
Effectiveness of Digital Cognitive Behavioral Therapy for Insomnia in Young People: Preliminary Findings from Systematic Review and Meta-Analysis

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
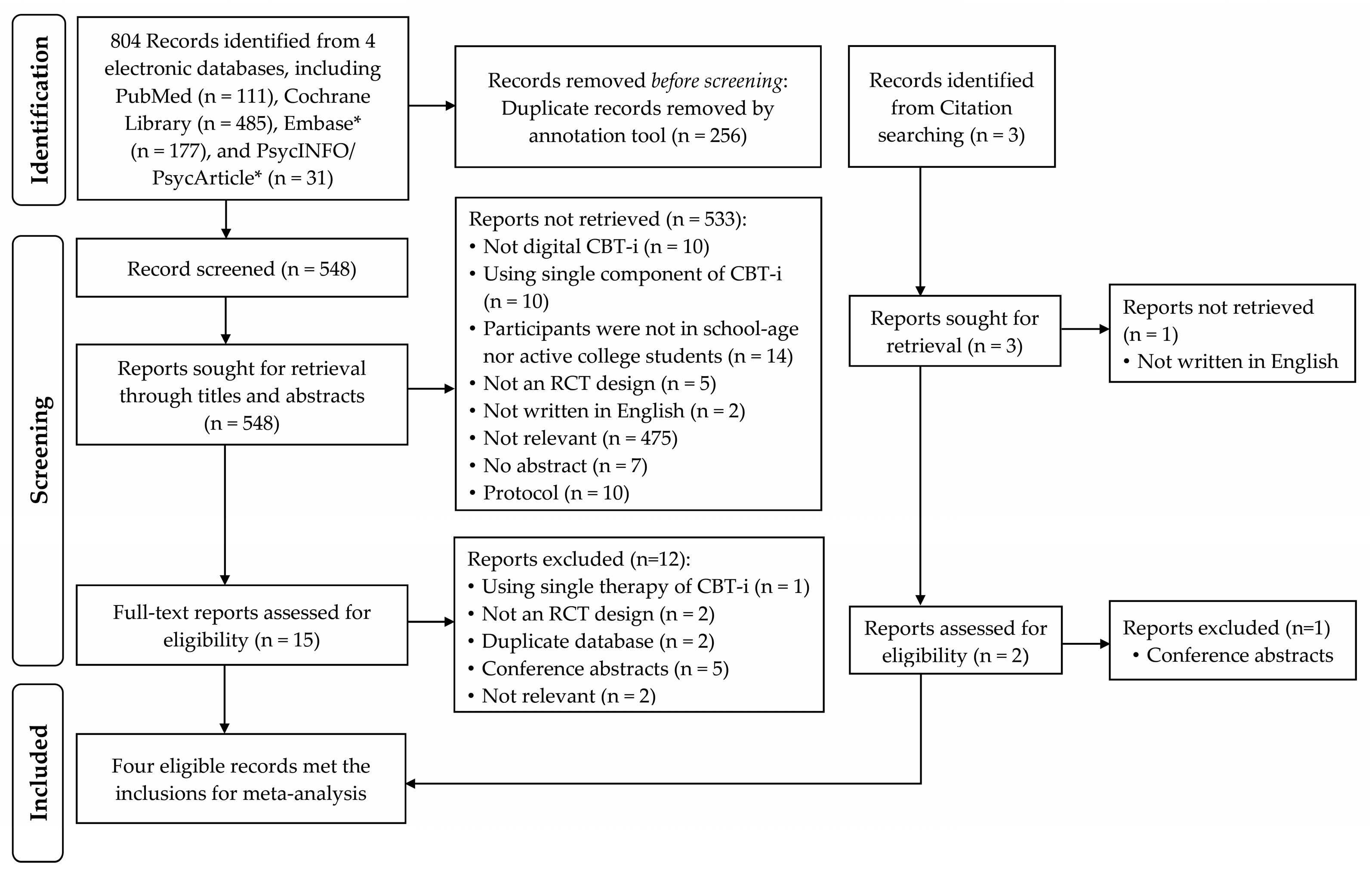
2.1. Search Strategy
2.2. Study Selection
2.3. Analytical Strategy
2.4. Quality Assessment
3. Results
3.1. Quality Assessments
3.2. Study Characteristics
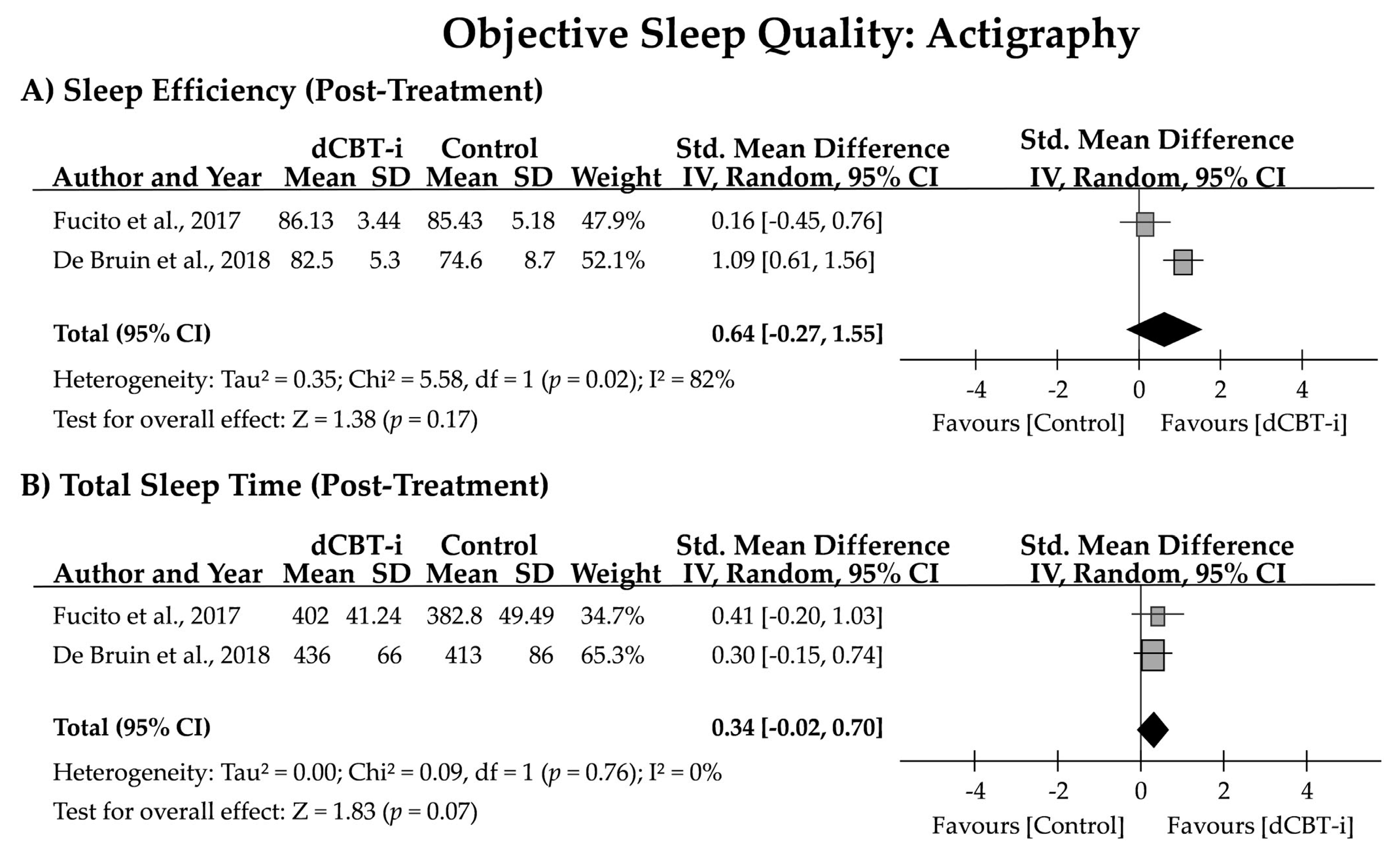
3.3. Short-Term and Long-Term Effects of dCBT-i
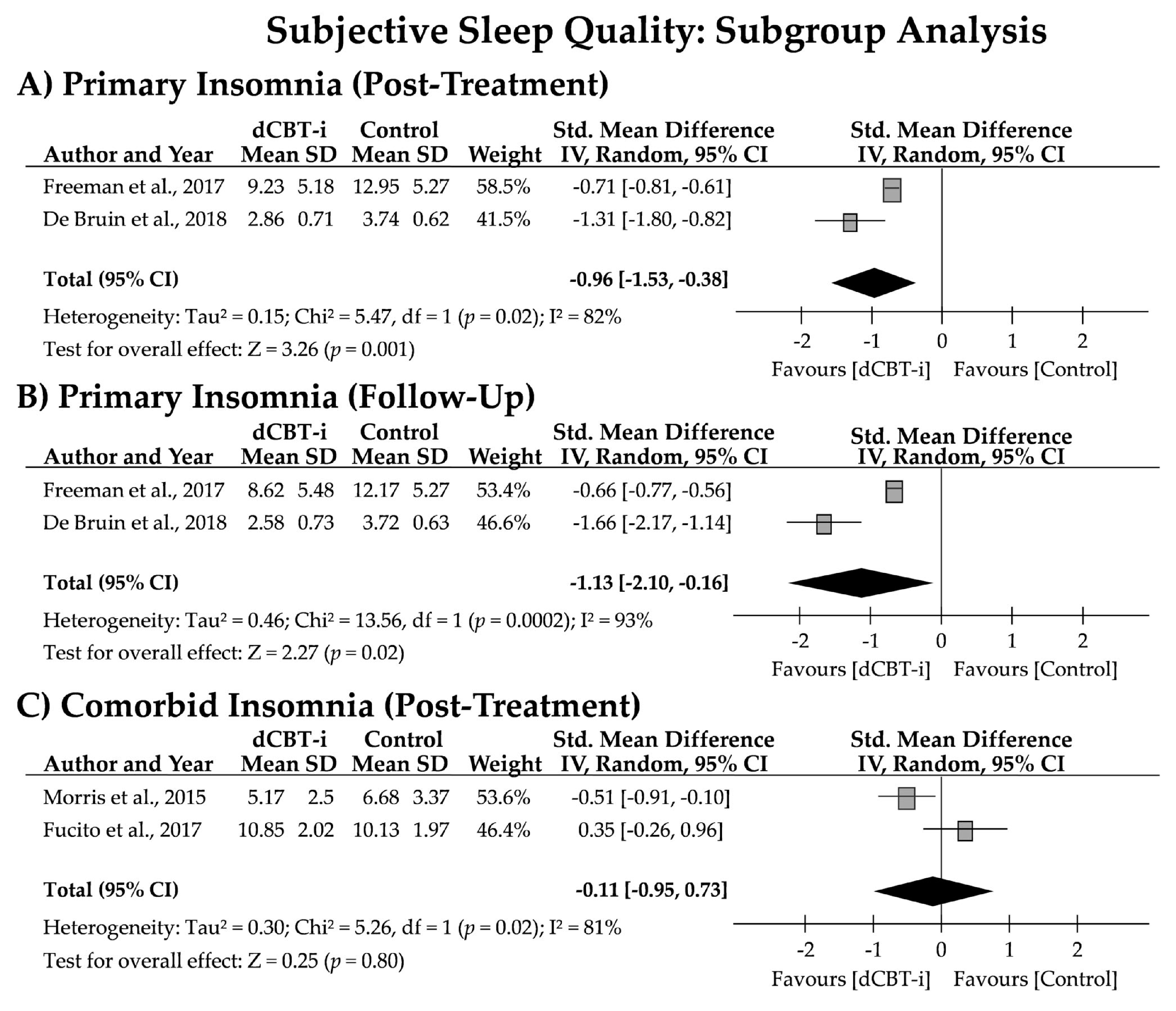
3.4. Effects of dCBT-i on Insomnia Subtypes
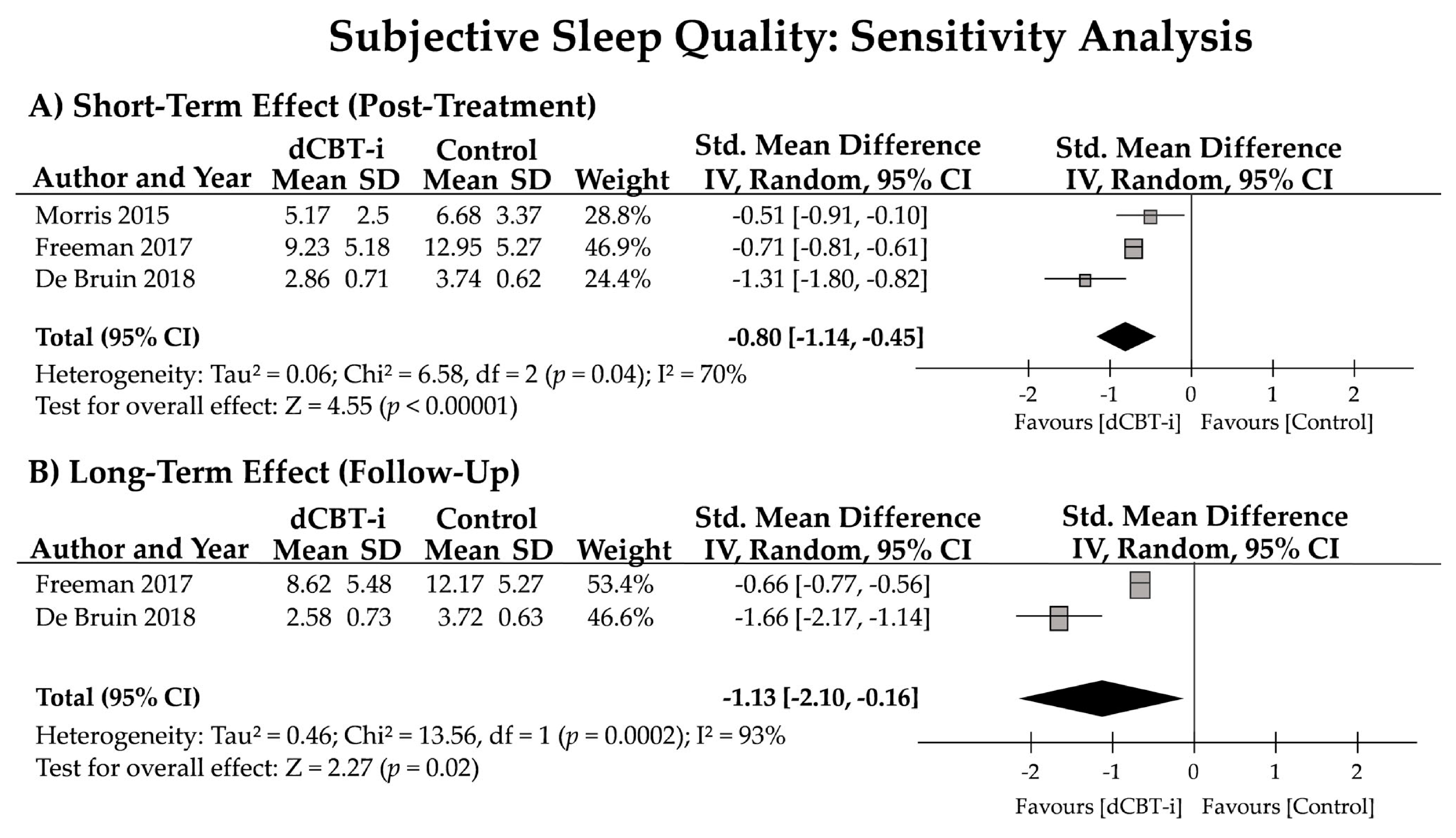
3.5. Sensitivity Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- De Zambotti, M.; Goldstone, A.; Colrain, I.M.; Baker, F.C. Insomnia Disorder in Adolescence: Diagnosis, Impact, and Treatment. Sleep Med. Rev. 2018, 39, 12–24. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar]
- Zhou, S.-J.; Wang, L.-L.; Yang, R.; Yang, X.-J.; Zhang, L.-G.; Guo, Z.-C.; Chen, J.-C.; Wang, J.-Q.; Chen, J.-X. Sleep Problems among Chinese Adolescents and Young Adults during the Coronavirus-2019 Pandemic. Sleep Med. 2020, 74, 39–47. [Google Scholar] [CrossRef] [PubMed]
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A New Instrument for Psychiatric Practice and Research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Morin, C.M.; Belleville, G.; Bélanger, L.; Ivers, H. The Insomnia Severity Index: Psychometric Indicators to Detect Insomnia Cases and Evaluate Treatment Response. Sleep 2011, 34, 601–608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marelli, S.; Castelnuovo, A.; Somma, A.; Castronovo, V.; Mombelli, S.; Bottoni, D.; Leitner, C.; Fossati, A.; Ferini-Strambi, L. Impact of COVID-19 Lockdown on Sleep Quality in University Students and Administration Staff. J. Neurol. 2020, 268, 8–15. [Google Scholar] [CrossRef] [PubMed]
- Sivertsen, B.; Harvey, A.G.; Lundervold, A.J.; Hysing, M. Sleep Problems and Depression in Adolescence: Results from a Large Population-Based Study of Norwegian Adolescents Aged 16–18 Years. Eur. Child Adolesc. Psychiatry 2014, 23, 681–689. [Google Scholar] [CrossRef]
- Alvaro, P.K.; Roberts, R.M.; Harris, J.K.; Bruni, O. The Direction of the Relationship between Symptoms of Insomnia and Psychiatric Disorders in Adolescents. J. Affect. Disord. 2017, 207, 167–174. [Google Scholar] [CrossRef]
- Becker, S.P.; Dvorsky, M.R.; Holdaway, A.S.; Luebbe, A.M. Sleep Problems and Suicidal Behaviors in College Students. J. Psychiatr. Res. 2018, 99, 122–128. [Google Scholar] [CrossRef]
- Navarro-Martínez, R.; Chover-Sierra, E.; Colomer-Pérez, N.; Vlachou, E.; Andriuseviciene, V.; Cauli, O. Sleep Quality and Its Association with Substance Abuse among University Students. Clin. Neurol. Neurosurg. 2020, 188, 105591. [Google Scholar] [CrossRef]
- Edinger, J.D.; Wohlgemuth, W.K.; Radtke, R.A.; Marsh, G.R.; Quillian, R.E. Cognitive Behavioral Therapy for Treatment of Chronic Primary Insomnia: A Randomized Controlled Trial. JAMA 2001, 285, 1856–1864. [Google Scholar] [CrossRef]
- Qaseem, A.; Kansagara, D.; Forciea, M.A.; Cooke, M.; Denberg, T.D.; Clinical Guidelines Committee of the American College of Physicians. Management of Chronic Insomnia Disorder in Adults: A Clinical Practice Guideline from the American College of Physicians. Ann. Intern. Med. 2016, 165, 125–133. [Google Scholar] [CrossRef] [PubMed]
- Edinger, J.D.; Arnedt, J.T.; Bertisch, S.M.; Carney, C.E.; Harrington, J.J.; Lichstein, K.L.; Sateia, M.J.; Troxel, W.M.; Zhou, E.S.; Kazmi, U.; et al. Behavioral and Psychological Treatments for Chronic Insomnia Disorder in Adults: An American Academy of Sleep Medicine Clinical Practice Guideline. J. Clin. Sleep Med. 2021, 17, 255–262. [Google Scholar] [CrossRef] [PubMed]
- Riemann, D.; Baglioni, C.; Bassetti, C.; Bjorvatn, B.; Dolenc Groselj, L.; Ellis, J.G.; Espie, C.A.; Garcia-Borreguero, D.; Gjerstad, M.; Gonçalves, M.; et al. European Guideline for the Diagnosis and Treatment of Insomnia. J. Sleep Res. 2017, 26, 675–700. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, M.D.; Gehrman, P.; Perlis, M.; Umscheid, C.A. Comparative Effectiveness of Cognitive Behavioral Therapy for Insomnia: A Systematic Review. BMC Fam. Pract. 2012, 13, 40. [Google Scholar] [CrossRef] [Green Version]
- Edinger, J.D.; Carney, C.E. Overcoming Insomnia: A Cognitive-Behavioral Therapy Approach, Therapist Guid, 2nd ed.; Oxford University Press: New York, NY, USA, 2014. [Google Scholar]
- Van Straten, A.; van der Zweerde, T.; Kleiboer, A.; Cuijpers, P.; Morin, C.M.; Lancee, J. Cognitive and Behavioral Therapies in the Treatment of Insomnia: A Meta-Analysis. Sleep Med. Rev. 2018, 38, 3–16. [Google Scholar] [CrossRef]
- Wu, J.Q.; Appleman, E.R.; Salazar, R.D.; Ong, J.C. Cognitive Behavioral Therapy for Insomnia Comorbid with Psychiatric and Medical Conditions: A Meta-Analysis. JAMA Intern. Med. 2015, 175, 1461–1472. [Google Scholar] [CrossRef] [Green Version]
- Geiger-Brown, J.M.; Rogers, V.E.; Liu, W.; Ludeman, E.M.; Downton, K.D.; Diaz-Abad, M. Cognitive Behavioral Therapy in Persons with Comorbid Insomnia: A Meta-Analysis. Sleep Med. Rev. 2015, 23, 54–67. [Google Scholar] [CrossRef]
- Schmitz, M.F. The ACP Guidelines for Treatment of Chronic Insomnia: The Challenge of Implementation. Behav. Sleep Med. 2016, 14, 699–700. [Google Scholar] [CrossRef]
- Koffel, E.; Bramoweth, A.D.; Ulmer, C.S. Increasing Access to and Utilization of Cognitive Behavioral Therapy for Insomnia (CBT-I): A Narrative Review. J. Gen. Intern. Med. 2018, 33, 955–962. [Google Scholar] [CrossRef] [Green Version]
- McCall, W.V. Cognitive Behavioral Therapy for Insomnia (CBT-I): What Is Known, and Advancing the Science by Avoiding the Pitfalls of the Placebo Effect. Sleep Med. Rev. 2018, 38, 1–2. [Google Scholar] [CrossRef]
- Buenaver, L.F.; Townsend, D.; Ong, J.C. Delivering Cognitive Behavioral Therapy for Insomnia in the Real World: Considerations and Controversies. Sleep Med. Clin. 2019, 14, 275–281. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.-G.; Kim, Y.-K. Cognitive Behavioral Therapy for Insomnia in the Digital Age. Adv. Exp. Med. Biol. 2019, 1192, 629–641. [Google Scholar] [CrossRef] [PubMed]
- Luik, A.I.; Kyle, S.D.; Espie, C.A. Digital Cognitive Behavioral Therapy (DCBT) for Insomnia: A State-of-the-Science Review. Curr. Sleep Med. Rep. 2017, 3, 48–56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zachariae, R.; Lyby, M.S.; Ritterband, L.M.; O’Toole, M.S. Efficacy of Internet-Delivered Cognitive-Behavioral Therapy for Insomnia—A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Sleep Med. Rev. 2016, 30, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Cheng, S.K.; Dizon, J. Computerised Cognitive Behavioural Therapy for Insomnia: A Systematic Review and Meta-Analysis. Psychother. Psychosom. 2012, 81, 206–216. [Google Scholar] [CrossRef]
- Dewald-Kaufmann, J.; de Bruin, E.; Michael, G. Cognitive Behavioral Therapy for Insomnia (CBT-i) in School-Aged Children and Adolescents. Sleep Med. Clin. 2019, 14, 155–165. [Google Scholar] [CrossRef]
- Werner-Seidler, A.; Johnston, L.; Christensen, H. Digitally-Delivered Cognitive-Behavioural Therapy for Youth Insomnia: A Systematic Review. Internet Interv. 2018, 11, 71–78. [Google Scholar] [CrossRef]
- Morris, J.; Firkins, A.; Millings, A.; Mohr, C.; Redford, P.; Rowe, A. Internet-Delivered Cognitive Behavior Therapy for Anxiety and Insomnia in a Higher Education Context. Anxiety Stress Coping 2015, 29, 415–431. [Google Scholar] [CrossRef] [Green Version]
- De Bruin, E.J.; Bögels, S.M.; Oort, F.J.; Meijer, A.M. Efficacy of Cognitive Behavioral Therapy for Insomnia in Adolescents: A Randomized Controlled Trial with Internet Therapy, Group Therapy and A Waiting List Condition. Sleep 2015, 38, 1913–1926. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Healthcare Interventions: Explanation and Elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. The Second Decade: Improving Adolescent Health and Development; (No. WHO/FRH/ADH/98.18 Rev. 1); World Health Organization: Geneva, Switzerland, 2001. [Google Scholar]
- American Academy of Sleep Medicine. International Classification of Sleep Disorders: Diagnostic and Coding Manual; American Academy of Sleep Medicine: Westchester, IL, USA, 2005; pp. 148–152. [Google Scholar]
- Higgins, J.P.T.; Thompson, S.G. Quantifying Heterogeneity in a Meta-Analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef] [PubMed]
- Deeks, J.; Higgins, J.; Altman, D.G. Chapter 10: Analysing Data and Undertaking Meta-Analyses. In Cochrane Handbook for Systematic Reviews of Interventions; Wiley Blackwell: Hoboken, NJ, USA, 2021. [Google Scholar]
- Hedges, L.V. Distribution Theory for Glass’s Estimator of Effect Size and Related Estimators. J. Educ. Stat. 1981, 6, 107–128. [Google Scholar] [CrossRef]
- Hedges, L.; Olkin, I. Statistical Methods for Meta-Analysis—1st Edition; Academic Press: New York, NY, USA, 1985. [Google Scholar]
- Lipsey, M.W.; Wilson, D.B. The Efficacy of Psychological, Educational, and Behavioral Treatment. Confirmation from Meta-Analysis. Am. Psychol. 1993, 48, 1181–1209. [Google Scholar] [CrossRef]
- Froud, R.; Eldridge, S.; Lall, R.; Underwood, M. Estimating the Number Needed to Treat from Continuous Outcomes in Randomised Controlled Trials: Methodological Challenges and Worked Example Using Data from the UK Back Pain Exercise and Manipulation (BEAM) Trial. BMC Med. Res. Methodol. 2009, 9, 35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kraemer, H.C.; Kupfer, D.J. Size of Treatment Effects and Their Importance to Clinical Research and Practice. Biol. Psychiatry 2006, 59, 990–996. [Google Scholar] [CrossRef] [PubMed]
- Freeman, D.; Sheaves, B.; Goodwin, G.M.; Yu, L.-M.; Nickless, A.; Harrison, P.J.; Emsley, R.; Luik, A.I.; Foster, R.G.; Wadekar, V.; et al. The Effects of Improving Sleep on Mental Health (OASIS): A Randomised Controlled Trial with Mediation Analysis. Lancet Psychiatry 2017, 4, 749–758. [Google Scholar] [CrossRef] [Green Version]
- Fucito, L.M.; DeMartini, K.S.; Hanrahan, T.H.; Yaggi, H.K.; Heffern, C.; Redeker, N.S. Using Sleep Interventions to Engage and Treat Heavy-Drinking College Students: A Randomized Pilot Study. Alcohol Clin. Exp. Res. 2017, 41, 798–809. [Google Scholar] [CrossRef] [Green Version]
- De Bruin, E.J.; Bögels, S.M.; Oort, F.J.; Meijer, A.M. Improvements of Adolescent Psychopathology after Insomnia Treatment: Results from a Randomized Controlled Trial over 1 Year. J. Child Psychol. Psychiatry 2018, 59, 509–522. [Google Scholar] [CrossRef]
- Espie, C.A.; Kyle, S.D.; Hames, P.; Gardani, M.; Fleming, L.; Cape, J. The Sleep Condition Indicator: A Clinical Screening Tool to Evaluate Insomnia Disorder. BMJ Open 2014, 4, e004183. [Google Scholar] [CrossRef]
- Krakow, B.J.; Melendrez, D.C.; Johnston, L.G.; Clark, J.O.; Santana, E.M.; Warner, T.D.; Hollifield, M.A.; Schrader, R.; Sisley, B.N.; Lee, S.A. Sleep Dynamic Therapy for Cerro Grande Fire Evacuees with Posttraumatic Stress Symptoms: A Preliminary Report. J. Clin. Psychiatry 2002, 63, 673–684. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, L.; Buysse, D.J.; Germain, A.; Moul, D.E.; Stover, A.; Dodds, N.E.; Johnston, K.L.; Pilkonis, P.A. Development of Short Forms from the PROMISTM Sleep Disturbance and Sleep-Related Impairment Item Banks. Behav. Sleep Med. 2011, 10, 6–24. [Google Scholar] [CrossRef] [PubMed]
- Kerkhof, G.A.; Geuke, M.E.H.; Brouwer, A.; Rijsman, R.M.; Schimsheimer, R.J.; Kasteel, V.V. Holland Sleep Disorders Questionnaire: A New Sleep Disorders Questionnaire Based on the International Classification of Sleep Disorders-2. J. Sleep Res. 2013, 22, 104–107. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, L.J.; Bisdounis, L.; Ballesio, A.; Omlin, X.; Kyle, S.D. The Impact of Cognitive Behavioural Therapy for Insomnia on Objective Sleep Parameters: A Meta-Analysis and Systematic Review. Sleep Med. Rev. 2019, 47, 90–102. [Google Scholar] [CrossRef] [PubMed]
- Vgontzas, A.N.; Fernandez-Mendoza, J.; Liao, D.; Bixler, E.O. Insomnia with Objective Short Sleep Duration: The Most Biologically Severe Phenotype of the Disorder. Sleep Med. Rev. 2013, 17, 241–254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vgontzas, A.N.; Liao, D.; Pejovic, S.; Calhoun, S.; Karataraki, M.; Basta, M.; Fernández-Mendoza, J.; Bixler, E.O. Insomnia with Short Sleep Duration and Mortality: The Penn State Cohort. Sleep 2010, 33, 1159–1164. [Google Scholar] [CrossRef]
- Li, Y.; Zhang, X.; Winkelman, J.W.; Redline, S.; Hu, F.B.; Stampfer, M.; Ma, J.; Gao, X. Association between Insomnia Symptoms and Mortality: A Prospective Study of U.S. Men. Circulation 2014, 129, 737–746. [Google Scholar] [CrossRef]
- De Almondes, K.M.; Costa, M.V.; Malloy-Diniz, L.F.; Diniz, B.S. Insomnia and Risk of Dementia in Older Adults: Systematic Review and Meta-Analysis. J. Psychiatr. Res. 2016, 77, 109–115. [Google Scholar] [CrossRef]
- Lund, H.G.; Rybarczyk, B.D.; Perrin, P.B.; Leszczyszyn, D.; Stepanski, E. The Discrepancy between Subjective and Objective Measures of Sleep in Older Adults Receiving CBT for Comorbid Insomnia. J. Clin. Psychol. 2013, 69, 1108–1120. [Google Scholar] [CrossRef] [Green Version]
- Cervena, K.; Dauvilliers, Y.; Espa, F.; Touchon, J.; Matousek, M.; Billiard, M.; Besset, A. Effect of Cognitive Behavioural Therapy for Insomnia on Sleep Architecture and Sleep EEG Power Spectra in Psychophysiological Insomnia. J. Sleep Res. 2004, 13, 385–393. [Google Scholar] [CrossRef]
- Hogan, S.E.; Delgado, G.M.; Hall, M.H.; Nimgaonkar, V.L.; Germain, A.; Buysse, D.J.; Wilckens, K.A. Slow-Oscillation Activity Is Reduced and High Frequency Activity Is Elevated in Older Adults with Insomnia. J. Clin. Sleep Med. 2020, 16, 1445–1454. [Google Scholar] [CrossRef] [PubMed]
- Krystal, A.D.; Edinger, J.D.; Wohlgemuth, W.K.; Marsh, G.R. NREM Sleep EEG Frequency Spectral Correlates of Sleep Complaints in Primary Insomnia Subtypes. Sleep 2002, 25, 630–640. [Google Scholar] [PubMed] [Green Version]
- Chen, P.-Y.; Jan, Y.-W.; Yang, C.-M. Are the Insomnia Severity Index and Pittsburgh Sleep Quality Index Valid Outcome Measures for Cognitive Behavioral Therapy for Insomnia? Inquiry from the Perspective of Response Shifts and Longitudinal Measurement Invariance in Their Chinese Versions. Sleep Med. 2017, 35, 35–40. [Google Scholar] [CrossRef] [PubMed]
- Hartmann, J.A.; Carney, C.E.; Lachowski, A.; Edinger, J.D. Exploring the Construct of Subjective Sleep Quality in Patients with Insomnia. J. Clin. Psychiatry 2015, 76, e768–e773. [Google Scholar] [CrossRef]
- Ebner-Priemer, U.W.; Kuo, J.; Welch, S.S.; Thielgen, T.; Witte, S.; Bohus, M.; Linehan, M.M. A Valence-Dependent Group-Specific Recall Bias of Retrospective Self-Reports: A Study of Borderline Personality Disorder in Everyday Life. J. Nerv. Ment. Dis. 2006, 194, 774–779. [Google Scholar] [CrossRef]
- Perez-Pozuelo, I.; Zhai, B.; Palotti, J.; Mall, R.; Aupetit, M.; Garcia-Gomez, J.M.; Taheri, S.; Guan, Y.; Fernandez-Luque, L. The Future of Sleep Health: A Data-Driven Revolution in Sleep Science and Medicine. NPJ Digit. Med. 2020, 3, 42. [Google Scholar] [CrossRef]
- Torous, J.; Onnela, J.-P.; Keshavan, M. New Dimensions and New Tools to Realize the Potential of RDoC: Digital Phenotyping via Smartphones and Connected Devices. Transl. Psychiatry 2017, 7, e1053. [Google Scholar] [CrossRef]
- Sequeira, L.; Battaglia, M.; Perrotta, S.; Merikangas, K.; Strauss, J. Digital Phenotyping with Mobile and Wearable Devices: Advanced Symptom Measurement in Child and Adolescent Depression. J. Am. Acad. Child Adolesc. Psychiatry 2019, 58, 841–845. [Google Scholar] [CrossRef]
- Korkalainen, H.; Nikkonen, S.; Kainulainen, S.; Dwivedi, A.K.; Myllymaa, S.; Leppänen, T.; Töyräs, J. Self-Applied Home Sleep Recordings: The Future of Sleep Medicine. Sleep Med. Clin. 2021, 16, 545–556. [Google Scholar] [CrossRef]
- Schwartz, A.R.; Cohen-Zion, M.; Pham, L.V.; Gal, A.; Sowho, M.; Sgambati, F.P.; Klopfer, T.; Guzman, M.A.; Hawks, E.M.; Etzioni, T.; et al. Brief Digital Sleep Questionnaire Powered by Machine Learning Prediction Models Identifies Common Sleep Disorders. Sleep Med. 2020, 71, 66–76. [Google Scholar] [CrossRef]
- Ge, F.; Zhang, D.; Wu, L.; Mu, H. Predicting Psychological State Among Chinese Undergraduate Students in the COVID-19 Epidemic: A Longitudinal Study Using a Machine Learning. Neuropsychiatr. Dis. Treat. 2020, 16, 2111–2118. [Google Scholar] [CrossRef] [PubMed]
- Alghwiri, A.A.; Almomani, F.; Alghwiri, A.A.; Whitney, S.L. Predictors of Sleep Quality among University Students: The Use of Advanced Machine Learning Techniques. Sleep Breath. 2021, 25, 1119–1126. [Google Scholar] [CrossRef]
- Philip, P.; Dupuy, L.; Morin, C.M.; de Sevin, E.; Bioulac, S.; Taillard, J.; Serre, F.; Auriacombe, M.; Micoulaud-Franchi, J.-A. Smartphone-Based Virtual Agents to Help Individuals with Sleep Concerns During COVID-19 Confinement: Feasibility Study. J. Med. Internet. Res. 2020, 22, e24268. [Google Scholar] [CrossRef] [PubMed]
- Barnett, I.; Torous, J.; Staples, P.; Sandoval, L.; Keshavan, M.; Onnela, J.-P. Relapse Prediction in Schizophrenia through Digital Phenotyping: A Pilot Study. Neuropsychopharmacology 2018, 43, 1660–1666. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thurzo, A.; Kurilová, V.; Varga, I. Artificial Intelligence in Orthodontic Smart Application for Treatment Coaching and Its Impact on Clinical Performance of Patients Monitored with AI-TeleHealth System. Healthcare 2021, 9, 1695. [Google Scholar] [CrossRef]
- Espie, C.A. “Stepped Care”: A Health Technology Solution for Delivering Cognitive Behavioral Therapy as a First Line Insomnia Treatment. Sleep 2009, 32, 1549–1558. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Random Sequence Generation (Selection Bias) | Allocation Concealment (Selection Bias) | Blinding of Participants | Blinding of Outcome Assessment (Detection Bias) | Incomplete Outcome Data (Attrition Bias) | Selective Reporting (Reporting Bias) | |
|---|---|---|---|---|---|---|
| Morris et al., 2015 [30] | + | + | + | + | + | ? |
| Freeman et all., 2017 [43] | + | + | + | + | + | + |
| Fucito et al., 2017 [44] | + | + | + | + | + | + |
| De Bruin et al., 2018 [45] | + | + | + | + | + | + |
| Author (Year) Location | Sample Size (F%) Mean Age (SD) | Recruitment Population | Group Allocation: Completed at Posttreatment (Dropout N.) | Therapy Delivery | Components of dCBT-i | Sleep-Related Outcomes |
|---|---|---|---|---|---|---|
| Morris et al. (2015) [30] UK | dCBT-i: N = 48 (60%) 20.69 ± 2.61 y/o WC: N = 47 (70%) 20.27 ± 1.56 y/o | Undergraduate students at the University of Bristol who want to learn stress management | dCBT-i: 36 (12) WC: 44 (3) | “Insomnia-relief” 7 modules; 6 weeks; text- and email-reminder sent weekly | SH, SC, SR, RT, PE | PSQI * |
| Freeman et al. (2017) [43] UK | dCBT-i: N = 1891 (72%) 24.8 ± 7.7 y/o WC: N = 1864 (71%) 24.6 ± 7.6 y/o | University students from 26 universities in the UK who were with insomnia; SCI ≤ 16 | dCBT-i: 733 (1158) WC: 1142 (722) | “Sleepio” 6 sessions, on average, of 20 min; weekly; web-based or via smartphone; email- or text-reminder sent to delayed responders | SH, SC, SR, RT, PE, CT | ISI * SCI-8 DDNSI |
| Fucito et al. (2017) [44] USA | dCBT-i: N = 21 (48%) 20.71 ± 1.42 y/o HC: N = 21 (48%) 20.33 ± 1.2 y/o | Undergraduate students with heavy-drinking and concern about sleep | dCBT-i: 19 (2) HC: 19 (2) | “Call it a Night” 4 modules; weekly; web-based; email reminder sent daily | SH, SC, RT, PE, CT | PSQI * PROMIS-SRI-SF Actigraphy * |
| De Bruin et al. (2018) [45] The Netherlands | dCBT-i: N = 39 (85%) 15.3 ± 1.4 y/o WC: N = 39 (72%) 15.9 ± 1.6 y/o | 12–19 y/o adolescents who met DSM-V insomnia criteria; medication-free | dCBT-i: 38 (1) WC: 39 (0) | dCBT-i 6 weeks; 90 min per session; web-based; 15 min online chat with therapist; text reminder sent to delayed responders | SH, SC, SR, RT, PE, CT | Sleep Diary HSDQi * Actigraphy * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsai, H.-J.; Yang, A.C.; Zhu, J.-D.; Hsu, Y.-Y.; Hsu, T.-F.; Tsai, S.-J. Effectiveness of Digital Cognitive Behavioral Therapy for Insomnia in Young People: Preliminary Findings from Systematic Review and Meta-Analysis. J. Pers. Med. 2022, 12, 481. https://doi.org/10.3390/jpm12030481
Tsai H-J, Yang AC, Zhu J-D, Hsu Y-Y, Hsu T-F, Tsai S-J. Effectiveness of Digital Cognitive Behavioral Therapy for Insomnia in Young People: Preliminary Findings from Systematic Review and Meta-Analysis. Journal of Personalized Medicine. 2022; 12(3):481. https://doi.org/10.3390/jpm12030481
Chicago/Turabian StyleTsai, Hsin-Jung, Albert C. Yang, Jun-Ding Zhu, Yu-Yun Hsu, Teh-Fu Hsu, and Shih-Jen Tsai. 2022. "Effectiveness of Digital Cognitive Behavioral Therapy for Insomnia in Young People: Preliminary Findings from Systematic Review and Meta-Analysis" Journal of Personalized Medicine 12, no. 3: 481. https://doi.org/10.3390/jpm12030481