
Nomogram for Predicting Portal Vein Thrombosis in Cirrhotic Patients: A Retrospective Cohort Study

Abstract
:1. Introduction
2. Materials and Methods
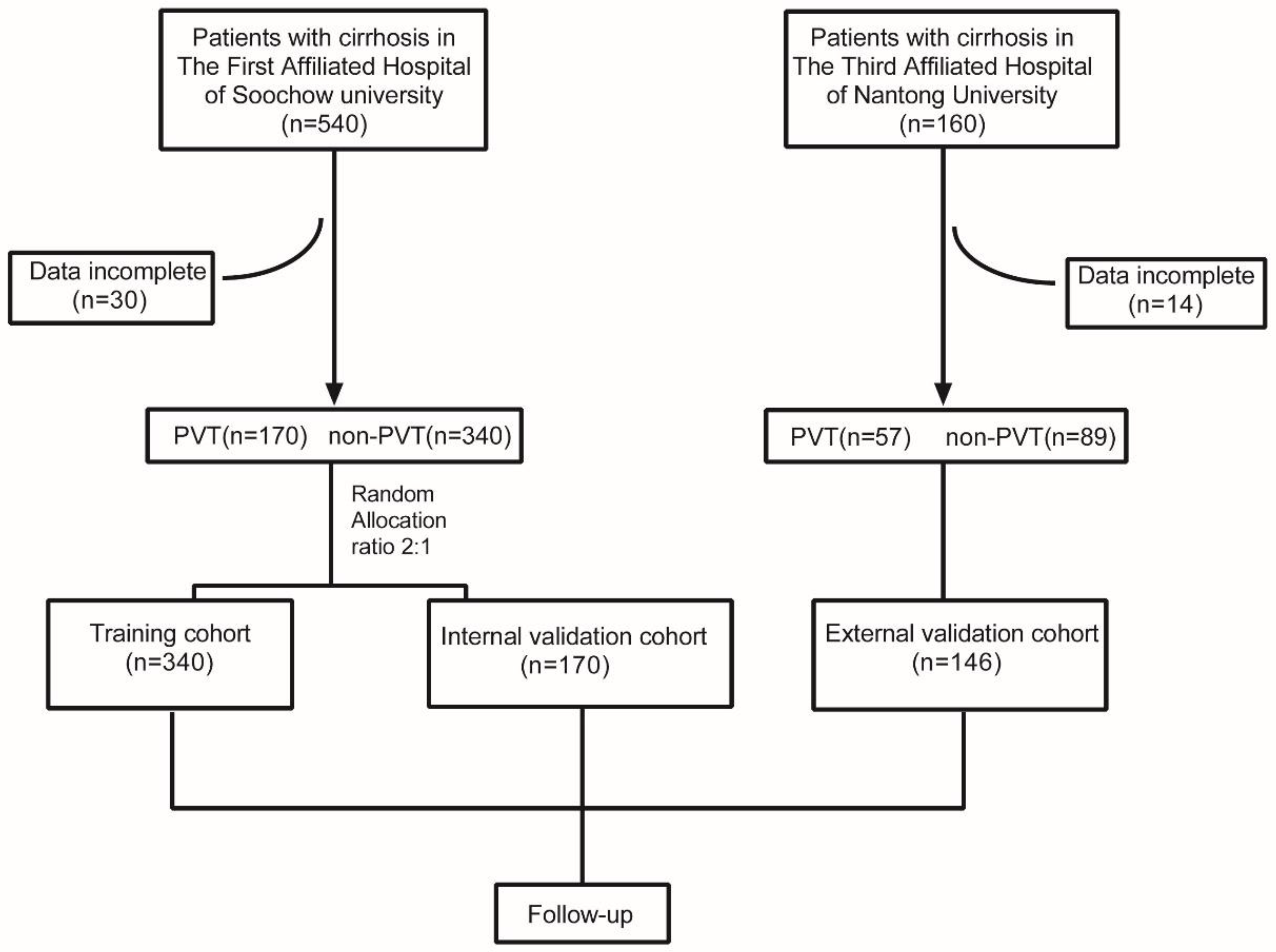
2.1. Patients
2.2. Inclusion and Exclusion Criteria
2.3. Data Collection
2.4. Follow-Up
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
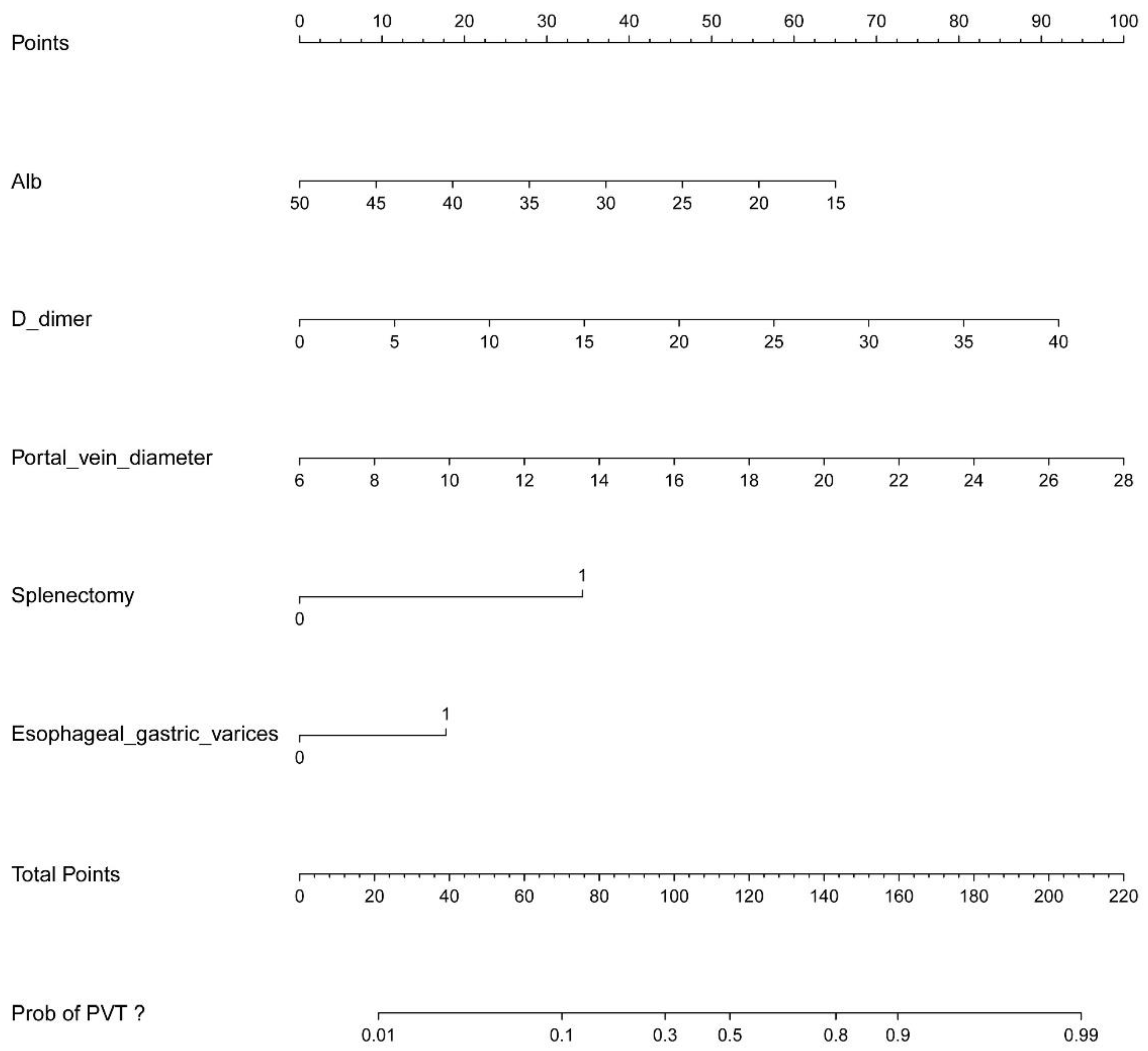
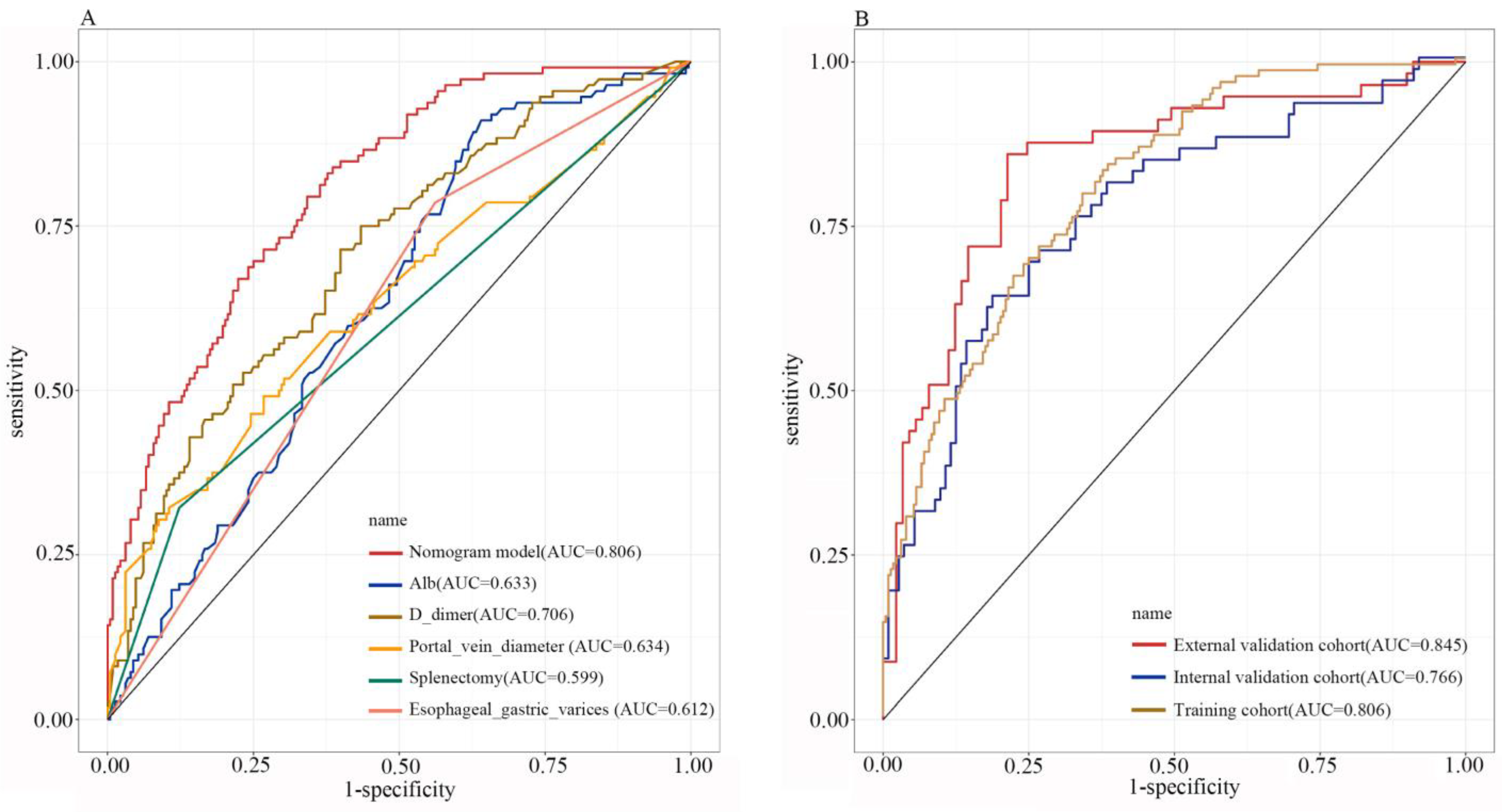
3.2. Nomogram Construction
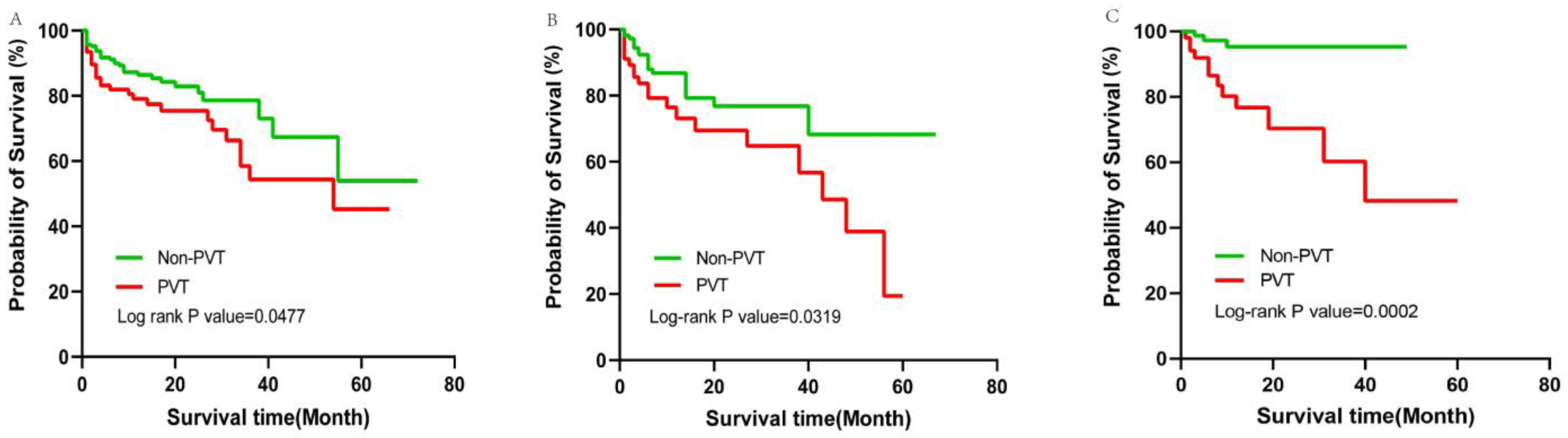
3.3. Outcome of Follow-Up
4. Discussion
5. Prognosis and Complications
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Noronha Ferreira, C.; Marinho, R.T.; Cortez-Pinto, H.; Ferreira, P.; Dias, M.S.; Vasconcelos, M.; Alexandrino, P.; Serejo, F.; Pedro, A.J.; Goncalves, A.; et al. Incidence, predictive factors and clinical significance of development of portal vein thrombosis in cirrhosis: A prospective study. Liver Int. 2019, 39, 1459–1467. [Google Scholar] [CrossRef] [PubMed]
- Tripodi, A.; Mannucci, P.M. The coagulopathy of chronic liver disease. N. Engl. J. Med. 2011, 365, 147–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Senzolo, M.; Garcia-Tsao, G.; Garcia-Pagan, J.C. Current knowledge and management of portal vein thrombosis in cirrhosis. J. Hepatol. 2021, 75, 442–453. [Google Scholar] [CrossRef] [PubMed]
- Hepatobiliary Disease Study Group; Chinese Society of Gastroenterology, Chinese Medical Association. Consensus for management of portal vein thrombosis in liver cirrhosis (2020, Shanghai). J. Dig. Dis. 2021, 22, 176–186. [Google Scholar] [CrossRef] [PubMed]
- Turon, F.; Driever, E.G.; Baiges, A.; Cerda, E.; Garcia-Criado, A.; Gilabert, R.; Bru, C.; Berzigotti, A.; Nunez, I.; Orts, L.; et al. Predicting portal thrombosis in cirrhosis: A prospective study of clinical, ultrasonographic and hemostatic factors. J. Hepatol. 2021, 75, 1367–1376. [Google Scholar] [CrossRef]
- Lopez-Gomez, M.; Llop, E.; Puente, A.; Hernandez Conde, M.; Ruiz, P.; Alvarez, S.; Martinez, J.L.; Abad, J.; Fernandez, N.; Perello, C.; et al. Non-malignant portal vein thrombosis in a cohort of cirrhotic patients: Incidence and risk factors. Hepatol. Res. 2021, 51, 1064–1072. [Google Scholar] [CrossRef]
- Dong, G.; Huang, X.Q.; Zhu, Y.L.; Ding, H.; Li, F.; Chen, S.Y. Increased portal vein diameter is predictive of portal vein thrombosis development in patients with liver cirrhosis. Ann. Transl. Med. 2021, 9, 289. [Google Scholar] [CrossRef]
- Nery, F.; Chevret, S.; Condat, B.; de Raucourt, E.; Boudaoud, L.; Rautou, P.E.; Plessier, A.; Roulot, D.; Chaffaut, C.; Bourcier, V.; et al. Causes and consequences of portal vein thrombosis in 1,243 patients with cirrhosis: Results of a longitudinal study. Hepatology 2015, 61, 660–667. [Google Scholar] [CrossRef]
- Chinese Society of Hepatology. Chinese guidelines on the management of liver cirrhosis. Chin. J. Hepatol. 2019, 27, 846–865. [Google Scholar] [CrossRef]
- Salerno, F.; Guevara, M.; Bernardi, M.; Moreau, R.; Wong, F.; Angeli, P.; Garcia-Tsao, G.; Lee, S.S. Refractory ascites: Pathogenesis, definition and therapy of a severe complication in patients with cirrhosis. Liver Int. 2010, 30, 937–947. [Google Scholar] [CrossRef]
- Chinese Society of Hepatology, C.M.A.; Xu, X.; Duan, Z.; Ding, H.; Li, W.; Jia, J.; Wei, L.; Linghu, E.; Zhuang, H. Chinese guidelines on the management of ascites and its related complications in cirrhosis. Hepatol. Int. 2019, 13, 1–21. [Google Scholar] [CrossRef] [Green Version]
- Violi, F.; Ferro, D. Clotting activation and hyperfibrinolysis in cirrhosis: Implication for bleeding and thrombosis. Semin. Thromb. Hemost. 2013, 39, 426–433. [Google Scholar] [CrossRef] [PubMed]
- Carr, B.I.; Guerra, V.; Donghia, R.; Farinati, F.; Giannini, E.G.; Muratori, L.; Rapaccini, G.L.; Di Marco, M.; Caturelli, E.; Zoli, M.; et al. Identification of Clinical Phenotypes and Related Survival in Patients with Large HCCs. Cancers 2021, 13, 592. [Google Scholar] [CrossRef] [PubMed]
- Folsom, A.R.; Lutsey, P.L.; Heckbert, S.R.; Cushman, M. Serum albumin and risk of venous thromboembolism. Thromb. Haemost. 2010, 104, 100–104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kunutsor, S.K.; Seidu, S.; Katechia, D.T.; Laukkanen, J.A. Inverse association between serum albumin and future risk of venous thromboembolism: Interrelationship with high sensitivity C-reactive protein. Ann. Med. 2018, 50, 240–248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Basili, S.; Carnevale, R.; Nocella, C.; Bartimoccia, S.; Raparelli, V.; Talerico, G.; Stefanini, L.; Romiti, G.F.; Perticone, F.; Corazza, G.R.; et al. Serum Albumin Is Inversely Associated With Portal Vein Thrombosis in Cirrhosis. Hepatol. Commun. 2019, 3, 504–512. [Google Scholar] [CrossRef] [Green Version]
- Cagin, Y.F.; Bilgic, Y.; Berber, I.; Yildirim, O.; Erdogan, M.A.; Firat, F.; Arslan, A.K.; Colak, C.; Seckin, Y.; Harputluoglu, M. The risk factors of portal vein thrombosis in patients with liver cirrhosis. Exp. Ther. Med. 2019, 17, 3189–3194. [Google Scholar] [CrossRef] [Green Version]
- Mikhailidis, D.P.; Mikhailidis, A.M.; Dandona, P. Effect of human plasma proteins on stabilisation of platelet anti-aggregatory activity of prostacyclin. Ann. Clin. Biochem. 1982, 19 (Pt 4), 241–244. [Google Scholar] [CrossRef] [Green Version]
- Joorgensen, K.A.; Stoffersen, E. Heparin like activity of albumin. Thromb. Res. 1979, 16, 569–574. [Google Scholar] [CrossRef]
- van Belle, A.; Buller, H.R.; Huisman, M.V.; Huisman, P.M.; Kaasjager, K.; Kamphuisen, P.W.; Kramer, M.H.; Kruip, M.J.; Kwakkel-van Erp, J.M.; Leebeek, F.W.; et al. Effectiveness of managing suspected pulmonary embolism using an algorithm combining clinical probability, D-dimer testing, and computed tomography. JAMA 2006, 295, 172–179. [Google Scholar] [CrossRef]
- Tritschler, T.; Kraaijpoel, N.; Le Gal, G.; Wells, P.S. Venous Thromboembolism: Advances in Diagnosis and Treatment. JAMA 2018, 320, 1583–1594. [Google Scholar] [CrossRef] [PubMed]
- Dai, J.; Qi, X.; Li, H.; Guo, X. Role of D-dimer in the Development of Portal Vein Thrombosis in Liver Cirrhosis: A Meta-analysis. Saudi J. Gastroenterol. 2015, 21, 165–174. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Xu, B.Y.; Wang, X.B.; Zheng, X.; Huang, Y.; Chen, J.; Meng, Z.J.; Gao, Y.H.; Qian, Z.P.; Liu, F.; et al. Prevalence and Clinical Significance of Portal Vein Thrombosis in Patients With Cirrhosis and Acute Decompensation. Clin. Gastroenterol. Hepatol. 2020, 18, 2564–2572.e1. [Google Scholar] [CrossRef] [PubMed]
- Ordieres-Ortega, L.; Demelo-Rodriguez, P.; Galeano-Valle, F.; Kremers, B.M.M.; Ten Cate-Hoek, A.J.; Ten Cate, H. Predictive value of D-dimer testing for the diagnosis of venous thrombosis in unusual locations: A systematic review. Thromb. Res. 2020, 189, 5–12. [Google Scholar] [CrossRef]
- Gris, J.C.; Bouvier, S.; Cochery-Nouvellon, E.; Faillie, J.L.; Lissalde-Lavigne, G.; Lefrant, J.Y. Fibrin-related markers in patients with septic shock: Individual comparison of D-dimers and fibrin monomers impacts on prognosis. Thromb. Haemost. 2011, 106, 1228–1230. [Google Scholar] [CrossRef]
- Fujinaga, A.; Ohta, M.; Endo, Y.; Tada, K.; Kawamura, M.; Nakanuma, H.; Ogawa, K.; Watanabe, K.; Kawasaki, T.; Masuda, T.; et al. Clinical Significance of Splenic Vessels and Anatomical Features in Laparoscopic Splenectomy. J. Laparoendosc. Adv. Surg. Tech. A 2021, 31, 632–637. [Google Scholar] [CrossRef]
- Yuan, H.L.; Wang, M.; Chu, W.W.; Li, F.X.; Lu, J.J.; Li, Y. Nomogram Model for Prediction of Portal Vein Thrombosis in Patients with Liver Cirrhosis After Splenectomy: A Retrospective Analysis of 2 Independent Cohorts. Med. Sci. Monit. 2021, 27, e929844. [Google Scholar] [CrossRef]
- Tsamalaidze, L.; Stauffer, J.A.; Brigham, T.; Asbun, H.J. Postsplenectomy thrombosis of splenic, mesenteric, and portal vein (PST-SMPv): A single institutional series, comprehensive systematic review of a literature and suggested classification. Am. J. Surg. 2018, 216, 1192–1204. [Google Scholar] [CrossRef]
- Naymagon, L. Venous thrombosis of the liver: Current and emerging concepts in management. Transl. Res. 2020, 225, 54–69. [Google Scholar] [CrossRef]
- Qi, X.; Han, G.; Ye, C.; Zhang, Y.; Dai, J.; Peng, Y.; Deng, H.; Li, J.; Hou, F.; Ning, Z.; et al. Splenectomy Causes 10-Fold Increased Risk of Portal Venous System Thrombosis in Liver Cirrhosis Patients. Med. Sci. Monit. 2016, 22, 2528–2550. [Google Scholar] [CrossRef]
- Cool, J.; Rosenblatt, R.; Kumar, S.; Lucero, C.; Fortune, B.; Crawford, C.; Jesudian, A. Portal vein thrombosis prevalence and associated mortality in cirrhosis in a nationally representative inpatient cohort. J. Gastroenterol. Hepatol. 2019, 34, 1088–1092. [Google Scholar] [CrossRef] [PubMed]
- Berry, K.; Taylor, J.; Liou, I.W.; Ioannou, G.N. Portal vein thrombosis is not associated with increased mortality among patients with cirrhosis. Clin. Gastroenterol. Hepatol. 2015, 13, 585–593. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Training Cohort | Internal Validation Cohort | External Validation Cohort | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total (n = 340) | Non-PVT (n = 228) | PVT (n = 112) | p Value | Total (n = 170) | Non-PVT (n = 112) | PVT (n = 58) | p Value | Total (n = 146) | Non-PVT (n = 89) | PVT (n = 57) | p Value | |
| Male | 193 | 127 | 66 | 0.572 | 105 | 70 | 35 | 0.784 | 99 | 61 | 38 | 0.813 |
| Age(year) | 59.06 ± 13.42 | 58.86 ± 14.17 | 59.49 ± 11.78 | 0.663 | 60.74 ± 13.12 | 60.96 ± 13.86 | 60.31 ± 11.65 | 0.759 | 56.90 ± 12.16 | 55.38 ± 12.19 | 59.26 ± 11.83 | 0.060 |
| Disease course(year) | 6.00 (1.00, 10.00) | 5.00 (1.00, 10.00) | 8.00 (3.00, 10.00) | 0.005 | 8.50 (1.00, 10.00) | 6.00 (1.00, 10.00) | 10.00 (4.75, 10.00) | 0.004 | 2.00 (1.00, 5.25) | 1.00 (1.00, 4.00) | 4.00 (1.00, 8.00) | 0.002 |
| Etiology | ||||||||||||
| Viral hepatitis | 149 | 104 | 45 | 0.342 | 64 | 40 | 24 | 0.470 | 97 | 58 | 39 | 0.685 |
| Schistosoma hepatitis | 48 | 27 | 21 | 0.086 | 32 | 24 | 8 | 0.227 | - | - | - | - |
| Autoimmune hepatitis | 43 | 28 | 15 | 0.772 | 25 | 17 | 8 | 0.809 | 15 | 9 | 6 | 0.936 |
| Alcohol hepatitis | 25 | 19 | 6 | 0.323 | 15 | 10 | 5 | 0.947 | 18 | 11 | 7 | 0.989 |
| Others 1 | 75 | 50 | 25 | 0.935 | 34 | 21 | 13 | 0.571 | 16 | 11 | 5 | 0.498 |
| Child–Pugh Score | 8.00 (6.00, 9.00) | 8.00 (6.00, 9.00) | 8.00 (7.00, 10.00) | 0.008 | 8.00 (7.00, 9.00) | 8.00 (6.00, 9.00) | 8.00 (7.00, 9.25) | 0.672 | 8.00 (6.00, 9.00) | 7.00 (5.00, 8.00) | 8.00 (7.00, 10.00) | 0.001 |
| WBC (×109/L) | 5.8 ± 3.9 | 5.63 ± 3.77 | 6.15 ± 4.15 | 0.248 | 5.75 ± 3.75 | 5.37 ± 3.02 | 6.50 ± 4.80 | 0.106 | 4.34 ± 2.52 | 3.94 ± 1.58 | 4.95 ± 3.44 | 0.042 |
| PLT (×109/L) | 78.50 (50.00, 129.25) | 78.50 (51.00, 122.75) | 78.00 (45.25, 146.75) | 0.814 | 77.5 (50.00, 117.00) | 75.50 (50.00, 103.50) | 86.50 (47.25, 161.25) | 0.166 | 77.50 (51.00, 152.75) | 75.00 (48.50, 124.50) | 86.00 (54.50, 191.00) | 0.124 |
| PDW (%) | 15.83 ± 2.46 | 15.86 ± 14.17 | 15.77 ± 2.12 | 0.771 | 15.61 ± 2.14 | 15.85 ± 2.05 | 15.17 ± 2.24 | 0.057 | 14.53 ± 3.03 | 14.69 ± 2.76 | 14.29 ± 3.42 | 0.495 |
| MPV (fL) | 11.35 ± 1.69 | 11.35 ± 1.68 | 11.34 ± 1.73 | 0.977 | 11.17 ± 1.52 | 11.21 ± 1.56 | 11.09 ± 2.24 | 0.639 | 11.26 ± 1.34 | 11.35 ± 1.30 | 11.12 ± 1.41 | 0.372 |
| Hb (g/L) | 97.24 ± 29.07 | 99.78 ± 29.81 | 92.08 ± 26.89 | 0.021 | 100.57 ± 29.95 | 102.37 ± 30.71 | 97.10 ± 28.36 | 0.278 | 112.10 ± 33.07 | 119.63 ± 33.60 | 100.33 ± 28.74 | <0.001 |
| ALT (U/L) | 24.10 (16.33, 38.28) | 25.00 (17.25, 39.18) | 22.75 (14.45, 37.15) | 0.177 | 22.85 (15.55, 33.80) | 22.75 (15.78, 39.00) | 23.55 (15.38, 30.65) | 0.643 | 30.50 (21.00, 61.00) | 38.00 (24.00, 99.00) | 25.00 (18.50, 37.50) | <0.001 |
| Alb (g/L) | 31.18 ± 5.62 | 32.07 ± 5.87 | 29.38 ± 4.58 | <0.001 | 30.64 ± 5.86 | 31.36 ± 6.52 | 29.24 ± 4.00 | 0.010 | 33.20 ± 6.22 | 33.56 ± 6.98 | 31.42 ± 3.93 | 0.020 |
| TG (μmol/L) | 1.04 ± 0.66 | 1.06 ± 0.69 | 0.99 ± 0.60 | 0.312 | 1.08 ± 0.69 | 1.13 ± 0.70 | 0.97 ± 0.78 | 0.147 | 1.10 ± 0.73 | 1.28 ± 0.83 | 0.78 ± 0.32 | <0.001 |
| PT (s) | 15.96 ± 3.19 | 15.64 ± 2.89 | 16.62 ± 3.66 | 0.007 | 15.84 ± 4.13 | 16.01 ± 4.71 | 15.51 ± 2.70 | 0.459 | 13.96 ± 2.64 | 13.61 ± 2.72 | 14.50 ± 2.42 | 0.046 |
| AT-IIIa (%) | 59.15 ± 19.41 | 60.14 ± 2.89 | 57.13 ± 18.23 | 0.178 | 59.67 ± 19.59 | 61.38 ± 20.27 | 56.36 ± 17.89 | 0.113 | 65.04 ± 21.95 | 66.81 ± 21.69 | 62.26 ± 22.26 | 0.222 |
| D-dimer (μg/mL) | 1.88 (0.72, 4.09) | 1.20 (0.55, 3.03) | 3.40 (1.47, 8.60) | <0.001 | 1.99 (0.69, 4.23) | 1.33 (0.54, 3.11) | 3.25 (1.71, 6.67) | <0.001 | 1.35 (0.39, 3.39) | 0.58 (0.21, 2.27) | 3.16 (1.62, 6.46) | <0.001 |
| PVD (mm) | 13.56 ± 3.09 | 13.02 ± 2.56 | 14.67 ± 3.74 | <0.001 | 13.91 ± 3.37 | 13.08 ± 2.89 | 15.51 ± 3.65 | <0.001 | 14.03 ± 2.84 | 13.27 ± 2.09 | 15.22 ± 3.42 | <0.001 |
| Ascites | 189 | 112 | 77 | 0.001 | 104 | 64 | 40 | 0.134 | 78 | 30 | 48 | <0.001 |
| Esophageal gastric varices | 216 | 128 | 88 | <0.001 | 107 | 62 | 45 | 0.004 | 84 | 32 | 52 | <0.001 |
| Splenectomy | 64 | 28 | 36 | <0.001 | 26 | 12 | 14 | 0.021 | 21 | 1 | 20 | <0.001 |
| Spleen thickness(mm) | 51.75 ± 14.12 | 50.06 ± 13.17 | 56.18 ± 15.58 | 0.001 | 51.03 ± 11.44 | 49.78 ± 11.44 | 53.89 ± 11.05 | 0.047 | 43.69 ± 12.78 | 41.70 ± 12.60 | 47.49 ± 12.42 | 0.025 |
| Spleen length(mm) | 140.88 ± 36.12 | 136.15 ± 35.32 | 153.32 ± 35.45 | <0.001 | 141.94 ± 33.32 | 140.32 ± 30.68 | 145.61 ± 38.78 | 0.382 | 140.71 ± 34.90 | 137.65 ± 33.62 | 146.59 ± 37.00 | 0.208 |
| Univariate Regression Analysis | Multivariate Regression Analysis | |||||||
|---|---|---|---|---|---|---|---|---|
| Wald Value | p Value | OR | 95% CI | Wald Value | p Value | OR | 95% CI | |
| Child–Pugh Score | 7.342 | 0.007 | 1.163 | 1.043, 1.298 | 0.290 | 0.590 | 0.939 | 0.747, 1.180 |
| PT | 6.778 | 0.009 | 1.009 | 1.024, 1.180 | 0.831 | 0.362 | 1.047 | 0.948, 1.157 |
| Hb | 5.210 | 0.022 | 0.991 | 0.983, 0.999 | 0.283 | 0.594 | 1.003 | 0.992, 1.014 |
| Alb | 16.286 | <0.001 | 0.908 | 0.867, 0.952 | 6.158 | 0.013 | 0.911 | 0.847, 0.981 |
| D-dimer | 23.328 | <0.001 | 1.136 | 1.079, 1.197 | 13.607 | <0.001 | 1.116 | 1.053, 1.184 |
| PVD | 19.205 | <0.001 | 1.195 | 1.103, 1.294 | 20.350 | <0.001 | 1.241 | 1.130, 1.363 |
| Splenectomy | 18.196 | <0.001 | 3.383 | 1.933, 5.924 | 23.658 | <0.001 | 5.512 | 2.771, 10.966 |
| Spleen length | 11.823 | 0.001 | 1.014 | 1.006, 1.021 | 0.909 | 0.340 | 1.006 | 0.994, 1.018 |
| Spleen thickness | 9.779 | 0.002 | 1.030 | 1.011, 1.050 | 0.055 | 0.815 | 1.004 | 0.974, 1.034 |
| Ascites | 11.475 | 0.001 | 2.279 | 1.415, 3.670 | 0.580 | 0.446 | 1.300 | 0.662, 2.553 |
| Esophageal gastric varices | 15.635 | <0.001 | 2.865 | 1.700, 4.826 | 6.708 | 0.010 | 2.424 | 1.240, 4.738 |
| Training Cohort | Internal Validation Cohort | External Validation Cohort | χ2 | p Value | |
|---|---|---|---|---|---|
| Total | 112 | 58 | 57 | 6.188 | 0.630 |
| Main trunk and branches of portal vein | 74 (66.07%) | 37 (63.79%) | 31 (54.39%) | ||
| Portal vein and splenic vein | 5 (4.46%) | 6 (10.34%) | 4 (7.02%) | ||
| Portal vein and superior mesenteric vein | 22 (19.64%) | 11 (18.97%) | 13 (22.80%) | ||
| Splenic vein or superior mesenteric vein | 3 (2.68%) | 1 (1.72%) | 4 (7.02%) | ||
| All 1 | 8 (7.12%) | 3 (5.17%) | 5 (8.77%) |
| Training Cohort | Internal Validation Cohort | External Validation Cohort | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total | Non-PVT | PVT | p Value | Total | Non-PVT | PVT | p Value | Total | Non-PVT | PVT | p Value | |
| Recurrent EGVB (n=) | 67 | 35 | 32 | 0.009 | 38 | 19 | 19 | 0.048 | 29 | 10 | 19 | 0.001 |
| RA (n=) | 59 | 35 | 24 | 0.172 | 28 | 18 | 10 | 0.850 | 52 | 25 | 27 | 0.016 |
| HE (n=) | 25 | 17 | 8 | 0.528 | 18 | 9 | 9 | 0.269 | 22 | 8 | 14 | 0.009 |
| Liver failure (n=) | 9 | 5 | 4 | 0.286 | 6 | 5 | 1 | 0.590 | 13 | 6 | 7 | 0.259 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ding, J.; Zhao, F.; Miao, Y.; Liu, Y.; Zhang, H.; Zhao, W. Nomogram for Predicting Portal Vein Thrombosis in Cirrhotic Patients: A Retrospective Cohort Study. J. Pers. Med. 2023, 13, 103. https://doi.org/10.3390/jpm13010103
Ding J, Zhao F, Miao Y, Liu Y, Zhang H, Zhao W. Nomogram for Predicting Portal Vein Thrombosis in Cirrhotic Patients: A Retrospective Cohort Study. Journal of Personalized Medicine. 2023; 13(1):103. https://doi.org/10.3390/jpm13010103
Chicago/Turabian StyleDing, Jingnuo, Fazhi Zhao, Youhan Miao, Yunnuo Liu, Huiting Zhang, and Weifeng Zhao. 2023. "Nomogram for Predicting Portal Vein Thrombosis in Cirrhotic Patients: A Retrospective Cohort Study" Journal of Personalized Medicine 13, no. 1: 103. https://doi.org/10.3390/jpm13010103