
Neurogenic Bladder Physiology, Pathogenesis, and Management after Spinal Cord Injury

 , and
, and
Abstract
:1. Introduction
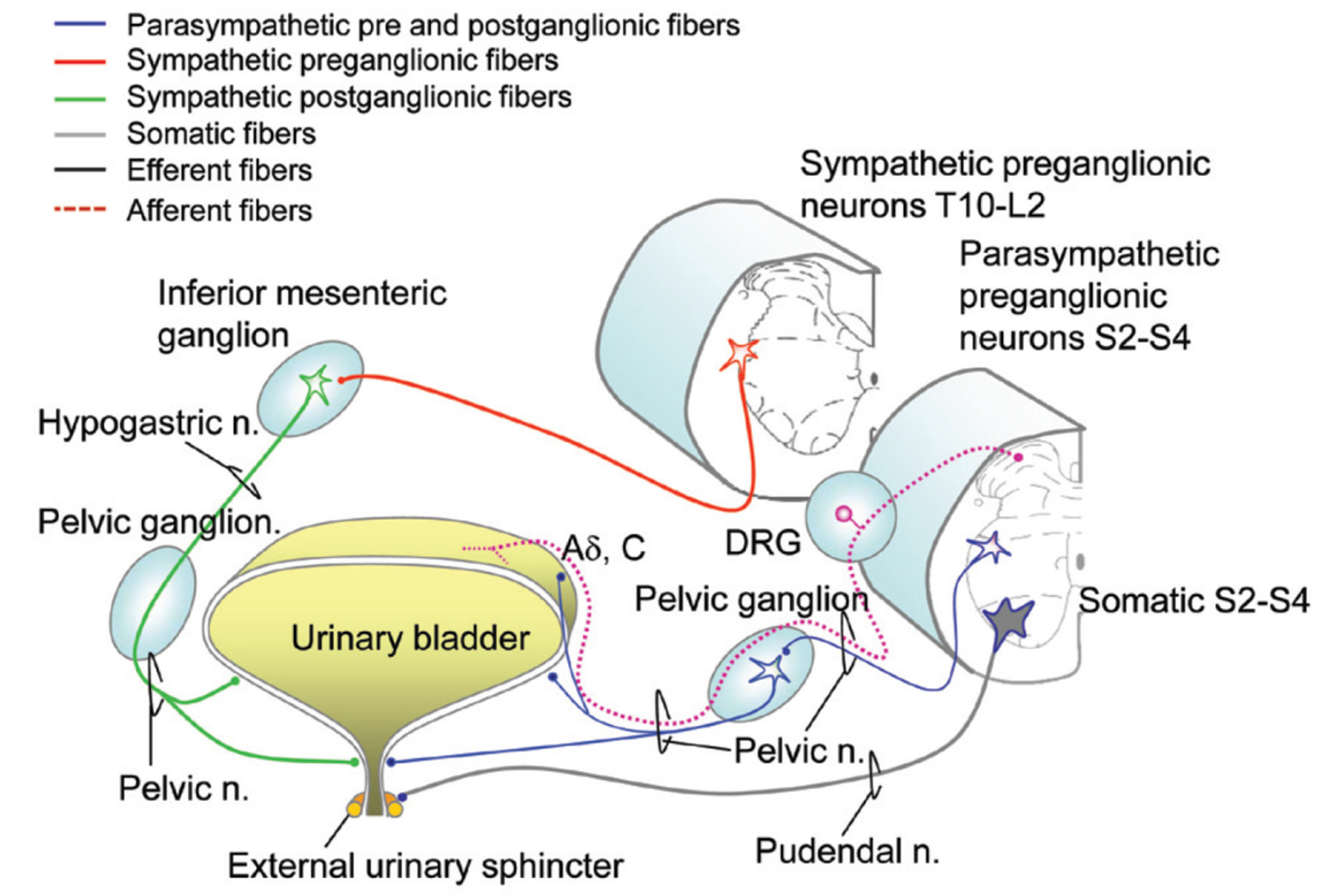
2. Basic Anatomy in the Normal Functioning Urinary Tract
3. Normal Physiology in the Functioning Urinary Tract
3.1. Storage Phase
3.2. Voiding Phase
Spinal Cord Injury
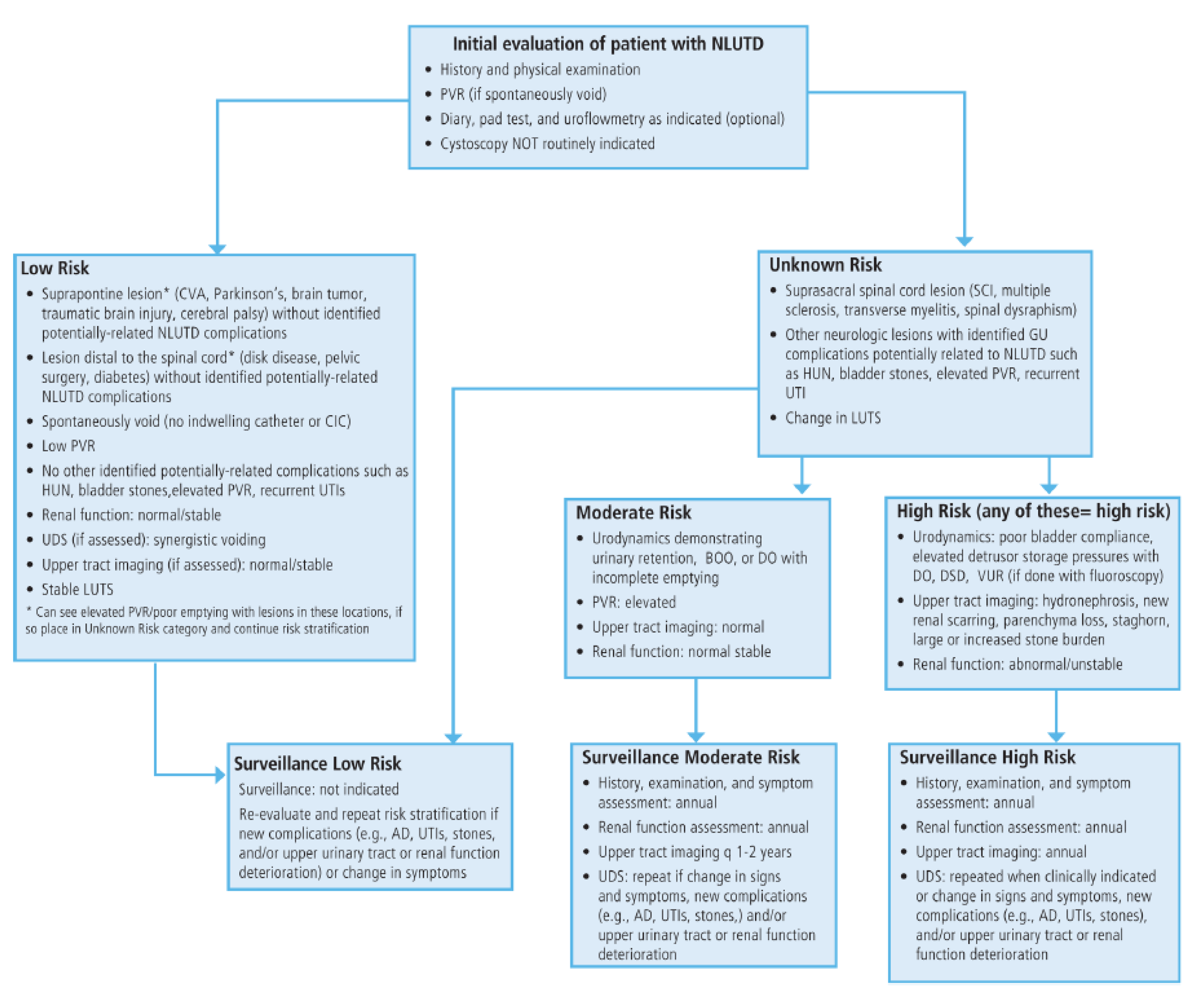
4. Assessment
5. Initial Evaluation History and Physical Examination and Urinalysis
6. Non-Invasive Testing
7. Urinary Tract Infections
8. Upper Tract Imaging
9. Invasive Testing
9.1. Urodynamics
9.2. Cystoscopy
10. Management Goals
10.1. Urinary Catheterization
10.2. Crede, Valsalva
10.3. Reflex Voiding
11. Pharmacological Interventions
11.1. Antimuscarinics
11.2. α1 Adrenergic Antagonists
11.3. Beta 3 Adrenergic Agonist
11.4. Bladder Chemodenervation
12. Surgical Management
12.1. Sphincterotomy/Intraurethral Stents
12.2. Sacral Anterior Root Stimulation (SARS) and Sacral Neuromodulation
12.3. Bladder Augmentation
12.4. Continent Urinary Diversion
12.5. Incontinent Urinary Diversion
13. Surveillance
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Jain, N.B.; Ayers, G.D.; Peterson, E.N.; Harris, M.B.; Morse, L.; O’Connor, K.C.; Garshick, E. Traumatic spinal cord injury in the United States, 1993–2012. JAMA 2015, 313, 2236–2243. [Google Scholar] [CrossRef] [PubMed]
- Spinal Cord Injury (SCI). 2016 Facts and Figures at a Glance. J. Spinal Cord Med. 2016, 39, 493–494. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benarroch, E.E. Physiology and Pathophysiology of the Autonomic Nervous System. Continuum 2020, 26, 12–24. [Google Scholar] [CrossRef]
- Wecht, J.M.; Krassioukov, A.V.; Alexander, M.; Handrakis, J.P.; McKenna, S.L.; Kennelly, M.; Trbovich, M.; Biering-Sorensen, F.; Burns, S.; Elliott, S.L.; et al. International Standards to document Autonomic Function following SCI (ISAFSCI): Second Edition. Top. Spinal Cord Inj. Rehabil. 2021, 27, 23–49. [Google Scholar] [CrossRef] [PubMed]
- Rahman, M.; Siddick, A. Neuroanatomy, Pontine Micturition Center. In StatPearls [Internet]; Updated 9 September 2021; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Stoffel, J.T. Detrusor sphincter dyssynergia: A review of physiology, diagnosis, and treatment strategies. Transl. Androl. Urol. 2016, 5, 127–135. [Google Scholar] [CrossRef]
- Matsuo, T.; Miyata, Y.; Kakoki, K.; Yuzuriha, M.; Asai, A.; Ohba, K.; Sakai, H. The efficacy of mirabegron additional therapy for lower urinary tract symptoms after treatment with α1-adrenergic receptor blocker monotherapy: Prospective analysis of elderly men. BMC Urol. 2016, 16, 45. [Google Scholar] [CrossRef] [Green Version]
- Dodd, W.; Motwani, K.; Small, C.; Pierre, K.; Patel, D.; Malnik, S.; Lucke-Wold, B.; Porche, K. Spinal cord injury and neurogenic lower urinary tract dysfunction: What do we know and where are we going? J. Men’s Health 2022, 18, 6. [Google Scholar] [CrossRef]
- Clark, C.B.; Ragam, R.; Das, A.K.; Shenot, P.J. Management of neurogenic detrusor overactivity. Can. J. Urol. 2021, 28, 33–37. [Google Scholar]
- Lim, V.; Mac-Thiong, J.M.; Dionne, A.; Begin, J.; Richard-Denis, A. Clinical Protocol for Identifying and Managing Bladder Dysfunction during Acute Care after Traumatic Spinal Cord Injury. J. Neurotrauma 2021, 38, 718–724. [Google Scholar] [CrossRef]
- Rupp, R.; Biering-Sørensen, F.; Burns, S.P.; Graves, D.E.; Guest, J.; Jones, L.; Read, M.S.; Rodriguez, G.M.; Schuld, C.; Tansey-MD, K.E.; et al. International Standards for Neurological Classification of Spinal Cord Injury: Revised 2019. Top. Spinal Cord Inj. Rehabil. 2021, 27, 1–22. [Google Scholar] [CrossRef]
- Krassioukov, A.; Linsenmeyer, T.A.; Beck, L.A.; Elliott, S.; Gorman, P.; Kirshblum, S.; Vogel, L.; Wecht, J.; Clay, S. Evaluation and Management of Autonomic Dysreflexia and Other Autonomic Dysfunctions: Preventing the Highs and Lows: Management of Blood Pressure, Sweating, and Temperature Dysfunction. Top. Spinal Cord Inj. Rehabil. 2021, 27, 225–290. [Google Scholar] [CrossRef] [PubMed]
- Eschlböck, S.; Wenning, G.; Fanciulli, A. Evidence-based treatment of neurogenic orthostatic hypotension and related symptoms. J. Neural. Transm. 2017, 124, 1567–1605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Linsenmeyer, T.A.; Gibbs, K.; Solinsky, R. Autonomic Dysreflexia After Spinal Cord Injury: Beyond the Basics. Curr. Phys. Med. Rehabil. Rep. 2020, 8, 443–451. [Google Scholar] [CrossRef]
- Ginsberg, D.A.; Boone, T.B.; Cameron, A.P.; Gousse, A.; Kaufman, M.R.; Keays, E.; Kennelly, M.J.; Lemack, G.E.; Rovner, E.S.; Souter, L.H.; et al. The AUA/SUFU Guideline on Adult Neurogenic Lower Urinary Tract Dysfunction: Diagnosis and Evaluation. J. Urol. 2021, 206, 1097–1105. [Google Scholar] [CrossRef] [PubMed]
- Ginsberg, D.A.; Boone, T.B.; Cameron, A.P.; Gousse, A.; Kaufman, M.R.; Keays, E.; Kennelly, M.J.; Lemack, G.E.; Rovner, E.S.; Souter, L.H.; et al. The AUA/SUFU Guideline on Adult Neurogenic Lower Urinary Tract Dysfunction: Treatment and Follow-up. J. Urol. 2021, 206, 1106–1113. [Google Scholar] [CrossRef]
- Kreydin, E.; Welk, B.; Chung, D.; Clemens, Q.; Yang, C.; Danforth, T.; Gousse, A.; Kielb, S.; Kraus, S.; Mangera, A.; et al. Surveillance and management of urologic complications after spinal cord injury. World J. Urol. 2018, 36, 1545–1553. [Google Scholar] [CrossRef]
- Goetz, L.L.; Cardenas, D.D.; Kennelly, M.; Bonne Lee, B.S.; Linsenmeyer, T.; Moser, C.; Pannek, J.; Wyndaele, J.J.; Biering-Sorensen, F. International Spinal Cord Injury Urinary Tract Infection Basic Data Set. Spinal Cord 2013, 51, 700–704. [Google Scholar] [CrossRef] [Green Version]
- Nicolle, L.E.; Bradley, S.; Colgan, R.; Rice, J.C.; Schaeffer, A.; Hooton, T.M. Infectious Diseases Society of America Guidelines for the Diagnosis and Treatment of Asymptomatic Bacteriuria in Adults. Clin. Infect. Dis. 2005, 40, 643–654. [Google Scholar] [CrossRef]
- Chew, A.B.; Suda, K.J.; Patel, U.C.; Fitzpatrick, M.A.; Ramanathan, S.; Burns, S.P.; Evans, C.T. Long-term prescribing of nitrofurantoin for urinary tract infections (UTI) in veterans with spinal cord injury (SCI). J. Spinal Cord Med. 2019, 42, 485–493. [Google Scholar] [CrossRef]
- Weld, K.J.; Graney, M.J.; Dmochowski, R.R. Clinical significance of detrusor sphincter dyssynergia type in patients with post-traumatic spinal cord injury. Urology 2000, 56, 565–568. [Google Scholar] [CrossRef]
- Laquerre, J. Hydronephrosis: Diagnosis, Grading, and Treatment. Radiol. Technol. 2020, 92, 135–151. [Google Scholar]
- Panicker, J.N.; Fowler, C.J.; Kessler, T.M. Lower urinary tract dysfunction in the neurological patient: Clinical assessment and management. Lancet Neurol. 2015, 14, 720–732. [Google Scholar] [CrossRef]
- Welk, B.; Schneider, M.P.; Thavaseelan, J.; Traini, L.R.; Curt, A.; Kessler, T.M. Early urological care of patients with spinal cord injury. World J. Urol. 2018, 36, 1537–1544. [Google Scholar] [CrossRef]
- Agrawal, M.; Joshi, M. Urodynamic patterns after traumatic spinal cord injury. J. Spinal Cord Med. 2015, 38, 128–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Groah, S.L.; Weitzenkamp, D.A.; Lammertse, D.P.; Whiteneck, G.G.; Lezotte, D.C.; Hamman, R.F. Excess risk of bladder cancer in spinal cord injury: Evidence for an association between indwelling catheter use and bladder cancer. Arch. Phys. Med. Rehabil. 2002, 83, 346–351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guo, W.B.; Shapiro, K.; Wang, Z.X.; Armann, K.; Shen, B.; Wang, J.C.; Roppolo, J.R.; de Groat, W.C.; Tai, C.F. Restoring both continence and micturition after chronic spinal cord injury by pudendal neuromodulation. Exp. Neurol. 2021, 340, 10. [Google Scholar] [CrossRef]
- Cameron, A.P.; Wallner, L.P.; Tate, D.G.; Sarma, A.V.; Rodriguez, G.M.; Clemens, J.Q. Bladder management after spinal cord injury in the United States 1972 to 2005. J. Urol. 2010, 184, 213–217. [Google Scholar] [CrossRef]
- Ismail, S.; Karsenty, G.; Chartier-Kastler, E.; Cussenot, O.; Compérat, E.; Rouprêt, M.; Phé, V. Prevalence, management, and prognosis of bladder cancer in patients with neurogenic bladder: A systematic review. Neurourol. Urodyn. 2018, 37, 1386–1395. [Google Scholar] [CrossRef]
- Kinnear, N.; Barnett, D.; O’Callaghan, M.; Horsell, K.; Gani, J.; Hennessey, D. The impact of catheter-based bladder drainage method on urinary tract infection risk in spinal cord injury and neurogenic bladder: A systematic review. Neurourol. Urodyn. 2020, 39, 854–862. [Google Scholar] [CrossRef]
- English, S.F. Update on voiding dysfunction managed with suprapubic catheterization. Transl. Androl. Urol. 2017, 6, S180–S185. [Google Scholar] [CrossRef] [Green Version]
- Lloyd, L.K.; Kuhlemeier, K.V.; Fine, P.R.; Stover, S.L. Initial bladder management in spinal cord injury: Does it make a difference? J. Urol. 1986, 135, 523–527. [Google Scholar] [CrossRef]
- Joshi, A.D.; Shukla, A.; Chawathe, V.; Gaur, A.K. Clean intermittent catheterization in long-term management of neurogenic bladder in spinal cord injury: Patient perspective and experiences. Int. J. Urol. 2022, 19, 317–323. [Google Scholar] [CrossRef] [PubMed]
- Hunter, K.F.; Bharmal, A.; Moore, K.N. Long-term bladder drainage: Suprapubic catheter versus other methods: A scoping review. Neurourol. Urodyn. 2013, 32, 944–951. [Google Scholar] [CrossRef] [PubMed]
- Romo, P.G.B.; Smith, C.P.; Cox, A.; Averbeck, M.A.; Dowling, C.; Beckford, C.; Manohar, P.; Duran, S.; Cameron, A.P. Non-surgical urologic management of neurogenic bladder after spinal cord injury. World J. Urol. 2018, 36, 1555–1568. [Google Scholar] [CrossRef] [PubMed]
- Greenstein, A.; Rucker, K.S.; Katz, P.G. Voiding by increased abdominal pressure in male spinal cord injury patients--long term follow up. Paraplegia 1992, 30, 253–255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cardenas, D.D.; Kelly, E.; Mayo, M.E. Manual stimulation of reflex voiding after spinal cord injury. Arch. Phys. Med. Rehabil. 1985, 66, 459–462. [Google Scholar]
- Madersbacher, H.; Mürtz, G.; Stöhrer, M. Neurogenic detrusor overactivity in adults: A review on efficacy, tolerability and safety of oral antimuscarinics. Spinal Cord 2013, 51, 432–441. [Google Scholar] [CrossRef]
- Madhuvrata, P.; Singh, M.; Hasafa, Z.; Abdel-Fattah, M. Anticholinergic Drugs for Adult Neurogenic Detrusor Overactivity: A Systematic Review and Meta-analysis. Eur. Urol. 2012, 62, 816–830. [Google Scholar] [CrossRef]
- Abrams, P.; Amarenco, G.; Bakke, A.; Buczyński, A.; Castro-Diaz, D.; Harrison, S.; Kramer, G.; Marsik, R.; Prajsner, A.; Stöhrer, M.; et al. Tamsulosin: Efficacy and safety in patients with neurogenic lower urinary tract dysfunction due to suprasacral spinal cord injury. J. Urol. 2003, 170, 1242–1251. [Google Scholar] [CrossRef]
- Perkash, I. Efficacy and safety of terazosin to improve voiding in spinal cord injury patients. J. Spinal Cord Med. 1995, 18, 236–239. [Google Scholar] [CrossRef]
- Suarez, O.; Osborn, D.; Kaufman, M.; Reynolds, W.S.; Dmochowski, R. Mirabegron for male lower urinary tract symptoms. Curr. Urol. Rep. 2013, 14, 580–584. [Google Scholar] [CrossRef] [PubMed]
- Trbovich, M.; Romo, T.; Polk, M.; Koek, W.; Kelly, C.; Stowe, S.; Kraus, S.; Kellogg, D. The treatment of neurogenic lower urinary tract dysfunction in persons with spinal cord injury: An open label, pilot study of anticholinergic agent vs. mirabegron to evaluate cognitive impact and efficacy. Spinal Cord Ser. Cases 2021, 7, 10. [Google Scholar] [CrossRef] [PubMed]
- Vasudeva, P.; Prasad, V.; Yadav, S.; Kumar, N.; Saurav, K.; Prashanth, Y.M.; Tyagi, V. Efficacy and safety of mirabegron for the treatment of neurogenic detrusor overactivity resulting from traumatic spinal cord injury: A prospective study. Neurourol. Urodyn. 2021, 40, 666–671. [Google Scholar] [CrossRef]
- Wöllner, J.; Pannek, J. Initial experience with the treatment of neurogenic detrusor overactivity with a new β-3 agonist (mirabegron) in patients with spinal cord injury. Spinal Cord 2016, 54, 78–82. [Google Scholar] [CrossRef]
- Mitcheson, H.D.; Samanta, S.; Muldowney, K.; Pinto, C.A.; Rocha, B.A.; Green, S.; Bennett, N.; Mudd, P.N., Jr.; Frenkl, T.L. Vibegron (RVT-901/MK-4618/KRP-114V) Administered Once Daily as Monotherapy or Concomitantly with Tolterodine in Patients with an Overactive Bladder: A Multicenter, Phase IIb, Randomized, Double-blind, Controlled Trial. Eur. Urol. 2019, 75, 274–282. [Google Scholar] [CrossRef]
- Aoki, K.; Momose, H.; Gotoh, D.; Morizawa, Y.; Hori, S.; Nakai, Y.; Miyake, M.; Anai, S.; Torimoto, K.; Tanaka, N.; et al. Video-urodynamic effects of vibegron, a new selective β3-adrenoceptor agonist, on antimuscarinic-resistant neurogenic bladder dysfunction in patients with spina bifida. Int. J. Urol. 2022, 29, 76–81. [Google Scholar] [CrossRef]
- Tamburro, F.R.; Castellan, P.; Neri, F.; Berardinelli, F.; Bada, M.; Sountoulides, P.; Giuliani, N.; Finazzi Agrò, E.; Schips, L.; Cindolo, L. Onabotulinumtoxin-A improves health status and urinary symptoms in subjects with refractory overactive bladder: Real-life experience. Urologia 2018, 85, 163–168. [Google Scholar] [CrossRef]
- Palazon-Garcia, R.; Alcobendas-Maestro, M.; Esclarin-de Ruz, A.; Benavente-Vaidepenas, A.M. Treatment of spasticity in spinal cord injury with botulinum toxin. J. Spinal Cord Med. 2019, 42, 281–287. [Google Scholar] [CrossRef]
- Kennelly, M.; Dmochowski, R.; Schulte-Baukloh, H.; Ethans, K.; Del Popolo, G.; Moore, C.; Jenkins, B.; Guard, S.; Zheng, Y.; Karsenty, G. Efficacy and safety of onabotulinumtoxinA therapy are sustained over 4 years of treatment in patients with neurogenic detrusor overactivity: Final results of a long-term extension study. Neurourol. Urodyn. 2017, 36, 368–375. [Google Scholar] [CrossRef]
- Li, G.P.; Wang, X.Y.; Zhang, Y. Efficacy and Safety of OnabotulinumtoxinA in Patients With Neurogenic Detrusor Overactivity Caused by Spinal Cord Injury: A Systematic Review and Meta-analysis. Int. Neurourol. J. 2018, 22, 275–286. [Google Scholar] [CrossRef] [Green Version]
- Yuan, H.; Cui, Y.; Wu, J.; Peng, P.; Sun, X.; Gao, Z. Efficacy and Adverse Events Associated With Use of OnabotulinumtoxinA for Treatment of Neurogenic Detrusor Overactivity: A Meta-Analysis. Int. Neurourol. J. 2017, 21, 53–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vainrib, M.; Reyblat, P.; Ginsberg, D.A. Long-term efficacy of repeat incisions of bladder neck/external sphincter in patients with spinal cord injury. Urology 2014, 84, 940–945. [Google Scholar] [CrossRef] [PubMed]
- van der Merwe, A.; Baalbergen, E.; Shrosbree, R.; Smit, S.; Heyns, C. Outcome of dual flange metallic urethral stents in the treatment of neuropathic bladder dysfunction after spinal cord injury. J. Endourol. 2012, 26, 1210–1215. [Google Scholar] [CrossRef]
- Kuris, E.O.; Alsoof, D.; Osorio, C.; Daniels, A.H. Bowel and Bladder Care in Patients With Spinal Cord Injury. J. Am. Acad. Orthop. Surg. 2022, 30, 263–272. [Google Scholar] [CrossRef]
- Lombardi, G.; Nelli, F.; Mencarini, M.; Del Popolo, G. Clinical concomitant benefits on pelvic floor dysfunctions after sacral neuromodulation in patients with incomplete spinal cord injury. Spinal Cord 2011, 49, 629–636. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wyndaele, J.J.; Birch, B.; Borau, A.; Burks, F.; Castro-Diaz, D.; Chartier-Kastler, E.; Drake, M.; Ishizuka, O.; Minigawa, T.; Opisso, E.; et al. Surgical management of the neurogenic bladder after spinal cord injury. World J. Urol. 2018, 36, 1569–1576. [Google Scholar] [CrossRef]
- Cendron, M.; Gearhart, J.P. The Mitrofanoff principle. Technique and application in continent urinary diversion. Urol. Clin. N. Am. 1991, 18, 615–621. [Google Scholar] [CrossRef]
- Monti, P.R.; Lara, R.C.; Dutra, M.A.; de Carvalho, J.R. New techniques for construction of efferent conduits based on the Mitrofanoff principle. Urology 1997, 49, 112–115. [Google Scholar] [CrossRef]
- Myers, J.B.; Lenherr, S.M.; Stoffel, J.T.; Elliott, S.P.; Presson, A.P.; Zhang, C.; Rosenbluth, J.; Jha, A.; Patel, D.P.; Welk, B. Patient Reported Bladder Related Symptoms and Quality of Life after Spinal Cord Injury with Different Bladder Management Strategies. J. Urol. 2019, 202, 574–584. [Google Scholar] [CrossRef]
- Narayanaswamy, B.; Wilcox, D.T.; Cuckow, P.M.; Duffy, P.G.; Ransley, P.G. The Yang-Monti ileovesicostomy: A problematic channel? BJU Int. 2001, 87, 861–865. [Google Scholar] [CrossRef]
- Chang, D.T.; Lawrentschuk, N. Orthotopic neobladder reconstruction. Urol. Ann. 2015, 7, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Vanni, A.J.; Stoffel, J.T. Ileovesicostomy for the neurogenic bladder patient: Outcome and cost comparison of open and robotic assisted techniques. Urology 2011, 77, 1375–1380. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Anatomic Location | Sympathetic NS (Norepinephrine) | Parasympathetic NS (Acetylcholine) | Somatic Innervation (Acetylcholine) |
|---|---|---|---|
| Kidney | Renal plexus | Renal plexus | NA |
| Ureters | T12–L2 | S2–S4 | Superior hypogastric plexus |
| Bladder Dome | Hypogastric Nerve (T10–L2) on β3 Adrenergic Receptors | Pelvic Nerves (S2–S4) on M3 ACH Receptors | NA |
| Bladder Neck | Hypogastric Nerve (T10–L2) on α1 Adrenergic Receptors | Pelvic Nerves (S2–S4) on M3 ACH Receptors | NA |
| External Urethral Sphincter/Pelvic Floor Muscles | NA | NA | Pudendal Nerve (S2–S4) on Nicotinic ACH Receptors |
| Spinal Cord Lesion | Bladder and External Urethral Sphincter Dysfunction |
|---|---|
| Suprasacral Upper Motor Neuron (UMN) Injury | Storage Dysfunction
|
| Mixed: UMN and/or LMN Injury | Storage Dysfunction
|
| Sacral/Infrasacral Lower Motor Neuron (LMN) Injury | Voiding Dysfunction
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Perez, N.E.; Godbole, N.P.; Amin, K.; Syan, R.; Gater, D.R., Jr. Neurogenic Bladder Physiology, Pathogenesis, and Management after Spinal Cord Injury. J. Pers. Med. 2022, 12, 968. https://doi.org/10.3390/jpm12060968
Perez NE, Godbole NP, Amin K, Syan R, Gater DR Jr. Neurogenic Bladder Physiology, Pathogenesis, and Management after Spinal Cord Injury. Journal of Personalized Medicine. 2022; 12(6):968. https://doi.org/10.3390/jpm12060968
Chicago/Turabian StylePerez, Nathalie Elisabeth, Neha Pradyumna Godbole, Katherine Amin, Raveen Syan, and David R. Gater, Jr. 2022. "Neurogenic Bladder Physiology, Pathogenesis, and Management after Spinal Cord Injury" Journal of Personalized Medicine 12, no. 6: 968. https://doi.org/10.3390/jpm12060968