Healthcare Professional Perspectives on the Use of Remote Patient-Monitoring Platforms during the COVID-19 Pandemic: A Cross-Sectional Study

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Population and Recruitment of Participants
2.3. Survey
- (1)
- Quality and safety of care (access, safety, relevance, timeliness, etc.) [22].
- (2)
- Patient engagement and partnership with physicians and health care professionals (confidence/trust, autonomy, decision making, information sharing, personal context, empathy, and expertise) as per the CADICEE tool [23].
- (3)
- Perceptions of the technology [24].
- (4)
- The sociodemographic characteristics of the health professionals who used the two platforms [24].
2.4. Data Collection
2.5. Statistical Analysis
3. Results
3.1. Characteristics of Participants
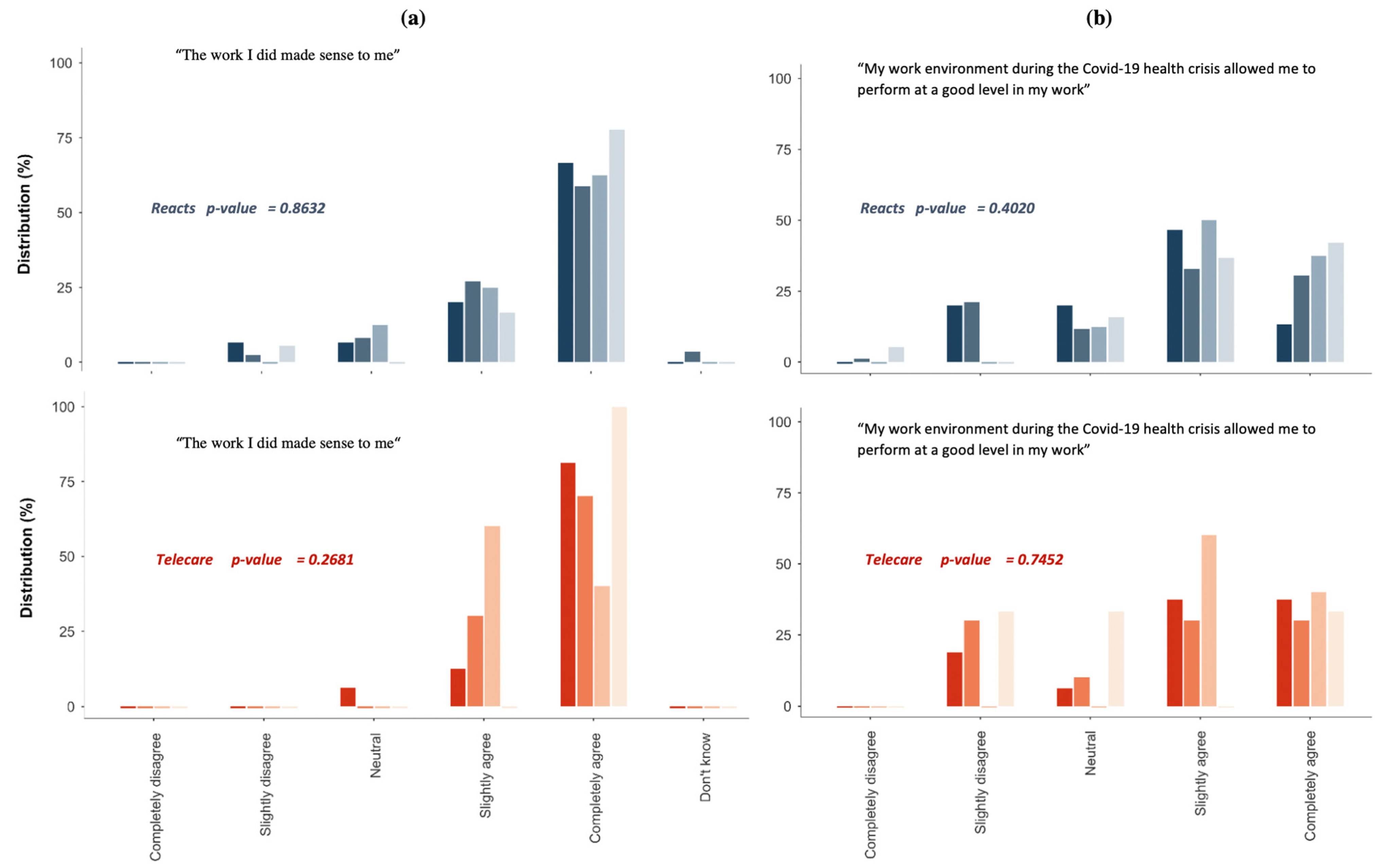
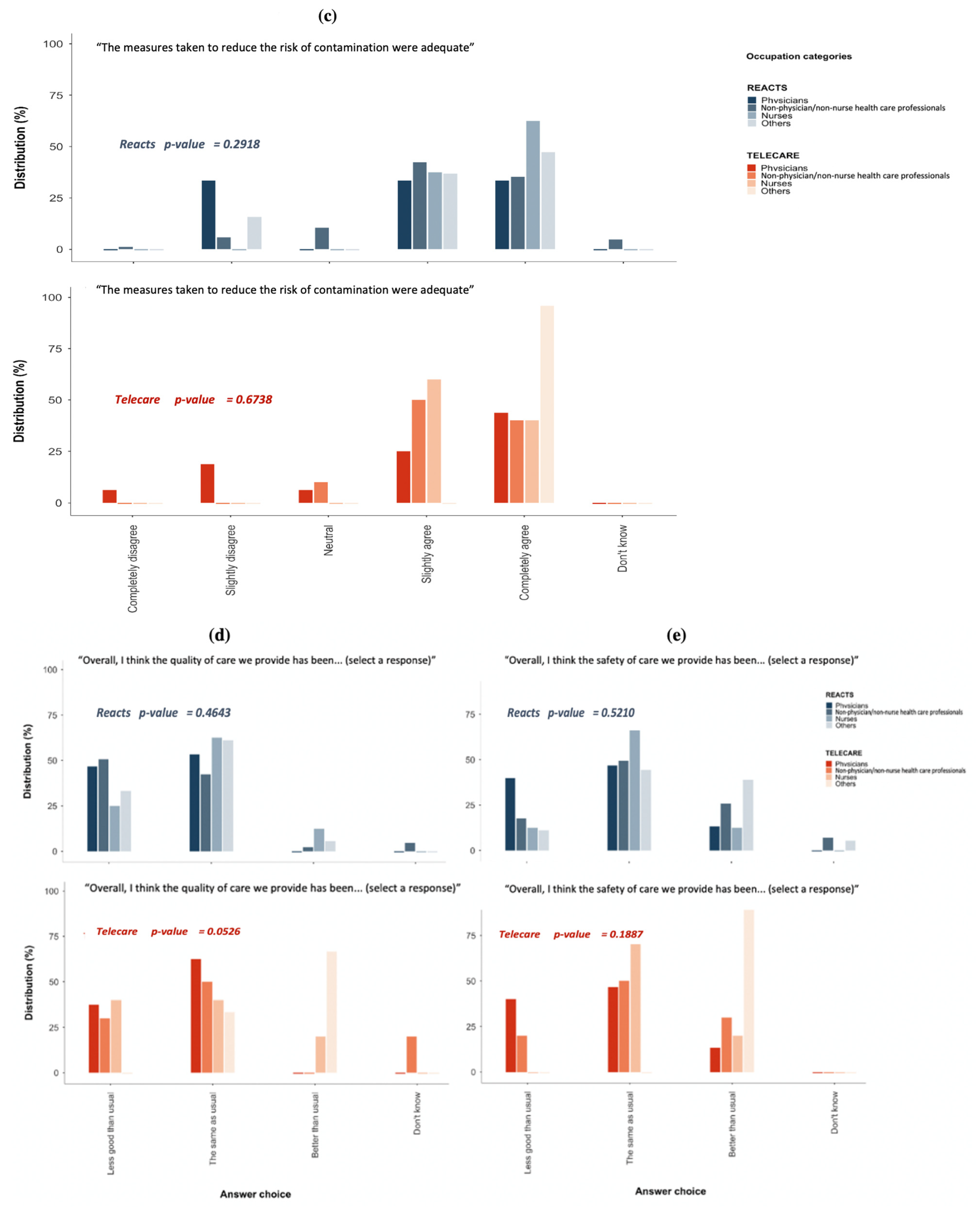
3.2. Perceptions of the Performance, Quality, and Safety of Care
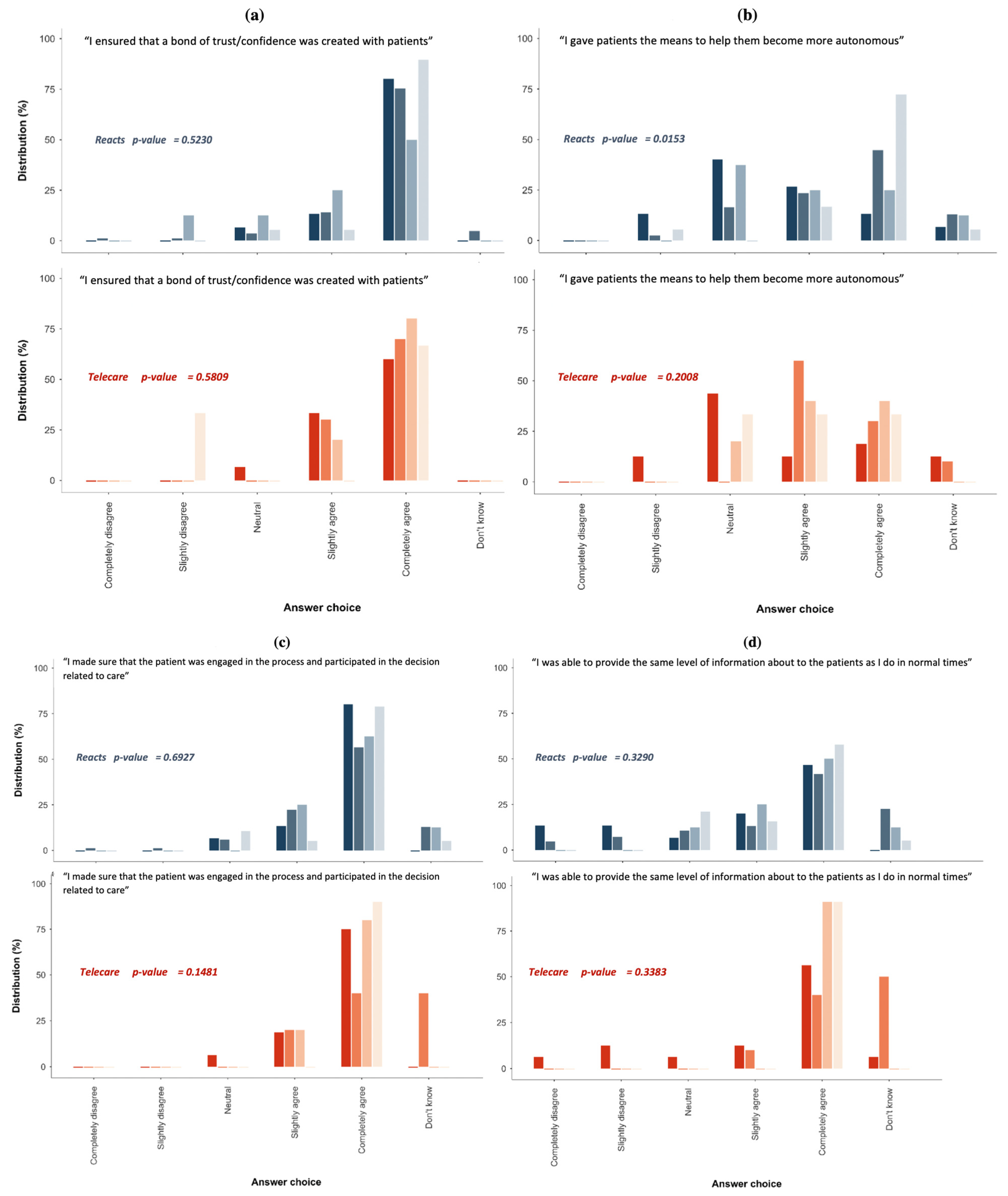
3.3. Perceptions of Patient Engagement in Care and the Relationship with the Care Team
3.4. Perceptions of the Role and Relevance (Usefulness, Advantages, and Limitations) of REACTS-Teleconsultation
3.5. Perceptions of the Role and Relevance (Usefulness, Advantages, and Limitations) of Telecare-Covid
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization (WHO). WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int (accessed on 8 February 2022).
- Government of Canada COVID-19 Daily Epidemiology Update. Available online: https://health-infobase.canada.ca/covid-19/epidemiological-summary-covid-19-cases.html (accessed on 8 February 2022).
- Gouvernement du Québec Données sur la COVID-19 au Québec. Available online: https://www.quebec.ca/sante/problemes-de-sante/a-z/coronavirus-2019/situation-coronavirus-quebec (accessed on 8 February 2022).
- World Health Organization (WHO). Coronavirus Disease (COVID-19) Pandemic. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (accessed on 8 February 2022).
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The Psychological Impact of Quarantine and How to Reduce It: Rapid Review of the Evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [Green Version]
- Bedford, J.; Enria, D.; Giesecke, J.; Heymann, D.; Ihekweazu, C.; Kobinger, G.; Lane, H.; Memish, Z.; Oh, M.; Sall, A.; et al. COVID-19: Towards Controlling of a Pandemic. Lancet 2020, 395, 1015–1018. [Google Scholar] [CrossRef]
- Institut National de Santé Publique du Québec Données COVID-19 au Québec. Available online: https://www.inspq.qc.ca/covid-19/donnees (accessed on 8 February 2022).
- Ministère de la Santé et des Services Sociaux Coronavirus (COVID-19). Available online: https://www.msss.gouv.qc.ca/professionnels/maladies-infectieuses/coronavirus-2019-ncov/ (accessed on 8 February 2022).
- Iyengar, K.; Mabrouk, A.; Jain, V.K.; Venkatesan, A.; Vaishya, R. Learning Opportunities from COVID-19 and Future Effects on Health Care System. Diabetes Metab. Syndr. 2020, 14, 943–946. [Google Scholar] [CrossRef] [PubMed]
- Shaukat, N.; Ali, D.M.; Razzak, J. Physical and Mental Health Impacts of COVID-19 on Healthcare Workers: A Scoping Review. Int. J. Emerg. Med. 2020, 13, 40. [Google Scholar] [CrossRef] [PubMed]
- Lai, J.; Ma, S.; Wang, Y.; Cai, Z.; Hu, J.; Wei, N.; Wu, J.; Du, H.; Chen, T.; Li, R.; et al. Factors Associated With Mental Health Outcomes Among Health Care Workers Exposed to Coronavirus Disease 2019. JAMA Netw. Open 2020, 3, e203976. [Google Scholar] [CrossRef]
- Lancet, T. COVID-19: Protecting Health-Care Workers. Lancet 2020, 395, 922. [Google Scholar] [CrossRef]
- Catton, H. Global Challenges in Health and Health Care for Nurses and Midwives Everywhere. Int. Nurs. Rev. 2020, 67, 4–6. [Google Scholar] [CrossRef] [Green Version]
- Muller, A.E.; Berg, R.C.; Jardim, P.S.J.; Johansen, T.B.; Ormstad, S.S. Can Remote Patient Monitoring Be the New Standard in Primary Care of Chronic Diseases, Post-COVID-19? Telemed. J. E. Health 2021. [Google Scholar] [CrossRef]
- CHUM le Programme Techno-Covid-Partenariat, un Programme de Recherche en Soutien aux Développements des Technologies et du Partenariat au CHUM et CUSM dans le Contexte de la COVID-19. 2020. Available online: https://www.chumontreal.qc.ca/crchum/nouvelles/le-programme-techno-covid-partenariat-un-programme-de-recherche-en-soutien-aux (accessed on 8 February 2022).
- Reacts Montreal Physician Creates New Telemedicine Platform. 2015. Available online: https://reacts.com/montreal-innovators-create-new-form-of-medical-videoconferencing/ (accessed on 8 February 2022).
- Ranganathan, P.; Aggarwal, R. Study Designs: Part 1—An Overview and Classification. Perspect. Clin. Res. 2018, 9, 184–186. [Google Scholar] [CrossRef]
- Hennekens, C.H.; Buring, J.E.; Mayrent, S.L. Epidemiology in Medicine; Little, Brown: Boston, MA, USA, 1987; ISBN 978-0-316-35636-7. [Google Scholar]
- Contandriopoulos, A.-P.; Champagne, F.; Potvin, L.; Denis, J.-L.; Boyle, P. Savoir Préparer Une Recherche- La Définir, La Structurer, La Financer; Morin, G., Ed.; Les Presses de l’Université de Montréal: Montréal, QC, Canada, 2005; ISBN 978-2-89105-825-4. [Google Scholar]
- Méot, A. Rappels de statistique descriptive. In Introduction aux Statistiques Inférentielles. De la Logique à la Pratique; De Boeck Supérieur: Wallonia, Belgium, 2003; pp. 19–52. [Google Scholar]
- Krippendorff, K. Reliability in Content Analysis: Some Common Misconceptions and Recommendations. Hum. Commun. Res. 2004, 30, 411–433. [Google Scholar] [CrossRef]
- Attkisson, C. The Client Satisfaction Questionnaire (CSQ) Scales. In Measures for Clinical Practice: A Sourcebook; Simon and Schuster: New York, NY, USA, 1996. [Google Scholar]
- Pomey, M.; Clavel, N.; Normandin, L.; Del Grande, C.; Philip Ghadiri, D.; Fernandez-McAuley, I.; Boivin, A.; Flora, L.; Janvier, A.; Karazivan, P.; et al. Assessing and Promoting Partnership between Patients and Health-care Professionals: Co-construction of the CADICEE Tool for Patients and Their Relatives. Health Expect. Int. J. Public Particip. Health Care Health Policy 2021, 24, 1230–1241. [Google Scholar] [CrossRef] [PubMed]
- Boulenger, S.; Motulsky, A.; Paré, G. Frequency, Nature and Impact of the Consultations Provided by Community Pharmacists in Quebec; CIRANO Project Reports 2018 rp-17; CIRANO: Montreal, QC, Canada, 2018. [Google Scholar]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap Consortium: Building an International Community of Software Platform Partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef] [PubMed]
- IBM. IBM SPSS Software; IBM Corp: Armonk, NY, USA, 2021. [Google Scholar]
- StataCorp Stata Statistical Software: Release 17; StataCorp LLC: College Station, TX, USA, 2021.
- Health Canada Annual Report on the Access to Information Act and the Privacy Act 2019 to 2020. 2021. Available online: https://www.canada.ca/en/health-canada/corporate/about-health-canada/reports-publications/access-information-privacy/2019-2020-annual-report-access-information-privacy-act.html (accessed on 8 February 2022).
- Ricci, R.P.; Morichelli, L.; Quarta, L.; Sassi, A.; Porfili, A.; Laudadio, M.T.; Gargaro, A.; Santini, M. Long-Term Patient Acceptance of and Satisfaction with Implanted Device Remote Monitoring. Europace 2010, 12, 674–679. [Google Scholar] [CrossRef] [PubMed]
- Hilty, D.M.; Ferrer, D.C.; Parish, M.B.; Johnston, B.; Callahan, E.J.; Yellowlees, P.M. The Effectiveness of Telemental Health: A 2013 Review. Telemed. J. E Health 2013, 19, 444–454. [Google Scholar] [CrossRef]
- Godleski, L.; Darkins, A.; Peters, J. Outcomes of 98,609 U.S. Department of Veterans Affairs Patients Enrolled in Telemental Health Services, 2006–2010. Psychiatr. Serv. Wash. DC 2012, 63, 383–385. [Google Scholar] [CrossRef]
- Worster, B.; Swartz, K. Telemedicine and Palliative Care: An Increasing Role in Supportive Oncology. Curr. Oncol. Rep. 2017, 19, 37. [Google Scholar] [CrossRef]
- Smrke, A.; Younger, E.; Wilson, R.; Husson, O.; Farag, S.; Merry, E.; Macklin-Doherty, A.; Cojocaru, E.; Arthur, A.; Benson, C.; et al. Telemedicine During the COVID-19 Pandemic: Impact on Care for Rare Cancers. JCO Glob. Oncol. 2020, 6, 1046–1051. [Google Scholar] [CrossRef]
- Bhaskar, S.; Bradley, S.; Chattu, V.K.; Adisesh, A.; Nurtazina, A.; Kyrykbayeva, S.; Sakhamuri, S.; Moguilner, S.; Pandya, S.; Schroeder, S.; et al. Telemedicine as the New Outpatient Clinic Gone Digital: Position Paper From the Pandemic Health System REsilience PROGRAM (REPROGRAM) International Consortium (Part 2). Front. Public Health 2020, 8, 410. [Google Scholar] [CrossRef]
- Zailani, S.; Gilani, M.S.; Nikbin, D.; Iranmanesh, M. Determinants of Telemedicine Acceptance in Selected Public Hospitals in Malaysia: Clinical Perspective. J. Med. Syst. 2014, 38, 111. [Google Scholar] [CrossRef]
- Hyder, M.A.; Razzak, J. Telemedicine in the United States: An Introduction for Students and Residents. J. Med. Internet Res. 2020, 22, e20839. [Google Scholar] [CrossRef]
- Ayatollahi, H.; Mirani, N.; Nazari, F.; Razavi, N. Iranian Healthcare Professionals’ Perspectives about Factors Influencing the Use of Telemedicine in Diabetes Management. World J. Diabetes 2018, 9, 92–98. [Google Scholar] [CrossRef] [PubMed]
- Shiferaw, K.B.; Mengiste, S.A.; Gullslett, M.K.; Zeleke, A.A.; Tilahun, B.; Tebeje, T.; Wondimu, R.; Desalegn, S.; Mehari, E.A. Healthcare Providers’ Acceptance of Telemedicine and Preference of Modalities during COVID-19 Pandemics in a Low-Resource Setting: An Extended UTAUT Model. PLoS ONE 2021, 16, e0250220. [Google Scholar] [CrossRef] [PubMed]
- Baudier, P.; Ammi, C.; Kondrateva, G. The Acceptability of Telemedicine Cabins by the Students. J. Innov. Econ. Manag. 2021, 35, 33–53. [Google Scholar] [CrossRef]
- Indria, D.; Alajlani, M.; Fraser, H.S.F. Clinicians Perceptions of a Telemedicine System: A Mixed Method Study of Makassar City, Indonesia. BMC Med. Inform. Decis. Mak. 2020, 20, 233. [Google Scholar] [CrossRef] [PubMed]
- MacNeill, V.; Sanders, C.; Fitzpatrick, R.; Hendy, J.; Barlow, J.; Knapp, M.; Rogers, A.; Bardsley, M.; Newman, S. Experiences of Front-Line Health Professionals in the Delivery of Telehealth: A Qualitative Study. Br. J. Gen. Pract. 2014, 64, e401–e407. [Google Scholar] [CrossRef] [Green Version]
- Kayyali, R.; Hesso, I.; Mahdi, A.; Hamzat, O.; Adu, A.; Nabhani Gebara, S. Telehealth: Misconceptions and Experiences of Healthcare Professionals in England. Int. J. Pharm. Pract. 2017, 25, 203–209. [Google Scholar] [CrossRef] [Green Version]
- Heiskanen, T.; Rinne, H.; Miettinen, S.; Salminen, A.-L. Uptake of Tele-Rehabilitation in Finland amongst Rehabilitation Professionals during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 4383. [Google Scholar] [CrossRef]
- American Speech-Language-Hearing Association Telepractice. Available online: https://www.asha.org/practice-portal/professional-issues/telepractice/ (accessed on 8 February 2022).
- Mahoney, M.F. Telehealth, Telemedicine, and Related Technologic Platforms: Current Practice and Response to the COVID-19 Pandemic. J. Wound Ostomy Cont. Nurs. 2020, 47, 439–444. [Google Scholar] [CrossRef]
- Bashir, A.; Bastola, D.R. Perspectives of Nurses Toward Telehealth Efficacy and Quality of Health Care: Pilot Study. JMIR Med. Inform. 2018, 6, e9080. [Google Scholar] [CrossRef] [Green Version]
- Russo, V.; Cassini, R.; Caso, V.; Donno, C.; Laezza, A.; Naddei, M.; Fiorelli, A.; Golino, P.; Nigro, G. Nursing Teleconsultation for the Outpatient Management of Patients with Cardiovascular Disease during COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 2087. [Google Scholar] [CrossRef]
- Peralta, E.A.; Taveras, M. Effectiveness of Teleconsultation Use in Access to Mental Health Services during the Coronavirus Disease 2019 Pandemic in the Dominican Republic. Indian J. Psychiatry 2020, 62, S492–S494. [Google Scholar] [CrossRef] [PubMed]
- King, H.C.; Bloomfield, B.S.; Wu, S.; Fischer, A.J. A Systematic Review of School Teleconsultation: Implications for Research and Practice. Sch. Psychol. Rev. 2021, 1–20. [Google Scholar] [CrossRef]
- Fischer, A.J.; Dart, E.H.; Radley, K.C.; Richardson, D.; Clark, R.; Wimberly, J. An Evaluation of the Effectiveness and Acceptability of Teleconsultation. J. Educ. Psychol. Consult. 2017, 27, 437–458. [Google Scholar] [CrossRef]
- Turcotte, V.; Chagnon, A.; Guénette, L. Experience and Perspectives of Users and Non-Users of the Ask Your Pharmacist Teleconsultation Platform. Explor. Res. Clin. Soc. Pharm. 2021, 2, 100031. [Google Scholar] [CrossRef]
- Grenier Ouimet, A.; Wagner, G.; Raymond, L.; Pare, G. Investigating Patients’ Intention to Continue Using Teleconsultation to Anticipate Postcrisis Momentum: Survey Study. J. Med. Internet Res. 2020, 22, e22081. [Google Scholar] [CrossRef]
- McKee, G.B.; Pierce, B.S.; Donovan, E.K.; Perrin, P.B. Examining Models of Psychologists’ Telepsychology Use during the COVID-19 Pandemic: A National Cross-Sectional Study. J. Clin. Psychol. 2021, 77, 2405–2423. [Google Scholar] [CrossRef]
- American Psychological Society Guidelines for the Practice of Telepsychology. 2013. Available online: https://www.apa.org/practice/guidelines/telepsychology (accessed on 8 February 2022).
- Australian Psychological Society 59. Psychological Services via Telehealth: Information for Consumers. Available online: https://psychology.org.au/getmedia/fd748495-90e7-40d8-bedb-c3d7999cbb2d/18aps-telehealth-consumers.pdf (accessed on 8 February 2022).
- Parker, K.; Uddin, R.; Ridgers, N.D.; Brown, H.; Veitch, J.; Salmon, J.; Timperio, A.; Sahlqvist, S.; Cassar, S.; Toffoletti, K.; et al. The Use of Digital Platforms for Adults’ and Adolescents’ Physical Activity During the COVID-19 Pandemic (Our Life at Home): Survey Study. J. Med. Internet Res. 2021, 23, e23389. [Google Scholar] [CrossRef]
- Sosa, J.P.; Ferreira Caceres, M.M. Technology and Digital Platforms In Fighting the COVID-19 Pandemic. Seek. J. Virol. Dis. 2020, 1, 1–7. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Section/Dimension | Questionnaire Item/Attribute |
|---|---|
| Section 1, Demographic characteristics | Gender |
| Age | |
| Profession (physician, nurse, non-physician/non-nurse, other) | |
| Years of experience | |
| Section 2, Perceptions of performance and of quality and safety of care | The work I did made sense to me. |
| My work environment during the COVID-19 health crisis allowed me to perform at a good level in my work. | |
| Overall, I think the quality of care we provide has been… (select a response) | |
| Overall, I think the safety of care we provide has been… (select a response) | |
| The measures taken to reduce the risk of contamination were adequate. | |
| Section 3, Perceptions of patient engagement in care and the relationship with the care team | I ensured that a bond of confidence/trust was created with patients. |
| I gave patients the means to help them become more autonomous. | |
| I made sure that the patient was engaged in the process and participated in the decisions related to care. | |
| I was able to provide the same amount of information about care to the patients as I do in normal times. | |
| I ensured that patients were always able to provide me with information on the state of their health (their health condition). | |
| I made a point of showing empathy for the patient. | |
| I considered the patient as a full member of the care team. | |
| Section 4. Perceptions of the role played by the technology/platform and its relevance (usefulness, advantages, and limitations) | The platform/technology is a good response to my needs or my patients’ needs (useful). |
| What were the advantages of using the platform/technology? | |
| What obstacles or problems prevented routine use of the platform/technology? | |
| Using the platform/technology reduced my daily use of personal protective equipment (PPE). | |
| Indicate whether the measure(s) should be maintained after the health crisis. |
| Characteristics | Total (n = 491) | REACTS-Teleconsultation | p-Value | Telecare-Covid | p-Value | ||
|---|---|---|---|---|---|---|---|
| Yes (n = 128) | No (n = 364) | Yes (n = 34) | No (n = 458) | ||||
| Gender *, n (%) | |||||||
| Male | 111 (22.7) | 26 (20.3) | 85 (23.5) | 0.587 | 10 (29.4) | 101 (22.2) | 0.546 |
| Female | 377 (76.9) | 101 (78.9) | 276 (76.2) | 24 (70.6) | 353 (77.4) | ||
| Age *, n (%) | |||||||
| <24 years | 30 (6.1) | 2 (1.6) | 28 (7.7) | 0.001 | 3 (8.8) | 27 (5.9) | 0.364 |
| 25–34 years | 157 (32.0) | 39 (30.5) | 118 (32.5) | 6 (17.7) | 151 (33.0) | ||
| 35–44 years | 146 (29.7) | 48 (37.5) | 98 (27.0) | 12 (35.3) | 134 (29.3) | ||
| 45–54 years | 112 (22.8) | 35 (27.3) | 77 (21.2) | 11 (32.4) | 101 (22.1) | ||
| ≥55 years | 46 (9.4) | 4 (3.1) | 42 (11.6) | 2 (5.9) | 42 (9.6) | ||
| Professions, n (%) | |||||||
| Physicians | 40 (8.2) | 15 (11.8) | 25 (6.9) | <0.001 | 16 (47.1) | 24 (5.3) | <0.001 |
| Non-physician/non-nurse health care professionals | 294 (59.9) | 85 (66.9) | 209 (57.4) | 10 (29.4) | 284 (62.1) | ||
| Nurses | 81 (16.5) | 8 (6.3) | 73 (20.1) | 5 (14.7) | 76 (16.6) | ||
| Other | 76 (15.5) | 19 (15.0) | 57 (15.7) | 3 (8.8) | 73 (16.0) | ||
| Years worked ** | |||||||
| Median (IQR) | 9 (13.0) | 10 (13.3) | 8 (13.0) | 0.563 | 10 (13.0) | 9 (13.0) | 0.735 |
| The Platform/Technology is a Good Response to My Needs or Patients’ Needs (Useful) | REACT-Teleconsultation n = 127 n (%) | Telecare-Covid n = 28 n (%) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| All | Physicians | Non-Physician/Non-Nurse Health Care Professionals | Nurses | Others | p-Value | All | Physicians | Non-Physician/Non-Nurse Health Care Professionals | Nurses | Others | p-Value | |
| Completely disagree | 5 (100) | 3 (60.0) | 1 (20.0) | 0 (0.0) | 1 (20.0) | NA | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0.983 |
| Slightly disagree | 17 (100) | 4 (23.5) | 12 (70.6) | 1 (5.9) | 0 (0.0) | 3 (100) | 2 (12) | 1 (10) | 0 (0.0) | 0 (0.0) | ||
| Neutral | 12 (100) | 2 (16.7) | 5 (41.7) | 4 (33.3) | 1 (8.3) | 3 (100) | 2 (66.7) | 1 (33.3) | 0 (0.0) | 0 (0.0) | ||
| Slightly agree | 39 (100) | 1 (2.6) | 33 (84.6) | 0 | 5 (12.8) | 10 (100) | 6 (60) | 2 (20) | 1 (10) | 1 (10) | ||
| Completely agree | 38 (100) | 5 (13.2) | 22 (57.9) | 2 (3.3) | 9 (23.7) | 14 (100) | 5 (35.7) | 4 (28.6) | 3 (21.4) | 2 (14.3) | ||
| I do not want to answer/I do not know/Does not apply | 16 (100) | 0 (0.0) | 12 (75.0) | 1 (6.2) | 3 (18.8) | 4 (100) | 1 (25.0) | 2 (50.0) | 1 (25.0) | 0 (0.0) | ||
| What were the advantages of using the platform/technology? | ||||||||||||
| Increased accessibility of services | 43 (100) | 11 (25.6) | 18 (41.9) | NA | 14 (32.6) | 0.568 | 5 (100) | 2 (40.0) | 3 (60.0) | NA | 0 (0.0) | 0.054 |
| Reduced waiting time | 21 (100) | 2 (9.5) | 12 (57.1) | NA | 7 (33.3) | 0.028 | 4 (100) | 1 (25.0) | 2 (50.0) | NA | 1 (25.0) | 0.266 |
| Improved quality of care | 11 (100) | 3 (27.3) | 7 (63.6) | NA | 1 (9.1) | 0.086 | 5 (100) | 2 (40.0) | 3 (60.0) | NA | 0 (0.0) | 0.054 |
| Improved efficiency of care | 19 (100) | 6 (31.6) | 10 (52.6) | NA | 3 (15.8) | 0.093 | 3 (100) | 1 (33.3) | 1 (33.3) | NA | 1 (33.3) | 0.678 |
| Increased number of times we can interact | 20 (100) | 4 (20.0) | 10 (50.0) | NA | 6 (30.0) | 0.378 | 2 (100) | 1 (50.0) | 1 (50.0) | NA | 0 (0.0) | 0.522 |
| Improved access and speed of care | 25 (100) | 6 (24.0) | 12 (48.0) | NA | 7 (28.0) | 0.386 | 4 (100) | 0 (0.0) | 3 (75.0) | NA | 1 (25.0) | 0.011 |
| Promotes user participation (user-partner approach) | 21 (100) | 4 (19.0) | 14 (66.7) | NA | 3 (14.3) | 0.002 | 4 (100) | 2 (50.0) | 0 (0.0) | NA | 2 (50.0) | 0.244 |
| Optimization of the use of resources (Adequate use and accessibility to skills) | 17 (100) | 4 (23.5) | 9 (52.9) | NA | 4 (23.5) | 0.302 | 3 (100) | 1 (33.3) | 2 (66.7) | NA | 0 (0.0) | 0.119 |
| Support for integrated service networks (inter-professional collaboration and service integration) | 8 (100) | 0 (0.0) | 6 (75.0) | NA | 2 (25.0) | 0.047 | 2 (100) | 0 (0.0) | 1 (50.0) | NA | 1 (50.0) | 0.238 |
| Using the platform/technology reduced my daily use of personal protective equipment (PPE) | ||||||||||||
| Completely disagree | 8 (100) | 1 (12.5) | 5 (62.5) | 1 (12.5) | 1 (12.5) | 10 (100) | 4 (40) | 2 (20) | 2 (20) | 2 (20) | ||
| Slightly disagree | 9 (100) | 2 (22) | 5 (55.6) | 1 (11.1) | 1 (11.1) | 1 (100) | 1 (100) | 0 | 0 | 0 | ||
| Neutral | 9 (100) | 1 (11.1) | 4 (44.5) | 2 (22.2) | 2 (22.2) | 0.149 | 7 (100) | 6 (85.7) | 0 | 1 (14.3) | 0 | 0.318 |
| Slightly agree | 29 (100) | 3 (10.3) | 20 (69.0) | 2 (6.9) | 4 (13.8) | 7(100) | 2 (28.6) | 4 (57.1) | 1 (14.3) | 0 | ||
| Completely agree | 55 (100) | 8 (14.5) | 37 (67.3) | 0 | 10 (18.2) | 4 (100) | 2 (50.0) | 1 (25.0) | 0 | 1 (25.0) | ||
| I do not want to answer/I do not know/Does not apply | 17 (100) | 0 | 14 (82.3) | 2 (11.8) | 1 (5.9) | 5 (100) | 1 (20.0) | 3 (60.0) | 1 (20.0) | 0 | ||
| Indicate whether the measure(s) should be maintained after the health crisis | 54 (100) | 14 (25.9) | 26 (30) | NA | 14 (25.9) | 0.003 | 18 (100) | 9 (50.0) | 5 (27.8) | NA | 4 (22.2) | 0.493 |
| Problems/Difficulties Encountered | REACT-Teleconsultation n = 117 n (%) | Telecare-Covid n = 28 n (%) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| All | Physicians | Non-Physician/Non-Nurse Health Care Professionals | Nurses | Other | p-Value | All | Physicians | Non-Physician/Non-Nurse Health Care Professionals | Nurses | Other | p-Value | |
| Lack of training and/or direct support for use | 34 (100) | 5 (14.7) | 24 (70.6) | 1 (2.9) | 4 (11.8) | 0.722 | 10 (100) | 7 (70.0) | 0 | 1 (10.0) | 2 (20.0) | 0.534 |
| Lack of usability of these technologies | 39 (100) | 9 (23.1) | 24 (61.5) | 1 (2.6) | 5 (12.8) | 0.068 | 3 (100) | 2 (66.7) | 0 | 0 | 1 (33.3) | 0.608 |
| Lack of interest in these technologies | 14 (100) | 3 (21.4) | 8 (57.1) | 1 (7.1) | 2 (14.3) | 0.600 | 3 (100) | 1 (33.3) | 1 (33.3) | 1 (33.3) | 0 | 0.522 |
| Additional workload | 43 (100) | 8 (18.6) | 28 (65.1) | 1 (2.3) | 6 (14.0) | 0.273 | 6 (100) | 2 (33.3) | 2 (33.3) | 1 (16.7) | 1 (16.7) | 0.393 |
| Lack of time | 21 (100) | 5 (23.8) | 13 (61.9) | 1 (4.8) | 2 (9.5) | 0.312 | 8 (100) | 4 (50.0) | 3 (37.5) | 1 (12.5) | 0 | 0.801 |
| Technical difficulties caused by being at a distance for certain tasks/exams | 67 (100) | 6 (9.0) | 54 (80.0) | 1 (1.5) | 6 (9.0) | NA | 5 (100) | 3 (60.0) | 2 (40.0) | 0 | 0 | 0.525 |
| Fear of a lack of confidentiality and of leaks of the information exchanged | 15 (100) | 3 (20.0) | 5 (33.3) | 0 | 7 (46.7) | NA | 3 (100) | 3 (100.00) | 0 | 0 | 0 | 0.678 |
| Dehumanization of the relationship with the patient | 30 (100) | 2 (6.7) | 17 (56.7) | 2 (6.67) | 9 (30.0) | 0.067 | 4 (100) | 0 | 0 | 0 | 0 | NA |
| Non-integration into our current technological systems and practices | 13 (100) | 2 (15.4) | 6 (46.2) | 0 | 5 (38.5) | 0.066 | 6 (100) | 1 (25.0) | 1 (25.0) | 1 (25.0) | 1 (25.0) | 0.608 |
| Other problems | 23 (100) | 3 (13.0) | 15 (65.2) | 0 | 5 (21.7) | 0.512 | 2 (100) | 5 (83.3) | 1 (16.7) | 0 | 0 | 0.721 |
| No problem encountered | 12 (100) | 1 (8.3) | 6 (50.0) | 1 (8.33) | 4 (33.3) | 0.225 | 2 (100) | 0 | 1 (50.0) | 1 (50.0) | 0 | 0.678 |
| I do not wish to answer/I do not know/Does not apply | 7 (100) | 0 | 3 (42.9) | 4 (57.1) | 0 | NA | 9 (100) | 1 (50.0) | 1 (50.0) | 0 | 0 | 0.522 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bouabida, K.; Malas, K.; Talbot, A.; Desrosiers, M.-È.; Lavoie, F.; Lebouché, B.; Taghizadeh, N.; Normandin, L.; Vialaron, C.; Fortin, O.; et al. Healthcare Professional Perspectives on the Use of Remote Patient-Monitoring Platforms during the COVID-19 Pandemic: A Cross-Sectional Study. J. Pers. Med. 2022, 12, 529. https://doi.org/10.3390/jpm12040529
Bouabida K, Malas K, Talbot A, Desrosiers M-È, Lavoie F, Lebouché B, Taghizadeh N, Normandin L, Vialaron C, Fortin O, et al. Healthcare Professional Perspectives on the Use of Remote Patient-Monitoring Platforms during the COVID-19 Pandemic: A Cross-Sectional Study. Journal of Personalized Medicine. 2022; 12(4):529. https://doi.org/10.3390/jpm12040529
Chicago/Turabian StyleBouabida, Khayreddine, Kathy Malas, Annie Talbot, Marie-Ève Desrosiers, Frédéric Lavoie, Bertrand Lebouché, Niloofar Taghizadeh, Louise Normandin, Cécile Vialaron, Olivier Fortin, and et al. 2022. "Healthcare Professional Perspectives on the Use of Remote Patient-Monitoring Platforms during the COVID-19 Pandemic: A Cross-Sectional Study" Journal of Personalized Medicine 12, no. 4: 529. https://doi.org/10.3390/jpm12040529