
Emergency Department Overcrowding: Understanding the Factors to Find Corresponding Solutions

 ,
,  , ,
, ,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
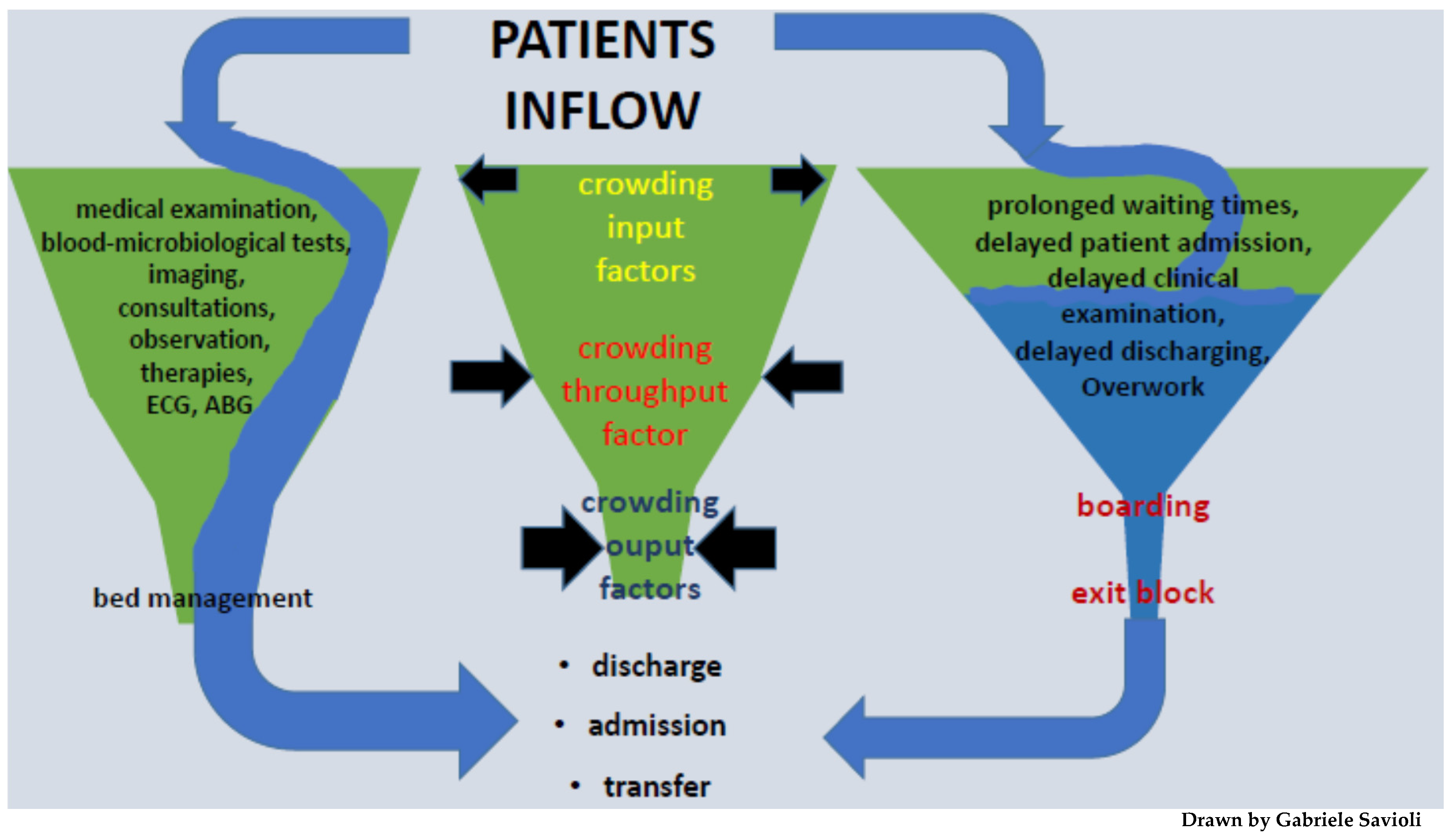
3. Overcrowding: The Input–Throughput–Output Model
- -
- Input factors: they are represented by factors determining patient access to the ED. They include the waiting time, the number of patients which arrived in the ED, as well as their severity and complexity. Input factors constitute one of the causes of crowding, but the least important [5,27,28,29,30,31]
- -
- Throughput factors (internal factors): they are represented by the process time, meaning the time between taking charge of the patient and the outcome (diagnosis and decision: discharge, hospitalization, and transfer). They include all the complementary exams that are performed in the ED (laboratory analysis and imaging). These factors are also affected by the healthcare personnel (in terms of quality of work, shift work, burnout, drop in performance, respect for shifts, and holidays) [3,6].
- -
- Output factors: they include patients boarding in the ED, availability of hospital beds, and the delay of transport (both internal and external) to leave the ED. The lack of hospital beds appears to be a fundamental cause of overcrowding, but so is the lack of home care. The reduction of beds (which in some realities have decreased by more than 50% in the last 20 years) is a worldwide phenomenon that has led to exit block, as well as to the collapse of the possibility of hospitalizing patients. Considering output factors, it is therefore evident that overcrowding is influenced by the fact that patients who should go to the ward are stationed in the emergency room and must continue to be assisted from a medical point of view [3,5,6].
- -
- -
- -
- Boarding has a great importance among the causative factors of overcrowding. Boarding is in fact capable of causing a considerable dissipation of resources, which are subtracted from new patients. These resources include space, beds, diagnostic imaging techniques, but also human resources, such as hospital staff. This generates an increase in LOS and negatively affects the output factors, perpetuating the maintenance of overcrowding [23,34,35] A great number of studies provide solutions to limit boarding, although this does not represent the only causative factor of overcrowding, but its resolution would seem mandatory to limit the phenomenon [21].
- -
- Exit block has a strong impact on overcrowding and is directly connected with the output factors. The solutions that can be promoted to alleviate exit block; however, they must not affect the patients’ outcome [36].
4. Signs of Overcrowding
- -
- delay in the treatment of patients due to a lack of suitable spaces
- -
- treatments administered in other spaces of the ED, including corridors
- -
- prolonged stay of patients in the emergency room at the end of medical treatment, pending transfer to the ward
- -
- inability to take care of patients transported by ambulance
- -
- obstruction of the entry and exit routes of the ED.
5. Exit Block: Definition
6. Boarding: Definition
7. The Access Block: Definition
8. Overcrowding: Consequences
9. Overcrowding and COVID Pandemic
10. Overcrowding: Possible Solutions
10.1. Microlevel Strategies
10.2. Macrolevel Strategies
11. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Di Somma, S.; Paladino, L.; Vaughan, L.; Lalle, I.; Magrini, L.; Magnanti, M. Overcrowding in emergency department: An international issue. Intern Emerg. Med. 2015, 10, 171–175. [Google Scholar] [CrossRef] [PubMed]
- Salway, R.; Valenzuela, R.; Shoenberger, J.; Mallon, W.; Viccellio, A. Emergency Department (ED) overcrowding: Evidence-based answers to frequently asked questions. Rev. Méd. Clínica Las Condes 2017, 28, 213–219. [Google Scholar] [CrossRef]
- Savioli, G.; Ceresa, I.F.; Novelli, V.; Ricevuti, G.; Bressan, M.A.; Oddone, E. How the coronavirus disease 2019 pandemic changed the patterns of healthcare utilization by geriatric patients and the crowding: A call to action for effective solutions to the access block. Intern. Emerg. Med. 2021, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Pitts, S.R.; Pines, J.M.; Handrigan, M.T.; Kellermann, A.L. National trends in emergency department occupancy, 2001 to 2008: Effect of inpatient admissions versus emergency department practice intensity. Ann Emerg Med. 2012, 60, 679–686.e3. [Google Scholar] [CrossRef] [PubMed]
- Richardson, D.B.; Mountain, D. Myths versus facts in emergency department overcrowding and hospital access block. Med. J. Aust. 2009, 190, 369–374. [Google Scholar] [CrossRef] [PubMed]
- Savioli, G.; Ceresa, I.; Guarnone, R.; Muzzi, A.; Novelli, V.; Ricevuti, G.; Iotti, G.; Bressan, M.; Oddone, E. Impact of Coronavirus Disease 2019 Pandemic on Crowding: A Call to Action for Effective Solutions to “Access Block”. West. J. Emerg. Med. 2021, 22, 860–870. [Google Scholar] [CrossRef]
- Emergency Medicine Practice Commitee, ACEP. Emergency Department Overcrowding: High Impact Solutions; ACEP: Irving, TX, USA, 2016. [Google Scholar]
- Australasian College for Emergency. Medicine Position Statement; Australasian College for Emergency: Melbourne, Australia, 2019. [Google Scholar]
- Australasian College for Emergency Medicine. P02 Policy on Standard Terminology; ACEM: Melbourne, Australia, 2014. [Google Scholar]
- Solberg, L.I.; Asplin, B.R.; Weinick, R.M.; Magid, D.J. Emergency department crowding: Consensus development of potential measures. Ann. Emerg. Med. 2003, 42, 824–834. [Google Scholar] [CrossRef]
- Pines, J.M. Emergency Department Crowding in California: A Silent Killer? Ann. Emerg. Med. 2013, 61, 612–614. [Google Scholar] [CrossRef]
- Ackroyd-Stolarz, S.; Guernsey, J.R.; MacKinnon, N.J.; Kovacs, G. The association between a prolonged stay in the emergency department and adverse events in older patients admitted to hospital: A retrospective cohort study. BMJ Qual. Saf. 2011, 20, 564–569. [Google Scholar] [CrossRef]
- Hong, K.J.; Shin, S.D.; Song, K.J.; Cha, W.C.; Cho, J.S. Association between ED crowding and delay in resuscitation effort. Am. J. Emerg. Med. 2013, 31, 509–515. [Google Scholar] [CrossRef]
- Pines, J.M.; Pollack, C.V., Jr.; Diercks, D.B.; Chang, A.M.; Shofer, F.S.; Hollander, J. The Association Between Emergency Department Crowding and Adverse Cardiovascular Outcomes in Patients with Chest Pain. Acad. Emerg. Med. 2009, 16, 617–625. [Google Scholar] [CrossRef] [PubMed]
- Pines, J.M.; Shofer, F.S.; Isserman, J.A.; Abbuhl, S.B.; Mills, A. The Effect of Emergency Department Crowding on Analgesia in Patients with Back Pain in Two Hospitals. Acad. Emerg. Med. 2010, 17, 276–283. [Google Scholar] [CrossRef] [PubMed]
- van der Linden, M.C.; Meester, B.E.; van der Linden, N. Emergency department crowding affects triage processes. Int. Emerg. Nurs. Nov. 2016, 29, 27–31. [Google Scholar] [CrossRef] [PubMed]
- Fitzgerald, G.; Jelinek, G.A.; Scott, D.; Gerdtz, M.F. Emergency department triage revisited. Emerg. Med. J. 2010, 27, 86–92. [Google Scholar] [CrossRef] [Green Version]
- Göransson, K.E.; Ehrenberg, A.; Marklund, B.; Ehnfors, M. Emergency department triage: Is there a link between nurses’ personal characteristics and accuracy in triage decisions? Accid. Emerg. Nurs. 2006, 14, 83–88. [Google Scholar] [CrossRef]
- Carter, E.J.; Pouch, S.M.; Larson, E.L. The Relationship Between Emergency Department Crowding and Patient Outcomes: A Systematic Review. J. Nurs. Sch. 2014, 46, 106–115. [Google Scholar] [CrossRef] [Green Version]
- American College of Emergency Physicians (ACEP). Crowding. Policy statement. Ann Emerg Med. 2013, 61, 726–727. [Google Scholar] [CrossRef]
- Kenny, J.F.; Chang, B.C.; Hemmert, K.C. Factors Affecting Emergency Department Crowding. Emerg. Med. Clin. North Am. 2020, 38, 573–587. [Google Scholar] [CrossRef]
- Rabin, E.; Kocher, K.; McClelland, M.; Pines, J.; Hwang, U.; Rathlev, N.; Asplin, B.; Trueger, N.S.; Weber, E. Solutions to Emergency Department ‘Boarding’ And Crowding Are Underused and May Need to Be Legislated. Health Aff. 2012, 31, 1757–1766. [Google Scholar] [CrossRef]
- Office USGA. Hospital Emergency Departments: Crowding Continues to Occur, and Some Patients Wait Longer than Recommended Time Frames. Available online: https://www.gao.gov/products/gao-09-347 (accessed on 12 December 2021).
- Asplin, B.R.; Magid, D.J.; Rhodes, K.V.; Solberg, L.I.; Lurie, N.; Camargo, C.A., Jr. A conceptual model of emergency department crowding. Ann. Emerg. Med. 2003, 42, 173–180. [Google Scholar] [CrossRef]
- Rathlev, N.K.; Chessare, J.; Olshaker, J.; Obendorfer, D.; Mehta, S.D.; Rothenhaus, T.; Crespo, S.; Magauran, B.; Davidson, K.; Shemin, R.; et al. Time Series Analysis of Variables Associated with Daily Mean Emergency Department Length of Stay. Ann. Emerg. Med. 2007, 49, 265–271. [Google Scholar] [CrossRef] [PubMed]
- Hoot, N.R.; Aronsky, D. Systematic Review of Emergency Department Crowding: Causes, Effects, and Solutions. Ann. Emerg. Med. 2008, 52, 126–136.e1. [Google Scholar] [CrossRef] [PubMed]
- Nagree, Y.; Ercleve, T.N.O.; Sprivulis, P.C. After-hours general practice clinics are unlikely to reduce low acuity patient attendances to metropolitan Perth emergency departments. Aust. Health Rev. 2004, 28, 285–291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dent, A.W.; Phillips, G.; Chenhall, A.J.; McGregor, L.R. The heaviest repeat users of an inner city emergency department are not general practice patients. Emerg. Med. 2003, 15, 322–329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sprivulis, P. Estimation of the general practice workload of a metropolitan teaching hospital emergency department. Emerg. Med. 2003, 15, 32–37. [Google Scholar] [CrossRef]
- Colineaux, H.; Pelissier, F.; Pourcel, L.; Lang, T.; Kelly-Irving, M.; Azema, O.; Charpentier, S.; Lamy, S. Why are people increasingly attending the emergency department? A study of the French healthcare system. Emerg. Med. J. 2019, 36, 548–553. [Google Scholar] [CrossRef]
- Hwang, U.; McCarthy, M.L.; Aronsky, D.; Asplin, B.; Crane, P.W.; Craven, C.K.; Epstein, S.K.; Fee, C.; Handel, D.A.; Pines, J.M.; et al. Measures of Crowding in the Emergency Department: A Systematic Review. Acad. Emerg. Med. 2011, 18, 527–538. [Google Scholar] [CrossRef]
- Institute of Medicine of the National Academies. Hospital-Based Emergency Care: At the Breaking Point; The National Academies Press: Washington, DC, USA, 2007; 424p, Available online: https://www.nap.edu/catalog/11621/hospital-based-emergency-care-at-the-breaking-point (accessed on 12 December 2021).
- Sayah, A.; Rogers, L.; Devarajan, K.; Kingsley-Rocker, L.; Lobon, L.F.; Minimizing, E.D. Waiting Times and Improving Patient Flow and Experience of Care. Emerg. Med. Int. 2014, 2014, 981472. [Google Scholar] [CrossRef] [Green Version]
- Derose, S.F.; Gabayan, G.Z.; Chiu, V.Y.; Yiu, S.C.; Sun, B.C. Emergency Department Crowding Predicts Admission Length-of-Stay but Not Mortality in a Large Health System. Med. Care 2014, 52, 602–611. [Google Scholar] [CrossRef] [Green Version]
- Nippak, P.M.D.; Isaac, W.W.; Ikeda-Douglas, C.J.; Marion, A.M.; Vandenbroek, M. Is there a relation between emergency department and inpatient lengths of stay? Can. J. Rural Med. 2014, 19, 12–20. [Google Scholar]
- Mason, S.; Knowles, E.; Boyle, A. Exit block in emergency departments: A rapid evidence review. Emerg. Med. J. 2016, 34, 46–51. [Google Scholar] [CrossRef] [PubMed]
- Celenza, T.; Bharath, J.; Scop, J. Attitudes toward careers in emergency medicine. EMA Emerg. Med. Australas 2012, 24, 11. [Google Scholar]
- Jelinek, G.A.; Weiland, T.J.; Mackinlay, C. Supervision and feedback for junior medical staff in Australian emergency departments: Findings from the emergency medicine capacity assessment study. BMC Med. Educ. 2010, 10, 74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fatovich, D.; Hirsch, R. Entry overload, emergency department overcrowding, and ambulance bypass. Emerg. Med. J. 2003, 20, 406–409. [Google Scholar] [CrossRef] [Green Version]
- Forero, R.; Hillman, K. Access Block and Overcrowding: A Literature Review. Prepared for the Australasian College for Emergency Medicine; University of New South Wales: Liverpool, NSW, Australia, 2003. [Google Scholar]
- Gilligan, P.; Winder, S.; Ramphul, N.; O'kelly, P. The Referral and Complete Evaluation Time Study. Eur. J. Emerg. Med. 2010, 17, 349–353. [Google Scholar] [CrossRef] [PubMed]
- Richardson, D.; McMahon, K.L. Emergency department access block occupancy predicts delay to surgery in patients with fractured neck of femur. Emerg. Med. Australas 2009, 21, 304–308. [Google Scholar] [CrossRef]
- Jelinek, G.; Mackinlay, C.; Weiland, T.; Hill, N.; Gerdtz, M. Barriers to the operation of mental health legislation in Australian emergency departments: A qualitative analysis. J. Law Med. 2011, 18, 716–723. [Google Scholar]
- Hossain, L.; Guan, D.C.K. Modelling coordination in hospital emergency departments through social network analysis. Disasters 2011, 36, 338–364. [Google Scholar] [CrossRef]
- Ye, L.; Zhou, G.; He, X.; Shen, W.; Gan, J.; Zhang, M. Prolonged length of stay in the emergency department in high-acuity patients at a Chinese tertiary hospital. Emerg. Med. Australas 2012, 24, 634–640. [Google Scholar] [CrossRef]
- Khanna, S.; Boyle, J.; Good, N.; Lind, J. Early discharge and its effect on ED length of stay and access block. Stud. Health Technol. Inform. 2012, 178, 92–98. [Google Scholar]
- Richardson, D. Relationship between inpatient hospital bed occupancy and ED performance. EMA Emerg. Med. Australas 2011, 23, 35. [Google Scholar]
- Martin, M.; Champion, R.; Kinsman, L.; Masman, K. Mapping patient flow in a regional Australian emergency department: A model driven approach. Int. Emerg. Nurs. 2011, 19, 75–85. [Google Scholar] [CrossRef] [PubMed]
- Definition of Boarded Patient. Available online: https://www.acep.org/patient-care/policy-statements/definition-of-boarded-patient/ (accessed on 13 December 2021).
- CENA (College of Emergency Nursing Australasia). Emergency Department Overcrowding and Access Block; CENA Position Statement: Liverpool, Australia, 2018. [Google Scholar]
- Laam, L.A.; Wary, A.A.; Strony, R.S.; Fitzpatrick, M.H.; Kraus, C.K. Quantifying the impact of patient boarding on emergency department length of stay: All admitted patients are negatively affected by boarding. J. Am. Coll. Emerg. Physicians Open 2021, 2, e12401. [Google Scholar] [CrossRef] [PubMed]
- Richardson, D. Access Block Point Prevalence Survey. Carried Out by the Road Trauma and Emergency Medicine Unit, Australian National University on behalf of the Australasian College for Emergency Medicine; ACEM: Melbourne, Australia, 2009. [Google Scholar]
- Plunkett, P.K.; Byrne, D.G.; Breslin, T.; Bennett, K.; Silke, B. Increasing wait times predict increasing mortality for emergency medical admissions. Eur. J. Emerg. Med. 2011, 18, 192–196. [Google Scholar] [CrossRef] [PubMed]
- Gilligan, P.; Winder, S.; O’Kelly, P. The reduce (reducing emergency department utilisation and crowding efforts) study. Acad. Emerg. Med. 2012, 19, 756. [Google Scholar]
- Carr, B.G.; Hollander, J.E.; Baxt, W.G.; Datner, E.M.; Pines, J.M. Trends in Boarding of Admitted Patients in US Emergency Departments 2003–2005. J. Emerg. Med. 2010, 39, 506–511. [Google Scholar] [CrossRef] [PubMed]
- Forero, R.; McCarthy, S.; Hillman, K. Access block and emergency department overcrowding. Crit. Care 2011, 15, 216. [Google Scholar] [CrossRef] [Green Version]
- Sklar, D.P.; Handel, D.A.; Hoekstra, J.; Baren, J.M.; Zink, B.; Hedges, J.R. The Future of Emergency Medicine: An Evolutionary Perspective. Acad. Med. 2010, 85, 490–495. [Google Scholar] [CrossRef]
- Braitberg, G. Emergency department overcrowding: Dying to get in? Med. J. Aust. 2007, 187, 624–625. [Google Scholar] [CrossRef]
- Forero, R.; Hillman, K.M.; McCarthy, S.; Fatovich, D.M.; Joseph, A.P.; Richardson, D.B. Access block and ED overcrowding. Emerg. Med. Australas 2010, 22, 119–135. [Google Scholar] [CrossRef]
- Walters, E.H.; Dawson, D.J. Whole-of-hospital response to admission access block: The need for a clinical revolution. Med. J. Aust. 2009, 191, 561–563. [Google Scholar] [CrossRef] [PubMed]
- Scott, I.; Vaughan, L.; Bell, D. Effectiveness of acute medical units in hospitals: A systematic review. Int. J. Qual. Health Care 2009, 21, 397–407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cha, W.C.; Shin, S.D.; Cho, J.S.; Song, K.J.; Singer, A.J.; Kwak, Y.H. The Association Between Crowding and Mortality in Admitted Pediatric Patients from Mixed Adult-Pediatric Emergency Departments in Korea. Pediatr. Emerg. Care 2011, 27, 1136–1141. [Google Scholar] [CrossRef] [PubMed]
- Guttmann, A.; Schull, M.J.; Vermeulen, M.J.; Stukel, T.A. Association between waiting times and short term mortality and hospital admission after departure from emergency department: Population based cohort study from Ontario, Canada. BMJ 2011, 342, d2983. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Richardson, D.B. Increase in patient mortality at 10 days associated with emergency department overcrowding. Med. J. Aust. 2006, 184, 213–216. [Google Scholar] [CrossRef]
- Polevoi, S.K.; Quinn, J.V.; Kramer, N.R. Factors associated with patients who leave without being seen. Acad. Emerg. Med. 2005, 12, 232–236. [Google Scholar] [CrossRef]
- Weiss, S.J.; Ernst, A.A.; Derlet, R.; King, R.; Bair, A.; Nick, T.G. Relationship between the National ED Overcrowding Scale and the number of patients who leave without being seen in an academic ED. Am. J. Emerg. Med. 2005, 23, 288–294. [Google Scholar] [CrossRef]
- Vieth, T.L.; Rhodes, K.V. The effect of crowding on access and quality in an academic ED. Am. J. Emerg. Med. 2006, 24, 787–794. [Google Scholar] [CrossRef]
- Asaro, P.V.; Lewis, L.M.; Boxerman, S.B. Emergency department overcrowding: Analysis of the factors of renege rate. Acad. Emerg. Med. 2007, 14, 157–162. [Google Scholar] [CrossRef]
- Kulstad, E.B.; Hart, K.M.; Waghchoure, S. Occupancy Rates and Emergency Department Work Index Scores Correlate with Leaving Without Being Seen. West. J. Emerg. Med. 2010, 11, 324–328. [Google Scholar]
- Schull, M.J.; Vermeulen, M.; Slaughter, G.; Morrison, L.; Daly, P. Emergency department crowding and thrombolysis delays in acute myocardial infarction. Ann. Emerg. Med. 2004, 44, 577–585. [Google Scholar] [CrossRef] [PubMed]
- Hwang, U.; Richardson, L.D.; Sonuyi, T.O.; Morrison, R.S. The Effect of Emergency Department Crowding on the Management of Pain in Older Adults with Hip Fracture. J. Am. Geriatr. Soc. 2006, 54, 270–275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCarthy, M.L.; Zeger, S.L.; Ding, R.; Levin, S.R.; Desmond, J.S.; Lee, J.; Aronsky, D. Crowding Delays Treatment and Lengthens Emergency Department Length of Stay, Even Among High-Acuity Patients. Ann. Emerg. Med. 2009, 54, 492–503.e4. [Google Scholar] [CrossRef] [PubMed]
- Jeanmonod, D.; Jeanmonod, R. Overcrowding in the emergency department and patient safety. Vignettes Patient Saf. 2018, 2, 257. Available online: http://www.intechopen.com/books/vignettes-in-patient-safety-volume-2/overcrowding-in-the-emergency-department-and-patient-safety (accessed on 12 December 2021).
- Pines, J.M.; Garson, C.; Baxt, W.G.; Rhodes, K.V.; Shofer, F.S.; Hollander, J.E. ED crowding is associated with variable perceptions of care compromise. Acad. Emerg. Med. 2007, 14, 1176–1181. [Google Scholar] [CrossRef]
- Pines, J.M.; Iyer, S.; Disbot, M.; Hollander, J.; Shofer, F.S.; Datner, E.M. The Effect of Emergency Department Crowding on Patient Satisfaction for Admitted Patients. Acad. Emerg. Med. 2008, 15, 825–831. [Google Scholar] [CrossRef]
- Australasian College for Emergency Medicine. ACEM Workforce Sustainability Survey Report; ACEM Australasian College for Emergency Medicine: Melbourne, Australia, 2016. [Google Scholar]
- Australian Medical Association. Position Statement on Quality and Safety in Public Hospitals; Australian Medical Association: Kingston, ACT, Australia, 2006. [Google Scholar]
- Mumma, B.E.; McCue, J.Y.; Li, C.-S.; Holmes, J.F. Effects of Emergency Department Expansion on Emergency Department Patient Flow. Acad. Emerg. Med. 2014, 21, 504–509. [Google Scholar] [CrossRef] [Green Version]
- Shepperd, S.; Iliffe, S.; Doll, H.A.; Clarke, M.; Kalra, L.; Wilson, A.D.; Bradley, D.G. Admission avoidance hospital at home. Cochrane Database Syst. Rev. 2016, 9, CD007491. [Google Scholar] [CrossRef] [Green Version]
- Lee, I.-H.; Chen, C.-T.; Lee, Y.-T.; Hsu, Y.-S.; Lu, C.-L.; Huang, H.-H.; Hsu, T.-F.; How, C.-K.; Yen, D.H.-T.; Yang, U.-C. A new strategy for emergency department crowding: High-turnover utility bed intervention. J. Chin. Med. Assoc. 2017, 80, 297–302. [Google Scholar] [CrossRef]
- Savioli, G.; Ceresa, I.F.; Maggioni, P.; Lava, M.; Ricevuti, G.; Manzoni, F.; Oddone, E.; Bressan, M.A. Impact of ED Organization with a Holding Area and a Dedicated Team on the Adherence to International Guidelines for Patients with Acute Pulmonary Embolism: Experience of an Emergency Department Organized in Areas of Intensity of Care. Medicines 2020, 7, 60. [Google Scholar] [CrossRef]
- Savioli, G.; Ceresa, I.F.; Manzoni, F.; Ricevuti, G.; Bressan, M.A.; Oddone, E. Role of a Brief Intensive Observation Area with a Dedicated Team of Doctors in the Management of Acute Heart Failure Patients: A Retrospective Observational Study. Medicines 2020, 56, 251. [Google Scholar] [CrossRef] [PubMed]
- Savioli, G.; Ceresa, I.F.; Luzzi, S.; Gragnaniello, C.; Lucifero, A.G.; Del Maestro, M.; Marasco, S.; Manzoni, F.; Ciceri, L.; Gelfi, E.; et al. Rates of Intracranial Hemorrhage in Mild Head Trauma Patients Presenting to Emergency Department and Their Management: A Comparison of Direct Oral Anticoagulant Drugs with Vitamin K Antagonists. Medicina 2020, 56, 308. [Google Scholar] [CrossRef] [PubMed]
- Ceresa, I.F.; Savioli, G.; Angeli, V.; Novelli, V.; Muzzi, A.; Grugnetti, G.; Cobianchi, L.; Manzoni, F.; Klersy, C.; Lago, P.; et al. Preparing for the Maximum Emergency with a Simulation: A Table-Top Test to Evaluate Bed Surge Capacity and Staff Compliance with Training. Open Access Emerg. Med. 2020, 12, 377–387. [Google Scholar] [CrossRef] [PubMed]
- Savioli, G.; Ceresa, I.F.; Luzzi, S.; Giotta Lucifero, A.; Pioli Di Marco, M.S.; Manzoni, F.; Preda, L.; Ricevuti, G.; Bressan, M.A. Mild Head Trauma: Is Antiplatelet Therapy a Risk Factor for Hemorrhagic Complications? Medicina 2021, 57, 357. [Google Scholar] [CrossRef] [PubMed]
- Savioli, G.; Ceresa, I.F.; Giordano, M.; Ferrari, I.; Varesi, A.; Floris, V.; Esposito, C.; Croesi, B.; Ricevuti, G.; Calvi, M.; et al. The Reliability of Anamnestic Data in the Management of Clostridium Tetani Infection in Elderly. Front. Med. 2021, 8, 684594. [Google Scholar] [CrossRef] [PubMed]
- Savioli, G.; Ceresa, I.F.; Macedonio, S.; Gerosa, S.; Belliato, M.; Luzzi, S.; Lucifero, A.G.; Manzoni, F.; Ricevuti, G.; Bressan, M.A. Major Trauma in Elderly Patients: Worse Mortality and Outcomes in an Italian Trauma Center. J. Emergencies Trauma Shock 2021, 14, 98–103. [Google Scholar]
- Savioli, G.; Ceresa, I.F.; Macedonio, S.; Gerosa, S.; Belliato, M.; Iotti, G.A.; Luzzi, S.; Del Maestro, M.; Mezzini, G.; Lucifero, A.G.; et al. Trauma Coagulopathy and Its Outcomes. Medicines 2020, 56, 205. [Google Scholar] [CrossRef] [Green Version]
- Lim, A.G.; Kivlehan, S.; Losonczy, L.I.; Murthy, S.; Dippenaar, E.; Lowsby, R.; Yang, M.L.C.L.; Jaung, M.S.; Stephens, P.A.; Benzoni, N.; et al. Critical care service delivery across healthcare systems in low-income and low-middle-income countries: Protocol for a systematic review. BMJ Open 2021, 11, e048423. [Google Scholar] [CrossRef]
- Alsabri, M.; Boudi, Z.; Lauque, D.; Dias, R.D.; Whelan, J.S.; Östlundh, L.; Alinier, G.; Onyeji, C.; Michel, P.; Liu, S.W.; et al. Impact of Teamwork and Communication Training Interventions on Safety Culture and Patient Safety in Emergency Departments: A Systematic Review. J. Patient Saf. 2020, 18, e351–e361. [Google Scholar] [CrossRef]
- Alsabri, M.; Boudi, Z.; Zoubeidi, T.; Alfaki, I.A.; Levy, P.; Oneyji, C.; Shan, L.; Camargo, C.A.; Michel, P.; Tazarourte, K.; et al. Analysis of Risk Factors for Patient Safety Events Occurring in the Emergency Department. J. Patient Saf. 2020, 18, e124–e135. [Google Scholar] [CrossRef]
- Boudi, Z.; Lauque, D.; Alsabri, M.; Östlundh, L.; Oneyji, C.; Khalemsky, A.; Rial, C.L.; Liu, S.W.; Camargo, C., Jr.; Aburawi, E.; et al. Association between boarding in the emergency department and in-hospital mortality: A systematic review. PLoS ONE 2020, 15, e0231253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haroutunian, P.; Alsabri, M.; Kerdiles, F.J.; Adel Ahmed Abdullah, H.; Bellou, A. Analysis of Factors and Medical Errors Involved in Patient Complaints in a European Emergency Department. Adv. J. Emerg. Med. 2017, 2, e4. [Google Scholar] [PubMed]
- Al-Kuwaiti, A.; Hefny, A.F.; Bellou, A.; Eid, H.O.; Abu-Zidan, F.M. Epidemiology of head injury in the United Arab Emirates. Turk. J. Trauma Emerg. Surg. 2012, 18, 213–218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lovett, P.B.; Illg, M.L.; Sweeney, B.E. A Successful Model for a Comprehensive Patient Flow Management Center at an Academic Health System. Am. J. Med. Qual. 2016, 31, 246–255. [Google Scholar] [CrossRef] [PubMed]
- Pollaris, G.; Sabbe, M. Reverse triage: More than just another method. Eur. J. Emerg. Med. 2016, 23, 240–247. [Google Scholar] [CrossRef]
- Chang, A.M.; Cohen, D.J.; Lin, A.; Augustine, J.; Handel, D.A.; Howell, E.; Kim, H.; Pines, J.M.; Schuur, J.D.; McConnell, K.J.; et al. Hospital Strategies for Reducing Emergency Department Crowding: A Mixed-Methods Study. Ann. Emerg. Med. 2018, 71, 497–505.e4. [Google Scholar] [CrossRef]


{kind=link}
| Parameter | Contributing Factors |
|---|---|
| Input | - emergencies (both medical and surgical) - visit type (both urgent and nonurgent) - ambulance arrivals - number of patients - triage score |
| Throughput | - time of processing - patients’ degree of gravity - process of triage and bed placement - bed availability (both in the ED and in the hospital) - staffing (nursing and other healthcare professionals), considering their experience and their training - other services (consultant and ancillary) - degree of boarding |
| Output | - hospital occupancy - inpatient bed shortage - transport delay (both internal and external) - staffing ratios - inefficient process of transferring care - inefficient planning of discharging patients - need of higher level of care - inpatients’ degree of gravity - lack of home care (both medical and not) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Savioli, G.; Ceresa, I.F.; Gri, N.; Bavestrello Piccini, G.; Longhitano, Y.; Zanza, C.; Piccioni, A.; Esposito, C.; Ricevuti, G.; Bressan, M.A. Emergency Department Overcrowding: Understanding the Factors to Find Corresponding Solutions. J. Pers. Med. 2022, 12, 279. https://doi.org/10.3390/jpm12020279
Savioli G, Ceresa IF, Gri N, Bavestrello Piccini G, Longhitano Y, Zanza C, Piccioni A, Esposito C, Ricevuti G, Bressan MA. Emergency Department Overcrowding: Understanding the Factors to Find Corresponding Solutions. Journal of Personalized Medicine. 2022; 12(2):279. https://doi.org/10.3390/jpm12020279
Chicago/Turabian StyleSavioli, Gabriele, Iride Francesca Ceresa, Nicole Gri, Gaia Bavestrello Piccini, Yaroslava Longhitano, Christian Zanza, Andrea Piccioni, Ciro Esposito, Giovanni Ricevuti, and Maria Antonietta Bressan. 2022. "Emergency Department Overcrowding: Understanding the Factors to Find Corresponding Solutions" Journal of Personalized Medicine 12, no. 2: 279. https://doi.org/10.3390/jpm12020279