

Agreement between Wedged Hepatic Venous Pressure and Portal Pressure in Hepatic Sinusoidal Obstruction Syndrome
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Intervention Procedure
2.3. Definitions
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
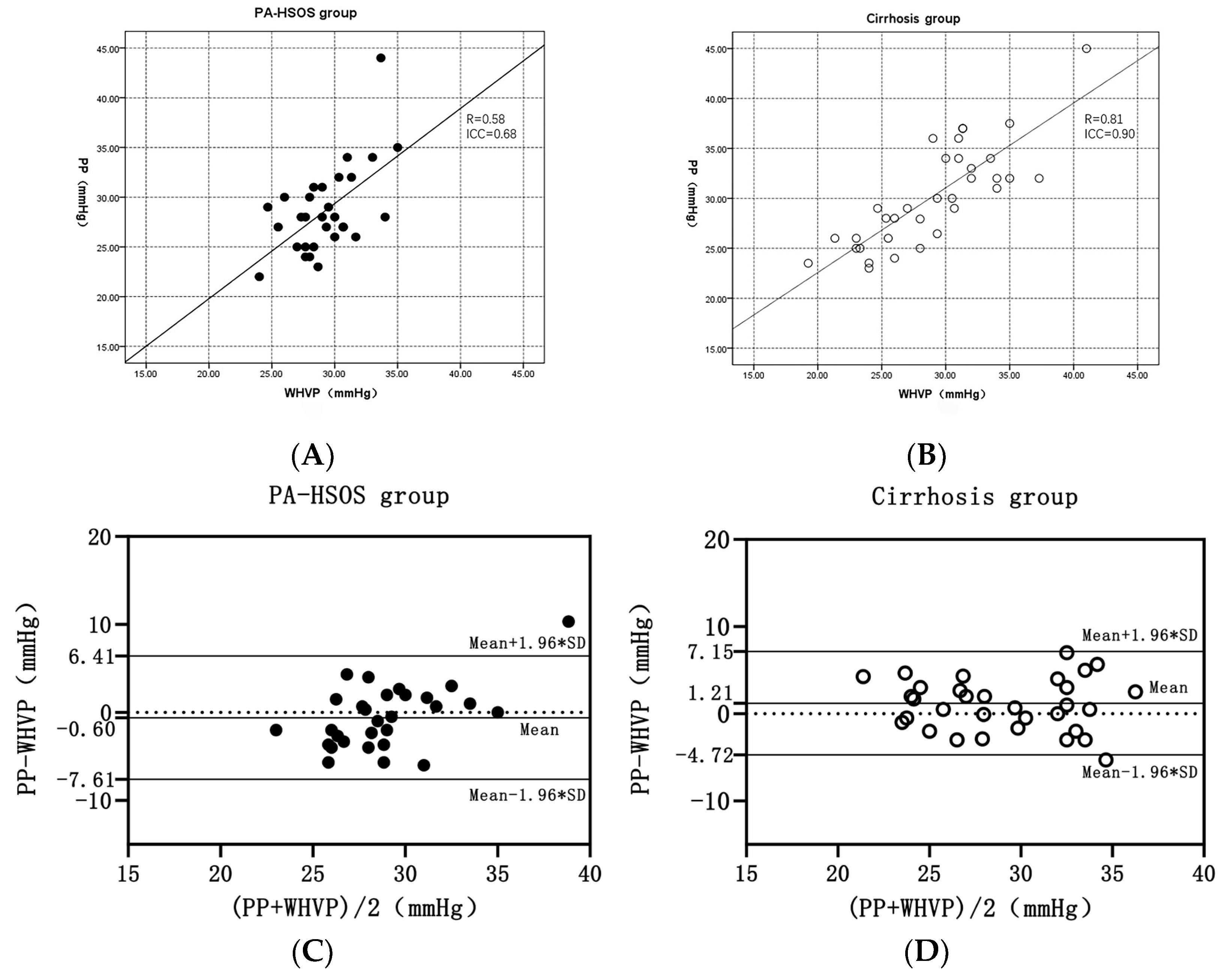
3.2. Correlation between WHVP and PP
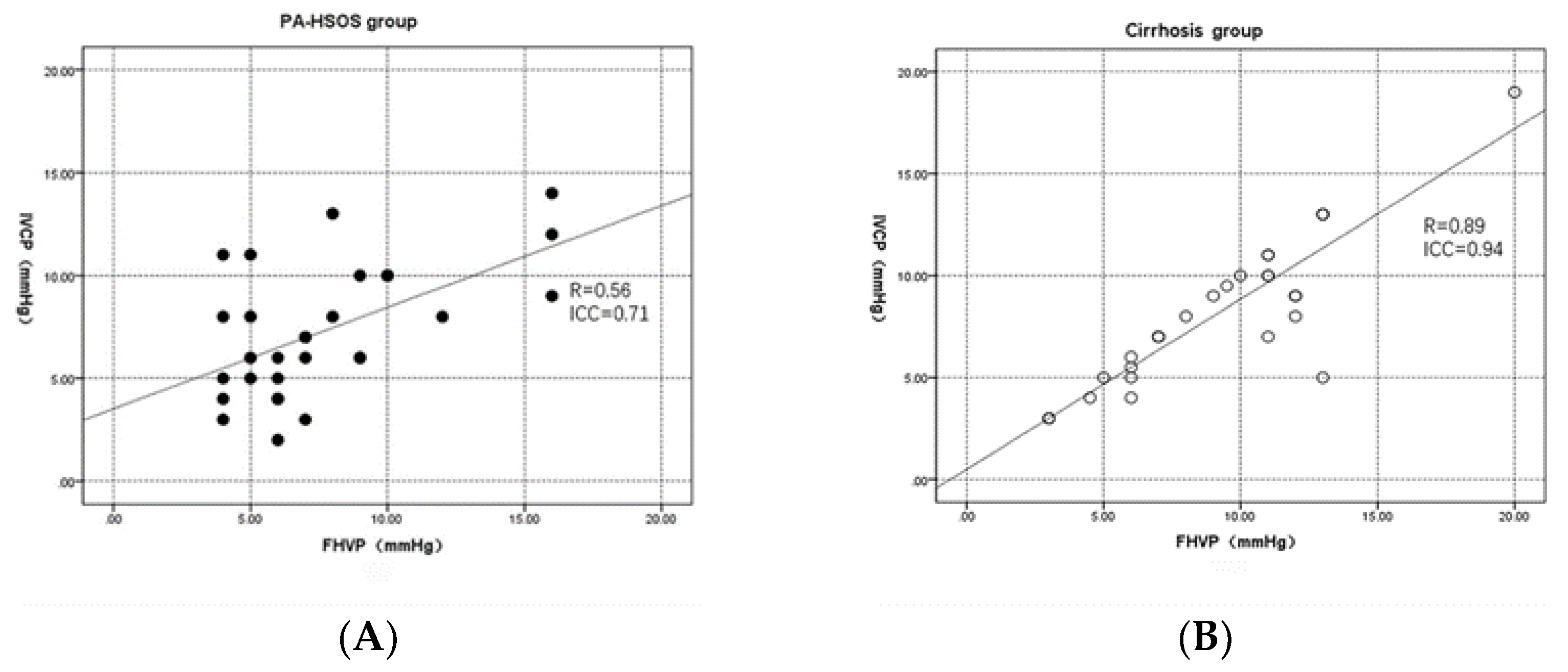
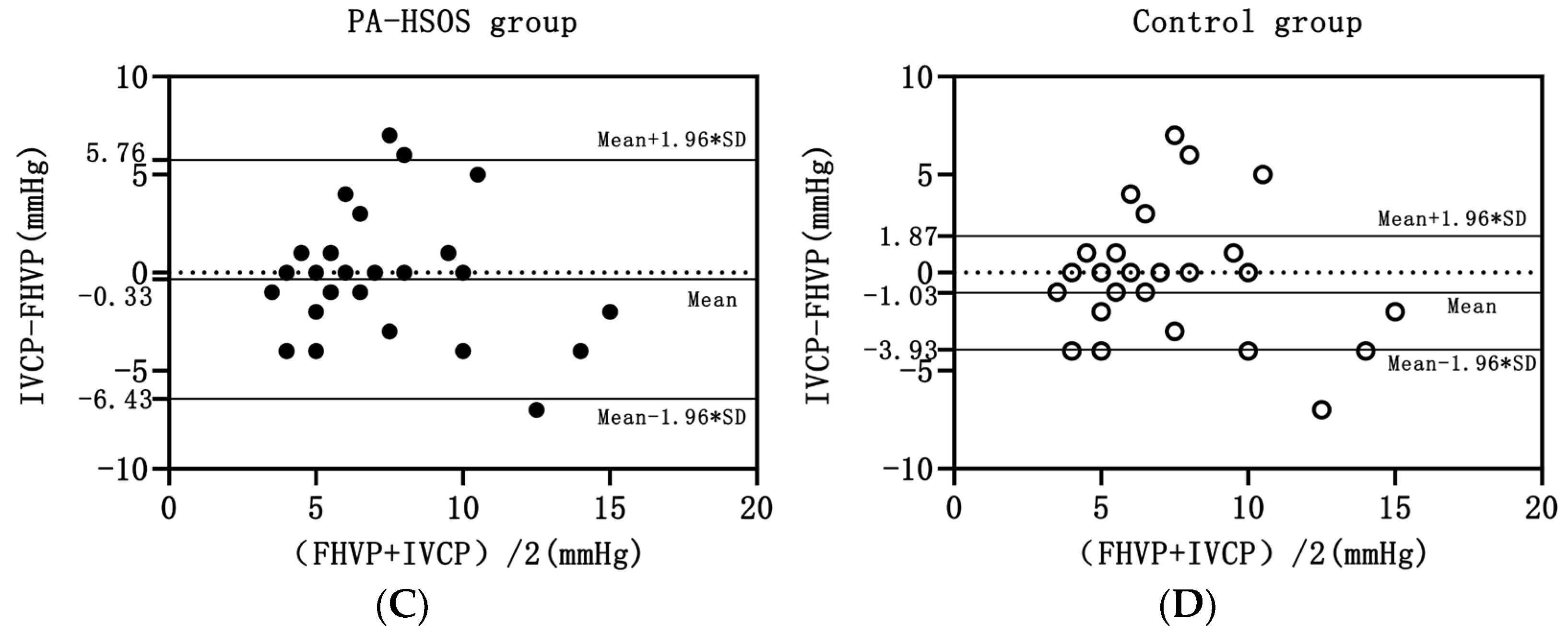
3.3. Correlation between FHVP and IVCP
3.4. Correlation between HVPG and PPG
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hu, Y.; Wen, Z. Validation and comparison of non-invasive prediction models based on liver stiffness measurement to identify patients who could avoid gastroscopy. Sci. Rep. 2021, 11, 150. [Google Scholar] [CrossRef] [PubMed]
- Simonetto, D.A.; Liu, M.; Kamath, P.S. Portal Hypertension and Related Complications: Diagnosis and Management. Mayo Clin. Proc. 2019, 94, 714–726. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bosch, J.; Gonzalez-Abraldes, J.; Berzigotti, A.; Garcia-Pagan, J.C. The clinical use of HVPG measurements in chronic liver disease. Nat. Rev. Gastroenterol. Hepatol. 2009, 6, 573–582. [Google Scholar] [CrossRef] [PubMed]
- Thalheimer, U.; Leandro, G.; Samonakis, D.N.; Triantos, C.K.; Patch, D.; Burroughs, A.K. Assessment of the agreement between wedge hepatic vein pressure and portal vein pressure in cirrhotic patients. Dig. Liver Dis. 2005, 37, 601–608. [Google Scholar] [CrossRef]
- Lin, H.-C.; Tsai, Y.-T.; Lee, F.-Y.; Chang, T.-T.; Wang, S.-S.; Lay, C.-S.; Lee, S.-D.; Lo, K.-J. Comparison between portal vein pressure and wedged hepatic vein pressure in hepatitis B-related cirrhosis. J. Hepatol. 1989, 9, 326–330. [Google Scholar] [CrossRef] [PubMed]
- Zhu, L.; Zhang, C.-Y.; Li, D.-P.; Chen, H.-B.; Ma, J.; Gao, H.; Ye, Y.; Wang, J.-Y.; Fu, P.P.; Lin, G. Tu-San-Qi (Gynura japonica): The culprit behind pyrrolizidine alkaloid-induced liver injury in China. Acta Pharmacol. Sin. 2021, 42, 1212–1222. [Google Scholar] [CrossRef]
- Lin, G.; Wang, J.Y.; Li, N.; Li, M.; Gao, H.; Ji, Y.; Zhang, F.; Wang, H.; Zhou, Y.; Ye, Y.; et al. Hepatic sinusoidal obstruction syndrome associated with consumption of Gynura segetum. J. Hepatol. 2010, 54, 666–673. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Vascular diseases of the liver. J. Hepatol. 2016, 64, 179–202. [Google Scholar] [CrossRef]
- Turco, L.; Garcia-Tsao, G. Portal Hypertension: Pathogenesis and Diagnosis. Clin. Liver Dis. 2019, 23, 573–587. [Google Scholar] [CrossRef]
- Vorobioff, J.; Groszmann, R.J.; Picabea, E.; Gamen, M.; Villavicencio, R.; Bordato, J.; Morel, I.; Audano, M.; Tanno, H.; Lerner, E.; et al. Prognostic value of hepatic venous pressure gradient measurements in alcoholic cirrhosis: A 10-year prospective study. Gastroenterology 1996, 111, 701–709. [Google Scholar] [CrossRef]
- Zhuge, Y.; Liu, Y.; Xie, W.; Zou, X.; Xu, J.; Wang, J.; Chinese Society of Gastroenterology Committee of Hepatobiliary Disease. Expert consensus on the clinical management of pyrrolizidine alkaloid-induced hepatic sinusoidal obstruction syndrome. J. Gastroenterol. Hepatol. 2019, 34, 634–642. [Google Scholar] [CrossRef] [PubMed]
- Zhang, F.; Zhuge, Y.; Zou, X.; Zhang, M.; Peng, C.; Li, Z.; Wang, T. Different scoring systems in predicting survival in Chinese patients with liver cirrhosis undergoing transjugular intrahepatic portosystemic shunt. Eur. J. Gastroenterol. Hepatol. 2014, 26, 853–860. [Google Scholar] [CrossRef] [PubMed]
- Leng, X.; Zhang, F.; Zhang, M.; Guo, H.; Yin, X.; Xiao, J.; Wang, Y.; Zou, X.; Zhuge, Y. Comparison of transjugular intrahepatic portosystemic shunt for treatment of variceal bleeding in patients with cirrhosis with or without spontaneous portosystemic shunt. Eur. J. Gastroenterol. Hepatol. 2019, 31, 853–858. [Google Scholar] [CrossRef] [PubMed]
- Ferrusquía-Acosta, J.; Bassegoda, O.; Turco, L.; Reverter, E.; Pellone, M.; Bianchini, M.; Pérez-Campuzano, V.; Ripoll, E.; García-Criado, Á.; Graupera, I.; et al. Agreement between wedged hepatic venous pressure and portal pressure in non-alcoholic steatohepatitis-related cirrhosis. J. Hepatol. 2021, 74, 811–818. [Google Scholar] [CrossRef] [PubMed]
- Escorsell, À.; Bru, C.; Gilabert, R.; Moitinho, E.; García-Pagán, J.C.; Bosch, J. Wedged hepatic venous pressure adequately reflects portal pressure in hepatitis C virus-related cirrhosis. Hepatology 1999, 30, 1393–1397. [Google Scholar] [CrossRef]
- Yang, X.-Q.; Ye, J.; Li, X.; Li, Q.; Song, Y.-H. Pyrrolizidine alkaloids-induced hepatic sinusoidal obstruction syndrome: Pathogenesis, clinical manifestations, diagnosis, treatment, and outcomes. World J. Gastroenterol. 2019, 25, 3753–3763. [Google Scholar] [CrossRef]
- Zhuge, Y.Z.; Wang, Y.; Zhang, F.; Zhu, C.K.; Zhang, W.; Zhang, M.; He, Q.; Yang, J.; He, J.; Chen, J.; et al. Clinical characteristics and treatment of pyrrolizidine alkaloid-related hepatic vein occlusive disease. Liver Int. 2018, 38, 1867–1874. [Google Scholar] [CrossRef]
- de Franchis, R.; Bosch, J.; Garcia-Tsao, G.; Reiberger, T.; Ripoll, C. Renewing consensus in portal hypertension. J. Hepatol. 2021, 76, 959–974. [Google Scholar] [CrossRef]
- Wang, X.; Zhang, W.; Zhang, M.; Zhang, F.; Xiao, J.; Yin, Q.; Han, H.; Li, T.; Lin, G.; Zhuge, Y. Development of a Drum Tower Severity Scoring (DTSS) system for pyrrolizidine alkaloid-induced hepatic sinusoidal obstruction syndrome. Hepatol. Int. 2022, 16, 669–679. [Google Scholar] [CrossRef]
- Hou, C.; Xu, J.; Qin, H.; Zhu, X.; Fei, Y.; Zhou, L. Efficacy of transjugular intrahepatic portosystemic shunt in the treatment of 21 patients with Gynura segetum-related hepatic sinusoidal obstruction syndrome. Chin. J. Digest. 2019, 39, 251–256. [Google Scholar]
- Groszmann, R.J.; Wongcharatrawee, S. The hepatic venous pressure gradient: Anything worth doing should be done right. Hepatology 2004, 39, 280–283. [Google Scholar] [CrossRef] [PubMed]
- Parikh, S. Hepatic venous pressure gradient: Worth another look? Dig. Dis. Sci. 2009, 54, 1178–1183. [Google Scholar] [CrossRef] [PubMed]
- Merkel, C.; Montagnese, S. Hepatic venous pressure gradient measurement in clinical hepatology. Dig. Liver Dis. 2011, 43, 762–767. [Google Scholar] [CrossRef] [PubMed]
- Krook, H. Estimation of Portal Venous Pressure by Occlusive Hepatic Vein Catheterization. Scand. J. Clin. Lab. Investig. 1953, 5, 285–292. [Google Scholar] [CrossRef]
- Zhang, W.; Peng, C.; Zhang, S.; Huang, S.; Shen, S.; Xu, G.; Zhang, F.; Xiao, J.; Zhang, M.; Zhuge, Y.; et al. EUS-guided portal pressure gradient measurement in patients with acute or subacute portal hypertension. Gastrointest. Endosc. 2020, 93, 565–572. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver. EASL Clinical Practice Guideline: Occupational liver diseases. J. Hepatol. 2019, 71, 1022–1037. [Google Scholar] [CrossRef] [Green Version]
- Xiao, J.; Tu, J.; Zhang, H.; Zhang, F.; Zhang, W.; Xu, H.; Yin, Q.; Yang, J.; Han, H.; Wang, Y.; et al. Risk factors of poor prognosis in patients with pyrrolidine alkaloid-induced hepatic sinusoidal obstruction syndrome after transjugular intrahepatic portosystemic shunt. Hepatol. Int. 2021, 15, 720–729. [Google Scholar] [CrossRef]
- Deplano, A.; Migaleddu, V.; Pischedda, A.; Garrucciu, G.; Gregu, G.; Multinu, C.; Piredda, M.; Tocco, A.; Urigo, F.; Cossu, P.A.; et al. Portohepatic gradient and portal hemodynamics in patients with cirrhosis due to hepatitis C virus infection. Dig. Dis. Sci. 1999, 44, 155–162. [Google Scholar] [CrossRef]
- Reverter, E.; Blasi, A.; Gonzalez-Abraldes, J.; Martínez-Palli, G.; Seijo, S.; Turon, F.; Berzigotti, A.; Balust, J.; Bosch, J.; Garcia-Pagan, J.C. Impact of deep sedation on the accuracy of hepatic and portal venous pressure measurements in patients with cirrhosis. Liver Int. 2013, 34, 16–25. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Patient Characteristics | PA-HSOS (n = 30) | Decompensated Cirrhosis (n = 34) | p-Value |
|---|---|---|---|
| Age (years) | 65 (59–68) | 58 (51–66) | 0.005 |
| Male | 21 (70%) | 25 (73%) | 0.294 |
| Arterial hypertension | 13 (43%) | 8 (24%) | 0.092 |
| Type 2 diabetes | 7 (23%) | 7 (21%) | 0.791 |
| Severity of liver disease | |||
| Ascites, no/light/medium/heavy | 0/2/24/4 | 6/11/13/4 | 0.002 |
| Portal velocity(cm/s) | 13.7 (11.1–20.1) | 31.0 (21.3–41.3) | <0.001 |
| TB(µmol/L) | 44.3 (30.7–77.3) | 18.3 (14.3–29.2) | <0.001 |
| Alb (g/L) | 32.4 (30.7–34.9) | 32.9 (31.1–36.4) | 0.633 |
| Scr (µmol/L) | 72.0 (60.8–103.3) | 69.0 (53.8–87.8) | 0.329 |
| INR | 1.3 (1.2–1.5) | 1.3 (1.2–1.4) | 0.477 |
| Hepatic hemodynamics | |||
| WHVP (mmHg) | 29.0 (27.7–30.8) | 29.3 (25.2–32.0) | 0.888 |
| PP (mmHg) | 28.0 (25.7–31.0) | 29.5 (26.0–34.0) | 0.195 |
| PP-WHVP (mmHg) | −0.8 (−3.7–+1.8) | 1.3 (−1.2–+4.0) | 0.017 |
| FHVP(mmHg) | 7.0 (5.0–9.0) | 8.0 (6.0–11.5) | 0.120 |
| IVCP(mmHg) | 7.0 (5.0–10.0) | 8.0 (5.0–10.2) | 0.354 |
| HVPG(mmHg) | 21.8 (18.9–24.4) | 20.0 (17.8–22.5) | 0.042 |
| PPG(mmHg) | 22.0 (18.0–24.2) | 22.5 (20.0–24.4) | 0.370 |
| R | 95% CI | p | ICC | 95% CI | p | |
|---|---|---|---|---|---|---|
| PA-HSOS group (n = 30) | 0.58 | 0.25–0.77 | 0.001 | 0.68 | 0.32–0.85 | 0.002 |
| Cirrhosis group (n = 34) | 0.81 | 0.68–0.90 | <0.001 | 0.90 | 0.79–0.95 | <0.001 |
| Viral-related cirrhosis (n = 20) | 0.85 | 0.73–0.92 | <0.001 | 0.92 | 0.79–0.97 | <0.001 |
| Alcohol-related cirrhosis (n = 14) | 0.82 | 0.38–0.97 | <0.001 | 0.90 | 0.69–0.97 | <0.001 |
| Patient Characteristics | PA-HSOS Group (n = 30) n (%) | Cirrhosis Group (n = 34) n (%) | p-Value |
|---|---|---|---|
| Agreement between WHVP and PP | 17 (56.7%) | 25 (73.5%) | 0.156 |
| Disagreement between WHVP and PP | 13 (43.3%) | 9 (26.5%) | |
| Underestimation of PP | 3 (10.0%) | 8 (23.5%) | 0.271 |
| Overestimation of PP | 10 (33.3%) | 1 (2.9%) | 0.004 |
| Major discrepancies between WHVP and PP | 4 (13.3%) | 5 (14.7%) | 1.000 |
| R | 95% CI | p | ICC | 95% CI | p | |
|---|---|---|---|---|---|---|
| PA-HSOS group (n = 30) | 0.56 | 0.22–0.80 | 0.001 | 0.71 | 0.40–0.86 | 0.001 |
| Cirrhosis group (n = 34) | 0.89 | 0.68–0.98 | <0.001 | 0.94 | 0.87–0.97 | <0.001 |
| Viral-related cirrhosis (n = 20) | 0.90 | 0.82–0.97 | <0.001 | 0.92 | 0.69–0.97 | <0.001 |
| Alcohol-related cirrhosis (n = 14) | 0.84 | 0.12–1.00 | 0.01 | 0.91 | 0.67–0.97 | <0.001 |
| R | 95% CI | p | ICC | 95% CI | p | |
|---|---|---|---|---|---|---|
| PA-HSOS group (n = 30) | 0.51 | 0.17–0.78 | 0.004 | 0.65 | 0.27–0.84 | 0.003 |
| Cirrhosis group (n = 34) | 0.26 | −0.25–0.55 | 0.156 | 0.41 | −0.21–0.72 | 0.074 |
| Viral-related cirrhosis (n = 20) | 0.38 | 0.00–0.66 | 0.125 | 0.55 | −0.21–0.83 | 0.057 |
| Alcohol-related cirrhosis (n = 14) | 0.38 | −0.32–0.77 | 0.209 | 0.38 | −0.32–0.77 | 0.096 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cheng, Y.; Gu, L.; Yin, X.; Wang, X.; Xiao, J.; Wang, Y.; Zhang, W.; Wang, L.; Zou, X.; Zhang, M.; et al. Agreement between Wedged Hepatic Venous Pressure and Portal Pressure in Hepatic Sinusoidal Obstruction Syndrome. J. Pers. Med. 2023, 13, 4. https://doi.org/10.3390/jpm13010004
Cheng Y, Gu L, Yin X, Wang X, Xiao J, Wang Y, Zhang W, Wang L, Zou X, Zhang M, et al. Agreement between Wedged Hepatic Venous Pressure and Portal Pressure in Hepatic Sinusoidal Obstruction Syndrome. Journal of Personalized Medicine. 2023; 13(1):4. https://doi.org/10.3390/jpm13010004
Chicago/Turabian StyleCheng, Yang, Lihong Gu, Xiaochun Yin, Xixuan Wang, Jiangqiang Xiao, Yi Wang, Wei Zhang, Lei Wang, Xiaoping Zou, Ming Zhang, and et al. 2023. "Agreement between Wedged Hepatic Venous Pressure and Portal Pressure in Hepatic Sinusoidal Obstruction Syndrome" Journal of Personalized Medicine 13, no. 1: 4. https://doi.org/10.3390/jpm13010004