
Closing the Gap: Bridging Peripheral Sensory Nerve Defects with a Chitosan-Based Conduit a Randomized Prospective Clinical Trial

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Inclusion and Exclusion Criteria
2.2.1. Preoperative Inclusion Criteria
2.2.2. Intraoperative Inclusion Criteria
2.2.3. Preoperative Exclusion Criteria
2.2.4. Intraoperative Exclusion Criteria
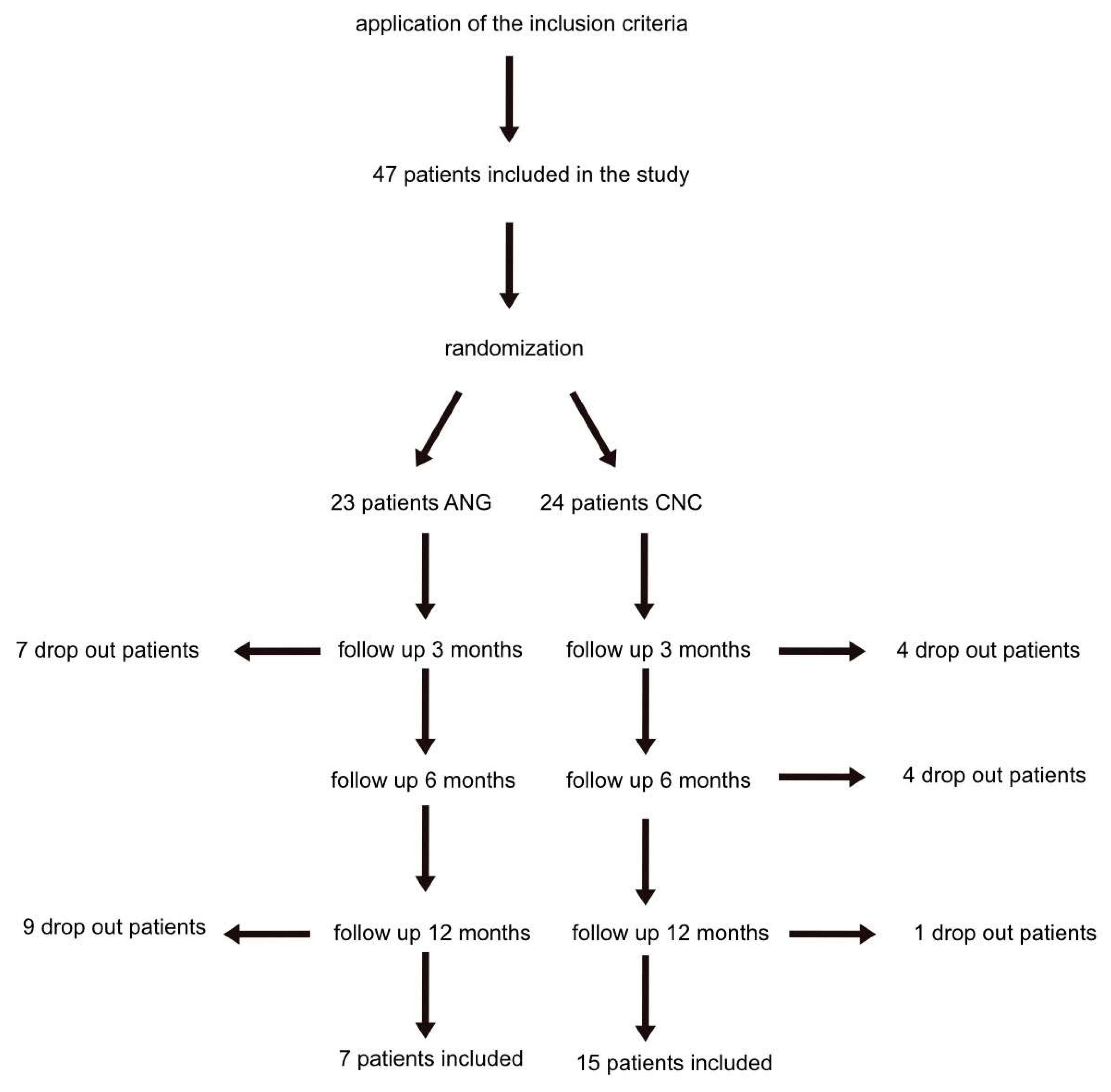
2.3. Participants and Randomization
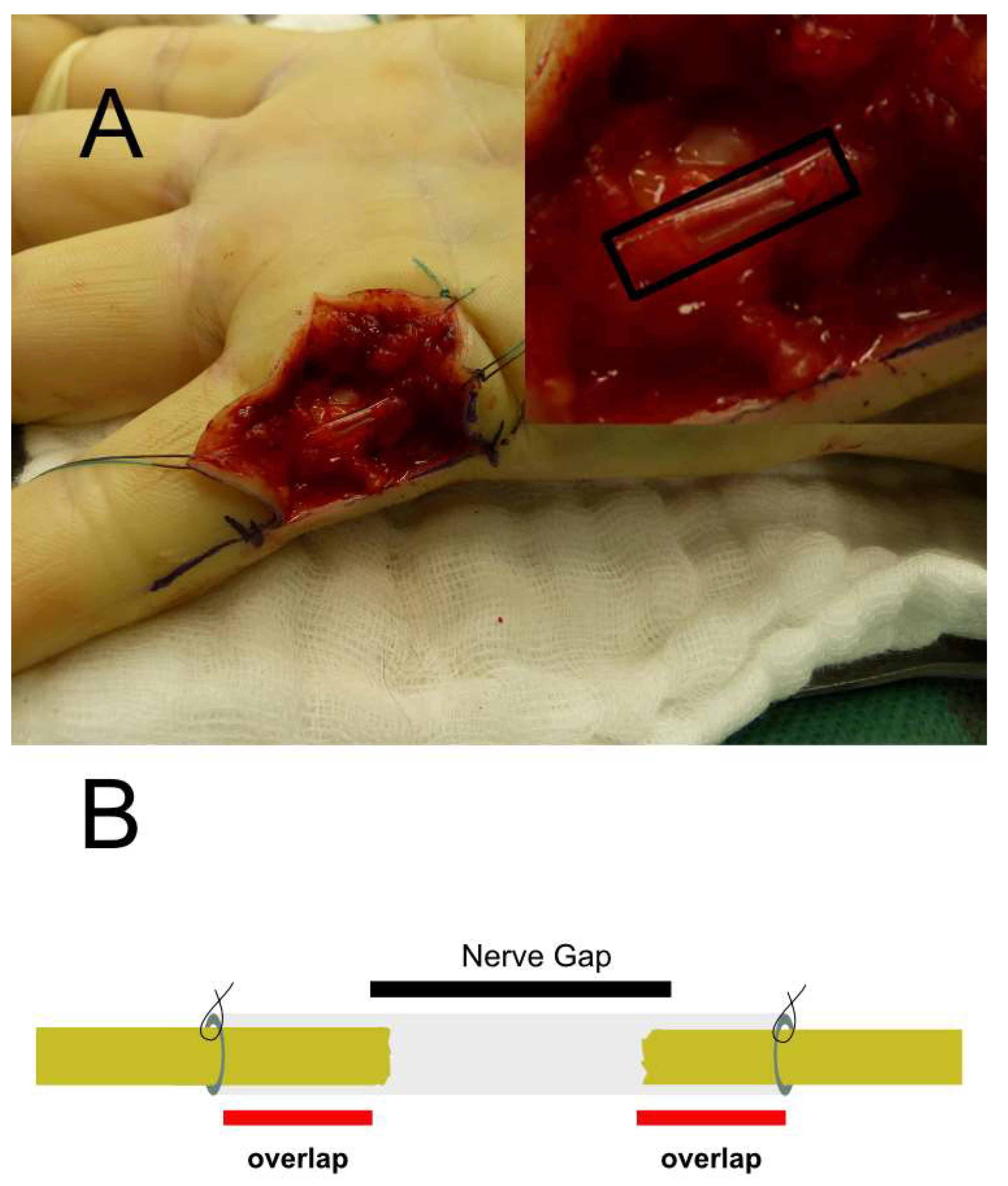
2.4. Interventions
2.5. Follow-Up and Blinding
2.6. Statistical Analysis
3. Results
3.1. Qualitative Analysis
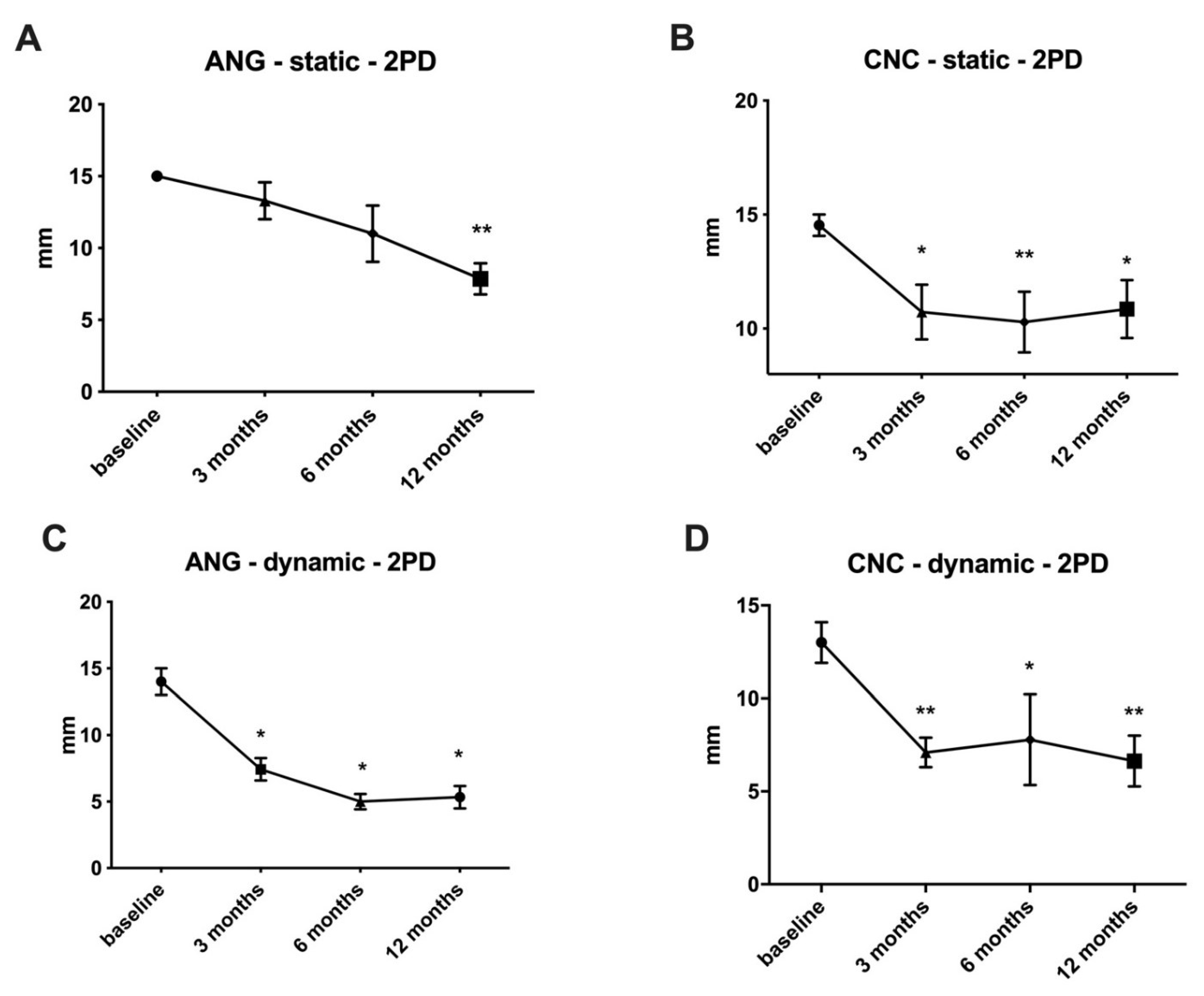
3.2. Primary Outcome Parameter–Tactile Gnosis (Two-Point Discrimination)
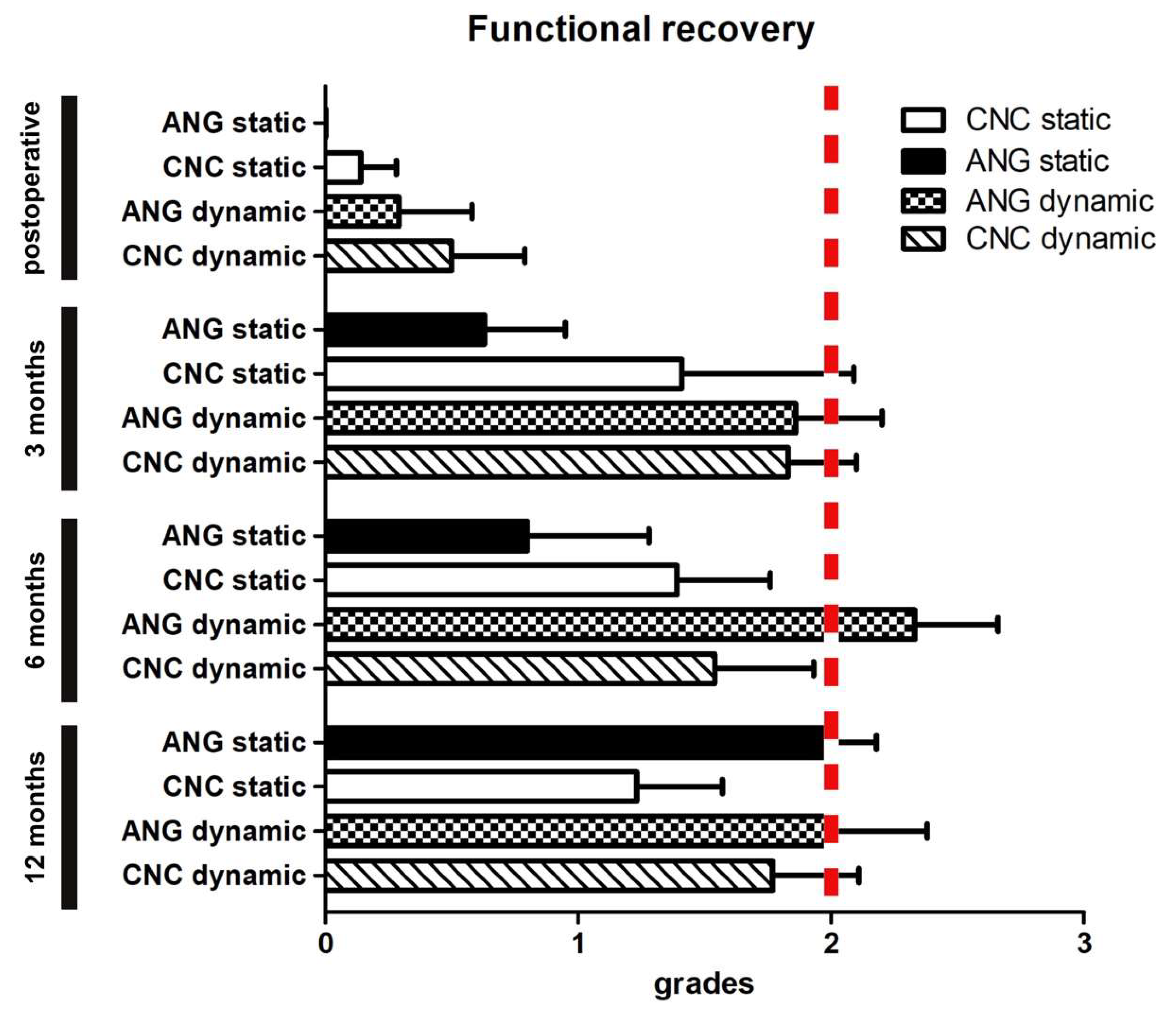
3.3. Secondary Outcome Parameter–Functional Analysis by Grading
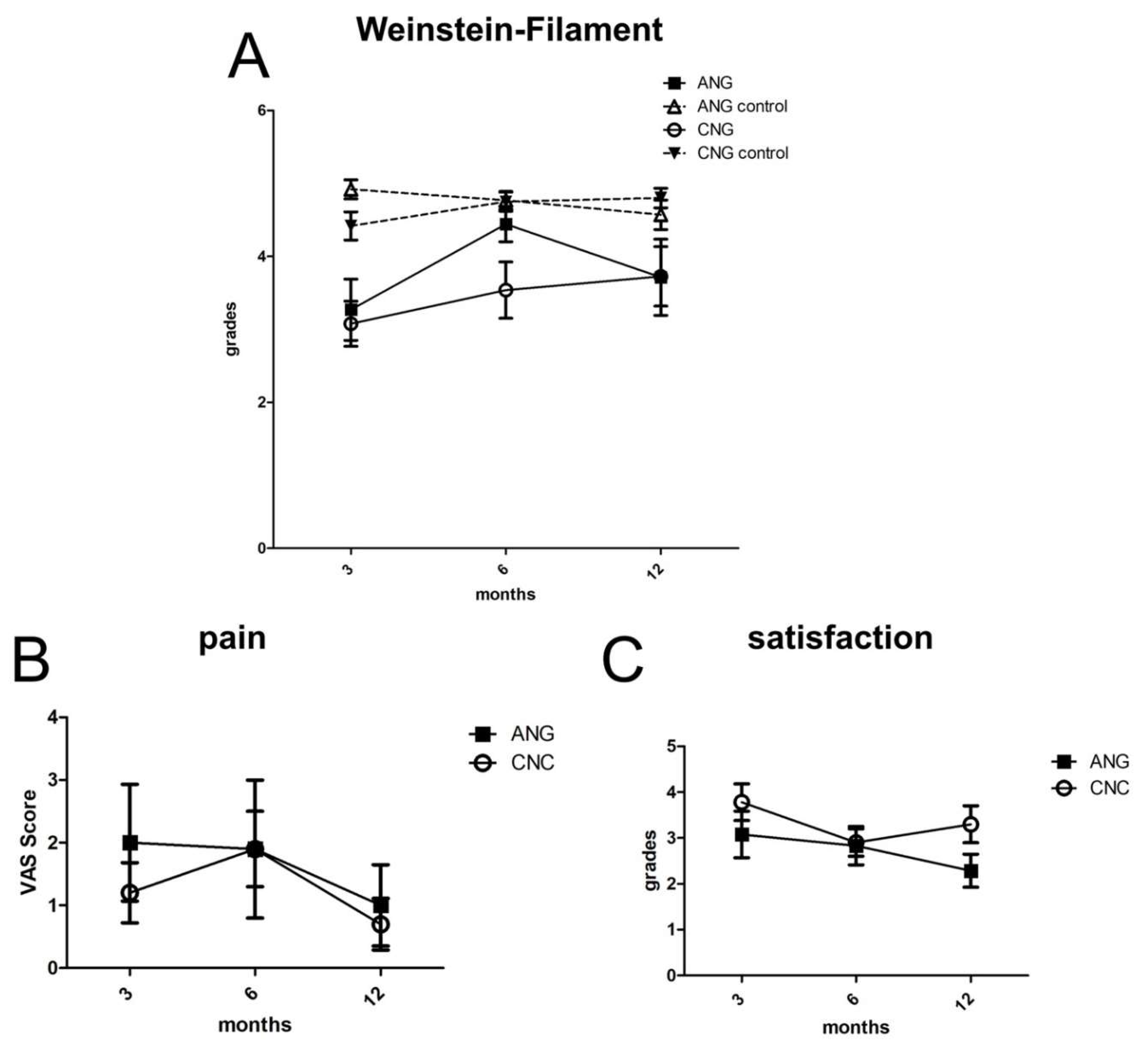
3.4. Secondary Outcome Parameter–Semmes Weinstein Monofilament Testing
3.5. Secondary Outcome Parameter–Pain Assessed by the Visual Analogue Scale and Patient Satisfaction
3.6. Adverse Events
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ANG | autologous nerve graft |
| CNC | Chitosan-based nerve conduit |
| FDA | Food and Drug Administration |
| PNI | peripheral nerve injury |
References
- Millesi, H. Nerve transplantation for reconstruction of peripheral nerves injured by the use of the microsurgical technic. Minerva Chir. 1967, 22, 950–951. [Google Scholar] [PubMed]
- Deumens, R.; Bozkurt, A.; Meek, M.F.; Marcus, M.A.; Joosten, E.A.; Weis, J.; Brook, G.A. Repairing injured peripheral nerves: Bridging the gap. Prog. Neurobiol. 2010, 92, 245–276. [Google Scholar] [CrossRef] [PubMed]
- Risitano, G.; Cavallaro, G.; Merrino, T.; Coppolino, S.; Ruggeri, F. Clinical results and thoughts on sensory nerve repair by autologous vein graft in emergency hand reconstruction. Chir. Main. 2002, 21, 194–197. [Google Scholar] [CrossRef]
- Manoli, T.; Schulz, L.; Stahl, S.; Jaminet, P.; Schaller, H.-E. Evaluation of sensory recovery after reconstruction of digital nerves of the hand using muscle-in-vein conduits in comparison to nerve suture or nerve autografting. Microsurgery 2014, 34, 608–615. [Google Scholar] [CrossRef]
- Bozkurt, A.; Claeys, K.G.; Schrading, S.; Rödler, J.V.; Altinova, H.; Schulz, J.B.; Weis, J.; Pallua, N.; Van Neerven, S.G.A. Clinical and biometrical 12-month follow-up in patients after reconstruction of the sural nerve biopsy defect by the collagen-based nerve guide Neuromaix. Eur. J. Med. Res. 2017, 22, 34. [Google Scholar] [CrossRef] [Green Version]
- Lohmeyer, J.A.; Shen, Z.L.; Walter, G.F.; Berger, A. Bridging extended nerve defects with an artifcial nerve graft containing Schwann cells pre-seeded on polyglactin filaments. Int. J. Artif. Organs 2007, 30, 64–74. [Google Scholar] [CrossRef]
- Freier, T.; Montenegro, R.; Shan Koh, H.; Shoichet, M.S. Chitin-based tubes for tissue engineering in the nervous system. Biomaterials 2005, 26, 4624–4632. [Google Scholar] [CrossRef]
- Schmidt, C.E.; Leach, J.B. Neural Tissue Engineering: Strategies for Repair and Regeneration. Annu. Rev. Biomed. Eng. 2003, 5, 293–347. [Google Scholar] [CrossRef] [Green Version]
- Gnavi, S.; Barwig, C.; Freier, T.; Haastert-Talini, K.; Grothe, C.; Geuna, S. The Use of Chitosan-Based Scaffolds to Enhance Regeneration in the Nervous System. Int. Rev. Neurobiol. 2013, 109, 1–62. [Google Scholar]
- Meyer, C.; Wrobel, S.; Raimondo, S.; Rochkind, S.; Heimann, C.; Shahar, A.; Ziv-Polat, O.; Geuna, S.; Grothe, C.; Haastert-Talini, K. Peripheral Nerve Regeneration through Hydrogel-Enriched Chitosan Conduits Containing Engineered Schwann Cells for Drug Delivery. Cell Transplant. 2016, 25, 159–182. [Google Scholar] [CrossRef] [Green Version]
- Li, R.; Liu, H.; Huang, H.; Bi, W.; Yan, R.; Tan, X.; Wen, W.; Wang, C.; Song, W.; Zhang, Y.; et al. Chitosan conduit combined with hyaluronic acid prevent sciatic nerve scar in a rat model of peripheral nerve crush injury. Mol. Med. Rep. 2018, 17, 4360–4368. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marcol, W.; Larysz-Brysz, M.; Kucharska, M.; Niekraszewicz, A.; Slusarczyk, W.; Kotulska, K.; Wlaszczuk, P.; Wlaszczuk, A.; Jedrzejowska-Szypulka, H.; Lewin-Kowalik, J. Reduction of post-traumatic neuroma and epineural scar formation in rat sciatic nerve by application of microcrystallic chitosan. Microsurgery 2011, 31, 642–649. [Google Scholar] [CrossRef] [PubMed]
- Neubrech, F.; Sauerbier, M.; Moll, W.; Seegmüller, J.; Heider, S.; Harhaus, L.; Bickert, B.; Kneser, U.; Kremer, T. Enhancing the Outcome of Traumatic Sensory Nerve Lesions of the Hand by Additional Use of a Chitosan Nerve Tube in Primary Nerve Repair. Plast. Reconstr. Surg. 2018, 142, 415–424. [Google Scholar] [CrossRef] [PubMed]
- Regas, I.; Loisel, F.; Haight, H.; Menu, G.; Obert, L.; Pluvy, I. Functionalized nerve conduits for peripheral nerve regeneration: A literature review. Hand Surg. Rehabil. 2020, 39, 343–351. [Google Scholar] [CrossRef]
- Safa, B.; Shores, J.T.; Ingari, J.V.; Weber, R.V.; Cho, M.; Zoldos, J.; Niacaras, T.R.; Nesti, L.J.; Thayer, W.P.; Buncke, G.M. Recovery of Motor Function after Mixed and Motor Nerve Repair with Processed Nerve Allograft. Plast. Reconstr. Surg. Glob. Open 2019, 7, e2163. [Google Scholar] [CrossRef]
- Nawrotek, K.; Tylman, M.; Rudnicka, K.; Gatkowska, J.; Wieczorek, M. Epineurium-mimicking chitosan conduits for peripheral nervous tissue engineering. Carbohydr. Polym. 2016, 152, 119–128. [Google Scholar] [CrossRef]
- Kehoe, S.; Zhang, X.F.F.; Boyd, D. FDA approved guidance conduits and wraps for peripheral nerve injury: A review of materials and efficacy. Injury 2012, 43, 553–572. [Google Scholar] [CrossRef]
- Wang, Y.; Sunitha, M.; Chung, K.C. How to measure outcomes of peripheral nerve surgery. Hand Clin. 2013, 29, 349–361. [Google Scholar] [CrossRef] [Green Version]
- Anjum, S.; Arora, A.; Alam, M.S.; Gupta, B. Development of antimicrobial and scar preventive chitosan hydrogel wound dressings. Int. J. Pharm. 2016, 508, 92–101. [Google Scholar] [CrossRef]
- Wang, Y.; Zhao, Y.; Sun, C.; Hu, W.; Zhao, J.; Li, G.; Zhang, L.; Liu, M.; Liu, Y.; Ding, F.; et al. Chitosan Degradation Products Promote Nerve Regeneration by Stimulating Schwann Cell Proliferation via miR-27a/FOXO1 Axis. Mol. Neurobiol. 2016, 53, 28–39. [Google Scholar] [CrossRef]
- Jiang, M.; Cheng, Q.; Su, W.; Wang, C.; Yang, Y.; Cao, Z.; Ding, F. The beneficial effect of chitooligosaccharides on cell behavior and function of primary Schwann cells is accompanied by up-regulation of adhesion proteins and neurotrophins. Neurochem. Res. 2014, 39, 2047–2057. [Google Scholar] [CrossRef] [PubMed]
- Meek, M.F.; Coert, J.H. Recovery of two-point discrimination function after digital nerve repair in the hand using resorbable FDA- and CE-approved nerve conduits. J. Plast. Reconstr. Aesthet. Surg. 2013, 66, 1307–1315. [Google Scholar] [CrossRef] [PubMed]
- Meek, M.F.; Coert, J.H. US Food and Drug Administration /Conformit Europe- approved absorbable nerve conduits for clinical repair of peripheral and cranial nerves. Ann. Plast. Surg. 2008, 60, 466–472. [Google Scholar] [CrossRef] [PubMed]
- Lohmeyer, J.A.; Siemers, F.; Machens, H.-G.; Mailänder, P. The clinical use of artificial nerve conduits for digital nerve repair: A prospective cohort study and literature review. J. Reconstr. Microsurg. 2009, 25, 55–61. [Google Scholar] [CrossRef] [Green Version]
- Chiriac, S.; Facca, S.; Diaconu, M.; Gouzou, S.; Liverneaux, P. Experience of using the bioresorbable copolyester poly(DL-lactide-ε-caprolactone) nerve conduit guide NeurolacTM for nerve repair in peripheral nerve defects: Report on a series of 28 lesions. J. Hand Surg. Eur. Vol. 2012, 37, 342–349. [Google Scholar] [CrossRef]
- Rinker, B.; Liau, J.Y. A prospective randomized study comparing woven polyglycolic acid and autogenous vein conduits for reconstruction of digital nerve gaps. J. Hand Surg. 2011, 36, 775–781. [Google Scholar] [CrossRef]
- Safa, B.; Jain, S.; Desai, M.J.; Greenberg, J.A.; Niacaris, T.R.; Do, J.A.N.; Leversedge, F.J.; Megee, D.M.; Zoldos, J.; Rinker, B.D.; et al. Peripheral nerve repair throughout the body with processed nerve allografts: Results from a large multicenter study. Microsurgery 2020, 40, 527–537. [Google Scholar] [CrossRef] [Green Version]
- Lundborg, G.; Rosén, B. The Two-Point Discrimination Test—Time For a Re-Appraisal? J. Hand Surg. 2004, 29, 418–422. [Google Scholar] [CrossRef]
- Gong, Y.; Gong, L.; Gu, X.; Ding, F. Chitooligosaccharides promote peripheral nerve regeneration in a rabbit common peroneal nerve crush injury model. Microsurgery 2009, 29, 650–656. [Google Scholar] [CrossRef]
- Rbia, N.; Bulstra, L.F.; Saffari, T.M.; Hovius, S.E.R.; Shin, A.Y. Collagen Nerve Conduits and Processed Nerve Allografts for the Reconstruction of Digital Nerve Gaps: A Single-Institution Case Series and Review of the Literature. World Neurosurg. 2019, 127, e1176–e1184. [Google Scholar] [CrossRef]
- Dellon, A.L.; Maloney, C.T. Salvage of Sensation in a Hallux-to-Thumb Transfer by Nerve Tube Reconstruction. J. Hand Surg. 2006, 31, 1495–1498. [Google Scholar] [CrossRef] [PubMed]
- Thomsen, L.; Bellemere, P.; Loubersac, T.; Gaisne, E.; Poirier, P.; Chaise, F. Treatment by collagen conduit of painful post-traumatic neuromas of the sensitive digital nerve: A retrospective study of 10 cases. Chir. Main. 2010, 29, 255–262. [Google Scholar] [CrossRef] [PubMed]
- Vlot, M.A.; Wilkens, S.C.; Chen, N.C.; Eberlin, K.R. Symptomatic Neuroma Following Initial Amputation for Traumatic Digital Amputation. J. Hand Surg. 2018, 43, e1–e86. [Google Scholar] [CrossRef] [PubMed]
- Keilhoff, G.; Fansa, H. Mesenchymal stem cells for peripheral nerve regeneration—A real hope or just an empty promise? Exp. Neurol. 2011, 232, 110–113. [Google Scholar] [CrossRef] [PubMed]
- Boecker, A.H.; Van Neerven, S.G.A.; Scheffel, J.; Tank, J.; Altinova, H.; Seidensticker, K.; Deumens, R.; Tolba, R.; Weis, J.; Brook, G.A.; et al. Pre-differentiation of mesenchymal stromal cells in combination with a microstructured nerve guide supports peripheral nerve regeneration in the rat sciatic nerve model. Eur J. Neurosci. 2015, 43, 404–416. [Google Scholar] [CrossRef] [Green Version]
- Yamamoto, D.; Tada, K.; Suganuma, S.; Hayashi, K.; Nakajima, T.; Nakada, M.; Matsuta, M.; Tsuchiya, H. Differentiated adipose-derived stem cells promote peripheral nerve regeneration. Muscle Nerve 2020, 62, 119–127. [Google Scholar] [CrossRef] [PubMed]
- Hersant, B.; SidAhmed-Mezi, M.; Aboud, C.; Niddam, J.; Levy, S.; Mernier, T.; La Padula, S.; Meningaud, J.-P. Synergistic Effects of Autologous Platelet-Rich Plasma and Hyaluronic Acid Injections on Facial Skin Rejuvenation. Aesthet. Surg. J. 2021, 41, NP854–NP865. [Google Scholar] [CrossRef]
- La Padula, S.; Hersant, B.; Pizza, C.; Chesné, C.; Jamin, A.; Mosbah, I.B.; Errico, C.; D’Andrea, F.; Rega, U.; Persichetti, P.; et al. Striae Distensae: In Vitro Study and Assessment of Combined Treatment With Sodium Ascorbate and Platelet-Rich Plasma on Fibroblasts. Aesthetic Plast. Surg. 2021, 45, 1282–1293. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ANG | CNC | p-Value | ||
|---|---|---|---|---|
| Age | 45.43 ± 5.85 | 35.93 ± 3.33 | 0.5331 | |
| Sex | ||||
| male | 86% (6) | 67% (10) | ||
| female | 14% (1) | 33% (5) | ||
| Injury | ||||
| crush | 29% (2) | 20% (3) | ||
| cut | 71% (5) | 73% (11) | ||
| both | 0% (0) | 7% (1) | ||
| Dominant hand | ||||
| right | 100% (7) | 80% (12) | ||
| left | 0% (0) | 13% (2) | ||
| Injury side | ||||
| right | 43% (3) | 60% (9) | ||
| left | 57% (4) | 40% (6) | ||
| dominant | 43% (3) | 47% (7) | ||
| Defect size (mm) | 12.80 ± 2.01 | 13.25 ± 1.89 | 0.6218 | |
| Regeneration length (mm) | 56.10 ± 0.76 | 66.88 ± 0.81 | 0.3653 | |
| Implantat length (mm) | 15.00 ± 2.76 | 17.38 ± 2.05 | 0.6746 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Böcker, A.; Aman, M.; Kneser, U.; Harhaus, L.; Siemers, F.; Stang, F. Closing the Gap: Bridging Peripheral Sensory Nerve Defects with a Chitosan-Based Conduit a Randomized Prospective Clinical Trial. J. Pers. Med. 2022, 12, 900. https://doi.org/10.3390/jpm12060900
Böcker A, Aman M, Kneser U, Harhaus L, Siemers F, Stang F. Closing the Gap: Bridging Peripheral Sensory Nerve Defects with a Chitosan-Based Conduit a Randomized Prospective Clinical Trial. Journal of Personalized Medicine. 2022; 12(6):900. https://doi.org/10.3390/jpm12060900
Chicago/Turabian StyleBöcker, Arne, Martin Aman, Ulrich Kneser, Leila Harhaus, Frank Siemers, and Felix Stang. 2022. "Closing the Gap: Bridging Peripheral Sensory Nerve Defects with a Chitosan-Based Conduit a Randomized Prospective Clinical Trial" Journal of Personalized Medicine 12, no. 6: 900. https://doi.org/10.3390/jpm12060900