronics 2019, 8, 1080. [Google Scholar] [CrossRef] [Green Version]
- Volosyak, I.; Valbuena, D.; Malechka, T.; Peuscher, J.; Gräser, A. Brain–computer interface using water-based elec-trodes. J. Neural Eng. 2010, 7, 066007. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.-L.; Liao, L.-D.; Liou, C.-H.; Chen, S.-A.; Ko, L.-W.; Chen, B.-W.; Wang, P.-S.; Chen, S.-F.; Lin, C.-T. Design of the multi-channel electroencephalography-based brain-computer interface with novel dry sensors. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. 2012, 2012, 1793–1797. [Google Scholar] [CrossRef]
- Nicolaou, N.; Georgiou, J. Monitoring Depth of Hypnosis under Propofol General Anaesthesia-Granger Causality and Hidden Markov Models. In Special Session on Brain-computer Interfaces and Brain Stimulation for Neurorehabilitation; SCITEPRESS: Setúbal, Portugal, 2013; Volume 2, pp. 256–261. [Google Scholar]
- Lee, M.; Yoon, J.-G.; Lee, S.-W. Predicting Motor Imagery Performance from Resting-State EEG Using Dynamic Causal Modeling. Front. Hum. Neurosci. 2020, 14, 321. [Google Scholar] [CrossRef]
- Lopes-Dias, C.; Sburlea, A.I.; Müller-Putz, G.R. A generic error-related potential classifier offers a comparable performance to a personalized classifier. In Proceedings of the 2020 42nd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Montreal, QC, Canada, 20–24 July 2020; pp. 2995–2998. [Google Scholar]
- Abarbanel, A. Gates, states, rhythms, and resonances: The scientific basis of neurofeedback training. J. Neurother. 1995, 1, 15–38. [Google Scholar] [CrossRef] [Green Version]
- Omejc, N.; Rojc, B.; Battaglini, P.P.; Marusic, U. Review of the therapeutic neurofeedback method using electroencephalography: EEG Neurofeedback. Bosn. J. Basic Med. Sci. 2019, 19, 213. [Google Scholar] [CrossRef] [Green Version]
- Martin, S.; Armstrong, E.; Thomson, E.; Vargiu, E.; Solà, M.; Dauwalder, S.; Miralles, F.; Daly Lynn, J. A qualitative study adopting a user-centered approach to design and validate a brain computer interface for cognitive rehabilitation for people with brain injury. Assist. Technol. 2018, 30, 233–241. [Google Scholar] [CrossRef]
- Liberati, G.; Pizzimenti, A.; Simione, L.; Riccio, A.; Schettini, F.; Inghilleri, M.; Mattia, D.; Cincotti, F. Developing brain-computer interfaces from a user-centered perspective: Assessing the needs of persons with amyotrophic lateral sclerosis, caregivers, and professionals. Appl. Ergon. 2015, 50, 139–146. [Google Scholar] [CrossRef]
- Lu, X.; Ding, P.; Li, S.; Gong, A.; Zhao, L.; Qian, Q.; Su, L.; Fu, Y. Human factors engineering of brain-computer interface and its applications: Human-centered brain-computer interface design and evaluation methodology. J. Biomed. Eng. 2021, 38, 210–223. [Google Scholar]
- Chan, S.; Chan, A. The validity and applicability of the Chinese version of the quebec user evaluation of satisfaction with assistive technology for people with spinal cord injury. Assist. Technol. 2006, 18, 25–33. [Google Scholar] [CrossRef] [PubMed]
- Colucci, M.; Tofani, M.; Trioschi, D.; Guarino, D.; Berardi, A.; Galeoto, G. Reliability and validity of the Italian version of Quebec User Evaluation of Satisfaction with Assistive Technology 2.0 (QUEST-IT 2.0) with users of mobility assistive device. Disabil. Rehabil. Assist. Technol. 2019, 16, 251–254. [Google Scholar] [CrossRef] [PubMed]
- Arjona, C.; Pentácolo, J.; Gareis, I.; Atum, Y.; Gentiletti, G.; Acevedo, R.; Rufiner, H.L. Evaluation of LDA Ensembles Classifiers for Brain Computer Interface. J. Physics: Conf. Ser. 2011, 332, 012025. [Google Scholar] [CrossRef]
- Kübler, A.; Holz, E.M.; Riccio, A.; Zickler, C.; Kaufmann, T.; Kleih, S.C.; Staiger-Sälzer, P.; Desideri, L.; Hoogerwerf, E.J.; Mattia, D. The user-centered design as novel perspective for evaluating the usability of BCI-controlled applications. PLoS ONE 2014, 9, e112392. [Google Scholar] [CrossRef] [Green Version]
- Zickler, C.; Riccio, A.; Leotta, F.; Hillian-Tress, S.; Halder, S.; Holz, E.; Staiger-Sälzer, P.; Hoogerwerf, E.-J.; Desideri, L.; Mattia, D.; et al. A Brain-Computer Interface as Input Channel for a Standard Assistive Technology Software. Clin. EEG Neurosci. 2011, 42, 236–244. [Google Scholar] [CrossRef]
- Abiri, R.; Zhao, X.; Heise, G.; Jiang, Y.; Abiri, F. Brain computer interface for gesture control of a social robot: An offline study. In Proceedings of the 2017 Iranian Conference on Electrical Engineering (ICEE), Tehran, Iran, 2–4 May 2017; pp. 113–117. [Google Scholar]
- Coscia, M.; Wessel, M.J.; Chaudary, U.; Millan, J.D.R.; Micera, S.; Guggisberg, A.; Vuadens, P.; Donoghue, J.; Birbaumer, N.; Hummel, F.C. Neurotechnology-aided interventions for upper limb motor rehabilitation in severe chronic stroke. Brain 2019, 142, 2182–2197. [Google Scholar] [CrossRef] [Green Version]
- Vinoj, P.G.; Jacob, S.; Menon, V.G.; Rajesh, S.; Khosravi, M.R. Brain-Controlled Adaptive Lower Limb Exoskeleton for Rehabilitation of Post-Stroke Paralyzed. IEEE Access 2019, 7, 132628–132648. [Google Scholar] [CrossRef]
- Bronte-Stewart, H.M.; Petrucci, M.N.; O’Day, J.J.; Afzal, M.F.; Parker, J.E.; Kehnemouyi, Y.M.; Wilkins, K.B.; Orthlieb, G.C.; Hoffman, S.L. Perspective: Evolution of control variables and policies for closed-loop deep brain stimulation for Parkinson’s disease using bidirectional deep-brain-computer interfaces. Front. Hum. Neurosci. 2020, 14, 353. [Google Scholar] [CrossRef]
- Kübler, A.; Kleih, S.; Mattia, D. Brain Computer Interfaces for Cognitive Rehabilitation After Stroke; Springer: Berlin/Heidelberg, Germany, 2017. [Google Scholar]
- Mane, R.; Chew, E.; Phua, K.S.; Ang, K.K.; Robinson, N.; Vinod, A.P.; Guan, C. Prognostic and monitory EEG-biomarkers for BCI upper-limb stroke rehabilitation. IEEE Trans. Neural Syst. Rehabil. Eng. 2019, 27, 1654–1664. [Google Scholar] [CrossRef]
- Parastarfeizabadi, M.; Kouzani, A.Z. Advances in closed-loop deep brain stimulation devices. J. Neuroeng. Rehabilitation 2017, 14, 79. [Google Scholar] [CrossRef]
- Campanella, S. Why it is time to develop the use of cognitive event-related potentials in the treatment of psychiatric diseases. Neuropsychiatr. Dis. Treat. 2013, 9, 1835–1845. [Google Scholar] [CrossRef] [PubMed]
- He, Z.; Li, Z.; Yang, F.; Wang, L.; Li, J.; Zhou, C.; Pan, J. Advances in Multimodal Emotion Recognition Based on Brain–Computer Interfaces. Brain Sci. 2020, 10, 687. [Google Scholar] [CrossRef] [PubMed]
- Daly, I.; Williams, D.; Malik, A.; Weaver, J.; Kirke, A.; Hwang, F.; Miranda, E.; Nasuto, S.J. Personalised, multi-modal, affective state detection for hybrid brain-computer music interfacing. IEEE Trans. Affect. Comput. 2018, 11, 111–124. [Google Scholar] [CrossRef] [Green Version]
- Abiri, R.; Borhani, S.; Kilmarx, J.; Esterwood, C.; Jiang, Y.; Zhao, X. A Usability Study of Low-Cost Wireless Brain-Computer Interface for Cursor Control Using Online Linear Model. IEEE Trans. Human-Machine Syst. 2020, 50, 287–297. [Google Scholar] [CrossRef]
- Colucci, A.; Vermehren, M.; Cavallo, A.; Angerhöfer, C.; Peekhaus, N.; Zollo, L.; Kim, W.-S.; Paik, N.-J.; Soekadar, S.R. Brain–Computer Interface-Controlled Exoskeletons in Clinical Neurorehabilitation: Ready or Not? Neurorehabilit. Neural Repair 2022, 36, 747–756. [Google Scholar] [CrossRef]
- Cuomo, G.; Maglianella, V.; Ghooshchy, S.G.; Zoccolotti, P.; Martelli, M.; Paolucci, S.; Morone, G.; Iosa, M. Motor imagery and gait control in Parkinson’s disease: Techniques and new perspectives in neurorehabilitation. Expert Rev. Neurother. 2021, 22, 43–51. [Google Scholar] [CrossRef]
- Paggiaro, A.; Birbaumer, N.; Cavinato, M.; Turco, C.; Formaggio, E.; Del Felice, A.; Masiero, S.; Piccione, F. Magnetoencephalography in Stroke Recovery and Rehabilitation. Front. Neurol. 2016, 7, 35. [Google Scholar] [CrossRef] [Green Version]
- Habelt, B.; Wirth, C.; Afanasenkau, D.; Mihaylova, L.; Winter, C.; Arvaneh, M.; Minev, I.R.; Bernhardt, N. A multimodal neuroprosthetic interface to record, modulate and classify electrophysiological correlates of cognitive function. bioRxiv 2021, bioRxiv 2021.07.29.454271. [Google Scholar]
- Boggio, P.S.; Rigonatti, S.P.; Ribeiro, R.B.; Myczkowski, M.L.; Nitsche, M.A.; Pascual-Leone, A.; Fregni, F. A randomized, double-blind clinical trial on the efficacy of cortical direct current stimulation for the treatment of major depression. Int. J. Neuropsychopharmacol. 2008, 11, 249–254. [Google Scholar] [CrossRef] [Green Version]
- Gomes, J.; Trevizol, A.; Ducos, D.; Gadelha, A.; Ortiz, B.; Fonseca, A.; Akiba, H.; Azevedo, C.; Guimaraes, L.; Shiozawa, P.; et al. Effects of transcranial direct current stimulation on working memory and negative symptoms in schizophrenia: A phase II randomized sham-controlled trial. Schizophr. Res. Cogn. 2018, 12, 20–28. [Google Scholar] [CrossRef]
- Knight, R.T.; Staines, W.R.; Swick, D.; Chao, L.L. Prefrontal cortex regulates inhibition and excitation in distributed neural networks. Acta Psychol. 1999, 101, 159–178. [Google Scholar] [CrossRef] [PubMed]
- Ehlers, C.L.; Desikan, A.; Wills, D.N. Event-related potential responses to the acute and chronic effects of alcohol in adolescent and adult Wistar rats. Alcohol. Clin. Exp. Res. 2014, 38, 749–759. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marco, J.; Fuentemilla, L.; Grau, C. Auditory sensory gating deficit in abstinent chronic alcoholics. Neurosci. Lett. 2005, 375, 174–177. [Google Scholar] [CrossRef]
- Fellous, J.-M.; Sapiro, G.; Rossi, A.; Mayberg, H.; Ferrante, M. Explainable Artificial Intelligence for Neuroscience: Behavioral Neurostimulation. Front. Neurosci. 2019, 13, 1346. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ehlers, C. ERP responses to ethanol and diazepam administration in squirrel monkeys. Alcohol 1988, 5, 315–320. [Google Scholar] [CrossRef] [PubMed]
- Cohen, H.L.; Ji, J.; Chorlian, D.B.; Begleiter, H.; Porjesz, B. Alcohol-related ERP Changes Recorded from Different Modalities: A Topographic Analysis. Alcohol. Clin. Exp. Res. 2002, 26, 303–317. [Google Scholar] [CrossRef]
- Thieme, A.; Belgrave, D.; Doherty, G. Machine Learning in Mental Health. ACM Trans. Comput. Interact. 2020, 27, 1–53. [Google Scholar] [CrossRef]
- Yan, W.; Liu, X.; Shan, B.; Zhang, X.; Pu, Y. Research on the Emotions Based on Brain-Computer Technology: A Bibliometric Analysis and Research Agenda. Front. Psychol. 2021, 12, 4995. [Google Scholar] [CrossRef]
- Gilleade, K.; Dix, A.; Allanson, J. Affective videogames and modes of affective gaming: Assist me, challenge me, emote me. In Proceedings of the International Conference on Changing Views, Vancouver, BC, Canada, 16–20 June 2005. [Google Scholar]
- Daly, I.; Malik, A.; Weaver, J.; Hwang, F.; Nasuto, S.J.; Williams, D.; Kirke, A.; Miranda, E. Identifying music-induced emotions from EEG for use in brain-computer music interfacing. In Proceedings of the 2015 International Conference on Affective Computing and Intelligent Interaction (ACII), Xi’an, China, 21–24 September 2015; pp. 923–929. [Google Scholar]
- Williams, D.; Kirke, A.; Miranda, E.R.; Roesch, E.; Daly, I.; Nasuto, S. Investigating affect in algorithmic composition systems. Psychol. Music. 2014, 43, 831–854. [Google Scholar] [CrossRef]
- Delisle-Rodriguez, D.; Cardoso, V.; Gurve, D.; Loterio, F.; Romero-Laiseca, M.A.; Krishnan, S.; Bastos-Filho, T. System based on subject-specific bands to recognize pedaling motor imagery: Towards a BCI for lower-limb rehabilitation. J. Neural Eng. 2019, 16, 056005. [Google Scholar] [CrossRef] [Green Version]
- Wu, F.; Gong, A.; Li, H.; Zhao, L.; Zhang, W.; Fu, Y. A new subject-specific discriminative and multi-scale filter bank tangent space mapping method for recognition of multiclass motor imagery. Front. Hum. Neurosci. 2021, 15, 595723. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.; Sharma, A.; Tsunoda, T. Subject-specific-frequency-band for motor imagery eeg signal recognition based on common spatial spectral pattern. In Proceedings of the Pacific Rim International Conference on Artificial Intelligence, Cuvu, Yanuka Island, Fiji, 26–30 August 2019; pp. 712–722. [Google Scholar]
- Gaur, P.; McCreadie, K.; Pachori, R.B.; Wang, H.; Prasad, G. An automatic subject specific channel selection method for enhancing motor imagery classification in EEG-BCI using correlation. Biomed. Signal Process. Control. 2021, 68, 102574. [Google Scholar] [CrossRef]
- Sellers, E.W.; Krusienski, D.J.; McFarland, D.J.; Vaughan, T.M.; Wolpaw, J.R. A P300 event-related potential brain–computer interface (BCI): The effects of matrix size and inter stimulus interval on performance. Biol. Psychol. 2006, 73, 242–252. [Google Scholar] [CrossRef] [PubMed]
- Erdogan, B.; Gencer, N.G. Application of wiener deconvolution model in p300 spelling paradigm. In Proceedings of the 2009 14th National Biomedical Engineering Meeting, Izmir, Turkey, 20–22 May 2009; pp. 1–4. [Google Scholar]
- Wang, H.; Pei, Z.; Xu, L.; Xu, T.; Bezerianos, A.; Sun, Y.; Li, J. Performance enhancement of P300 detection by multiscale-CNN. IEEE Trans. Instrum. Meas. 2021, 70, 1–12. [Google Scholar] [CrossRef]
- Li, M.; Lin, F.; Xu, G. A TrAdaBoost Method for Detecting Multiple Subjects’ N200 and P300 Potentials Based on Cross-Validation and an Adaptive Threshold. Int. J. Neural Syst. 2020, 30, 2050009. [Google Scholar] [CrossRef]
- Ravi, A.; Pearce, S.; Zhang, X.; Jiang, N. User-specific channel selection method to improve SSVEP BCI decoding robustness against variable inter-stimulus distance. In Proceedings of the 2019 9th International IEEE/EMBS Conference on Neural Engineering (NER), San Francisco, CA, USA, 20–23 March 2019; pp. 283–286. [Google Scholar]
- Rejer, I. Wavelet transform in detection of the subject specific frequencies for SSVEP-based BCI. In Proceedings of the International Multi-Conference on Advanced Computer Systems, Miedzyzdroje, Poland, 19–21 October 2016; pp. 146–155. [Google Scholar]
- Mehdizavareh, M.H.; Hemati, S.; Soltanian-Zadeh, H. Enhancing performance of subject-specific models via subject-independent information for SSVEP-based BCIs. PLoS ONE 2020, 15, e0226048. [Google Scholar] [CrossRef] [Green Version]
- Peters, B.; Higger, M.; Quivira, F.; Bedrick, S.; Dudy, S.; Eddy, B.; Kinsella, M.; Memmott, T.; Wiedrick, J.; Fried-Oken, M.; et al. Effects of simulated visual acuity and ocular motility impairments on SSVEP brain-computer interface performance: An experiment with Shuffle Speller. Brain-Comput. Interfaces 2018, 5, 58–72. [Google Scholar] [CrossRef]
- Hsu, C.-C.; Yeh, C.-L.; Lee, W.-K.; Hsu, H.-T.; Shyu, K.-K.; Li, L.P.-H.; Wu, T.-Y.; Lee, P.-L. Extraction of high-frequency SSVEP for BCI control using iterative filtering based empirical mode decomposition. Biomed. Signal Process. Control 2020, 61, 102022. [Google Scholar] [CrossRef]
- Yu, X.; Qi, W. A user study of wearable EEG headset products for emotion analysis. In Proceedings of the 2018 International Conference on Algorithms, Computing and Artificial Intelligence, Sanya, China, 21 December 2018; pp. 1–7. [Google Scholar]
- Qi, W.; Ovur, S.E.; Li, Z.; Marzullo, A.; Song, R. Multi-sensor guided hand gesture recognition for a teleoperated robot using a recurrent neural network. IEEE Robot. Autom. Lett. 2021, 6, 6039–6045. [Google Scholar] [CrossRef]
- Borton, D.; Micera, S.; Millán, J.D.R.; Courtine, G. Personalized neuroprosthetics. Sci. Transl. Med. 2013, 5, 210rv2. [Google Scholar] [CrossRef]
- Chi, X.; Wan, C.; Wang, C.; Zhang, Y.; Chen, X.; Cui, H. A Novel Hybrid Brain-Computer Interface Combining Motor Imagery and Intermodulation Steady-State Visual Evoked Potential. IEEE Trans. Neural Syst. Rehabil. Eng. 2022, 30, 1525–1535. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reference | Specific Works for Personalized BCI | Personalized Component |
|---|---|---|
| Weyand et al., 2015 [15] | Proposes the use of personalized mental tasks; explores a user-centered approach Proposes user-selected weighted slope scores (WS-US) and user-selected pair-wise accuracy rankings (PWAR-US) | Personalized BCI paradigm |
| Yeo et al., 2018 [33] | Proposes the Repeatable Battery for the Assessment of Neuropsychological Status (RBANS) | |
| Kuzovkin et al., 2019 [34] | Realizes visualization of mental state space for personalized BCI | |
| Wang et al., 2021 [31] | A classifier-based approach for personalized channel selection in deep belief networks is proposed | Personalized channel selection |
| Astigarraga et al., 2016 [19] | Presents a brain–computer interface for motion imaging based on a distributed algorithm for EEG channel selection | |
| Arvaneh et al., 2011 [14] | Proposes a sparse common spatial pattern (SCSP) algorithm for brain signal channel selection | |
| Ugarte et al., 2017 [35] | An algorithm model is proposed to select different types of brain signal processing methods for subjects by predicting their wishes | Personalized feature extraction and selection |
| Bormane et al., 2009 [13] | A feature selection method is proposed to effectively reduce the dimension of multi-channel feature space | |
| Wang et al.,2021 [31] | A personalized feature extraction method based on filter banks and elastic networks is proposed | |
| Kalaganis et al., 2020 [36] | A data enhancement method for graph signals is proposed to improve the accuracy of personalized classification | Personalized classification model |
| Mastakouri et al., 2017 [16] | Proposes a personalized model based on a transfer learning algorithm for the rehabilitation of patients with motion disorders | |
| Bashashati et al., 2016 [37] | Uses a Bayesian-based optimization algorithm to adjust parameters | The whole personalized BCI algorithm |
| Ugarte et al.,2017 [35] | An algorithm model is proposed to select different types of brain signal processing methods for subjects |
| Index | Computing Method | Explanation |
|---|---|---|
| Classification positive accuracy | p is the correct classification rate; Ci,i is the ith element of the diagonal of the confusion matrix; N is the total number of trials | |
| Information transmission rate | ITR is the amount of information transmitted in unit time, N is the target number, P is the accuracy rate, and T is the time required to output an instruction | |
| Cohen’s kappa | Κ is the consistency indicator between nominal scales, Ci,: and C:,i are row i and column i of the confusion matrix, respectively, and N is the total number of trials | |
| Sensitivity | Se is sensitivity, TP is true positive, TN is true negative | |
| Specificity | Sp is specific, TP is true positive, TN is true negative | |
| Noise factor | F is false positive, FP is false positive, TP is true positive | |
| F-measurement | is a measure of classifier performance under different significance levels α, F is the false detection rate, Se is sensitivity | |
| Failure rate [30] | is the failure rate, M is the number of failed BCI products during the working time, N is the total number of BCI products, and Δt is BCI working time | |
| Mean time between failures [30] | MTBF is the mean time between failures; λ is the average failure rate | |
| Fitts Throughput [57] | TP is throughput; ID is index of difficulty; MT is mean movement time | |
| Receiver Operating Characteristic Curve(ROC) [57] | The abscissa of the curve is the false positive rate (FPR). N is the number of real negative samples, and FP is the number of positive samples predicted by the classifier among N negative samples. The ordinate is the true positive rate (TPR). P is the number of real positive samples, and TP is the number of positive samples predicted by the classifier among the P positive samples. | |
| Area Under Curve (AUC) [57] | Calculated by mean and variance | Area under ROC curve, generally between 0.5 and 1 |
| Reference | Applications | Direction |
|---|---|---|
| Abiri et al. 2017 [60] | Designed a social robot based on gesture control. | Auxiliary Control |
| Uma et al. 2017 [43] | Developed a personalized GUI application that collaborated with the EEG device, accessed the user’s needs, | |
| Coscia M et al. 2019 [61] | adjusted and improved the duration and intensity of brain/neural exoskeleton (B/NE)training according to the patient’s individual ability. | |
| Vinoj et al., 2019 [62] | Developed a brain-controlled lower limb exoskeleton, and customized it according to the degree of disability to assist users with lower limb disorders in rehabilitation training. | |
| Bronte-Stewart et al., 2020 [63] | A personalized dual threshold control strategy was proposed to drive closed-loop subthalamic nucleus deep brain stimulation (STN-DBS). | Parkinson’s |
| Kübler et al., 2017 [64] | A neuromental algorithm was developed to assign different neural feedback training modules to different stroke patients. | Cerebral apoplexy |
| Mane et al., 2019 [65] | Used biometric markers to predict patients’ expected responses to existing interventions and provide patients with high expectations. | |
| Parastarfeizabadi et al., 2017 [66] | Adaptive adjustment of stimulus parameters. | Rehabilitation of mental disorders |
| Campanella.,2013 [67] | ERPs and machine learning can help predict the disease progression and treatment results of specific subjects. | |
| He et al., 2020 [68] | Personalized tasks through emotional reflex control and automatically modified the human–computer interaction process. | Emotional recognition |
| Daly et al., 2017 [69] | Developed a high-performance emotional state detection system. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ma, Y.; Gong, A.; Nan, W.; Ding, P.; Wang, F.; Fu, Y. Personalized Brain–Computer Interface and Its Applications. J. Pers. Med. 2023, 13, 46. https://doi.org/10.3390/jpm13010046
Ma Y, Gong A, Nan W, Ding P, Wang F, Fu Y. Personalized Brain–Computer Interface and Its Applications. Journal of Personalized Medicine. 2023; 13(1):46. https://doi.org/10.3390/jpm13010046
Chicago/Turabian StyleMa, Yixin, Anmin Gong, Wenya Nan, Peng Ding, Fan Wang, and Yunfa Fu. 2023. "Personalized Brain–Computer Interface and Its Applications" Journal of Personalized Medicine 13, no. 1: 46. https://doi.org/10.3390/jpm13010046