
A Deep Learning Method for Quantification of Femoral Head Necrosis Based on Routine Hip MRI for Improved Surgical Decision Making
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
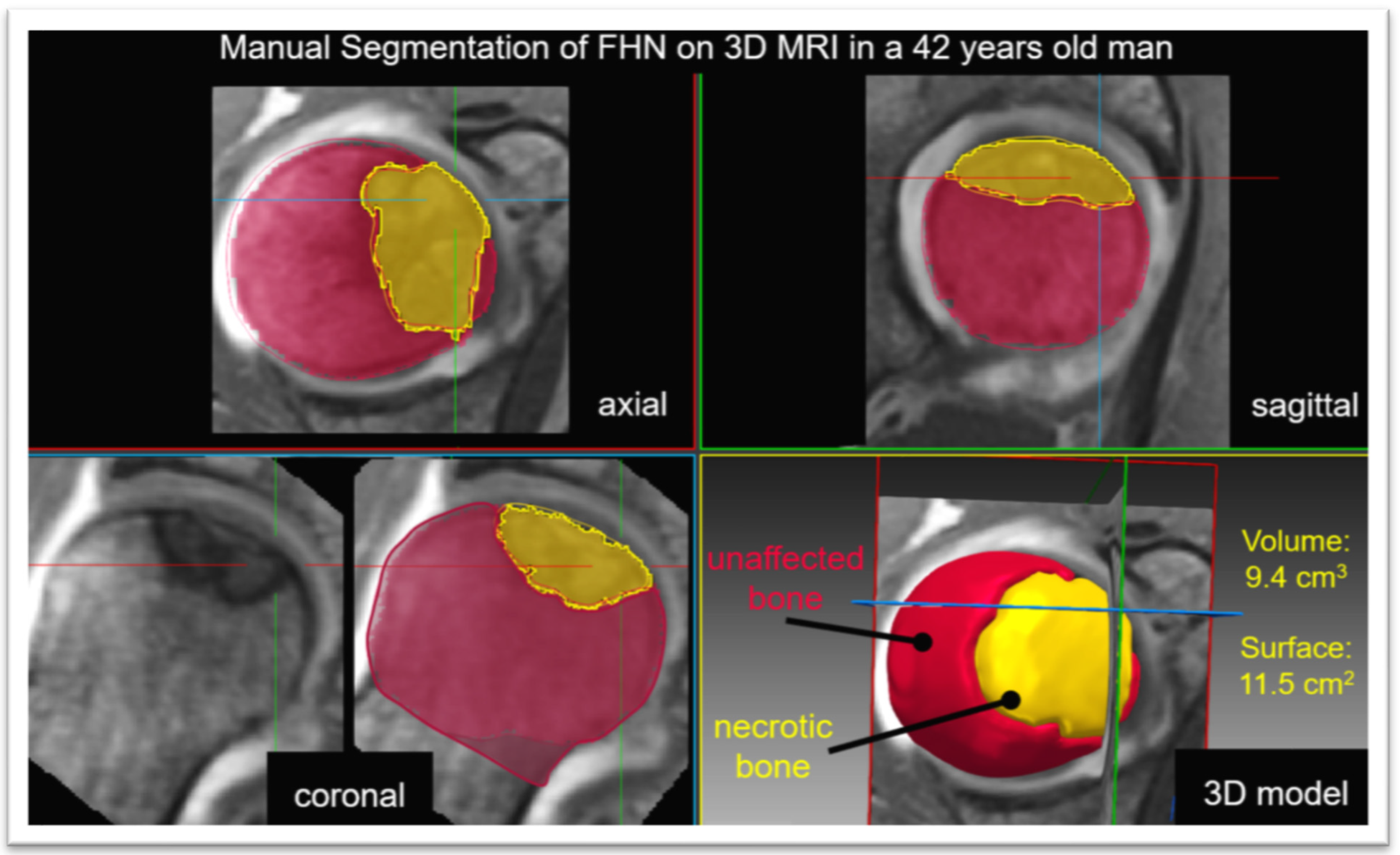
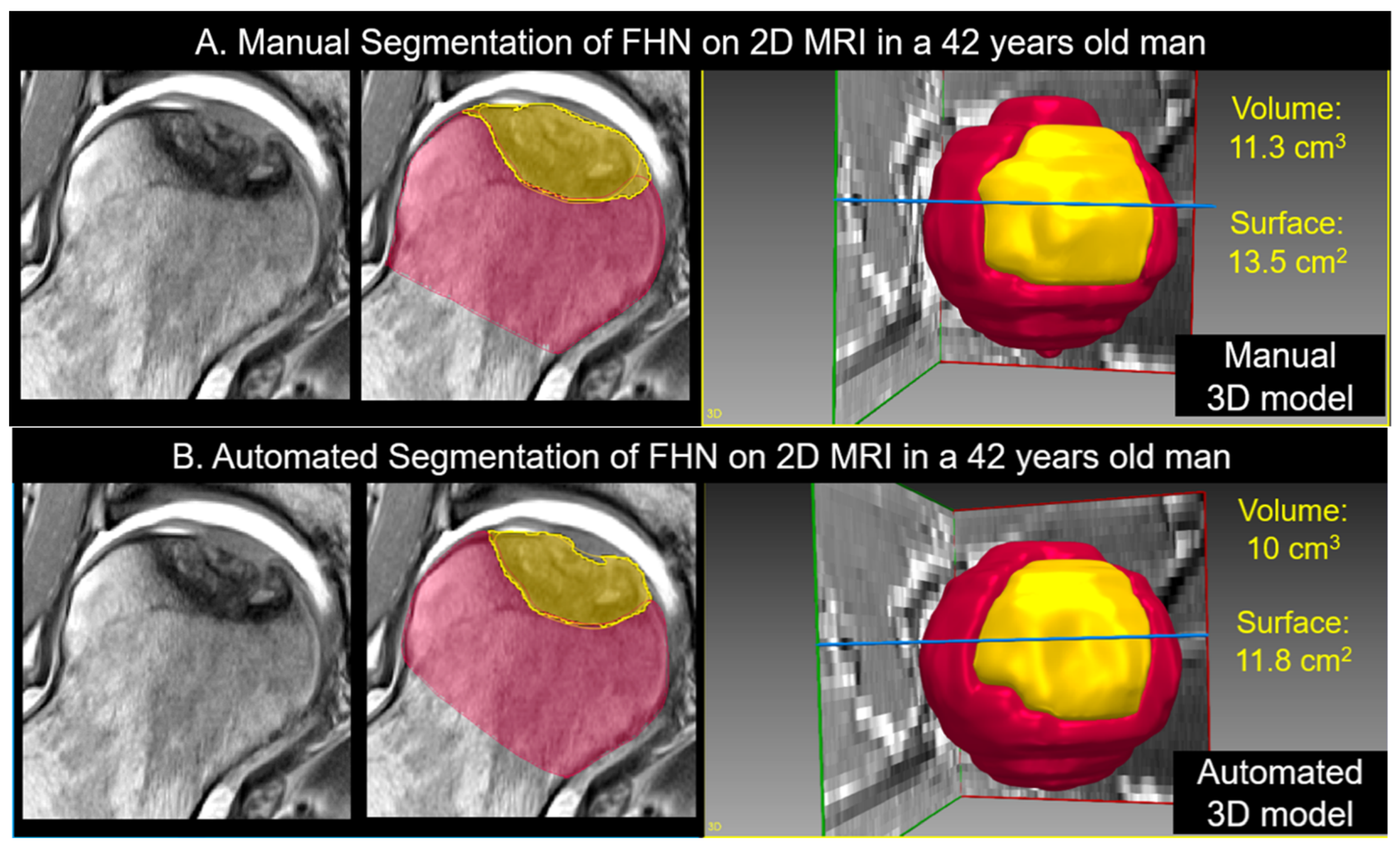
2.1. Manual and Automatic Segmentation of FHN
2.2. Statistical Analysis
3. Results
3.1. Manual Segmentation of 3D MRI versus Manual Segmentation of 2D MRI
3.2. Manual Segmentation of 2D MRI Versus Automatic Segmentation of 2D MRI
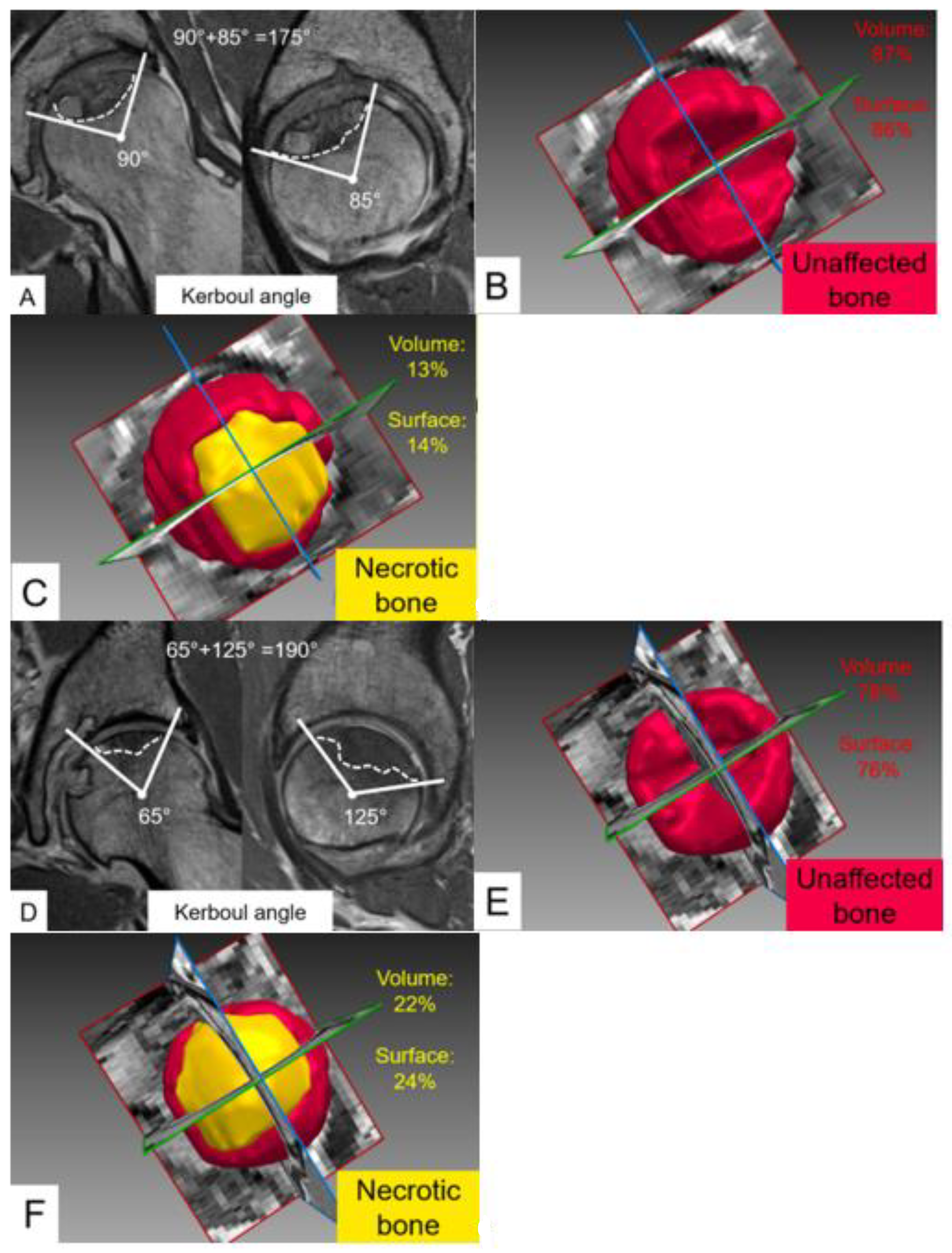
3.3. Quantitative Comparison of Early and Advanced Stages of Femoral Head Necrosis
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bassounas, A.E.; Karantanas, A.H.; Fotiadis, D.I.; Malizos, K.N. Femoral head osteonecrosis: Volumetric MRI assessment and outcome. Eur. J. Radiol. 2007, 63, 10–15. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, S.; Kapadia, B.H.; Jauregui, J.J.; Cherian, J.J.; Mont, M.A. Natural History of Osteonecrosis. In Osteonecrosis; Koo, K.H., Mont, M., Jones, L., Eds.; Springer: Berlin/Heidelberg, Germany, 2014; pp. 161–164. [Google Scholar] [CrossRef]
- Mont, M.A.; Salem, H.S.; Piuzzi, N.S.; Goodman, S.B.; Jones, L.C. Nontraumatic Osteonecrosis of the Femoral Head: Where Do We Stand Today? A 5-Year Update. J. Bone Jt. Surg. 2020, 102, 1084–1099. [Google Scholar] [CrossRef]
- Lubega, N.; Mkandawire, N.C.; Sibande, G.C.; Norrish, A.R.; Harrison, W.J. Joint replacement in Malawi. J. Bone Jt. Surg. 2009, 91, 341–343. [Google Scholar] [CrossRef] [Green Version]
- Steppacher, S.D.; Sedlmayer, R.; Tannast, M.; Schmaranzer, F.; A Siebenrock, K. Surgical hip dislocation with femoral osteotomy and bone grafting prevents head collapse in hips with advanced necrosis. HIP Int. J. Clin. Exp. Res. Hip Pathol. Ther. 2019, 30, 398–406. [Google Scholar] [CrossRef]
- Chughtai, M.; Piuzzi, N.S.; Khlopas, A.; Jones, L.C.; Goodman, S.B.; Mont, M.A. An evidence-based guide to the treatment of osteonecrosis of the femoral head. Bone Jt. J. 2017, 99-B, 1267–1279. [Google Scholar] [CrossRef] [PubMed]
- McAuley, J.P.; Szuszczewicz, E.S.; Young, A.; A Engh, C. Total Hip Arthroplasty in Patients 50 Years and Younger. Clin. Orthop. Relat. Res. 2004, 418, 119–125. [Google Scholar] [CrossRef] [PubMed]
- Cao, L.; Guo, C.; Chen, J.; Chen, Z.; Yan, Z. Free Vascularized Fibular Grafting Improves Vascularity Compared with Core Decompression in Femoral Head Osteonecrosis: A Randomized Clinical Trial. Clin. Orthop. Relat. Res. 2017, 475, 2230–2240. [Google Scholar] [CrossRef] [Green Version]
- Camp, J.F.; Colwell, C.W. Core decompression of the femoral head for osteonecrosis. J. Bone Jt. Surg. 1986, 68, 1313–1319. [Google Scholar] [CrossRef]
- Sugioka, Y.; Yamamoto, T. Transtrochanteric Posterior Rotational Osteotomy for Osteonecrosis. Clin. Orthop. Relat. Res. 2008, 466, 1104–1109. [Google Scholar] [CrossRef]
- Ganz, R.; Gill, T.J.; Gautier, E.; Ganz, K.; Krügel, N.; Berlemann, U. Surgical dislocation of the adult hip. J. Bone Jt. Surg. 2001, 83, 1119–1124. [Google Scholar] [CrossRef]
- Yoon, B.-H.; Mont, M.A.; Koo, K.-H.; Chen, C.-H.; Cheng, E.Y.; Cui, Q.; Drescher, W.; Gangji, V.; Goodman, S.B.; Ha, Y.-C.; et al. The 2019 Revised Version of Association Research Circulation Osseous Staging System of Osteonecrosis of the Femoral Head. J. Arthroplast. 2019, 35, 933–940. [Google Scholar] [CrossRef] [PubMed]
- Karantanas, A.H.; E Drakonaki, E. The Role of MR Imaging in Avascular Necrosis of the Femoral Head. Semin. Musculoskelet. Radiol. 2011, 15, 281–300. [Google Scholar] [CrossRef] [PubMed]
- Cherian, S.F.; Laorr, A.; Saleh, K.J.; Kuskowski, M.A.; Bailey, R.F.; Cheng, E.Y. Quantifying the extent of femoral head involvement in osteonecrosis. J. Bone Jt. Surg. 2003, 85, 309–315. [Google Scholar] [CrossRef] [PubMed]
- Schmaranzer, F.; Todorski, I.A.S.; Lerch, T.D.; Schwab, J.; Cullmann-Bastian, J.; Tannast, M. Intra-articular Lesions: Imaging and Surgical Correlation. Semin. Musculoskelet. Radiol. 2017, 21, 487–506. [Google Scholar] [CrossRef]
- Meier, M.K.; Lerch, T.D.; Steppacher, S.D.; Siebenrock, K.A.; Tannast, M.; Vavron, P.; Schmaranzer, E.; Schmaranzer, F. High prevalence of hip lesions secondary to arthroscopic over- or undercorrection of femoroacetabular impingement in patients with postoperative pain. Eur. Radiol. 2021, 32, 3097–3111. [Google Scholar] [CrossRef]
- Schmaranzer, F.; Lerch, T.D.; Steppacher, S.D.; A Siebenrock, K.; Tannast, M. Femoral cartilage damage occurs at the zone of femoral head necrosis and can be accurately detected on traction MR arthrography of the hip in patients undergoing joint preserving hip surgery. J. Hip Preserv. Surg. 2021, 8, 28–39. [Google Scholar] [CrossRef]
- Schmaranzer, F.; Helfenstein, R.; Zeng, G.; Lerch, T.; Novais, E.N.; Wylie, J.D.; Kim, Y.-J.; Siebenrock, K.A.; Tannast, M.; Zheng, G. Automatic MRI-Based Three-Dimensional Models of Hip Cartilage Provide Improved Morphologic and Biochemical Analysis. Clin. Orthop. Relat. Res. 2019, 477, 1036–1052. [Google Scholar] [CrossRef]
- Ha, Y.-C.; Jung, W.H.; Kim, J.-R.; Seong, N.H.; Kim, S.-Y.; Koo, K.-H. Prediction of Collapse in Femoral Head Osteonecrosis: A Modified Kerboul Method with Use of Magnetic Resonance Images. J. Bone Jt. Surg. 2006, 88, 35–40. [Google Scholar] [CrossRef]
- Tönnis, D.; Heinecke, A. Current Concepts Review—Acetabular and Femoral Anteversion. J. Bone Jt. Surg. 1999, 81, 1747–1770. [Google Scholar] [CrossRef]
- Kovalenko, B.; Bremjit, P.; Fernando, N. Classifications in Brief: Tönnis Classification of Hip Osteoarthritis. Clin. Orthop. Relat. Res. 2018, 476, 1680–1684. [Google Scholar] [CrossRef]
- Isensee, F.; Jaeger, P.F.; Kohl, S.A.A.; Petersen, J.; Maier-Hein, K.H. nnU-Net: A self-configuring method for deep learning-based biomedical image segmentation. Nat. Methods 2020, 18, 203–211. [Google Scholar] [CrossRef] [PubMed]
- Tan, Y.; He, H.; Wan, Z.; Qin, J.; Wen, Y.; Pan, Z.; Wang, H.; Chen, L. Study on the outcome of patients with aseptic femoral head necrosis treated with percutaneous multiple small-diameter drilling core decompression: A retrospective cohort study based on magnetic resonance imaging and equivalent sphere model analysis. J. Orthop. Surg. Res. 2020, 15, 264. [Google Scholar] [CrossRef] [PubMed]
- Arbab, D.; König, D.P. Atraumatic Femoral Head Necrosis in Adults. Dtsch. Ärzteblatt Int. 2016, 113, 31–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, P.; Liu, X.; Xu, J.; Li, T.; Sun, W.; Li, Z.; Gao, F.; Shi, L.; Li, Z.; Wu, X.; et al. Deep learning for diagnosing osteonecrosis of the femoral head based on magnetic resonance imaging. Comput. Methods Programs Biomed. 2021, 208, 106229. [Google Scholar] [CrossRef]
- Zhu, L.; Han, J.; Guo, R.; Wu, D.; Wei, Q.; Chai, W.; Tang, S. An Automatic Classification of the Early Osteonecrosis of Femoral Head with Deep Learning. Curr. Med. Imaging 2021, 16, 1323–1331. [Google Scholar] [CrossRef]
- Li, Y.; Tian, H. Deep Learning-Based End-to-End Diagnosis System for Avascular Necrosis of Femoral Head. IEEE J. Biomed. Health Inform. 2020, 25, 2093–2102. [Google Scholar] [CrossRef]
- Kerboul, M.; Thomine, J.; Postel, M.; Merle d’Aubigné, R. The conservative surgical treatment of idiopathic aseptic necrosis of the femoral head. J. Bone Jt. Surg. 1974, 56, 291–296. [Google Scholar] [CrossRef]
- Boontanapibul, K.; Huddleston, J.I.; Amanatullah, D.F.; Maloney, W.J.; Goodman, S.B. Modified Kerboul Angle Predicts Outcome of Core Decompression with or without Additional Cell Therapy. J. Arthroplast. 2021, 36, 1879–1886. [Google Scholar] [CrossRef]
- Steinberg, M.E.; Oh, S.C.; Khoury, V.; Udupa, J.K.; Steinberg, D.R. Lesion size measurement in femoral head necrosis. Int. Orthop. 2018, 42, 1585–1591. [Google Scholar] [CrossRef]
- Koo, K.H.; Kim, R. Quantifying the extent of osteonecrosis of the femoral head. A new method using MRI. J. Bone Jt. Surg. 1995, 77, 875–880. [Google Scholar] [CrossRef]
- Theodorou, D.J.; Malizos, K.N.; Beris, A.E.; Theodorou, S.J.; Soucacos, P.N. Multimodal Imaging Quantitation of the Lesion Size in Osteonecrosis of the Femoral Head. Clin. Orthop. Relat. Res. 2001, 386, 54–63. [Google Scholar] [CrossRef]
- Steinberg, D.R.; Steinberg, M.E.; Garino, J.P.; Dalinka, M.; Udupa, J.K. Determining Lesion Size in Osteonecrosis of the Femoral Head. J. Bone Jt. Surg. 2006, 88, 27–34. [Google Scholar] [CrossRef]
- Beck, D.M.; Park, B.K.; Youm, T.; Wolfson, T.S. Arthroscopic Treatment of Labral Tears and Concurrent Avascular Necrosis of the Femoral Head in Young Adults. Arthrosc. Tech. 2013, 2, e367–e371. [Google Scholar] [CrossRef]
- Vora, A. Management of osteonecrosis in children and young adults with acute lymphoblastic leukaemia. Br. J. Haematol. 2011, 155, 549–560. [Google Scholar] [CrossRef]
- Klontzas, M.E.; Stathis, I.; Spanakis, K.; Zibis, A.H.; Marias, K.; Karantanas, A.H. Deep Learning for the Differential Diagnosis between Transient Osteoporosis and Avascular Necrosis of the Hip. Diagnostics 2022, 12, 1870. [Google Scholar] [CrossRef]
- Bento, M.; Fantini, I.; Park, J.; Rittner, L.; Frayne, R. Deep Learning in Large and Multi-Site Structural Brain MR Imaging Datasets. Front. Neuroinform. 2022, 15, 805669. [Google Scholar] [CrossRef]
- Gao, Y.; Xiao, X.; Han, B.; Li, G.; Ning, X.; Wang, D.; Cai, W.; Kikinis, R.; Berkovsky, S.; Di Ieva, A.; et al. Deep Learning Methodology for Differentiating Glioma Recurrence from Radiation Necrosis Using Multimodal Magnetic Resonance Imaging: Algorithm Development and Validation. JMIR Med. Inform. 2020, 8, e19805. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Parameter | Mean ± SD/Number of Hips (%) |
|---|---|
| Patients (hips) | 26 (30 hips) |
| Age (Mean ± SD) | 30 ± 7 |
| Sex (male in%) | 53.85 |
| Etiology, hips | |
| Idiopathic (%) Posttraumatic (%) Systemic (%) Perthes Disease (%) Treatment, hips (%) Non-Operative Treatment Hip Arthroscopy Surgical Hip Dislocation (total) Concomitant Femoral Osteotomy Periacetabular Osteotomy First Surgery: Total Arthroplasty | 13 (43) 3 (10) 11 (37) 3 (10) 12 (40) 0 (0) 14 (47) 5 (16) 1 * (3) 3 (10) |
| Tönnis grade of osteoarthritis, hips (%) | |
| Tönnis grade < 2 | 28 (93) |
| Tönnis grade ≥ 2 | 2 (7) |
| ARCO grading | |
| ARCO I (%) ARCO II (%) ARCO IIIA (%) ARCO IIIB (%) | 2 (7) 4 (13) 13 (43) 11 (37) |
| Modified Kerboul angle (Mean ± SD°) | 198 ± 77 |
| Parameter | Manual Segmentation of 3D MRI | Manual Segmentation of 2D MRI | Automatic Segmentation of 2D MRI | |||
|---|---|---|---|---|---|---|
| Mean ± SD | Range | Mean ± SD | Range | Mean ± SD | Range | |
| Volume of necrosis (cm3) | 8.9 ± 7.4 | 0.7 to 29 | 8.8 ± 7.4 | 0.6 to 28 | 7.9 ± 6.3 | 0.9 to 23 |
| Volume of unaffected bone (cm3) | 39 ± 15 | 20 to 72 | 41 ± 15 | 20 to 71 | 42 ± 14 | 22 to 73 |
| Percent of necrotic bone volume (%) | 19 ± 15 | 2 to 59 | 18 ± 15 | 1 to 54 | 16 ± 13 | 2 to 47 |
| Surface of necrotic bone (cm2) | 14 ± 9.3 | 1.3 to 35 | 13 ± 9.5 | 1.6 to 38 | 12 ± 8.2 | 0.8 to 33 |
| Unaffected femoral head surface (cm2) | 59 ± 14 | 36 to 90 | 59 ± 13 | 42 to 87 | 59 ± 12 | 44 to 84 |
| Percent of necrotic femoral head surface (%) | 23 ± 15 | 2 to 58 | 23 ± 16 | 3 to 60 | 20 ± 14 | 2 to 54 |
| Parameter | Difference (Mean ± SD) | CI | p Value | Correlation | p Value |
|---|---|---|---|---|---|
| Volume of necrosis (cm3) | 0.08 ± 2.8 | −0.97 to 1.1 | 0.873 | Rp = 0.928 | <0.001 |
| Volume of unaffected bone (cm3) | −1.5 ± 3.4 | −2.7 to −0.2 | 0.0234 | Rp = 0.975 | <0.001 |
| Percent of necrotic bone volume (%) | 1 ± 6 | −2 to 3 | 0.526 | Rp = 0.928 | <0.001 |
| Surface of necrotic bone (cm2) | 0.4 ± 3.3 | −0.9 to 1.6 | 0.536 | Rp = 0.938 | <0.001 |
| Unaffected femoral head surface (cm2) | −0.5 ± 4.2 | −2.1 to 1.1 | 0.515 | Rp = 0.958 | <0.001 |
| Percent of necrotic femoral head surface (%) | 1 ± 5 | 1 to 3 | 0.467 | Rp = 0.940 | <0.001 |
| Parameter | Difference, Mean ± SD | CI | p Value | Correlation | p Value |
|---|---|---|---|---|---|
| Volume of necrosis (cm3) | 0.9 ± 2.7 | −0.1 to 1.9 | 0.0858 | Rp = 0.936 | <0.001 |
| Volume of unaffected bone (cm3) | −0.8 ± 2.8 | −1.8 to 0.3 | 0.152 | Rp = 0.982 | <0.001 |
| Percent of necrotic bone volume (%) | 2 ± 5 | 0 to 4 | 0.10 | Rp = 0.935 | <0.001 |
| Necrotic bone surface (cm2) | 1.5 ± 4 | −0.01 to 3 | 0.0517 | Rp = 0.910 | <0.001 |
| Unaffected femoral head surface (cm2) | 0.7 ± 2.6 | −0.3 to 1.6 | 0.173 | Rp = 0.979 | <0.001 |
| Percent of necrotic femoral head surface (%) | 3 ± 7 | 0 to 5 | 0.0641 | Rp = 0.892 | <0.001 |
| Parameters | Manual 2D Segmentation Median (IQR) | Automatic 2D Segmentation Median (IQR) | ||||
|---|---|---|---|---|---|---|
| ARCO 0-II | ARCO > II | p-Value | ARCO 0-II | ARCO > II | p-Value | |
| Modified Kerboul angle (°) | 153 (58) | 195 (70) | 0.0775 | 153 (58) | 195 (70) | 0.0775 |
| Volume of necrosis (cm3) | 2.2 (2.7) | 8.9 (10.1) | 0.0133 | 2.2 (4) | 8.8 (7.9) | 0.0257 |
| Volume of unaffected bone (cm3) | 40 (12.2) | 36 (19.2) | 0.315 | 41 (9.9) | 37 (12.5) | 0.270 |
| Percent of necrotic bone volume (%) | 4 (8) | 15 (16) | 0.0226 | 6 (6) | 13 (16) | 0.0199 |
| Necrotic bone surface (cm2) | 4.5 (4) | 12 (13.6) | 0.0152 | 4.8 (3.6) | 12 (8.2) | 0.0133 |
| Unaffected femoral head surface (cm2) | 54 (12) | 55 (16) | 0.713 | 52 (12) | 55 (16) | 0.825 |
| Percent of necrotic femoral head surface (%) | 8 (10) | 20 (26) | 0.0257 | 9(4) | 21 (12) | 0.0116 |
| Parameter | Manual Segmentation of 3D MRI | Manual Segmentation of 2D MRI | Automatic Segmentation of 2D MRI | |||
|---|---|---|---|---|---|---|
| vs Modified Kerboul | p-Value | vs Modified Kerboul | p-Value | vs Modified Kerboul | p-Value | |
| Volume of necrosis (cm3) | Rp = 0.859 | <0.001 | Rp = 0.865 | <0.001 | Rp = 0.867 | <0.001 |
| Percent of necrotic bone volume (%) | Rp = 0.883 | <0.001 | Rp = 0.896 | <0.001 | Rp = 0.913 | <0.001 |
| Surface of necrotic bone (cm2) | Rp = 0.861 | <0.001 | Rp = 0.869 | <0.001 | Rp = 0.866 | <0.001 |
| Percent of necrotic femoral head surface (%) | Rp = 0.881 | <0.001 | Rp = 0.881 | <0.001 | Rp = 0.909 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ruckli, A.C.; Nanavati, A.K.; Meier, M.K.; Lerch, T.D.; Steppacher, S.D.; Vuilleumier, S.; Boschung, A.; Vuillemin, N.; Tannast, M.; Siebenrock, K.A.; et al. A Deep Learning Method for Quantification of Femoral Head Necrosis Based on Routine Hip MRI for Improved Surgical Decision Making. J. Pers. Med. 2023, 13, 153. https://doi.org/10.3390/jpm13010153
Ruckli AC, Nanavati AK, Meier MK, Lerch TD, Steppacher SD, Vuilleumier S, Boschung A, Vuillemin N, Tannast M, Siebenrock KA, et al. A Deep Learning Method for Quantification of Femoral Head Necrosis Based on Routine Hip MRI for Improved Surgical Decision Making. Journal of Personalized Medicine. 2023; 13(1):153. https://doi.org/10.3390/jpm13010153
Chicago/Turabian StyleRuckli, Adrian C., Andreas K. Nanavati, Malin K. Meier, Till D. Lerch, Simon D. Steppacher, Sébastian Vuilleumier, Adam Boschung, Nicolas Vuillemin, Moritz Tannast, Klaus A. Siebenrock, and et al. 2023. "A Deep Learning Method for Quantification of Femoral Head Necrosis Based on Routine Hip MRI for Improved Surgical Decision Making" Journal of Personalized Medicine 13, no. 1: 153. https://doi.org/10.3390/jpm13010153