
The Prognostic Value of the GNRI in Patients with Stomach Cancer Undergoing Surgery
 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Literature Search Strategies
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction and Quality Assessment
2.4. Statistical Methods
3. Results
3.1. Characteristics of Studies
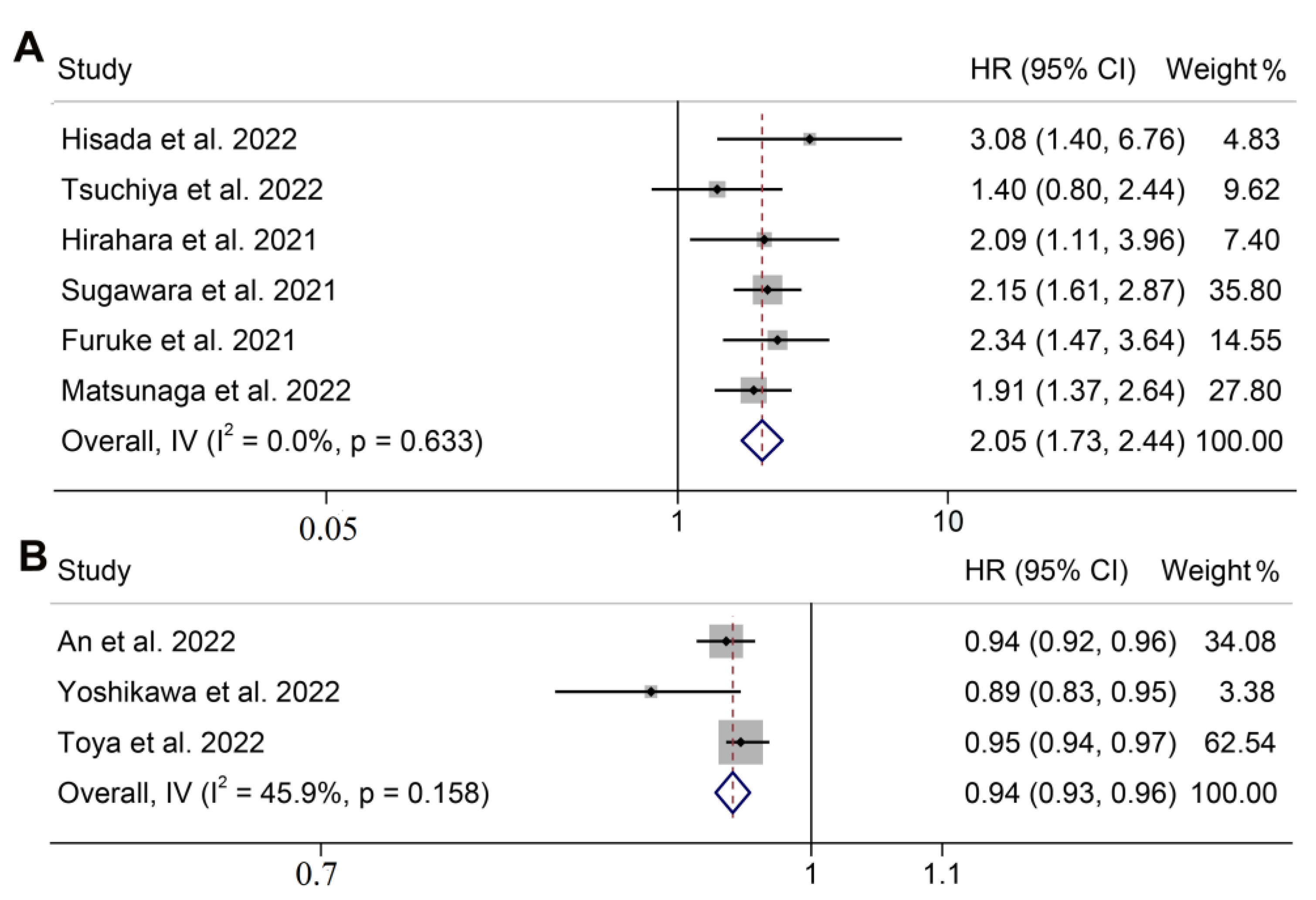
3.2. GNRI and Overall Survival
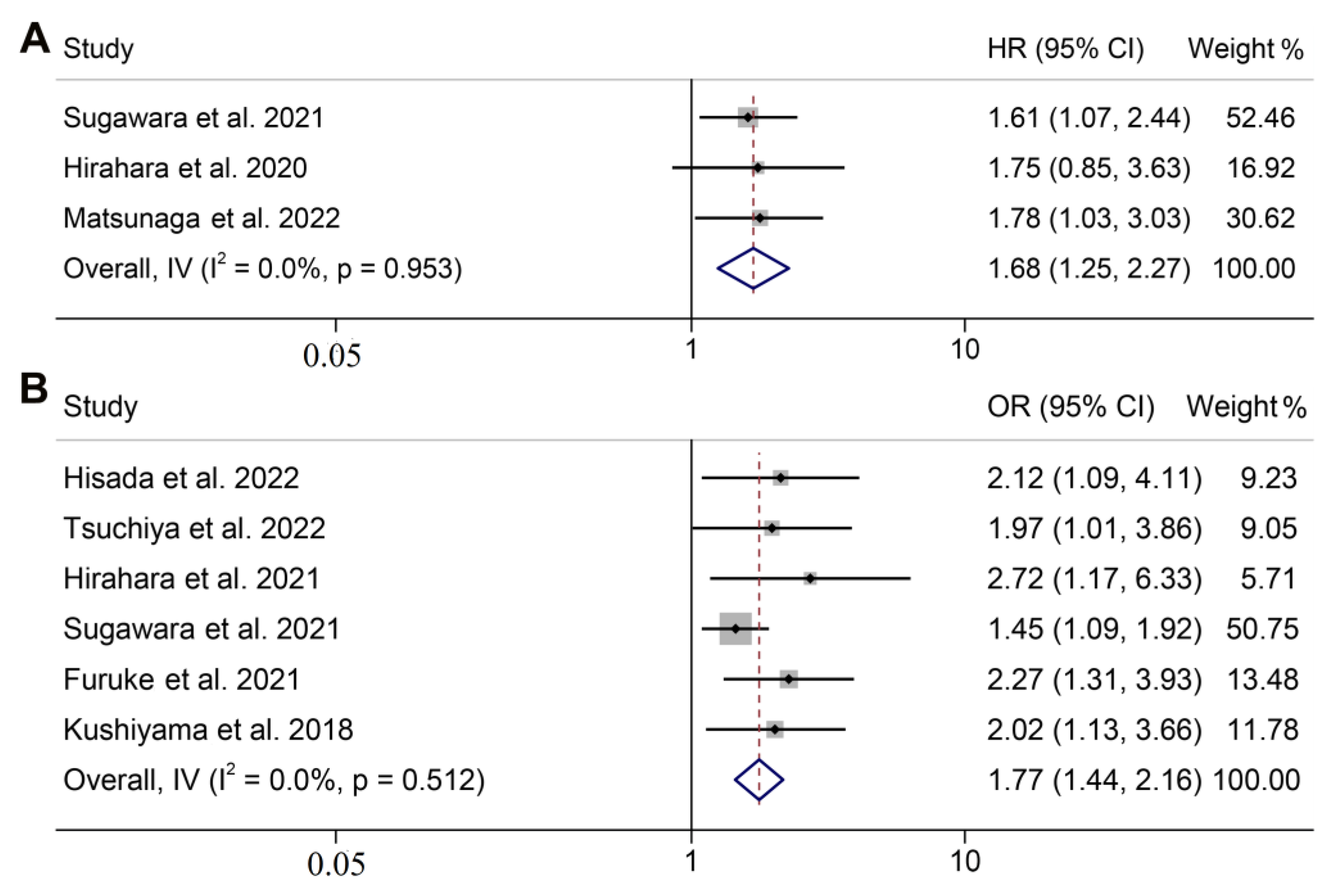
3.3. GNRI and Cancer-Specific Survival
3.4. GNRI and Postoperative Complications
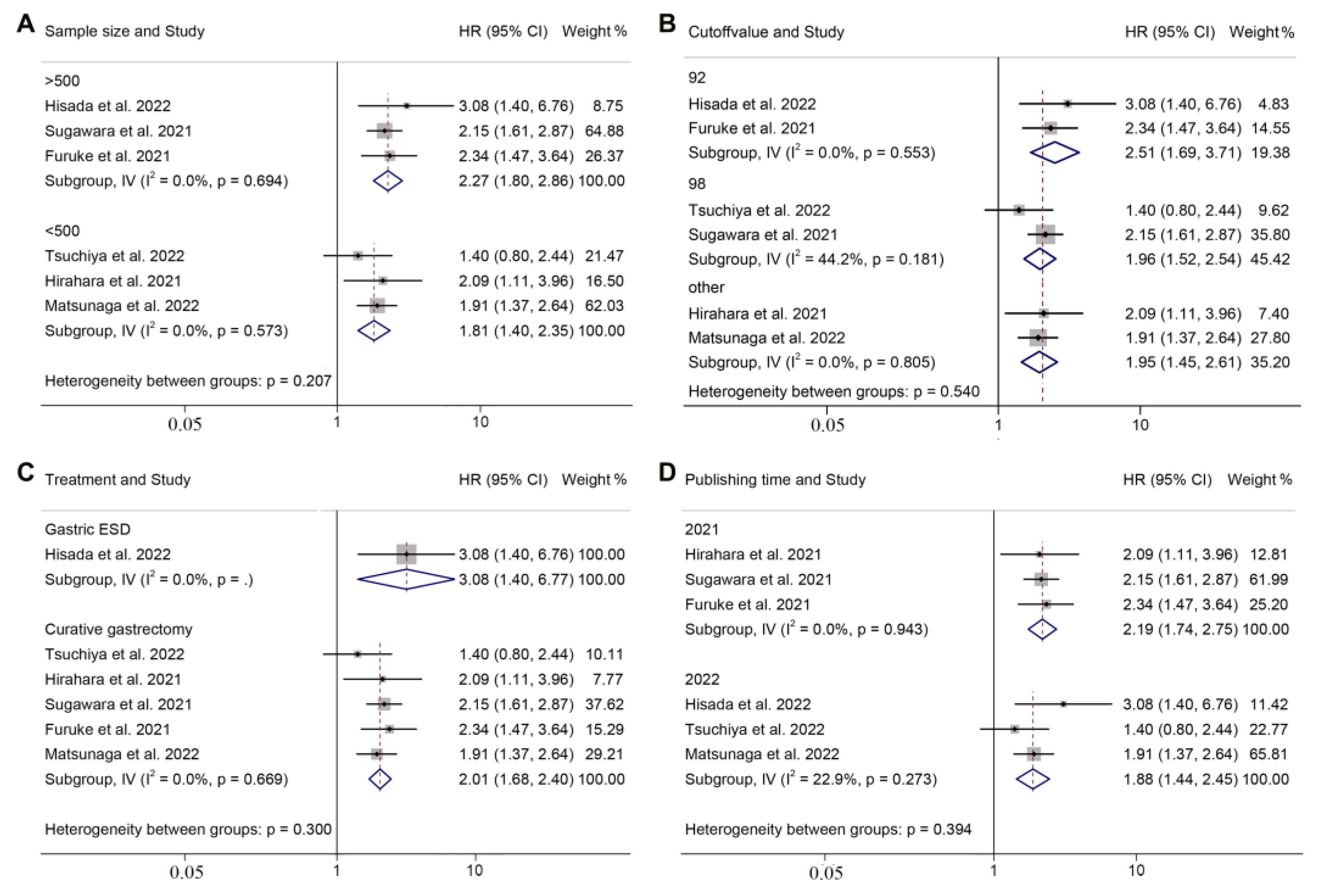
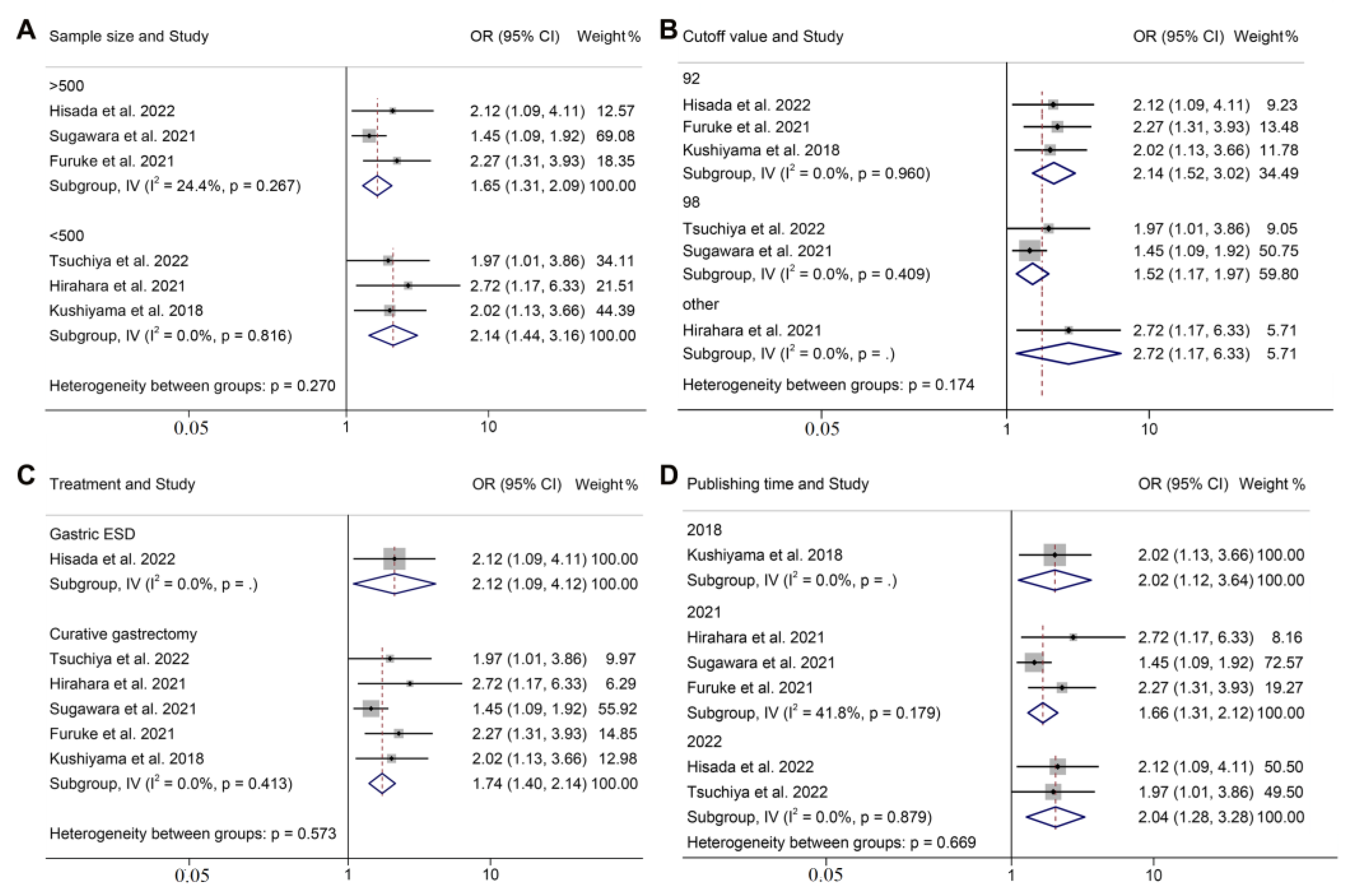
3.5. Subgroup Analysis of OS and Postoperative Complications
3.6. Publication Bias
3.7. Sensitivity Analysis
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Fukuda, Y.; Yamamoto, K.; Hirao, M.; Nishikawa, K.; Maeda, S.; Haraguchi, N.; Miyake, M.; Hama, N.; Miyamoto, A.; Ikeda, M.; et al. Prevalence of Malnutrition Among Gastric Cancer Patients Undergoing Gastrectomy and Optimal Preoperative Nutritional Support for Preventing Surgical Site Infections. Ann. Surg. Oncol. 2015, 22 (Suppl. 3), S778–S785. [Google Scholar] [CrossRef] [PubMed]
- Park, S.Y.; Yoon, J.K.; Lee, S.J.; Haam, S.; Jung, J. Postoperative change of the psoas muscle area as a predictor of survival in surgically treated esophageal cancer patients. J. Thorac. Dis. 2017, 9, 355–361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mariette, C.; De Botton, M.L.; Piessen, G. Surgery in esophageal and gastric cancer patients: What is the role for nutrition support in your daily practice? Ann. Surg. Oncol. 2012, 19, 2128–2134. [Google Scholar] [CrossRef]
- Saunders, J.; Smith, T. Malnutrition: Causes and consequences. Clin. Med. 2010, 10, 624–627. [Google Scholar] [CrossRef] [PubMed]
- Schiesser, M.; Kirchhoff, P.; Müller, M.K.; Schäfer, M.; Clavien, P.A. The correlation of nutrition risk index, nutrition risk score, and bioimpedance analysis with postoperative complications in patients undergoing gastrointestinal surgery. Surgery 2009, 145, 519–526. [Google Scholar] [CrossRef]
- Kuzu, M.A.; Terzioğlu, H.; Genç, V.; Erkek, A.B.; Ozban, M.; Sonyürek, P.; Elhan, A.H.; Torun, N. Preoperative nutritional risk assessment in predicting postoperative outcome in patients undergoing major surgery. World J. Surg. 2006, 30, 378–390. [Google Scholar] [CrossRef]
- Bouillanne, O.; Morineau, G.; Dupont, C.; Coulombel, I.; Vincent, J.P.; Nicolis, I.; Benazeth, S.; Cynober, L.; Aussel, C. Geriatric Nutritional Risk Index: A new index for evaluating at-risk elderly medical patients. Am. J. Clin. Nutr. 2005, 82, 777–783. [Google Scholar] [CrossRef] [Green Version]
- Zhou, J.; Fang, P.; Li, X.; Luan, S.; Xiao, X.; Gu, Y.; Shang, Q.; Zhang, H.; Yang, Y.; Zeng, X.; et al. Prognostic Value of Geriatric Nutritional Risk Index in Esophageal Carcinoma: A Systematic Review and Meta-Analysis. Front. Nutr. 2022, 9, 831283. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duval, S.; Tweedie, R. Trim and fill: A simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics 2000, 56, 455–463. [Google Scholar] [CrossRef] [PubMed]
- Yoshikawa, T.; Yamauchi, A.; Hamasaki, R.; Mori, Y.; Osawa, K.; Ito, R.; Kawai, Y.; Nakagami, S.; Azuma, S.; Morita, T.; et al. The Safety and Clinical Validity of Endoscopic Submucosal Dissection for Early Gastric Cancer in Patients Aged More Than 85 Years. Cancers 2022, 14, 3311. [Google Scholar] [CrossRef] [PubMed]
- Tsuchiya, N.; Kunisaki, C.; Kondo, H.; Sato, S.; Sato, K.; Watanabe, J.; Takeda, K.; Kosaka, T.; Akiyama, H.; Endo, I. Prognostic Factors Affecting Short- and Long-Term Outcomes of Gastrectomy for Gastric Cancer in Older Patients. Dig. Surg. 2022, 39, 109–116. [Google Scholar] [CrossRef] [PubMed]
- Toya, Y.; Shimada, T.; Hamada, K.; Watanabe, K.; Nakamura, J.; Fukushi, D.; Hatta, W.; Shinkai, H.; Ito, H.; Matsuhashi, T.; et al. Prediction model of 3-year survival after endoscopic submucosal dissection for early gastric cancer in elderly patients aged ≥85 years: EGC-2 model. J. Cancer Res. Clin. Oncol. 2022. [Google Scholar] [CrossRef] [PubMed]
- Matsunaga, T.; Saito, H.; Osaki, T.; Takahashi, S.; Iwamoto, A.; Fukuda, K.; Taniguchi, K.; Kuroda, H.; Takeuchi, T.; Sugamura, K.; et al. Impact of geriatric nutritional risk index on outcomes after gastrectomy in elderly patients with gastric cancer: A retrospective multicenter study in Japan. BMC Cancer 2022, 22, 540. [Google Scholar] [CrossRef] [PubMed]
- Hisada, H.; Tsuji, Y.; Obata, M.; Cho, R.; Nagao, S.; Miura, Y.; Mizutani, H.; Ohki, D.; Yakabi, S.; Takahashi, Y.; et al. The impact of sarcopenia on short- and long-term outcomes of endoscopic submucosal dissection for early gastric cancer. J. Gastroenterol. 2022, 57, 952–961. [Google Scholar] [CrossRef]
- An, S.; Eo, W.; Lee, S. Comparison of the Clinical Value of the Geriatric Nutritional Risk Index and Prognostic Nutritional Index as Determinants of Survival Outcome in Patients with Gastric Cancer. J. Cancer 2022, 13, 3348–3357. [Google Scholar] [CrossRef]
- Sugawara, K.; Yamashita, H.; Urabe, M.; Okumura, Y.; Yagi, K.; Aikou, S.; Seto, Y. Geriatric Nutrition Index Influences Survival Outcomes in Gastric Carcinoma Patients Undergoing Radical Surgery. JPEN J. Parenter Enter. Nutr. 2021, 45, 1042–1051. [Google Scholar] [CrossRef]
- Hirahara, N.; Tajima, Y.; Fujii, Y.; Kaji, S.; Kawabata, Y.; Hyakudomi, R.; Yamamoto, T.; Taniura, T. Prediction of postoperative complications and survival after laparoscopic gastrectomy using preoperative Geriatric Nutritional Risk Index in elderly gastric cancer patients. Surg. Endosc. 2021, 35, 1202–1209. [Google Scholar] [CrossRef]
- Furuke, H.; Matsubara, D.; Kubota, T.; Kiuchi, J.; Kubo, H.; Ohashi, T.; Shimizu, H.; Arita, T.; Yamamoto, Y.; Konishi, H.; et al. Geriatric Nutritional Risk Index Predicts Poor Prognosis of Patients After Curative Surgery for Gastric Cancer. Cancer Diagn. Progn. 2021, 1, 43–52. [Google Scholar] [CrossRef] [PubMed]
- Hirahara, N.; Matsubara, T.; Fujii, Y.; Kaji, S.; Hyakudomi, R.; Yamamoto, T.; Uchida, Y.; Miyazaki, Y.; Ishitobi, K.; Kawabata, Y.; et al. Preoperative geriatric nutritional risk index is a useful prognostic indicator in elderly patients with gastric cancer. Oncotarget 2020, 11, 2345–2356. [Google Scholar] [CrossRef]
- Kushiyama, S.; Sakurai, K.; Kubo, N.; Tamamori, Y.; Nishii, T.; Tachimori, A.; Inoue, T.; Maeda, K. The Preoperative Geriatric Nutritional Risk Index Predicts Postoperative Complications in Elderly Patients with Gastric Cancer Undergoing Gastrectomy. In Vivo 2018, 32, 1667–1672. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toya, Y.; Endo, M.; Akasaka, R.; Morishita, T.; Yanai, S.; Nakamura, S.; Eizuka, M.; Sugimoto, R.; Uesugi, N.; Sugai, T.; et al. Prognostic nutritional index is an independent prognostic factor for older patients aged ≥ 85 years treated by gastric endoscopic submucosal dissection. BMC Gastroenterol. 2021, 21, 328. [Google Scholar] [CrossRef] [PubMed]
- Shimada, T.; Yamagata, T.; Kanno, Y.; Ohira, T.; Harada, Y.; Koike, Y.; Tanaka, M.; Komabayashi, D.; Shimizu, T.; Okano, H.; et al. Predictive Factors for Short-Term Survival after Non-Curative Endoscopic Submucosal Dissection for Early Gastric Cancer. Digestion 2021, 102, 630–639. [Google Scholar] [CrossRef] [PubMed]
- Toya, Y.; Endo, M.; Nakamura, S.; Akasaka, R.; Yanai, S.; Kawasaki, K.; Koeda, K.; Eizuka, M.; Fujita, Y.; Uesugi, N.; et al. Long-term outcomes and prognostic factors with non-curative endoscopic submucosal dissection for gastric cancer in elderly patients aged ≥ 75 years. Gastric. Cancer 2019, 22, 838–844. [Google Scholar] [CrossRef] [Green Version]
- Ruan, G.T.; Zhang, Q.; Zhang, X.; Tang, M.; Song, M.M.; Zhang, X.W.; Li, X.R.; Zhang, K.P.; Ge, Y.Z.; Yang, M.; et al. Geriatric Nutrition Risk Index: Prognostic factor related to inflammation in elderly patients with cancer cachexia. J. Cachexia Sarcopenia Muscle 2021, 12, 1969–1982. [Google Scholar] [CrossRef]
- Hisada, H.; Tamura, N.; Tsuji, Y.; Nagao, S.; Fukagawa, K.; Miura, Y.; Mizutani, H.; Ohki, D.; Yakabi, S.; Minatsuki, C.; et al. The impact of sarcopenia on adverse events associated with gastric endoscopic submucosal dissection. Surg. Endosc. 2022, 36, 6387–6395. [Google Scholar] [CrossRef]
- Clavien, P.A.; Barkun, J.; de Oliveira, M.L.; Vauthey, J.N.; Dindo, D.; Schulick, R.D.; de Santibañes, E.; Pekolj, J.; Slankamenac, K.; Bassi, C.; et al. The Clavien-Dindo classification of surgical complications: Five-year experience. Ann. Surg. 2009, 250, 187–196. [Google Scholar] [CrossRef] [Green Version]
- Goins, E.C.; Weber, J.M.; Truong, T.; Moss, H.A.; Previs, R.A.; Davidson, B.A.; Havrilesky, L.J. Malnutrition as a risk factor for post-operative morbidity in gynecologic cancer: Analysis using a national surgical outcomes database. Gynecol. Oncol. 2022, 165, 309–316. [Google Scholar] [CrossRef]
- Li, Q.D.; Li, H.; Li, F.J.; Wang, M.S.; Li, Z.J.; Han, J.; Li, Q.H.; Ma, X.J.; Wang da, N. Nutrition deficiency increases the risk of stomach cancer mortality. BMC Cancer 2012, 12, 315. [Google Scholar]
- McMillan, D.C. The systemic inflammation-based Glasgow Prognostic Score: A decade of experience in patients with cancer. Cancer Treat. Rev. 2013, 39, 534–540. [Google Scholar] [CrossRef]
- Kono, T.; Sakamoto, K.; Shinden, S.; Ogawa, K. Pre-therapeutic nutritional assessment for predicting severe adverse events in patients with head and neck cancer treated by radiotherapy. Clin. Nutr. 2017, 36, 1681–1685. [Google Scholar] [CrossRef] [PubMed]
- Tashiro, M.; Yamada, S.; Sonohara, F.; Takami, H.; Suenaga, M.; Hayashi, M.; Niwa, Y.; Tanaka, C.; Kobayashi, D.; Nakayama, G.; et al. Clinical Impact of Neoadjuvant Therapy on Nutritional Status in Pancreatic Cancer. Ann. Surg. Oncol. 2018, 25, 3365–3371. [Google Scholar] [CrossRef] [PubMed]
- Onodera, T.; Goseki, N.; Kosaki, G. [Prognostic nutritional index in gastrointestinal surgery of malnourished cancer patients]. Nihon Geka Gakkai Zasshi 1984, 85, 1001–1005. [Google Scholar]
- Ignacio de Ulíbarri, J.; González-Madroño, A.; de Villar, N.G.; González, P.; González, B.; Mancha, A.; Rodríguez, F.; Fernández, G. CONUT: A tool for controlling nutritional status. First validation in a hospital population. Nutr. Hosp. 2005, 20, 38–45. [Google Scholar] [PubMed]
- Wang, H.; Li, C.; Yang, R.; Jin, J.; Liu, D.; Li, W. Prognostic Value of the Geriatric Nutritional Risk Index in Non-Small Cell Lung Cancer Patients: A Systematic Review and Meta-Analysis. Front. Oncol. 2021, 11, 794862. [Google Scholar] [CrossRef]
- Nishi, I.; Seo, Y.; Hamada-Harimura, Y.; Yamamoto, M.; Ishizu, T.; Sugano, A.; Sato, K.; Sai, S.; Obara, K.; Suzuki, S.; et al. Geriatric nutritional risk index predicts all-cause deaths in heart failure with preserved ejection fraction. ESC Heart Fail. 2019, 6, 396–405. [Google Scholar] [CrossRef] [Green Version]
- Yasumura, K.; Abe, H.; Iida, Y.; Kato, T.; Nakamura, M.; Toriyama, C.; Nishida, H.; Idemoto, A.; Shinouchi, K.; Mishima, T.; et al. Prognostic impact of nutritional status and physical capacity in elderly patients with acute decompensated heart failure. ESC Heart Fail. 2020, 7, 1801–1808. [Google Scholar] [CrossRef]
- Yamada, S.; Yamamoto, S.; Fukuma, S.; Nakano, T.; Tsuruya, K.; Inaba, M. Geriatric Nutritional Risk Index (GNRI) and Creatinine Index Equally Predict the Risk of Mortality in Hemodialysis Patients: J-DOPPS. Sci. Rep. 2020, 10, 5756. [Google Scholar] [CrossRef] [Green Version]
- Hayama, T.; Hashiguchi, Y.; Ozawa, T.; Watanabe, M.; Fukushima, Y.; Shimada, R.; Nozawa, K.; Matsuda, K.; Fujii, S.; Fukagawa, T. The preoperative geriatric nutritional risk index (GNRI) is an independent prognostic factor in elderly patients underwent curative resection for colorectal cancer. Sci. Rep. 2022, 12, 3682. [Google Scholar] [CrossRef] [PubMed]
- Funamizu, N.; Sakamoto, A.; Utsunomiya, T.; Uraoka, M.; Nagaoka, T.; Iwata, M.; Ito, C.; Tamura, K.; Sakamoto, K.; Ogawa, K.; et al. Geriatric nutritional risk index as a potential prognostic marker for patients with resectable pancreatic cancer: A single-center, retrospective cohort study. Sci. Rep. 2022, 12, 13644. [Google Scholar] [CrossRef] [PubMed]
- Dai, H.; Xu, J. Preoperative geriatric nutritional risk index is an independent prognostic factor for postoperative survival after gallbladder cancer radical surgery. BMC Surg. 2022, 22, 133. [Google Scholar]
- Kanno, H.; Goto, Y.; Sasaki, S.; Fukutomi, S.; Hisaka, T.; Fujita, F.; Akagi, Y.; Okuda, K. Geriatric nutritional risk index predicts prognosis in hepatocellular carcinoma after hepatectomy: A propensity score matching analysis. Sci. Rep. 2021, 11, 9038. [Google Scholar] [CrossRef]
- Yamana, I.; Takeno, S.; Shibata, R.; Shiwaku, H.; Maki, K.; Hashimoto, T.; Shiraishi, T.; Iwasaki, A.; Yamashita, Y. Is the Geriatric Nutritional Risk Index a Significant Predictor of Postoperative Complications in Patients with Esophageal Cancer Undergoing Esophagectomy? Eur. Surg. Res. 2015, 55, 35–42. [Google Scholar] [CrossRef]
- Chen, X.Y.; Lin, Y.; Yin, S.Y.; Shen, Y.T.; Zhang, X.C.; Chen, K.K.; Zhou, C.J.; Zheng, C.G. The geriatric nutritional risk index is an effective tool to detect GLIM-defined malnutrition in rectal cancer patients. Front. Nutr. 2022, 9, 1061944. [Google Scholar] [CrossRef]
- Minnella, E.M.; Awasthi, R.; Loiselle, S.E.; Agnihotram, R.V.; Ferri, L.; Carli, F. Effect of Exercise and Nutrition Prehabilitation on Functional Capacity in Esophagogastric Cancer Surgery: A Randomized Clinical Trial. JAMA Surg. 2018, 153, 1081–1089. [Google Scholar] [CrossRef] [Green Version]
- Miranti, E.H.; Stolzenberg-Solomon, R.; Weinstein, S.J.; Selhub, J.; Männistö, S.; Taylor, P.; Freedman, N.; Albanes, D.; Abnet, C.; Murphy, G. Low vitamin B(12) increases risk of gastric cancer: A prospective study of one-carbon metabolism nutrients and risk of upper gastrointestinal tract cancer. Int. J. Cancer 2017, 141, 1120–1129. [Google Scholar] [CrossRef] [Green Version]
- Meng, Q.; Tan, S.; Jiang, Y.; Han, J.; Xi, Q.; Zhuang, Q.; Wu, G. Post-discharge oral nutritional supplements with dietary advice in patients at nutritional risk after surgery for gastric cancer: A randomized clinical trial. Clin. Nutr. 2021, 40, 40–46. [Google Scholar] [CrossRef]
- Solheim, T.S.; Laird, B.; Balstad, T.R.; Stene, G.B.; Bye, A.; Johns, N.; Pettersen, C.H.; Fallon, M.; Fayers, P.; Fearon, K.; et al. A randomized phase II feasibility trial of a multimodal intervention for the management of cachexia in lung and pancreatic cancer. J. Cachexia Sarcopenia Muscle 2017, 8, 778–788. [Google Scholar] [CrossRef]
- Fearon, K.; Strasser, F.; Anker, S.D.; Bosaeus, I.; Bruera, E.; Fainsinger, R.L.; Jatoi, A.; Loprinzi, C.; MacDonald, N.; Mantovani, G.; et al. Definition and classification of cancer cachexia: An international consensus. Lancet Oncol. 2011, 12, 489–495. [Google Scholar] [CrossRef] [PubMed]
- Fearon, K.C.; Glass, D.J.; Guttridge, D.C. Cancer cachexia: Mediators, signaling, and metabolic pathways. Cell Metab. 2012, 16, 153–166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jendretzki, J.; Henniger, D.; Schiffmann, L.; Wolz, C.; Kollikowski, A.; Meining, A.; Einsele, H.; Winkler, M.; Löffler, C. Every fifth patient suffered a high nutritional risk-Results of a prospective patient survey in an oncological outpatient center. Front. Nutr. 2022, 9, 1033265. [Google Scholar] [CrossRef]
- Teunissen, S.C.C.M.; Wesker, W.; Kruitwagen, C.; de Haes, H.C.J.M.; Voest, E.E.; de Graeff, A. Symptom prevalence in patients with incurable cancer: A systematic review. J. Pain Symptom Manag. 2007, 34, 94–104. [Google Scholar] [CrossRef]
- Bozzetti, F. Nutritional intervention is indicated in malnourished cancer patients. Clin. Nutr. 2019, 38, 477. [Google Scholar] [CrossRef]
- Uster, A.; Ruehlin, M.; Mey, S.; Gisi, D.; Knols, R.; Imoberdorf, R.; Pless, M.; Ballmer, P.E. Effects of nutrition and physical exercise intervention in palliative cancer patients: A randomized controlled trial. Clin. Nutr. 2018, 37, 1202–1209. [Google Scholar] [CrossRef]
- Guo, Y.; Li, Z.X.; Zhang, J.Y.; Ma, J.-L.; Zhang, L.; Zhang, Y.; Zhou, T.; Liu, W.-D.; Han, Z.-X.; Li, W.-Q.; et al. Association Between Lifestyle Factors, Vitamin and Garlic Supplementation, and Gastric Cancer Outcomes: A Secondary Analysis of a Randomized Clinical Trial. JAMA Netw. Open 2020, 3, e206628. [Google Scholar] [CrossRef]
- Adiamah, A.; Rollins, K.E.; Kapeleris, A.; Welch, N.T.; Iftikhar, S.Y.; Allison, S.P.; Lobo, D.N. Postoperative arginine-enriched immune modulating nutrition: Long-term survival results from a randomised clinical trial in patients with oesophagogastric and pancreaticobiliary cancer. Clin. Nutr. 2021, 40, 5482–5485. [Google Scholar] [CrossRef]
- Xu, L.; Zhang, X.; Lu, J.; Dai, J.-X.; Lin, R.-Q.; Tian, F.-X.; Liang, B.; Guo, Y.-N.; Luo, H.-Y.; Li, N.; et al. The Effects of Dinner-to-Bed Time and Post-Dinner Walk on Gastric Cancer Across Different Age Groups: A Multicenter Case-Control Study in Southeast China. Medicine 2016, 95, e3397. [Google Scholar] [CrossRef]
- Song, Q.; Wang, J.; Jia, Y.; Wang, C.; Wang, N.; Tan, B.; Ma, W.; Guan, S.; Jiang, D.; Cheng, Y. Shorter dinner-to-bed time is associated with gastric cardia adenocarcinoma risk partly in a reflux-dependent manner. Ann. Surg. Oncol. 2014, 21, 2615–2619. [Google Scholar] [CrossRef] [PubMed]
- Li, W.Q.; Zhang, J.Y.; Ma, J.L.; Li, Z.-X.; Zhang, L.; Zhang, Y.; Guo, Y.; Zhou, T.; Li, J.-Y.; Shen, L.; et al. Effects of Helicobacter pylori treatment and vitamin and garlic supplementation on gastric cancer incidence and mortality: Follow-up of a randomized intervention trial. BMJ 2019, 366, l5016. [Google Scholar] [CrossRef] [Green Version]
- Ma, J.L.; Zhang, L.; Brown, L.M.; Li, J.-Y.; Shen, L.; Pan, K.-F.; Liu, W.-D.; Hu, Y.; Han, Z.-X.; Crystal-Mansour, S.; et al. Fifteen-year effects of Helicobacter pylori, garlic, and vitamin treatments on gastric cancer incidence and mortality. J. Natl. Cancer Inst. 2012, 104, 488–492. [Google Scholar] [CrossRef] [PubMed]
- Amini, L.; Chekini, R.; Nateghi, M.R.; Haghani, H.; Jamialahmadi, T.; Sathyapalan, T.; Sahebkar, A. The Effect of Combined Vitamin C and Vitamin E Supplementation on Oxidative Stress Markers in Women with Endometriosis: A Randomized, Triple-Blind Placebo-Controlled Clinical Trial. Pain Res. Manag. 2021, 2021, 5529741. [Google Scholar] [CrossRef] [PubMed]
- Rozemeijer, S.; de Grooth, H.J.; Elbers, P.; Girbes, A.R.J.; den Uil, C.A.; Dubois, E.A.; Wils, E.-J.; Rettig, T.C.D.; van Zanten, A.R.H.; Vink, R.; et al. Early high-dose vitamin C in post-cardiac arrest syndrome (VITaCCA): Study protocol for a randomized, double-blind, multi-center, placebo-controlled trial. Trials 2021, 22, 546. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Study Region | Study Design | Study Period | Sample Size | Male/ Female | Age (Years) | Treatment | Cut-Off | Outcome | NOS Score |
|---|---|---|---|---|---|---|---|---|---|---|
| Toya et al. 2022 [15] | Tohoku, Japan | R | January 2002–December 2017 | 740 | 469/271 | 86 (85–93.0) a | Gastric ESD | Continuous | OS (U) | 6 |
| Matsunaga et al. 2022 [16] | Multi-center, Japan | R | January 2005–December 2015 | 497 | 330/167 | 80.6 ± 4.0 | Curative gastrectomy | 97/95.8 | OS (M), CSS (M) | 8 |
| An et al. 2022 [18] | Gangdong, Korea | R | June 2006–December 2017 | 450 | 301/149 | 60 (52–69) a | Curative gastrectomy | Continuous | OS (M) | 7 |
| Hisada et al. 2022 [17] | Tokyo, Japan | R | January 2009–December 2019 | 767 | 559/208 | 75 (65–95) b | Gastric ESD | 92 | OS (M), complications (M) | 8 |
| Yoshikawa et al. 2022 [13] | Osaka, Japan | R | January 2006–December 2020 | 44 | 30/14 | 86 (85–96) b | Gastric ESD | Continuous | OS (U) | 6 |
| Tsuchiya et al. 2022 [14] | Yokohama, Japan | R | April 2002–December 2018 | 186 | 128/58 | 82 (80–93) b | Curative gastrectomy | 98 | OS (U), complications (M) | 7 |
| Hirahara et al. 2021 [20] | Shimane, Japan | R | January 2010–December 2017 | 303 | 209/94 | 65–91 c | Curative gastrectomy | 85.7 | OS (M), complications (M) | 7 |
| Sugawara et al. 2021 [19] | Tokyo, Japan | R | April 2001–December 2014 | 1166 | 816/350 | 25–91 c | Curative gastrectomy | 98 | OS (M), CSS (M), complications (U) | 8 |
| Furuke et al. 2021 [21] | Kyoto, Japan | R | 2008–2016 | 795 | 534/261 | 68 (29–89) b | Curative gastrectomy | 92 | OS (M), complications (U) | 8 |
| Hirahara et al. 2020 [22] | Shimane, Japan | R | January 2010–December 2017 | 297 | 205/92 | 65–91 c | Curative gastrectomy | 90.9 | CSS (M) | 7 |
| Kushiyama et al. 2018 [23] | Osaka, Japan | R | January 2006–December 2015 | 348 | 230/118 | 79.6 ± 3.8 | Curative gastrectomy | 92 | Complications (M) | 7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, Q.; Zhang, L.; Jin, Q.; He, Y.; Wu, M.; Peng, H.; Li, Y. The Prognostic Value of the GNRI in Patients with Stomach Cancer Undergoing Surgery. J. Pers. Med. 2023, 13, 155. https://doi.org/10.3390/jpm13010155
Zhang Q, Zhang L, Jin Q, He Y, Wu M, Peng H, Li Y. The Prognostic Value of the GNRI in Patients with Stomach Cancer Undergoing Surgery. Journal of Personalized Medicine. 2023; 13(1):155. https://doi.org/10.3390/jpm13010155
Chicago/Turabian StyleZhang, Qianqian, Lilong Zhang, Qi Jin, Yongheng He, Mingsheng Wu, Hongxing Peng, and Yijin Li. 2023. "The Prognostic Value of the GNRI in Patients with Stomach Cancer Undergoing Surgery" Journal of Personalized Medicine 13, no. 1: 155. https://doi.org/10.3390/jpm13010155