
Demographic Patterns of MS Patients Using BRISA: An MS-Specific App in Germany



Abstract
:1. Introduction
2. Methods
2.1. Data Source
2.2. Study Participants
- -
- Answered at least one onboarding question or provided information for at least one parameter analyzed in this study.
- -
- Consent for health data usage for scientific purposes.
2.3. Data Collection
- -
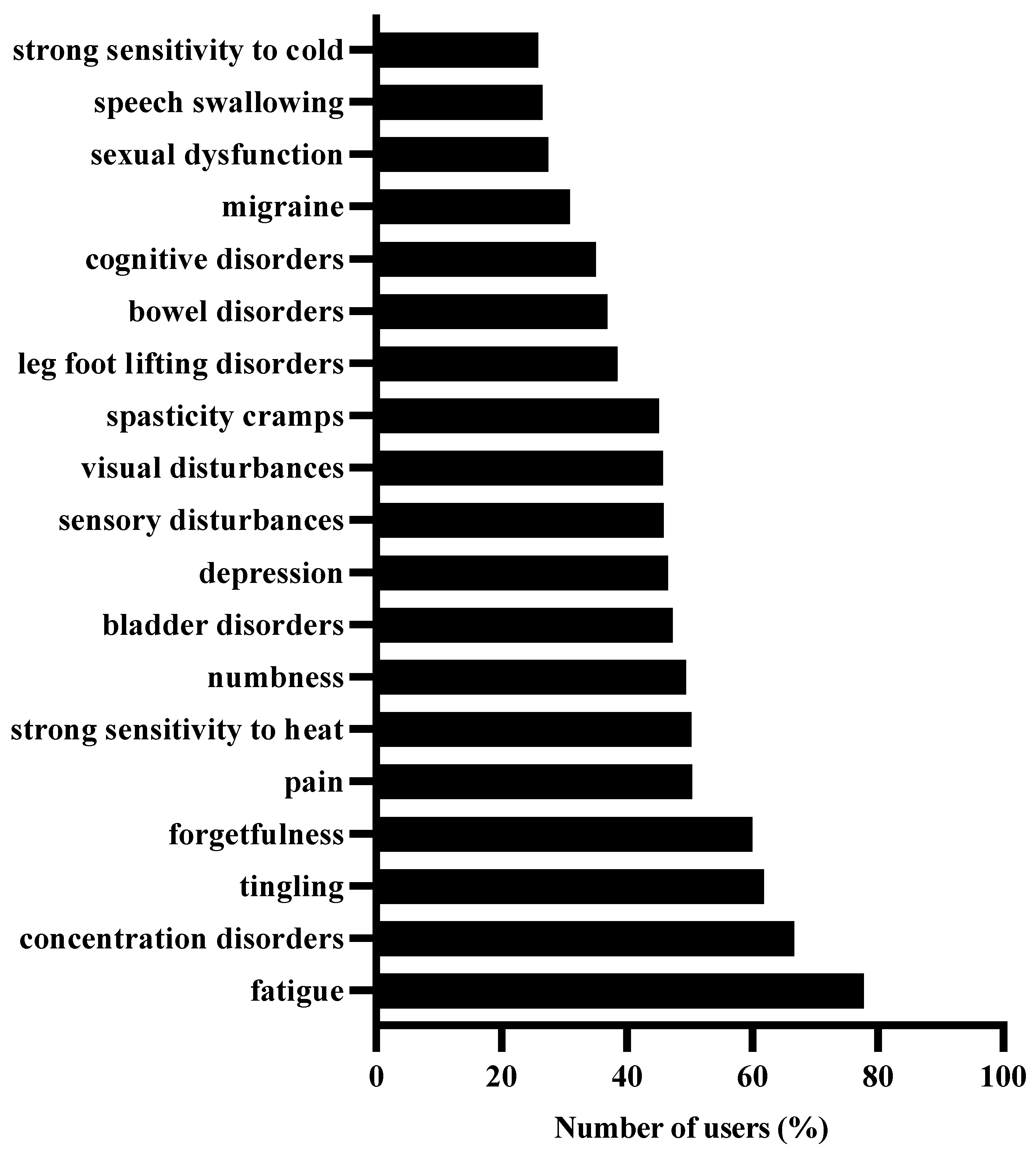
- Strong sensitivity to cold, strong sensitivity to heat, speech swallowing, sexual dysfunction, migraine, cognitive disorders, concentration disorders, bowel disorders, bladder disorders, leg foot lifting disorders, spasticity cramps, visual disturbances, sensory disturbances, depression, numbness, pain, forgetfulness, tingling, fatigue.
2.4. Data Processing and Analysis
2.4.1. Part 1: Demographic Characteristics of BRISA Users
- -
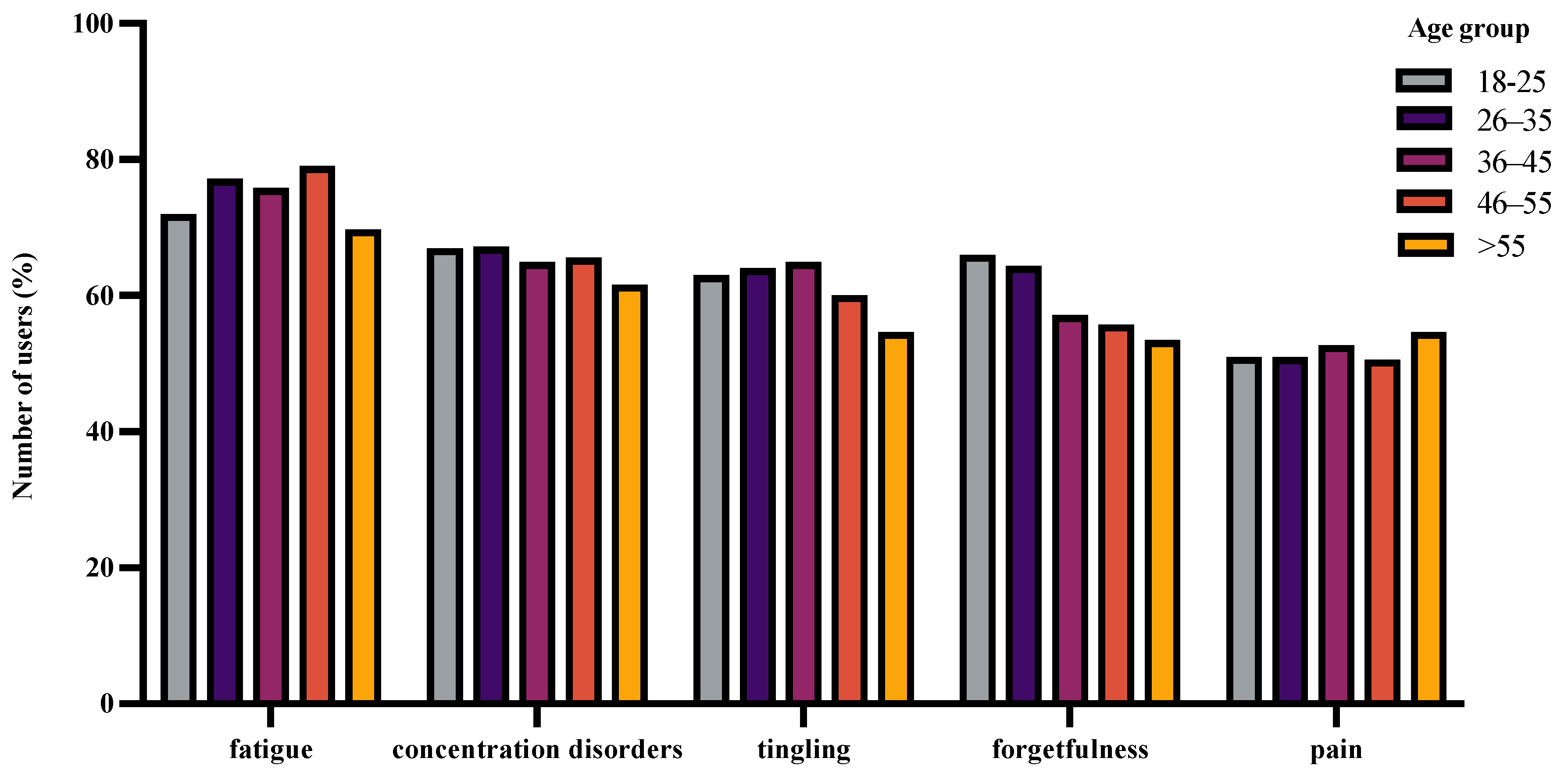
- Age was calculated using the year of birth. For all age-related analysis, users between the ages of 18 and 85 were considered. They were further classified into 5 subgroups based on age: 18–25, 26–35, 36–45, 46–55, and >55 years.
- -
- To study sex-based age distribution, users who answered both parameters were included. This applies to all cases throughout the study, where two or more parameters were involved, unless mentioned otherwise.
- -
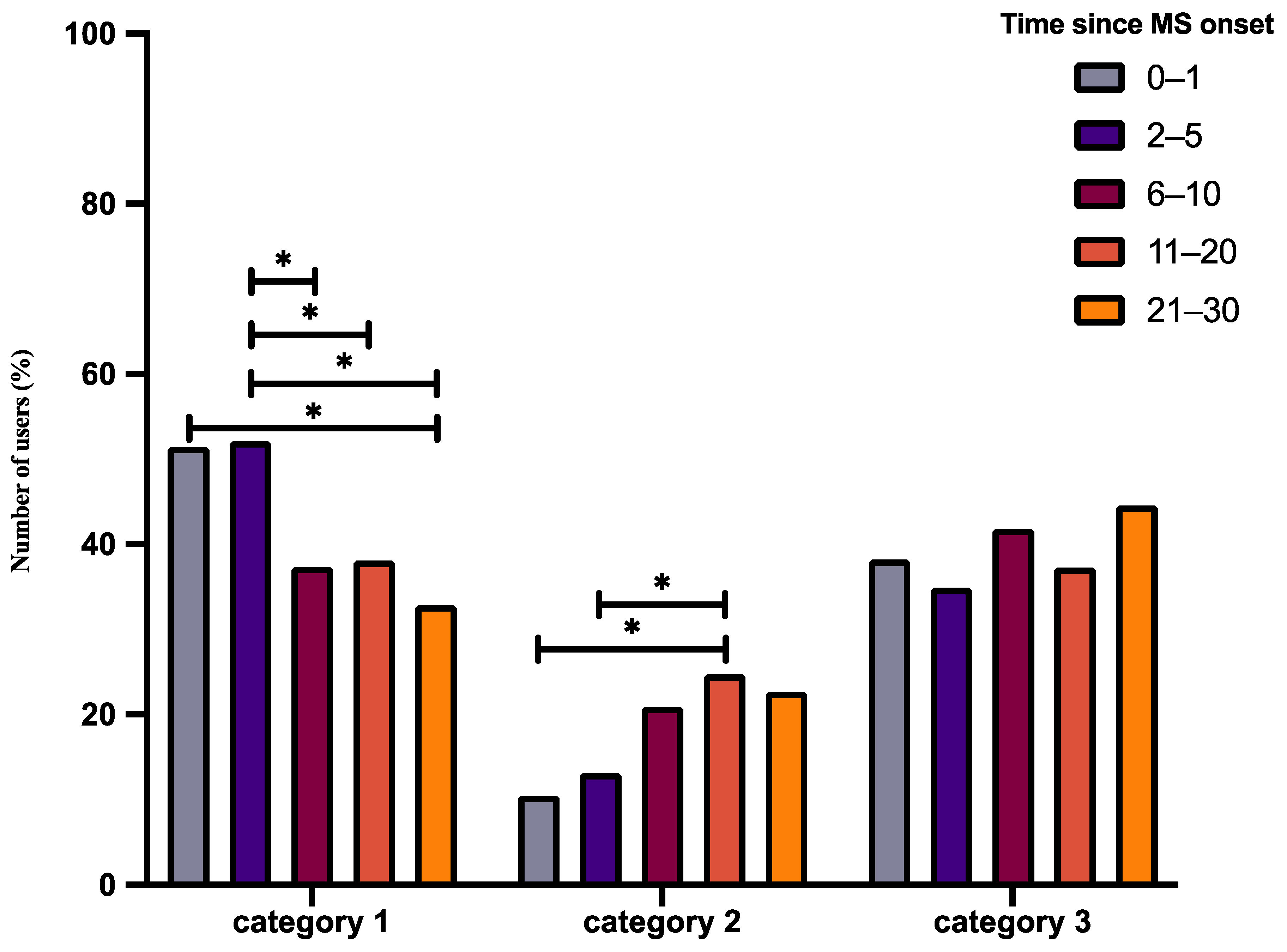
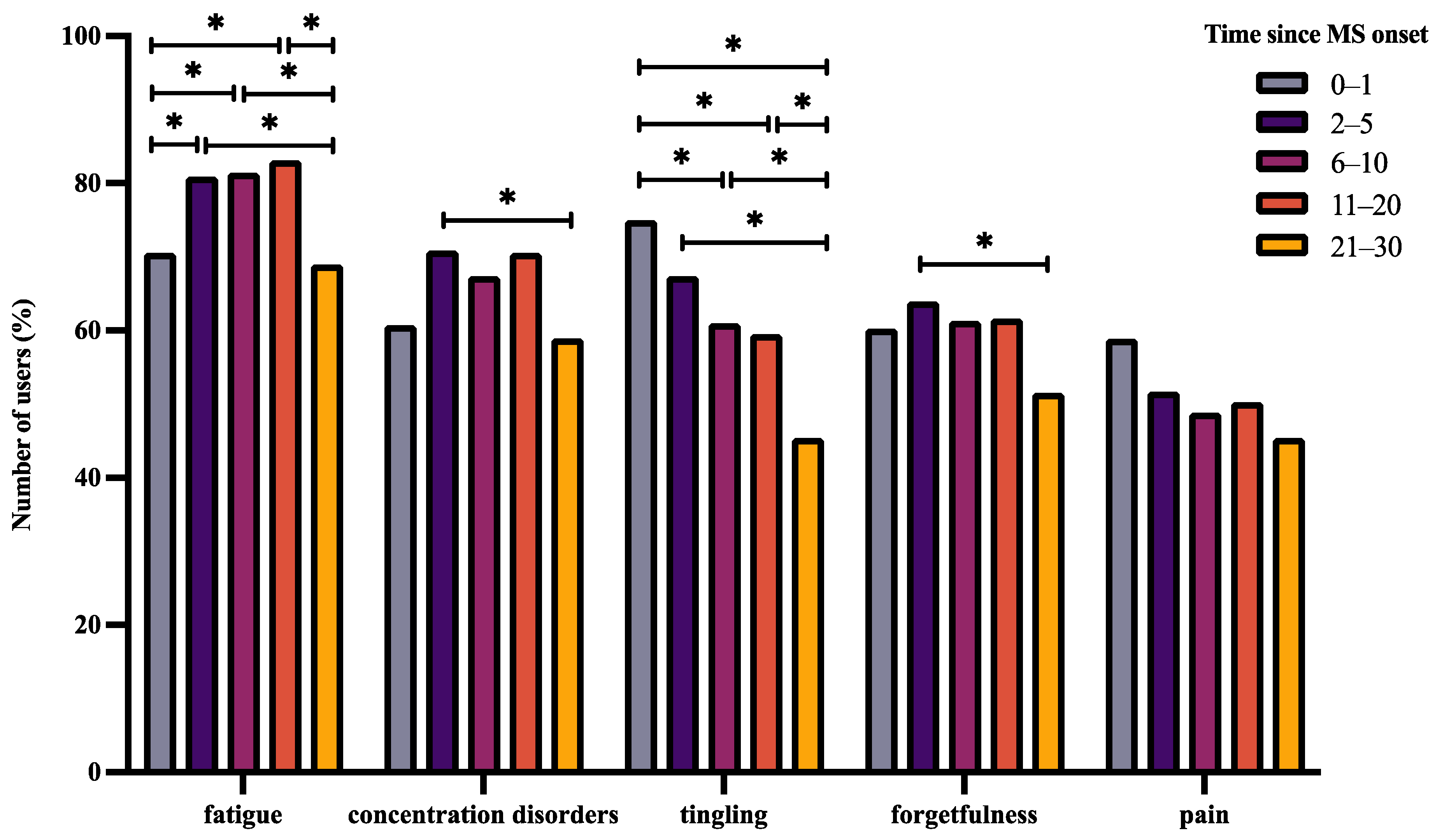
- Time since diagnosis was computed using the year of diagnosis. All entries up to 30 years since diagnosis were considered for analysis. Based on the years since diagnosis, users were further grouped into 5 categories: 0–1 year, 2–5 years, 6–10 years, 11–20 years, and 21–30 years.
- -
2.4.2. Part 2: Symptoms of Concern of BRISA Users
2.5. Statistical Methodology
3. Results
3.1. Demographic Characteristics of Users
3.1.1. Demographic Characteristics
3.1.2. Medications Used
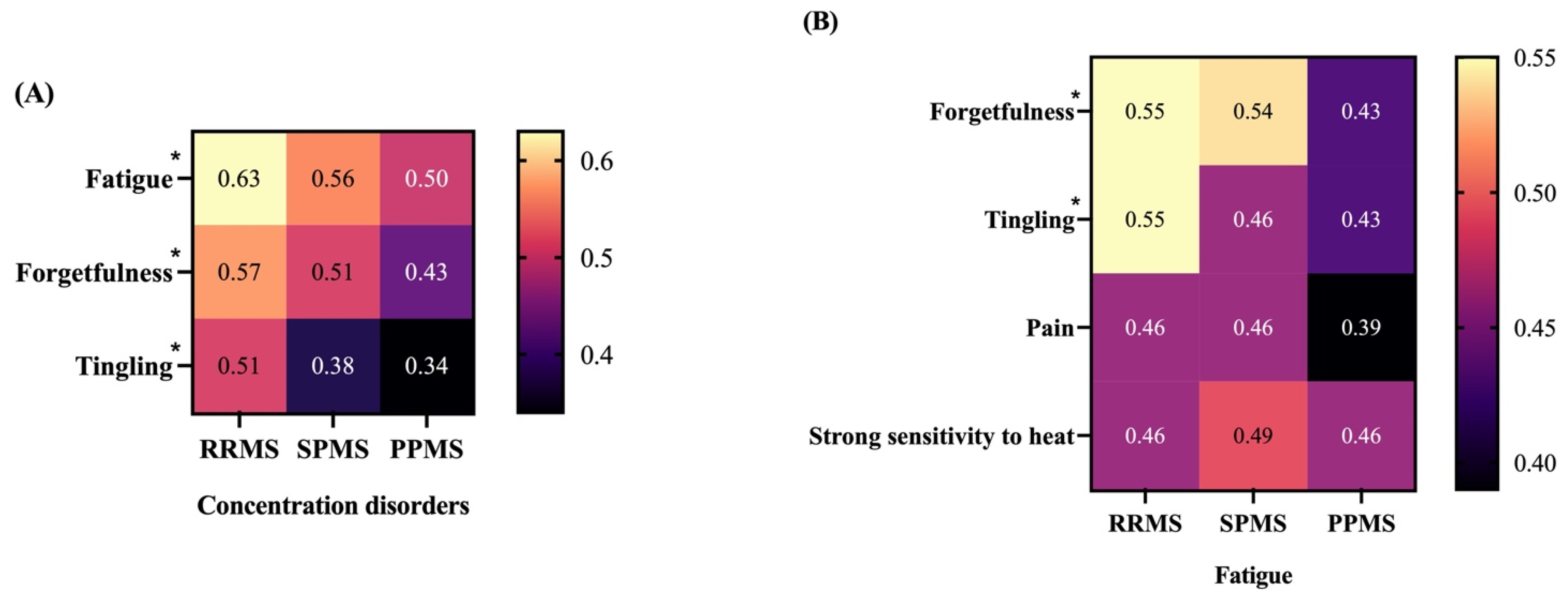
3.2. Symptoms That Concern BRISA Users
4. Discussion
4.1. Demographic Characteristics of BRISA Users
4.1.1. Demographic Characteristics
4.1.2. Medication
4.2. Symptoms That Affect BRISA Users
5. Limitations
6. Conclusions and Outlook
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hauser, S.L.; Cree, B.A.C. Treatment of Multiple Sclerosis: A Review. Am. J. Med. 2020, 133, 1380–1390. [Google Scholar] [CrossRef] [PubMed]
- Dillenseger, A.; Weidemann, M.L.; Trentzsch, K.; Inojosa, H.; Haase, R.; Schriefer, D.; Voigt, I.; Scholz, M.; Akgün, K.; Ziemssen, T. Digital Biomarkers in Multiple Sclerosis. Brain Sci. 2021, 11, 1519. [Google Scholar] [CrossRef] [PubMed]
- Browne, P.; Chandraratna, D.; Angood, C.; Tremlett, H.; Baker, C.; Taylor, B.V.; Thompson, A.J. Atlas of Multiple Sclerosis 2013: A growing global problem with widespread inequity. Neurology 2014, 83, 1022–1024. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walton, C.; King, R.; Rechtman, L.; Kaye, W.; Leray, E.; Marrie, R.A.; Robertson, N.; La Rocca, N.; Uitdehaag, B.; Van Der Mei, I.; et al. Rising prevalence of multiple sclerosis worldwide: Insights from the Atlas of MS, third edition. Mult. Scler. J. 2020, 26, 1816–1821. [Google Scholar] [CrossRef]
- Hemmer, B. Diagnose und Therapie der Multiplen Sklerose, Neuromyelitis-optica- Spektrum-Erkrankungen und MOG-IgG-assoziierten Erkrankungen, S2k-Leitlinie. Available online: https://dgn.org/wp-content/uploads/2021/04/030050_LL-Report_Multiple_Sklerose_2021.pdf (accessed on 15 March 2022).
- Garg, N.; Smith, T.W. An update on immunopathogenesis, diagnosis, and treatment of multiple sclerosis. Brain Behav. 2015, 5, e00362. [Google Scholar] [CrossRef]
- Sebastian, P.; Cherbuin, N.; Barcellos, L.F.; Roalstad, S.; Casper, C.; Hart, J.; Aaen, G.S.; Krupp, L.; Benson, L.; Gorman, M.; et al. Association Between Time Spent Outdoors and Risk of Multiple Sclerosis. Neurology 2021, 98, 267–278. [Google Scholar] [CrossRef]
- Hart, F.M.; Bainbridge, J. Cost-Effectiveness of Disease- Modifying Therapies in Multiple Sclerosis: A Managed Care Perspective. Suppl. Featured Publ. 2016, 22. [Google Scholar]
- Schriefer, D.; Haase, R.; Ettle, B.; Ziemssen, T. Patient- versus physician-reported relapses in multiple sclerosis: Insights from a large observational study. Eur. J. Neurol. 2020, 27, 2531–2538. [Google Scholar] [CrossRef]
- Multiple scleorsis in Europe. Available online: https://emsp.org/wp-content/uploads/2021/06/MS-in-EU-access.pdf (accessed on 15 March 2022).
- Scholz, M.; Haase, R.; Schriefer, D.; Voigt, I.; Ziemssen, T. Electronic Health Interventions in the Case of Multiple Sclerosis: From Theory to Practice. Brain Sci. 2021, 11, 180. [Google Scholar] [CrossRef]
- Haase, R.; Voigt, I.; Scholz, M.; Schlieter, H.; Benedict, M.; Susky, M.; Dillenseger, A.; Ziemssen, T. Profiles of eHealth Adoption in Persons with Multiple Sclerosis and Their Caregivers. Brain Sci. 2021, 11, 1087. [Google Scholar] [CrossRef]
- Mokry, C.; Warnke, C.; Gehring, K.; Hegen, H.; Salmen, A.; Kraemer, M.; Kleiter, I.; Fasshauer, E.; Scheiderbauer, J.; Lühmann, D.; et al. Implementation study of the 2021 German guideline for diagnosis and treatment of multiple sclerosis. Mult. Scler. Relat. Disord. 2022, 57, 103434. [Google Scholar] [CrossRef]
- Daltrozzo, T.; Hapfelmeier, A.; Donnachie, E.; Schneider, A.; Hemmer, B. A Systematic Assessment of Prevalence, Incidence and Regional Distribution of Multiple Sclerosis in Bavaria From 2006 to 2015. Front. Neurol. 2018, 9, 871. [Google Scholar] [CrossRef]
- von Bismarck, O.; Dankowski, T.; Ambrosius, B.; Hessler, N.; Antony, G.; Ziegler, A.; Hoshi, M.-M.; Aly, L.; Luessi, F.; Groppa, S.; et al. Treatment choices and neuropsychological symptoms of a large cohort of early MS. Neurol. Neuroimmunol. Neuroinflamm. 2018, 5, e446. [Google Scholar] [CrossRef] [Green Version]
- Miclea, A.; Salmen, A.; Zoehner, G.; Diem, L.; Kamm, C.P.; Chaloulos-Iakovidis, P.; Miclea, M.; Briner, M.; Kilidireas, K.; Stefanis, L.; et al. Age-dependent variation of female preponderance across different phenotypes of multiple sclerosis: A retrospective cross-sectional study. CNS Neurosci. Ther. 2019, 25, 527–531. [Google Scholar] [CrossRef] [Green Version]
- The MS Registry—MS-Register. Available online: https://www.msregister.de/en/ms-register/das-ms-register/ (accessed on 2 March 2022).
- Ohle, L.-M.; Ellenberger, D.; Flachenecker, P.; Friede, T.; Haas, J.; Hellwig, K.; Parciak, T.; Warnke, C.; Paul, F.; Zettl, U.K.; et al. Chances and challenges of a long-term data repository in multiple sclerosis: 20th birthday of the German MS registry. Sci. Rep. 2021, 11, 13340. [Google Scholar] [CrossRef]
- Bol, N.; Helberger, N.; Weert, J.C.M. Differences in mobile health app use: A source of new digital inequalities? Inf. Soc. 2018, 34, 183–193. [Google Scholar] [CrossRef] [Green Version]
- Haase, R.; Schultheiss, T.; Kempcke, R.; Thomas, K.; Ziemssen, T. Modern communication technology skills of patients with multiple sclerosis. Mult. Scler. 2013, 19, 1240–1241. [Google Scholar] [CrossRef]
- Bidmon, S.; Terlutter, R. Gender Differences in Searching for Health Information on the Internet and the Virtual Patient-Physician Relationship in Germany: Exploratory Results on How Men and Women Differ and Why. J. Med. Internet Res. 2015, 17, e156. [Google Scholar] [CrossRef]
- Wiendl, H.; Gold, R.; Berger, T.; Derfuss, T.; Linker, R.; Mäurer, M.; Aktas, O.; Baum, K.; Berghoff, M.; Bittner, S.; et al. Multiple Sclerosis Therapy Consensus Group (MSTCG): Position statement on disease-modifying therapies for multiple sclerosis (white paper). Ther. Adv. Neurol. Disord. 2021, 14, 17562864211039648. [Google Scholar] [CrossRef]
- He, A.; Merkel, B.; Brown, J.W.L.; Ryerson, L.Z.; Kister, I.; Malpas, C.B.; Sharmin, S.; Horakova, D.; Havrdova, E.K.; Spelman, T.; et al. Timing of high-efficacy therapy for multiple sclerosis: A retrospective observational cohort study. Lancet Neurol. 2020, 19, 307–316. [Google Scholar] [CrossRef]
- Simpson, A.; Mowry, E.M.; Newsome, S.D. Early Aggressive Treatment Approaches for Multiple Sclerosis. Curr. Treat Options Neurol. 2021, 23, 19. [Google Scholar] [CrossRef]
- Harding, K.; Williams, O.; Willis, M.; Hrastelj, J.; Rimmer, A.; Joseph, F.; Tomassini, V.; Wardle, M.; Pickersgill, T.; Robertson, N.; et al. Clinical Outcomes of Escalation vs Early Intensive Disease-Modifying Therapy in Patients With Multiple Sclerosis. JAMA Neurol. 2019, 76, 536–541. [Google Scholar] [CrossRef]
- Giovannoni, G.; Kappos, L.; de Seze, J.; Hauser, S.L.; Overell, J.; Koendgen, H.; Manfrini, M.; Wang, Q.; Wolinsky, J.S. Risk of requiring a walking aid after 6.5 years of ocrelizumab treatment in patients with relapsing multiple sclerosis: Data from the OPERA I and OPERA II trials. Eur. J. Neurol. 2022, 29, 1238–1242. [Google Scholar] [CrossRef]
- Engmann, N.J.; Sheinson, D.; Bawa, K.; Ng, C.D.; Pardo, G. Persistence and adherence to ocrelizumab compared with other disease-modifying therapies for multiple sclerosis in U.S. commercial claims data. JMCP 2021, 27, 639–649. [Google Scholar] [CrossRef]
- Liu, Z.; Liao, Q.; Wen, H.; Zhang, Y. Disease modifying therapies in relapsing-remitting multiple sclerosis: A systematic review and network meta-analysis. Autoimmun. Rev. 2021, 20, 102826. [Google Scholar] [CrossRef]
- Hauser, S.L.; Bar-Or, A.; Cohen, J.A.; Comi, G.; Correale, J.; Coyle, P.K.; Cross, A.H.; de Seze, J.; Leppert, D.; Montalban, X.; et al. Ofatumumab versus Teriflunomide in Multiple Sclerosis. N. Engl. J. Med. 2020, 383, 546–557. [Google Scholar] [CrossRef]
- Hauser, S.L.; Kappos, L.; Arnold, D.L.; Bar-Or, A.; Brochet, B.; Naismith, R.T.; Traboulsee, A.; Wolinsky, J.S.; Belachew, S.; Koendgen, H.; et al. Five years of ocrelizumab in relapsing multiple sclerosis. Neurology 2020, 95, e1854–e1867. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Z.; Lv, Y.; Gu, Z.-C.; Ma, C.-L.; Zhong, M.-K. Risk for Cardiovascular Adverse Events Associated With Sphingosine-1-Phosphate Receptor Modulators in Patients With Multiple Sclerosis: Insights From a Pooled Analysis of 15 Randomised Controlled Trials. Front. Immunol. 2021, 12, 795574. [Google Scholar] [CrossRef] [PubMed]
- Sorensen, P.S.; Sellebjerg, F. Pulsed immune reconstitution therapy in multiple sclerosis. Ther. Adv. Neurol. Disord. 2019, 12, 1756286419836913. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghasemi, N.; Razavi, S.; Nikzad, E. Multiple Sclerosis: Pathogenesis, Symptoms, Diagnoses and Cell-Based Therapy. Cell J. 2017, 19, 1. [Google Scholar] [PubMed]
- Lerdal, A.; Gulowsen Celius, E.; Krupp, L.; Dahl, A.A. A prospective study of patterns of fatigue in multiple sclerosis: Patterns of fatigue in multiple sclerosis. Eur. J. Neurol. 2007, 14, 1338–1343. [Google Scholar] [CrossRef] [Green Version]
- Scherder, R.J.; Kant, N.; Wolf, E.T.; Pijnenburg, B.C.M.; Scherder, E.J.A. Sensory Function and Chronic Pain in Multiple Sclerosis. Pain Res. Manag. 2018, 2018, 1924174. [Google Scholar] [CrossRef]
- Silveira, C.; Guedes, R.; Maia, D.; Curral, R.; Coelho, R. Neuropsychiatric Symptoms of Multiple Sclerosis: State of the Art. Psychiatry Investig. 2019, 16, 877–888. [Google Scholar] [CrossRef]
- Kalb, R.; Beier, M.; Benedict, R.H.; Charvet, L.; Costello, K.; Feinstein, A.; Gingold, J.; Goverover, Y.; Halper, J.; Harris, C.; et al. Recommendations for cognitive screening and management in multiple sclerosis care. Mult. Scler. 2018, 24, 1665–1680. [Google Scholar] [CrossRef] [Green Version]
- Nazareth, T.A.; Rava, A.R.; Polyakov, J.L.; Banfe, E.N.; Ii, R.W.W.; Zerkowski, K.B.; Herbert, L.B. Relapse prevalence, symptoms, and health care engagement: Patient insights from the Multiple Sclerosis in America 2017 survey. Mult. Scler. Relat. Disord. 2018, 26, 219–234. [Google Scholar] [CrossRef] [Green Version]
- Braley, T.J.; Chervin, R.D. Fatigue in Multiple Sclerosis: Mechanisms, Evaluation, and Treatment. Sleep 2010, 33, 1061–1067. [Google Scholar] [CrossRef]
- Numbness or Tingling. National Multiple Sclerosis Society n.d. Available online: https://www.nationalmssociety.org/Symptoms-Diagnosis/MS-Symptoms/Numbness (accessed on 4 March 2022).
- Joy, J.E.; Richard, B.; Johnston, J. Multiple Sclerosis: Current Status and Strategies for the Future; National Academies Press (US): Washington, DC, USA, 2001. [Google Scholar]
- Korakas, N.; Tsolaki, M. Cognitive Impairment in Multiple Sclerosis: A Review of Neuropsychological Assessments. Cogn. Behav. Neurol. 2016, 29, 55–67. [Google Scholar] [CrossRef]
- Silveira, S.L.; Cederberg, K.L.J.; Jeng, B.; Sikes, E.M.; Sandroff, B.M.; Jones, C.D.; Motl, R.W. Symptom clusters and quality of life in persons with multiple sclerosis across the lifespan. Qual. Life Res. 2021, 30, 1061–1071. [Google Scholar] [CrossRef]
- Shahrbanian, S.; Duquette, P.; Kuspinar, A.; Mayo, N.E. Contribution of symptom clusters to multiple sclerosis consequences. Qual. Life Res. 2015, 24, 617–629. [Google Scholar] [CrossRef]
- Symptoms and Association with Health Outcomes in Relapsing-Remitting Multiple Sclerosis: Results of a US Patient Survey n.d. Available online: https://www.hindawi.com/journals/msi/2014/203183/ (accessed on 4 March 2022).
- Flensner, G.; Ek, A.-C.; Söderhamn, O.; Landtblom, A.-M. Sensitivity to heat in MS patients: A factor strongly influencing symptomology—An explorative survey. BMC Neurol. 2011, 11, 27. [Google Scholar] [CrossRef] [Green Version]
- Learmonth, Y.C.; Motl, R.W.; Sandroff, B.M.; Pula, J.H.; Cadavid, D. Validation of patient determined disease steps (PDDS) scale scores in persons with multiple sclerosis. BMC Neurol. 2013, 13, 37. [Google Scholar] [CrossRef] [Green Version]
- Multiple Sclerosis Quality of Life Inventory (MSQLI). National Multiple Sclerosis Society n.d. Available online: https://www.nationalmssociety.org/For-Professionals/Researchers/Resources-for-MS-Researchers/Research-Tools/Clinical-Study-Measures/Multiple-Sclerosis-Quality-of-Life-Inventory-(MSQL (accessed on 2 May 2022).







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Efficacy Category | Medication |
|---|---|
| Category 1 | dimethyl fumarate, diroximel fumarate, interferon-beta, glatiramer acetate, and teriflunomide |
| Category 2 | cladribine, spingosine-1-phosphate receptor modulators |
| Category 3 | monoclonal antibodies |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Balakrishnan, P.; Groenberg, J.; Jacyshyn-Owen, E.; Eberl, M.; Friedrich, B.; Joschko, N.; Ziemssen, T. Demographic Patterns of MS Patients Using BRISA: An MS-Specific App in Germany. J. Pers. Med. 2022, 12, 1100. https://doi.org/10.3390/jpm12071100
Balakrishnan P, Groenberg J, Jacyshyn-Owen E, Eberl M, Friedrich B, Joschko N, Ziemssen T. Demographic Patterns of MS Patients Using BRISA: An MS-Specific App in Germany. Journal of Personalized Medicine. 2022; 12(7):1100. https://doi.org/10.3390/jpm12071100
Chicago/Turabian StyleBalakrishnan, Preetha, Jannis Groenberg, Elizabeth Jacyshyn-Owen, Markus Eberl, Benjamin Friedrich, Natalie Joschko, and Tjalf Ziemssen. 2022. "Demographic Patterns of MS Patients Using BRISA: An MS-Specific App in Germany" Journal of Personalized Medicine 12, no. 7: 1100. https://doi.org/10.3390/jpm12071100