
Personalized Model to Predict Small for Gestational Age at Delivery Using Fetal Biometrics, Maternal Characteristics, and Pregnancy Biomarkers: A Retrospective Cohort Study of Births Assisted at a Spanish Hospital

 , , and
, , and 
Abstract
:1. Introduction
2. Material and Methods
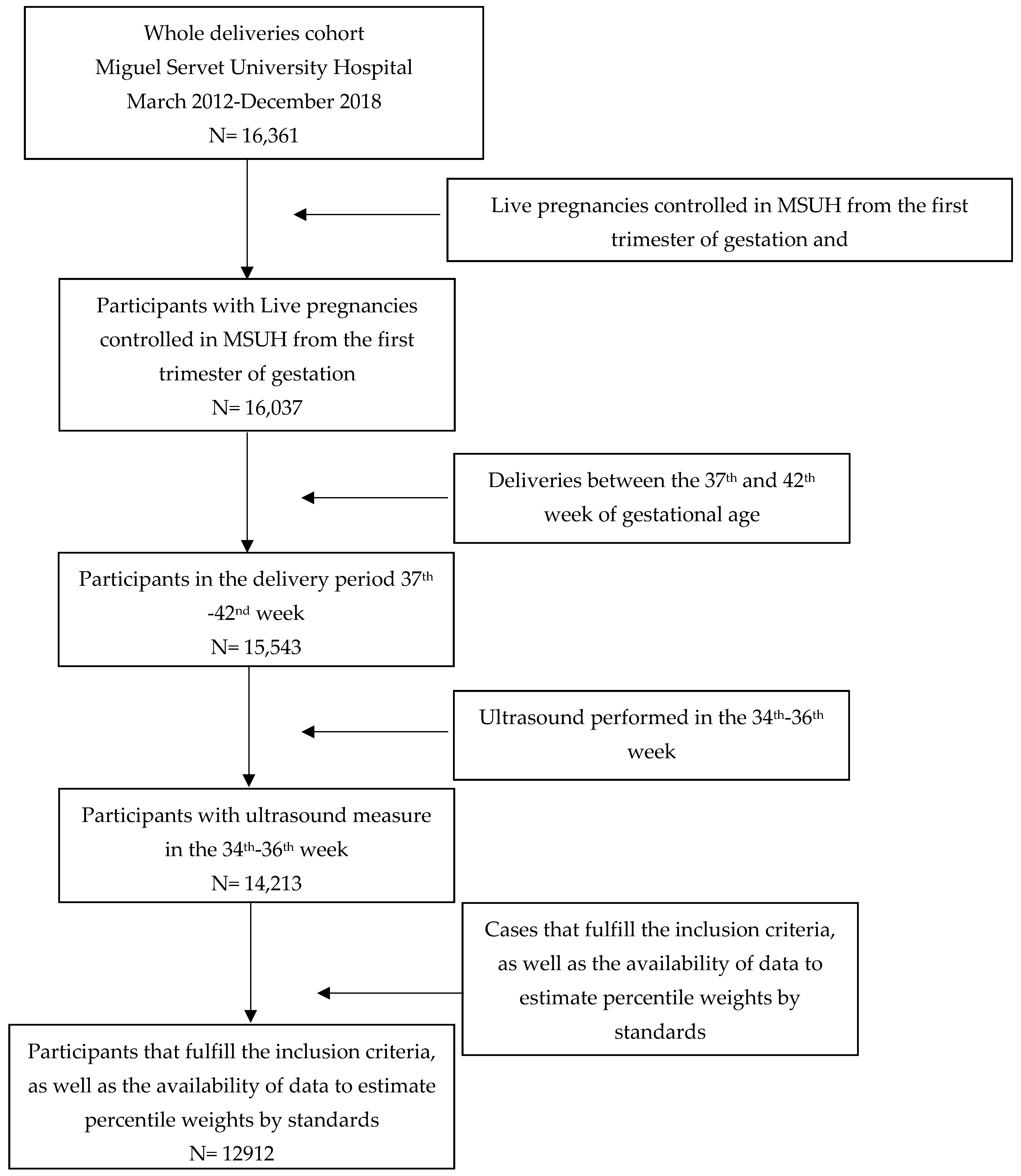
2.1. Study Design
2.2. Estimated Percentile Weight
2.3. Estimated Abdominal Circumference Percentile
2.4. Statistical Analysis
3. Results
3.1. Descriptive Results
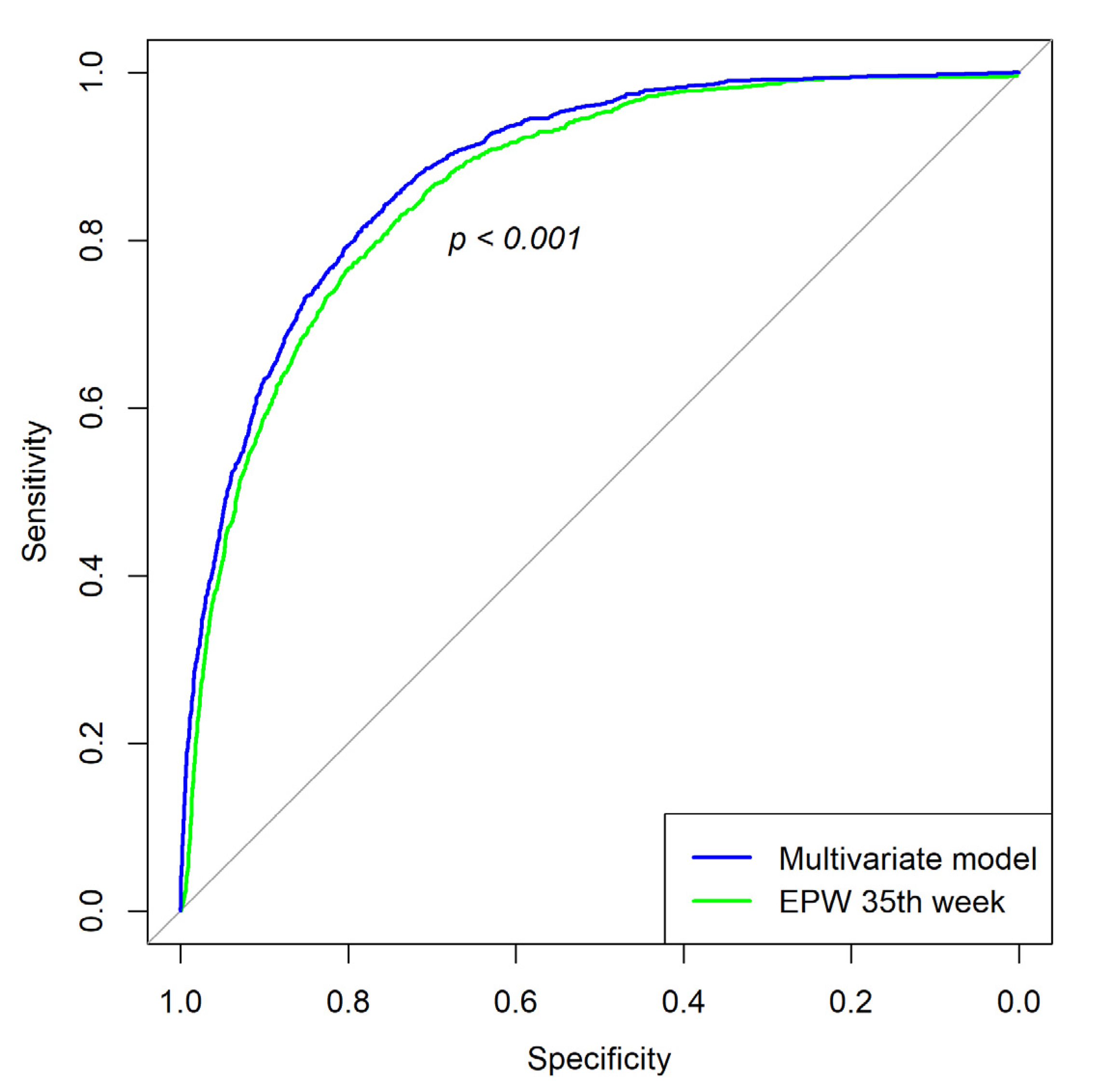
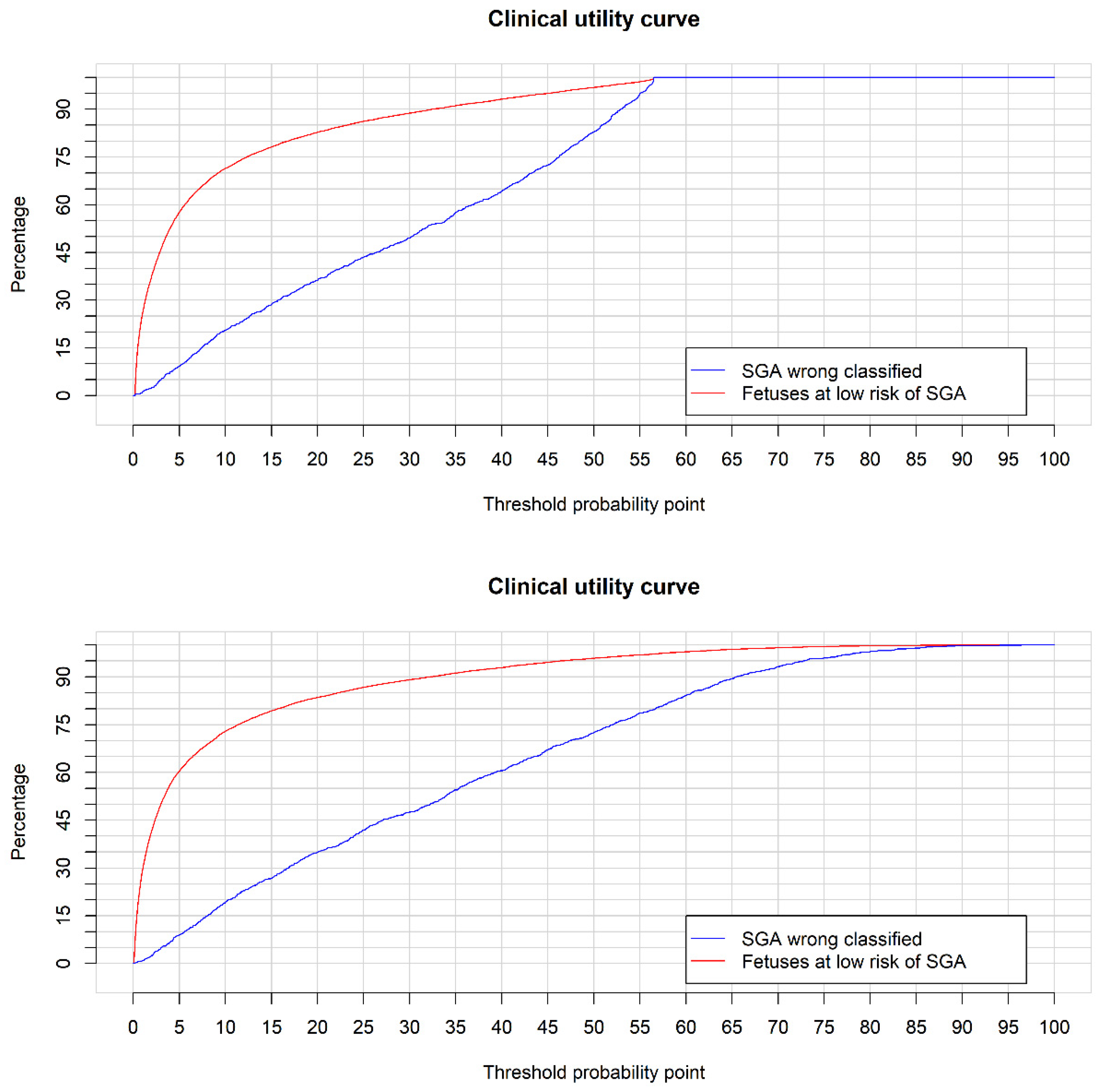
3.2. Small for Gestational Age Prediction
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Figueras, F.; Gratacós, E. Update on the diagnosis and classification of fetal growth restriction and proposal of a stage-based management protocol. Fetal Diagn Ther. 2014, 36, 86–98. [Google Scholar] [CrossRef] [PubMed]
- McIntire, D.D.; Bloom, S.L.; Casey, B.M.; Leveno, K.J. Weight in relation to morbidity and mortality among newborn infants. Eng. J. Med. 1999, 340, 1234–1248. [Google Scholar] [CrossRef] [PubMed]
- Gardosi, J.; Madurasinghe, V.; Williams, M.; Malik, A.; Francis, A. Maternal and fetal risk factors for stillbirth: Population based study. BMJ 2013, 346, f108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malhotra, A.; Allison, B.J.; Castillo-Melendez, M.; Jenkin, G.; Polglase, G.R.; Miller, S.L. Neonatal morbidities of fetal growth restriction: Pathophysiology and impact. Front. Endocrinol. 2019, 10, 55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ciobanu, A.; Formuso, C.; Syngelaki, A.; Akolekar, R.; Nicolaides, K.H. Prediction of small-for-gestational-age neonates at 35–37 weeks’ gestation: Contribution of maternal factors and growth velocity between 20 and 36 weeks. Ultrasound Obstet. Gynecol. 2019, 53, 488–495. [Google Scholar] [CrossRef]
- Villar, J.; Ismail, L.C.; Victora, C.G.; Ohuma, E.O.; Bertino, E.; Altman, D.G.; Lambert, A.; Papageorghiou, A.T.; Carvalho, M.; Jaffer, Y.A.; et al. International standards for newborn weight, length, and head circumference by gestational age and sex: The Newborn Cross-Sectional Study of the INTERGROWTH-21st Project. Lancet 2014, 384, 857–868. [Google Scholar] [CrossRef]
- WHO Multicentre Growth Reference Study Group. WHO Child Growth Standards based on length/height, weight and age. Acta Paediatr. Suppl. 2006, 450, 76–85. [Google Scholar]
- McCowan, L.M.; Figueras, F.; Anderson, N.H. Evidence-based national guidelines for the management of suspected fetal growth restriction: Comparison, consensus, and controversy. Am. J. Obstet. Gynecol. 2018, 218, 855–868. [Google Scholar] [CrossRef] [Green Version]
- Figueras, F.; Eixarch, E.; Gratacós, E.; Gardosi, J. Predictiveness of antenatal umbilical artery Doppler for adverse pregnancy outcome in small-for-gestational-age babies according to customised birthweight centiles: Population-based study. BJOG Int. J. Obstet. Gynaecol. 2008, 115, 590–594. [Google Scholar] [CrossRef]
- Skovron, M.L.; Berkowitz, G.S.; Lapinski, R.H.; Kim, J.M.; Chitkara, U. Evaluation of early third-trimester ultrasound screening for intrauterine growth retardation. J. Ultrasound Obstet. Gynecol. Med. 1991, 10, 153–159. [Google Scholar] [CrossRef]
- Caradeux, J.; Martinez-Portilla, R.J.; Peguero, A.; Sotiriadis, A.; Figueras, F. Diagnostic performance of third-trimester ultrasound for the prediction of late-onset fetal growth restriction: A systematic review and meta-analysis. Am. J. Obstet. Gynecol. 2019, 220, 449–459. [Google Scholar] [CrossRef] [PubMed]
- Triunfo, S.; Crovetto, F.; Scazzocchio, E.; Parra-Saavedra, M.; Gratacós, E.; Figueras, F. Contingent versus routine third-trimester screening for late fetal growth restriction. Ultrasound Obstet. Gynecol. 2016, 47, 81–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Souka, A.P.; Papastefanou, I.; Pilalis, A.; Michalitsi, V.; Kassanos, D. Performance of third-trimester ultrasound for prediction of small-for-gestational-age neonates and evaluation of contingency screening policies. Ultrasound Obstet. Gynecol. 2012, 39, 535–542. [Google Scholar] [CrossRef] [PubMed]
- Souka, A.P.; Papastefanou, I.; Pilalis, A.; Michalitsi, V.; Panagopoulos, P.; Kassanos, D. Performance of the ultrasound examination in the early and late third trimester for the prediction of birth weight deviations. Prenat Diagn. 2013, 33, 915–920. [Google Scholar] [CrossRef] [PubMed]
- Di Lorenzo, G.; Monasta, L.; Ceccarello, M.; Cecotti, V.; D’Ottavio, G. Third trimester abdominal circumference, estimated fetal weight and uterine artery doppler for the identification of newborns small and large for gestational age. Eur. J. Obstet. Gynecol. Reprod. Biol. 2013, 166, 133–138. [Google Scholar] [CrossRef]
- Valiño, N.; Giunta, G.; Gallo, D.M.; Akolekar, R.; Nicolaides, K.H.; Akolekar, D.R. Biophysical and biochemical markers at 30–34 weeks’ gestation in the prediction of adverse perinatal outcome. Ultrasound Obstet. Gynecol. 2016, 47, 194–202. [Google Scholar] [CrossRef] [Green Version]
- Valiño, N.; Giunta, G.; Gallo, D.M.; Akolekar, R.; Nicolaides, K.H.; Akolekar, D.R. Biophysical and biochemical markers at 35–37 weeks’ gestation in the prediction of adverse perinatal outcome. Ultrasound Obstet. Gynecol. 2016, 47, 203–209. [Google Scholar] [CrossRef] [Green Version]
- Fadigas, C.; Saiid, Y.; Gonzalez, R.; Poon, L.C.; Nicolaides, K.H. Prediction of small-for-gestational-age neonates: Screening by fetal biometry at 35-37 weeks. Ultrasound Obstet. Gynecol. 2015, 45, 559–565. [Google Scholar] [CrossRef]
- Bakalis, S.; Silva, M.; Akolekar, R.; Poon, L.C.; Nicolaides, K.H. Prediction of small-for-gestational-age neonates: Screening by fetal biometry at 30–34 weeks. Ultrasound Obstet. Gynecol. 2015, 45, 551–558. [Google Scholar] [CrossRef]
- Bligh, L.N.; Flatley, C.J.; Kumar, S. Reduced growth velocity at term is associated with adverse neonatal outcomes in non-small for gestational age infants. Eur. J. Obstet. Gynecol. Reprod. Biol. 2019, 240, 125–129. [Google Scholar] [CrossRef]
- Miranda, J.; Triunfo, S.; Rodriguez-Lopez, M.; Sairanen, M.; Kouru, H.; Parra-Saavedra, M.; Crovetto, F.; Figureas, F.; Crispi, F.; Gratacós, E. Performance of third-trimester combined screening model for prediction of adverse perinatal outcome. Ultrasound Obstet. Gynecol. 2017, 50, 353–360. [Google Scholar] [CrossRef]
- McKenna, D.; Tharmaratnam, S.; Mahsud, S.; Bailie, C.; Harper, A.; Dornan, J. A randomized trial using ultrasound to identify the high-risk fetus in a low-risk population. Obstet. Gynecol. 2003, 101, 626–632. [Google Scholar] [PubMed]
- Erkamp, J.S.; Voerman, E.; Steegers, E.A.P.; Mulders, A.G.M.G.J.; Reiss, I.K.M.; Duijts, L.; Jaddoe, V.W.V.; Gaillard, R. Second and third trimester fetal ultrasound population screening for risks of preterm birth and small-size and large-size for gestational age at birth: A population-based prospective cohort study. BMC Med. 2020, 18, 63. [Google Scholar] [CrossRef] [PubMed]
- Litwińska, E.; Litwińska, M.; Oszukowski, P.; Szaflik, K.; Kaczmarek, P. Combined screening for early and late pre-eclampsia and intrauterine growth restriction by maternal history, uterine artery Doppler, mean arterial pressure and biochemical markers. Adv. Clin. Exp. Med. 2017, 26, 439–448. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhong, Y.; Zhu, F.; Ding, Y. Serum screening in first trimester to predict pre-eclampsia, small for gestational age and preterm delivery: Systematic review and meta-analysis. BMC Pregnancy Childbirth. 2015, 15, 191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pihl, K.; Larsen, T.; Krebs, L.; Christiansen, M. First trimester maternal serum PAPP-A, β-hCG and ADAM12 in prediction of small-for-gestational-age fetuses. Prenat Diagn. 2008, 28, 1131–1135. [Google Scholar] [CrossRef] [PubMed]
- Leung, T.Y.; Sahota, D.S.; Chan, L.W.; Law, L.W.; Fung, T.Y.; Leung, T.N.; Lau, T.K. Prediction of birth weight by fetal crown-rump length and maternal serum levels of pregnancy-associated plasma protein-A in the first trimester. Ultrasound Obstet. Gynecol. 2008, 31, 10–14. [Google Scholar] [CrossRef]
- Dukhovny, S.; Zera, C.; Little, S.E.; McElrath, T.; Wilkins-Haug, L. Eliminating first trimester markers: Will replacing PAPP-A and βhCG miss women at risk for small for gestational age? J. Matern. Neonatal. Med. 2014, 27, 1761–1764. [Google Scholar] [CrossRef]
- Yaron, Y.; Heifetz, S.; Ochshorn, Y.; Lehavi, O.; Orr-Urtreger, A. Decreased first trimester PAPP-A is a predictor of adverse pregnancy outcome. Prenat Diagn. 2002, 22, 778–782. [Google Scholar] [CrossRef]
- Canini, S.; Prefumo, F.; Pastorino, D.; Crocetti, L.; Afflitto, C.G.; Venturini, P.L.; De Biasio, P. Association between birth weight and first-trimester free β-human chorionic gonadotropin and pregnancy-associated plasma protein A. Fertil Steril. 2008, 89, 174–178. [Google Scholar] [CrossRef]
- Pettker, C.M.; Goldberg, J.D.; El-Sayed, Y.Y.; Copel, J.A. Committee opinion No 700: Methods for estimating the due date. Obstet. Gynecol. 2017, 129, 150–154. [Google Scholar]
- Hadlock, F.P.; Harrist, R.B.; Sharman, R.S.; Deter, R.L.; Park, S.K. Estimation of fetal weight with the use of head, body, and femur measurements--a prospective study. Am. J. Obstet. Gynecol. 1985, 151, 333–337. [Google Scholar] [CrossRef]
- Hadlock, F.P.; Harrist, R.B.; Martinez-Poyer, J. In utero analysis of fetal growth: A sonographic weight standard. Radiology 1991, 181, 129–133. [Google Scholar] [CrossRef] [PubMed]
- Savirón-Cornudella, R.; Esteban, L.M.; Lerma, D.; Cotaina, L.; Borque, Á.; Sanz, G.; Castan, S. Comparison of fetal weight distribution improved by paternal height by Spanish standard versus Intergrowth 21 st standard. J. Perinat. Med. 2018, 46, 750–759. [Google Scholar] [CrossRef] [Green Version]
- Carrascosa, A.; Fernández, J.M.; Ferrández, Á.; López-Siguero, J.P.; López, D.; Sánchez, E.; Colaborador, G. Estudios Españoles de crecimiento 2010. Rev Esp Endocrinol Pediatr. 2011, 259–262. [Google Scholar]
- Smulian, J.C.; Ananth, C.V.; Vintzileos, A.M.; Guzman, E.R. Revisiting sonographic abdominal circumference measurements: A comparison of outer centiles with established nomograms. Ultrasound Obstet. Gynecol. 2001, 18, 237–243. [Google Scholar] [CrossRef]
- Hanley, J.A.; McNeil, B.J. The meaning and use of the area under a receiver operating characteristic (ROC) curve. Radiology 1982, 143, 29–36. [Google Scholar] [CrossRef] [Green Version]
- Gu, W.; Pepe, M.S. Estimating the capacity for improvement in risk prediction with a marker. Biostatistics 2009, 10, 172–186. [Google Scholar] [CrossRef] [Green Version]
- Hosmer, D.W.; Lemeshow, S.; Sturdivant, R.X. Applied Logistic Regression, 3rd ed.; John Wiley & Sons: Hoboken, NJ, USA, 2013; pp. 1–510. [Google Scholar]
- Borque-Fernando, A.; Esteban-Escaño, L.M.; Rubio-Briones, J.; Lou-Mercadé, A.C.; García-Ruiz, R.; Tejero-Sánchez, A.; Muñoz-Rivero, M.V.; Cabañuz-Plo, T.; Alfaro-Torres, J.; Marquina-Ibáñez, I.M.; et al. A preliminary study of the ability of the 4kscore test, the prostate cancer prevention trial-risk calculator and the european research screening prostate-risk calculator for predicting high-grade prostate cancer. Actas Urol Esp. 2016, 40, 155–163. [Google Scholar] [CrossRef] [Green Version]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2008; Available online: https://www.R-project.org/ (accessed on 8 February 2008).
- Bakalis, S.; Peeva, G.; Gonzalez, R.; Poon, L.C.; Nicolaides, K.H. Prediction of small-for-gestational-age neonates: Screening by biophysical and biochemical markers at 30–34 weeks. Ultrasound Obstet. Gynecol. 2015, 46, 446–451. [Google Scholar] [CrossRef] [Green Version]
- Miranda, J.; Rodriguez-Lopez, M.; Triunfo, S.; Sairanen, M.; Kouru, H.; Parra-Saavedra, M.; Crovetto, F.; Figueras, F.; Crispi, F.; Gratacós, E. Prediction of fetal growth restriction using estimated fetal weight vs a combined screening model in the third trimester. Ultrasound Obstet. Gynecol. 2017, 50, 603–611. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Savirón-Cornudella, R.; Esteban, L.M.; Aznar-Gimeno, R.; Dieste-Pérez, P.; Pérez-López, F.R.; Campillos, J.M.; Castán-Larraz, B.; Sanz, G.; Tajada-Duaso, M. Clinical medicine prediction of late-onset small for gestational age and fetal growth restriction by fetal biometry at 35 weeks and impact of ultrasound-delivery interval: Comparison of six fetal growth standards. J. Clin. Med. 2021, 10, 2984. [Google Scholar] [CrossRef] [PubMed]
- Triunfo, S.; Crispi, F.; Gratacós, E.; Figueras, F. Prediction of delivery of small-for-gestational-age neonates and adverse perinatal outcome by fetoplacental Doppler at 37 weeks’ gestation. Ultrasound Obstet. Gynecol. 2017, 49, 364–371. [Google Scholar] [CrossRef] [Green Version]
- Fadigas, C.; Peeva, G.; Mendez, O.; Poon, L.C.; Nicolaides, K.H. Prediction of small-for-gestational-age neonates: Screening by placental growth factor and soluble fms-like tyrosine kinase-1 at 35–37 weeks. Ultrasound Obstet. Gynecol. 2015, 46, 191–197. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinical Characteristics | Pregnancies SGA (n = 1281) | Pregnancies Non-SGA (n = 11,631) | p-Value |
|---|---|---|---|
| Maternal characteristics | |||
| Maternal age (years) | 33.4 (29.9–36.4) | 33.2 (30.0–36.1) | 0.299 |
| Maternal body mass index (kg/m2) | 22.5 (20.7–25.4) | 23.4 (21.2–26.4) | <0.001 |
| Maternal height (cm) | 161 (157–165) | 163 (160–168) | <0.001 |
| Parity | |||
| 0 | 872 (68.1%) | 6151 (52.9%) | <0.001 |
| 1 | 339 (26.5%) | 4411 (37.9%) | |
| ≥2 | 70 (5.4%) | 1069 (9.2%) | |
| Previous cesarean | |||
| 0 | 1211 (94.5%) | 10,739 (92.3%) | 0.004 |
| 1 | 69 (5.4%) | 826 (7.1%) | |
| ≥2 | 1 (0.1%) | 66 (0.6%) | |
| In vitro fertilization | |||
| No | 1217 (95.0) | 11,121 (95.6%) | 0.394 |
| Yes | 64 (5.0%) | 510 (4.4%) | |
| Maternal smoking habits | |||
| Yes | 352 (27.5%) | 1676 (14.4%) | <0.001 |
| No | 929 (72.5%) | 9955 (85.6%) | |
| Hypertension | |||
| No | 1235 (96.4%) | 11,485 (98.7%) | <0.001 |
| Chronic | 5 (0.4%) | 25 (0.2%) | |
| Preeclampsia | 18 (1.4%) | 47 (0.4%) | |
| Gestational | 23 (1.8%) | 74 (0.6%) | |
| Diabetes | |||
| No | 1126 (87.9%) | 10,356 (89.0%) | 0.343 |
| Pregestational | 6 (0.5%) | 81 (0.7%) | |
| Gestational | 132 (10.3%) | 1043 (9.0%) | |
| Carbohydrate intolerance | 17 (1.3%) | 151 (1.3%) | |
| Ultrasound parameters at 35 (34–36) weeks | |||
| Gestational age (weeks) at ultrasound | 35.1 (35.0–35.3) | 35.1 (35.0–35.3) | 0.345 |
| Estimated fetal weight (grams) by Hadlock | 2186 (2042–2349) | 2532 (2362–2715) | <0.001 |
| Abdominal fetal circumference (cm) | 293 (284–301) | 311 (302–321) | <0.001 |
| Percentile weight by MSUH standard | |||
| <10 | 513 (42.1%) | 542 (4.7%) | <0.001 |
| ≥10 | 768 (57.9%) | 11,089 (95.3%) | |
| Percentile AC by Smulian standard | |||
| <10 | 237 (18.5%) | 200 (17.6%) | <0.001 |
| ≥10 | 1044 (81.5%) | 11,431 (82.4%) | |
| Pregnancy and perinatal outcomes | |||
| PAPP-A | 0.84 (0.57–1.25) | 0.99 (0.68–1.42) | <0.001 |
| β-HCG | 0.91 (0.61–1.42) | 1.00 (0.67–1.51) | <0.001 |
| Gestational age at delivery | 39.6 (38.7–40.4) | 40.7 (40.0–41.3) | <0.001 |
| Newborn gender | |||
| Female | 663 (51.8%) | 5617 (48.3%) | 0.020 |
| Male | 618 (48.2%) | 6014 (51.7%) | |
| Birth weight | 2650 (2480–2760) | 3350 (3100–3610) | <0.001 |
| Variable | Odds Ratio (95% C.I.) | p-Value |
|---|---|---|
| rcs (EPW) | 0.937 (0.928–0.947) | <0.001 |
| rcs (EPW)’ | 1.067 (1.030–1.106) | <0.001 |
| rcs (EPW)’’ | 0.813 (0.700–0.942) | 0.006 |
| Maternal age | 1.050 (1.035–1.065) | <0.001 |
| Maternal height | 0.948 (0.937–0.959) | <0.001 |
| Parity | 0.639 (0.572–0.711) | <0.001 |
| rcs (PAPP-A) | 0.439 (0.031–0.591) | <0.001 |
| rcs (PAPP-A)’ | 2.211 (1.490–3.066) | <0.001 |
| β-HCG | 0.880 (0.806–0.956) | 0.004 |
| Hypertension | ||
| Chronic: no | 2.887 (0.807–8.665) | 0.075 |
| Preeclampsia: no | 4.885 (2.443–9.476) | <0.001 |
| Gestational: no | 3.854 (2.066–7.009) | <0.001 |
| Smoking habits: no | 0.479 (0.408–0.563) | <0.001 |
| Abdominal circumference percentile | 0.120 (0.066–0.217) | <0.001 |
| Variable | AUC (95% C.I.) | Discrimination Rate (%) at 10% FPR |
|---|---|---|
| Abdominal circumference percentile | 0.840 (0.829–0.850) | 52.3 |
| EPW | 0.864 (0.854–0.873) | 58.9 |
| +Maternal age | 0.865 (0.855–0.874) | 59.4 |
| +Maternal height | 0.867 (0.859–0.878) | 60.1 |
| +Parity | 0.873 (0.863–0.882) | 60.7 |
| +PAPP-A | 0.874 (0.865–0.884) | 61.5 |
| +β-HCG | 0.875 (0.865–0.884) | 61.0 |
| +Hypertension | 0.877 (0.868–0.886) | 61.8 |
| +Smoking habit | 0.880 (0.871–0.889) | 61.8 |
| +Abdominal circumference percentile | 0.882 (0.873–0.891) | 63.5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dieste-Pérez, P.; Savirón-Cornudella, R.; Tajada-Duaso, M.; Pérez-López, F.R.; Castán-Mateo, S.; Sanz, G.; Esteban, L.M. Personalized Model to Predict Small for Gestational Age at Delivery Using Fetal Biometrics, Maternal Characteristics, and Pregnancy Biomarkers: A Retrospective Cohort Study of Births Assisted at a Spanish Hospital. J. Pers. Med. 2022, 12, 762. https://doi.org/10.3390/jpm12050762
Dieste-Pérez P, Savirón-Cornudella R, Tajada-Duaso M, Pérez-López FR, Castán-Mateo S, Sanz G, Esteban LM. Personalized Model to Predict Small for Gestational Age at Delivery Using Fetal Biometrics, Maternal Characteristics, and Pregnancy Biomarkers: A Retrospective Cohort Study of Births Assisted at a Spanish Hospital. Journal of Personalized Medicine. 2022; 12(5):762. https://doi.org/10.3390/jpm12050762
Chicago/Turabian StyleDieste-Pérez, Peña, Ricardo Savirón-Cornudella, Mauricio Tajada-Duaso, Faustino R. Pérez-López, Sergio Castán-Mateo, Gerardo Sanz, and Luis Mariano Esteban. 2022. "Personalized Model to Predict Small for Gestational Age at Delivery Using Fetal Biometrics, Maternal Characteristics, and Pregnancy Biomarkers: A Retrospective Cohort Study of Births Assisted at a Spanish Hospital" Journal of Personalized Medicine 12, no. 5: 762. https://doi.org/10.3390/jpm12050762