Depression, Stress, and Suicide in Korean Adults before and during the COVID-19 Pandemic Using Data from the Korea National Health and Nutritional Examination Survey

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
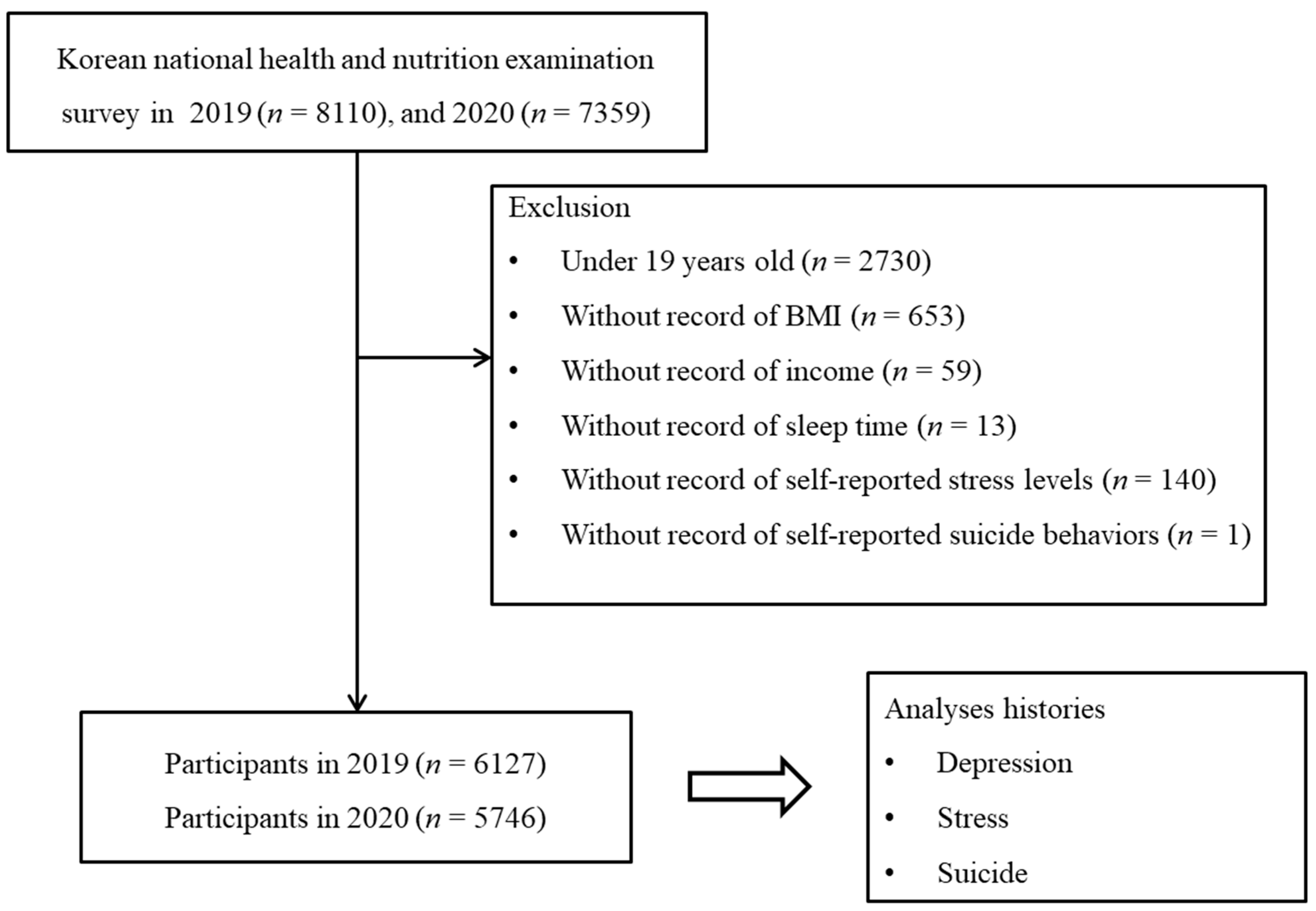
2.1. Study Population and Data Collection
2.2. Survey
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- The Lancet Psychiatry. COVID-19 and mental health. Lancet Psychiatry 2021, 8, 87. [Google Scholar] [CrossRef]
- Matschke, J.; Lütgehetmann, M.; Hagel, C.; Sperhake, J.P.; Schröder, A.S.; Edler, C.; Mushumba, H.; Fitzek, A.; Allweiss, L.; Dandri, M.; et al. Neuropathology of patients with COVID-19 in Germany: A post-mortem case series. Lancet Neurol. 2020, 19, 919–929. [Google Scholar] [CrossRef]
- Park, J.-H.; Jang, W.; Kim, S.-W.; Lee, J.; Lim, Y.-S.; Cho, C.-G.; Park, S.-W.; Kim, B.H. The Clinical Manifestations and Chest Computed Tomography Findings of Coronavirus Disease 2019 (COVID-19) Patients in China: A Proportion Meta-Analysis. Clin. Exp. Otorhinolaryngol. 2020, 13, 95–105. [Google Scholar] [CrossRef] [PubMed]
- Pierce, M.; Hope, H.; Ford, T.; Hatch, S.; Hotopf, M.; John, A.; Kontopantelis, E.; Webb, R.; Wessely, S.; McManus, S.; et al. Mental health before and during the COVID-19 pandemic: A longitudinal probability sample survey of the UK population. Lancet Psychiatry 2020, 7, 883–892. [Google Scholar] [CrossRef]
- Pierce, M.; McManus, S.; Jessop, C.; John, A.; Hotopf, M.; Ford, T.; Hatch, S.; Wessely, S.; Abel, K.M. Says who? The significance of sampling in mental health surveys during COVID-19. Lancet Psychiatry 2020, 7, 567–568. [Google Scholar] [CrossRef]
- Thomas, S.P. Focus on Depression and Suicide in the Era of COVID-19. Issues Ment. Health Nurs. 2020, 41, 559. [Google Scholar] [CrossRef]
- Chen, F.; Zheng, D.; Liu, J.; Gong, Y.; Guan, Z.; Lou, D. Depression and anxiety among adolescents during COVID-19: A cross-sectional study. Brain Behav. Immun. 2020, 88, 36–38. [Google Scholar] [CrossRef]
- Kotabagi, P.; Fortune, L.; Essien, S.; Nauta, M.; Yoong, W. Anxiety and depression levels among pregnant women with COVID-19. Acta Obstet. Gynecol. Scand. 2020, 99, 953–954. [Google Scholar] [CrossRef]
- Kim, S.; Hwang, J. Examining Risk Factors for Mental Health during the COVID-19 Pandemic-Focusing on Older Adults in South Korea. Int. J. Public Health 2022, 67, 1604487. [Google Scholar] [CrossRef]
- Kim, H.; Jhon, M.; Kim, J.-W.; Kang, H.-J.; Ryu, S.; Kim, J.-M.; Lee, J.-Y.; Kim, S.-W. Factors Associated with Depression and Anxiety in Korean Adolescents During the COVID-19 Pandemic. Psychiatry Investig. 2022, 19, 551–561. [Google Scholar] [CrossRef]
- Vuong, Q.H.; Napier, N.K. Acculturation and global mindsponge: An emerging market perspective. Int. J. Intercult. Relat. 2015, 49, 354–367. [Google Scholar] [CrossRef]
- Nguyen, M.H.; Le, T.T.; Nguyen, H.T.; Ho, M.T.; Nguyen, H.T.T.; Vuong, Q.H. Alice in Suicideland: Exploring the Suicidal Ideation Mechanism through the Sense of Connectedness and Help-Seeking Behaviors. Int. J. Environ. Res. Public Health 2021, 18, 3681. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.U.; Park, J.I.; Lee, S.; Oh, I.H.; Choi, J.M.; Oh, C.M. Changing trends in suicide rates in South Korea from 1993 to 2016: A descriptive study. BMJ Open 2018, 8, e023144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, G.E.; Jo, M.W.; Shin, Y.W. Increased prevalence of depression in South Korea from 2002 to 2013. Sci. Rep. 2020, 10, 16979. [Google Scholar] [CrossRef]
- Korea National Health and Nutrition Examination Survey. Available online: https://knhanes.kdca.go.kr/knhanes/main.do (accessed on 2 October 2021).
- Min, C.; Kim, H.-J.; Park, I.-S.; Park, B.; Kim, J.-H.; Sim, S.; Choi, H.G. The association between sleep duration, sleep quality, and food consumption in adolescents: A cross-sectional study using the Korea Youth Risk Behavior Web-based Survey. BMJ Open 2018, 8, e022848. [Google Scholar] [CrossRef]
- Li, Y.; Scherer, N.; Felix, L.; Kuper, H. Prevalence of depression, anxiety and post-traumatic stress disorder in health care workers during the COVID-19 pandemic: A systematic review and meta-analysis. PLoS ONE 2021, 16, e0246454. [Google Scholar] [CrossRef]
- Pérez-Cano, H.J.; Moreno-Murguía, M.B.; Morales-López, O.; Crow-Buchanan, O.; English, J.A.; Lozano-Alcázar, J.; Somilleda-Ventura, S.A. Anxiety, depression, and stress in response to the coronavirus disease-19 pandemic. Cir. Cir. 2020, 88, 562–568. [Google Scholar] [CrossRef]
- Santomauro, D.F.; Herrera, A.M.M.; Shadid, J.; Zheng, P.; Ashbaugh, C.; Pigott, D.M.; Abbafati, C.; Adolph, C.; Amlag, J.O.; Aravkin, A.Y.; et al. Global prevalence and burden of depressive and anxiety disorders in 204 countries and territories in 2020 due to the COVID-19 pandemic. Lancet 2021, 398, 1700–1712. [Google Scholar] [CrossRef]
- Zhang, Y.; Bao, X.; Yan, J.; Miao, H.; Guo, C. Anxiety and Depression in Chinese Students During the COVID-19 Pandemic: A Meta-Analysis. Front. Public Health 2021, 9, 697642. [Google Scholar] [CrossRef]
- Fodjo, J.N.S.; Ngarka, L.; Njamnshi, W.Y.; Nfor, L.N.; Mengnjo, M.K.; Mendo, E.L.; Angwafor, S.A.; Basseguin, J.G.A.; Nkouonlack, C.; Njit, E.N.; et al. Fear and depression during the COVID-19 outbreak in Cameroon: A nation-wide observational study. BMC Psychiatry 2021, 21, 356. [Google Scholar] [CrossRef]
- González-Sanguino, C.; Ausín, B.; Castellanos, M.Á.; Saiz, J.; López-Gómez, A.; Ugidos, C.; Muñoz, M. Mental health consequences during the initial stage of the 2020 Coronavirus pandemic (COVID-19) in Spain. Brain Behav. Immun. 2020, 87, 172–176. [Google Scholar] [CrossRef] [PubMed]
- Min, S.; Jeong, Y.H.; Kim, J.; Koo, J.W.; Ahn, Y.M. The Aftermath: Post-pandemic Psychiatric Implications of the COVID-19 Pandemic, a South Korean Perspective. Front. Psychiatry 2021, 12, 671722. [Google Scholar] [CrossRef] [PubMed]
- Chong, T.W.H.; Curran, E.; Ames, D.; Lautenschlager, N.T.; Castle, D.J. Mental health of older adults during the COVID-19 pandemic: Lessons from history to guide our future. Int. Psychogeriatr. 2020, 32, 1249–1250. [Google Scholar] [CrossRef] [PubMed]
- Vuong, Q.; Le, T.; Khuc, Q.; Nguyen, M. A New Theory of Serendipity: Nature, Emergence and Mechanism; De Gruyter: Berlin, Germany, 2022. [Google Scholar]
- Kim, S.Y.; Kim, D.W. Does the Clinical Spectrum of Coronavirus Disease 2019 (COVID-19) Show Regional Differences? Clin. Exp. Otorhinolaryngol. 2020, 13, 83–84. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | Year | p Value * | ||
|---|---|---|---|---|
| 2019 | 2020 | |||
| Age (yrs, mean, SD) | 51.7 (16.9) | 52.0 (17.3) | 0.799 | |
| Age groups (yrs, n, %) | 0.892 | |||
| 19–39 | 1656 (34.9) | 1552 (34.3) | ||
| 40–59 | 2258 (39.3) | 2009 (39.2) | ||
| ≥60 | 2213 (25.8) | 2185 (26.5) | ||
| Sex (n, %) | 0.695 | |||
| Males | 2719 (49.7) | 2590 (50.0) | ||
| Females | 3408 (50.3) | 3156 (50.0) | ||
| Income (mean, SD) | 3.2 (1.4) | 3.3 (1.4) | 0.551 | |
| Income group (n, %) | 0.938 | |||
| 1 (lowest) | 932 (11.4) | 804 (11.0) | ||
| 2 | 1131 (16.5) | 1043 (15.6) | ||
| 3 | 1240 (21.5) | 1183 (21.3) | ||
| 4 | 1383 (24.6) | 1332 (25.0) | ||
| 5 (highest) | 1441 (26.0) | 1384 (27.1) | ||
| Employment (n, %) | 0.068 | |||
| Unemployed | 2557 (1.2) | 2520 (1.3) | ||
| Employed | 3570 (1.9) | 3226 (1.8) | ||
| Educational status (n, %) | 0.498 | |||
| Elementary school or under, Unknown | 1331 (16.2) | 1297 (16.9) | ||
| Junior high school | 554 (7.5) | 517 (7.1) | ||
| High school | 1963 (34.1) | 1884 (36.2) | ||
| College or over | 2279 (42.1) | 2048 (39.7) | ||
| House type (n, %) | 0.678 | |||
| Detached house | 1906 (27.7) | 1859 (27.7) | ||
| Condominium | 3343 (57.0) | 3203 (60.2) | ||
| Raw houses | 829 (14.5) | 655 (11.7) | ||
| Others | 49 (0.8) | 29 (0.4) | ||
| Marriage status (n, %) | 0.103 | |||
| Married | 4210 (66.6) | 3744 (63.5) | ||
| Unmarried | 861 (10.5) | 843 (10.9) | ||
| Unknown | 1056 (22.9) | 1159 (25.6) | ||
| Body mass index (mean, SD) | 23.9 (3.6) | 24.2 (3.7) | 0.001 * | |
| Smoking status (n, %) | ||||
| Nonsmoker | 3635 (56.5) | 3451 (56.8) | ||
| Past smoker | 1418 (23.1) | 1331 (23.8) | ||
| Current smoker | 1074 (20.3) | 964 (19.4) | ||
| Alcohol consumption (n, %) | 0.070 | |||
| Nonconsumer | 2824 (42.1) | 2805 (44.4) | ||
| 1 to 5 times/mo | 2005 (36.0) | 1777 (33.3) | ||
| ≥2 times/week | 1298 (21.9) | 1164 (22.3) | ||
| Sleep duration (mean, SD) | 6.9 (1.4) | 7.0 (1.4) | 0.097 | |
| Hypertension (n, %) | 1549 (20.4) | 1481 (20.7) | 0.817 | |
| Dyslipidemia (n, %) | 1190 (16.4) | 1280 (18.5) | 0.021 * | |
| Stroke (n, %) | 138 (1.8) | 119 (1.5) | 0.273 | |
| Ischemic heart disease (n, %) | 181 (2.4) | 175 (2.1) | 0.390 | |
| Diabetes mellitus (n, %) | 600 (8.1) | 645 (9.1) | 0.137 | |
| Chronic kidney disease (n, %) | 24 (0.4) | 102 (1.5) | <0.001 * | |
| Depression (n, %) | ||||
| Doctor-diagnosed | 285 (4.1) | 292 (4.5) | 0.326 | |
| Current | 159 (2.2) | 182 (2.7) | 0.115 | |
| Stress (n, %) | 0.741 | |||
| None | 965 (13.9) | 901 (13.4) | ||
| A little | 3533 (57.4) | 3270 (57.7) | ||
| A lot | 1347 (23.8) | 1295 (23.6) | ||
| Very severe | 282 (4.8) | 280 (5.3) | ||
| Suicide (n, %) | ||||
| Planning suicide | 83 (1.3) | 109 (1.7) | 0.126 | |
| Attempting suicide | 25 (0.4) | 26 (0.4) | 0.830 | |
| Characteristics | Odds Ratios for Depression in 2020 Compared to 2019 | |||||
|---|---|---|---|---|---|---|
| Crude | p Value * | Adjusted † | p Value * | |||
| Doctor-diagnosed depression | ||||||
| Total participants (n = 11,873) | 1.11 (0.90–1.37) | 0.328 | 1.05 (0.85–1.30) | 0.647 | ||
| Age | ||||||
| 19–39 years old (n = 3208) | 1.81 (1.17–2.81) | 0.008 * | 1.58 (1.00–2.50) | 0.049 * | ||
| 40–59 years old (n = 4267) | 0.84 (0.59–1.19) | 0.331 | 0.78 (0.55–1.09) | 0.148 | ||
| ≥60 years old (n = 4398) | 0.94 (0.68–1.30) | 0.696 | 0.92 (0.66–1.29) | 0.633 | ||
| Sex | ||||||
| Males (n = 5309) | 1.11 (0.76–1.62) | 0.586 | 1.00 (0.69–1.46) | 0.989 | ||
| Females (n = 6564) | 1.12 (0.87–1.42) | 0.379 | 1.06 (0.83–1.36) | 0.625 | ||
| Current depression | ||||||
| Total participants (n = 11,873) | 1.24 (0.95–1.63) | 0.117 | 1.19 (0.91–1.56) | 0.213 | ||
| Age | ||||||
| 19–39 years old (n = 3208) | 2.01 (1.15–3.52) | 0.014 | 1.75 (0.97–3.18) | 0.064 | ||
| 40–59 years old (n = 4267) | 0.90 (0.59–1.39) | 0.642 | 0.84 (0.54–1.30) | 0.429 | ||
| ≥60 years old (n = 4398) | 1.06 (0.69–1.64) | 0.777 | 1.08 (0.69–1.71) | 0.736 | ||
| Sex | ||||||
| Males (n = 5309) | 1.19 (0.75–1.90) | 0.462 | 1.06 (0.66–1.69) | 0.817 | ||
| Females (n = 6564) | 1.27 (0.93–1.74) | 0.130 | 1.25 (0.90–1.72) | 0.183 | ||
| Characteristics | Odds Ratios for Stress Level in 2020 Compared to 2019 | ||||
|---|---|---|---|---|---|
| Crude | p Value * | Adjusted † | p Value * | ||
| Total participants (n = 11,873) | |||||
| A little stress | 1.04 (0.90–1.21) | 0.587 | 1.08 (0.94–1.24) | 0.300 | |
| A lot of stress | 1.03 (0.85–1.23) | 0.792 | 1.07 (0.90–1.27) | 0.458 | |
| Very severe stress | 1.15 (0.89–1.49) | 0.283 | 1.19 (0.93–1.54) | 0.168 | |
| Characteristics | Odds Ratios for Suicide in 2020 Compared to 2019 | ||||
|---|---|---|---|---|---|
| Crude | p Value * | Adjusted † | p Value * | ||
| Total participants (n = 11,873) | |||||
| Planning suicide | 1.34 (0.92–1.96) | 0.130 | 1.31 (0.90–1.90) | 0.161 | |
| Attempting suicide | 0.93 (0.50–1.76) | 0.831 | 0.78 (0.41–1.48) | 0.438 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, S.Y.; Yoo, D.M.; Kwon, M.J.; Kim, J.H.; Kim, J.-H.; Wee, J.H.; Choi, H.G. Depression, Stress, and Suicide in Korean Adults before and during the COVID-19 Pandemic Using Data from the Korea National Health and Nutritional Examination Survey. J. Pers. Med. 2022, 12, 1305. https://doi.org/10.3390/jpm12081305
Kim SY, Yoo DM, Kwon MJ, Kim JH, Kim J-H, Wee JH, Choi HG. Depression, Stress, and Suicide in Korean Adults before and during the COVID-19 Pandemic Using Data from the Korea National Health and Nutritional Examination Survey. Journal of Personalized Medicine. 2022; 12(8):1305. https://doi.org/10.3390/jpm12081305
Chicago/Turabian StyleKim, So Young, Dae Myoung Yoo, Mi Jung Kwon, Ji Hee Kim, Joo-Hee Kim, Jee Hye Wee, and Hyo Geun Choi. 2022. "Depression, Stress, and Suicide in Korean Adults before and during the COVID-19 Pandemic Using Data from the Korea National Health and Nutritional Examination Survey" Journal of Personalized Medicine 12, no. 8: 1305. https://doi.org/10.3390/jpm12081305