
Automated Machine Learning in Predicting 30-Day Mortality in Patients with Non-Cholestatic Cirrhosis

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Inclusion and Exclusion Criteria
2.3. Clinical Data Collection
2.4. Statistics Analysis
3. Results
3.1. Characteristics of the Patients
3.2. Models Based on AutoML Algorithms
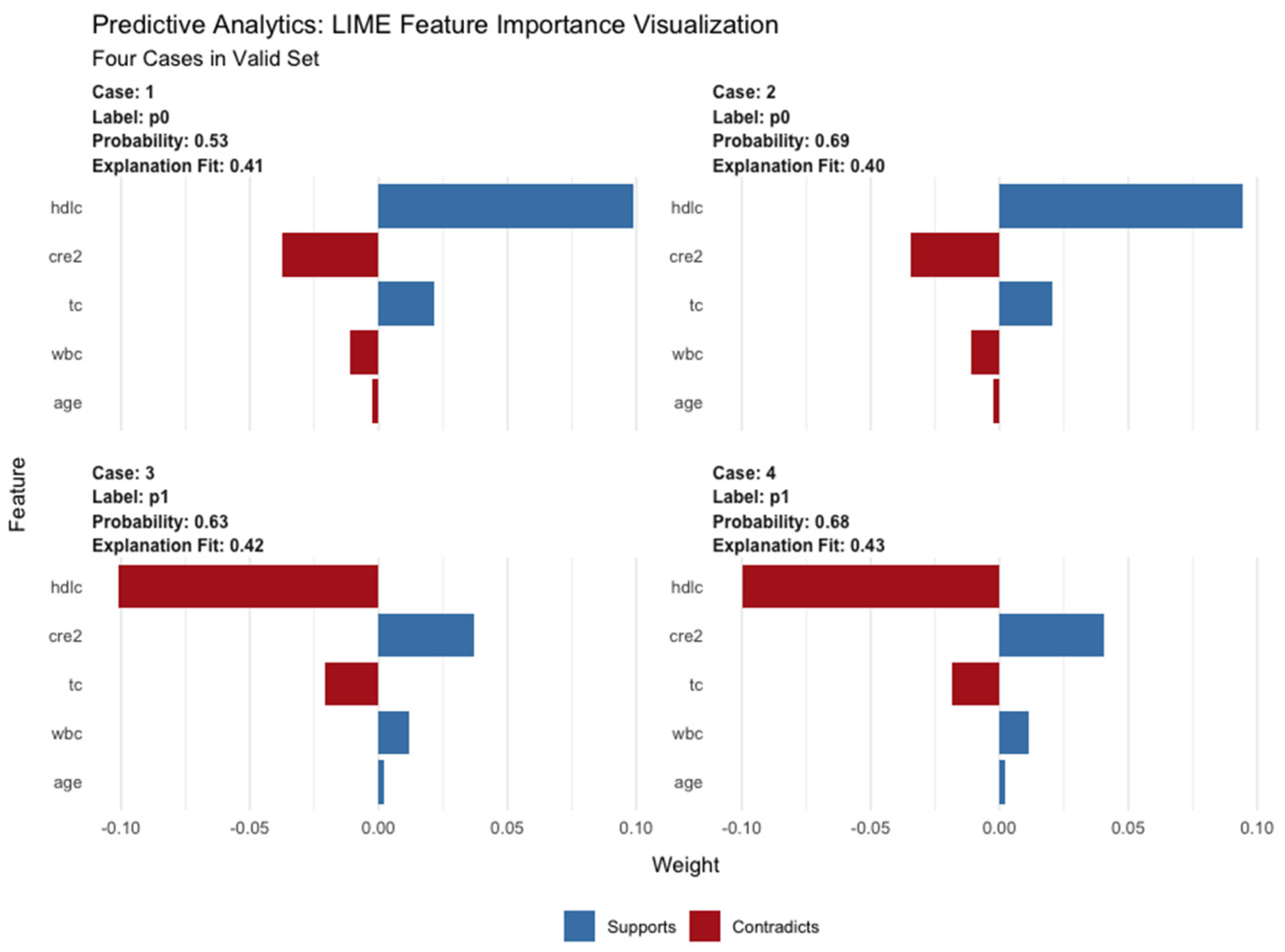
3.3. Interpretation of the AutoML Model Based on XGBoost Algorithm
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bernardi, M.; Angeli, P.; Claria, J.; Moreau, R.; Gines, P.; Jalan, R.; Caraceni, P.; Fernandez, J.; Gerbes, A.L.; O’Brien, A.J.; et al. Albumin in decompensated cirrhosis: New concepts and perspectives. Gut 2020, 69, 1127–1138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lindor, K.D.; Gershwin, M.E.; Poupon, R.; Kaplan, M.; Bergasa, N.V.; Heathcote, E.J. American Association for Study of Liver D: Primary biliary cirrhosis. Hepatology 2009, 50, 291–308. [Google Scholar] [CrossRef] [PubMed]
- D’Amico, G.; Morabito, A.; D’Amico, M.; Pasta, L.; Malizia, G.; Rebora, P.; Valsecchi, M.G. Clinical states of cirrhosis and competing risks. J. Hepatol. 2018, 68, 563–576. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D’Amico, G.; Garcia-Tsao, G.; Pagliaro, L. Natural history and prognostic indicators of survival in cirrhosis: A systematic review of 118 studies. J. Hepatol. 2006, 44, 217–231. [Google Scholar] [CrossRef] [PubMed]
- D’Amico, G.; Pasta, L.; Morabito, A.; D’Amico, M.; Caltagirone, M.; Malizia, G.; Tine, F.; Giannuoli, G.; Traina, M.; Vizzini, G.; et al. Competing risks and prognostic stages of cirrhosis: A 25-year inception cohort study of 494 patients. Aliment. Pharm. 2014, 39, 1180–1193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pugh, R.N.H.; Murray-Lyon, I.M.; Dawson, J.L.; Pietroni, M.C.; Williams, R. Transection of the oe sophagus for bleeding oesophageal varice. Br. J. Surg. 1973, 60, 646–649. [Google Scholar] [CrossRef]
- Wiesner, R.; Edwards, E.; Freeman, R.; Harper, A.; Kim, R.; Kamath, P.; Kremers, W.; Lake, J.; Howard, T.; Merion, R.M.; et al. Model for end-stage liver disease (MELD) and allocation of donor livers. Gastroenterology 2003, 124, 91–96. [Google Scholar] [CrossRef] [Green Version]
- Kamath, P.S.; Kim, W.R. Advanced Liver Disease Study G: The model for end-stage liver disease (MELD). Hepatology 2007, 45, 797–805. [Google Scholar] [CrossRef]
- Deo, R.C. Machine Learning in Medicine. Circulation 2015, 132, 1920–1930. [Google Scholar] [CrossRef] [Green Version]
- Liu, G.; Lu, D.; Lu, J. Pharm-AutoML an open-source, end-to-end automated machine learning package for clinical outcome prediction. CPT Pharmacomet. Syst. Pharm. 2021, 10, 478–488. [Google Scholar] [CrossRef]
- Biggins, S.W.; Kim, W.R.; Terrault, N.A.; Saab, S.; Balan, V.; Schiano, T.; Benson, J.; Therneau, T.; Kremers, W.; Wiesner, R.; et al. Evidence-based incorporation of serum sodium concentration into MELD. Gastroenterology 2006, 130, 1652–1660. [Google Scholar] [CrossRef] [PubMed]
- Johnson, P.J.; Berhane, S.; Kagebayashi, C.; Satomura, S.; Teng, M.; Reeves, H.L.; O’Beirne, J.; Fox, R.; Skowronska, A.; Palmer, D.; et al. Assessment of liver function in patients with hepatocellular carcinoma: A new evidence-based approach-the ALBI grade. J. Clin. Oncol. 2015, 33, 550–558. [Google Scholar] [CrossRef] [PubMed]
- Cicognani, C.; Malavolti, M.; Morselli-Labate, A.M.; Zamboni, L.; Sama, C.; Barbara, L. Serum Lipid and Lipoprotein Patterns in Patients with Liver Cirrhosis and Chronic Active Hepatitis. Arch. Intern. Med. 1997, 157, 792–796. [Google Scholar] [CrossRef] [PubMed]
- Etogo-Asse, F.E.; Vincent, R.P.; Hughes, S.A.; Auzinger, G.; Le Roux, C.W.; Wendon, J.; Bernal, W. High density lipoprotein in patients with liver failure; relation to sepsis, adrenal function and outcome of illness. Liver Int. 2012, 32, 128–136. [Google Scholar] [CrossRef]
- Trieb, M.; Rainer, F.; Stadlbauer, V.; Douschan, P.; Horvath, A.; Binder, L.; Trakaki, A.; Knuplez, E.; Scharnagl, H.; Stojakovic, T.; et al. HDL-related biomarkers are robust predictors of survival in patients with chronic liver failure. J. Hepatol. 2020, 73, 113–120. [Google Scholar] [CrossRef] [Green Version]
- Habib, A.; Mihas, A.A.; Abou-Assi, S.G.; Williams, L.M.; Gavis, E.; Pandak, W.M.; Heuman, D.M. High-Density Lipoprotein Cholesterol as an Indicator of Liver Function and Prognosis in Noncholestatic Cirrhotics. Clin. Gastroenterol. Hepatol. 2005, 3, 286–291. [Google Scholar] [CrossRef]
- Dogan, I.; Karaman, K.; Sonmez, B.; Celik, S.; Turker, O. Relationship between serum neutrophil count and infarct size in patients with acute myocardial infarction. Nucl. Med. Commun. 2009, 30, 797–801. [Google Scholar] [CrossRef]
- Trieb, M.; Horvath, A.; Birner-Gruenberger, R.; Spindelboeck, W.; Stadlbauer, V.; Taschler, U.; Curcic, S.; Stauber, R.E.; Holzer, M.; Pasterk, L.; et al. Liver disease alters high-density lipoprotein composition, metabolism and function. Biochim. Biophys Acta 2016, 1861, 630–638. [Google Scholar] [CrossRef] [Green Version]
- Galbois, A.; Thabut, D.; Tazi, K.A.; Rudler, M.; Mohammadi, M.S.; Bonnefont-Rousselot, D.; Bennani, H.; Bezeaud, A.; Tellier, Z.; Guichard, C.; et al. Ex vivo effects of high-density lipoprotein exposure on the lipopolysaccharide-induced inflammatory response in patients with severe cirrhosis. Hepatology 2009, 49, 175–184. [Google Scholar] [CrossRef]
- Thabut, D.; Tazi, K.A.; Bonnefont-Rousselot, D.; Aller, M.; Farges, O.; Guimont, M.C.; Tellier, Z.; Guichard, C.; Ogier-Denis, E.; Poynard, T.; et al. High-density lipoprotein administration attenuates liver proinflammatory response, restores liver endothelial nitric oxide synthase activity, and lowers portal pressure in cirrhotic rats. Hepatology 2007, 46, 1893–1906. [Google Scholar] [CrossRef]
- Bajaj, J.S.; Reddy, K.R.; O’Leary, J.G.; Vargas, H.E.; Lai, J.C.; Kamath, P.S.; Tandon, P.; Wong, F.; Subramanian, R.M.; Thuluvath, P.; et al. Serum Levels of Metabolites Produced by Intestinal Microbes and Lipid Moieties Independently Associated with Acute-on-Chronic Liver Failure and Death in Patients with Cirrhosis. Gastroenterology 2020, 159, 1715–1730.e1712. [Google Scholar] [CrossRef] [PubMed]
- Bajaj, J.S.; O’Leary, J.G.; Reddy, K.R.; Wong, F.; Biggins, S.W.; Patton, H.; Fallon, M.B.; Garcia-Tsao, G.; Maliakkal, B.; Malik, R.; et al. Survival in infection-related acute-on-chronic liver failure is defined by extrahepatic organ failures. Hepatology 2014, 60, 250–256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, F.; Sun, W.; Xiao, Q.; Liang, C.; Jiang, S.; Lian, Y.; Shao, J.; Tan, S.; Zheng, S. Peripheral T lymphocytes predict the severity and prognosis in patients with HBV-related acute-on-chronic liver failure. Medicine 2021, 100, e24075. [Google Scholar] [CrossRef] [PubMed]
- Belcher, J.M.; Garcia-Tsao, G.; Sanyal, A.J.; Bhogal, H.; Lim, J.K.; Ansari, N.; Coca, S.G.; Parikh, C.R.; Consortium, T.-A. Association of AKI with mortality and complications in hospitalized patients with cirrhosis. Hepatology 2013, 57, 753–762. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jalan, R.; Pavesi, M.; Saliba, F.; Amoros, A.; Fernandez, J.; Holland-Fischer, P.; Sawhney, R.; Mookerjee, R.; Caraceni, P.; Moreau, R.; et al. The CLIF Consortium Acute Decompensation score (CLIF-C ADs) for prognosis of hospitalised cirrhotic patients without acute-on-chronic liver failure. J. Hepatol. 2015, 62, 831–840. [Google Scholar] [CrossRef] [Green Version]
- Chancharoenthana, W.; Leelahavanichkul, A. Acute kidney injury spectrum in patients with chronic liver disease: Where do we stand? World J. Gastroenterol 2019, 25, 3684–3703. [Google Scholar] [CrossRef]
- Adebayo, D.; Morabito, V.; Davenport, A.; Jalan, R. Renal dysfunction in cirrhosis is not just a vasomotor nephropathy. Kidney Int. 2015, 87, 509–515. [Google Scholar] [CrossRef] [Green Version]
- Muslimovic, A.; Rasic, S.; Tulumovic, D.; Hasanspahic, S.; Rebic, D. Inflammatory Markers and Procoagulants in Chronic Renal Disease Stages 1–4. Med. Arch. 2015, 69, 307–310. [Google Scholar] [CrossRef] [Green Version]
- Gines, P.; Sola, E.; Angeli, P.; Wong, F.; Nadim, M.K.; Kamath, P.S. Hepatorenal syndrome. Nat. Rev. Dis. Prim. 2018, 4, 23. [Google Scholar] [CrossRef]
- Northup, P.G.; Caldwell, S.H. Coagulation in liver disease: A guide for the clinician. Clin. Gastroenterol. Hepatol. 2013, 11, 1064–1074. [Google Scholar] [CrossRef]
- Li, J.; Liang, X.; You, S.; Feng, T.; Zhou, X.; Zhu, B.; Luo, J.; Xin, J.; Jiang, J.; Shi, D.; et al. Development and validation of a new prognostic score for hepatitis B virus-related acute-on-chronic liver failure. J. Hepatol. 2021, 75, 1104–1115. [Google Scholar] [CrossRef] [PubMed]
- Wu, T.; Li, J.; Shao, L.; Xin, J.; Jiang, L.; Zhou, Q.; Shi, D.; Jiang, J.; Sun, S.; Jin, L.; et al. Development of diagnostic criteria and a prognostic score for hepatitis B virus-related acute-on-chronic liver failure. Gut 2018, 67, 2181–2191. [Google Scholar] [CrossRef] [PubMed]
- Sajja, K.C.; Mohan, D.P.; Rockey, D.C. Age and ethnicity in cirrhosis. J. Investig. Med. 2014, 62, 920–926. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total (n = 932) | Survival (n = 796) | Mortality (n = 136) | p | |
|---|---|---|---|---|
| Sex, n (%) | 0.742 | |||
| Male | 581(62) | 494(62) | 87(64) | |
| Female | 351(38) | 302(38) | 49(36) | |
| Age (years) | 61(50, 69) | 60(49, 69) | 67(53, 73) | <0.001 |
| BMI | 23.24 ± 3.19 | 23.33 ± 3.14 | 22.50 ± 3.56 | 0.074 |
| Etiology | 0.784 | |||
| ALD | 80(9) | 67(8) | 13(10) | |
| Others | 852(91) | 729(92) | 123(90) | |
| Complication, n (%) | <0.001 | |||
| Ascites | 123(13) | 115(14) | 8(6) | |
| Hypersplenism | 69(7) | 67(8) | 2(1) | |
| EGVB | 283(30) | 247(31) | 36(26) | |
| HE | 102(11) | 79(10) | 23(17) | |
| Hypohepatia | 355(38) | 288(37) | 67(49) | |
| WBC (1012 g/L) | 4.87(3.30, 7.23) | 4.53(3.15, 6.48) | 7.29(4.91, 10.91) | <0.001 |
| PLT (109 g/L) | 77.00(50.00, 124.25) | 78.00(51.00, 126.00) | 76.00(49.00, 112.25) | 0.489 |
| TBIL (μmol/L) | 2.14(1.23, 4.46) | 1.99(1.20, 3.75) | 4.93(1.93, 13.59) | <0.001 |
| Creatinine (mg/dL) | 0.74(0.60, 0.94) | 0.73(0.59, 0.92) | 0.84(0.65, 1.40) | <0.001 |
| ALT (U/L) | 28.00(18.00, 52.02) | 27.55(17.90, 48.00) | 33.10(19.67, 89.50) | 0.003 |
| AST (U/L) | 41.65(28.67, 71.75) | 40.00(28.08, 67.53) | 52.95(32.88, 106.40) | <0.001 |
| Albumin (g/L) | 30.40(26.67, 34.10) | 30.70(27.00, 34.70) | 28.00(23.98, 31.50) | <0.001 |
| Na (mmol/L) | 139.50(137.00, 141.80) | 139.50(137.00, 141.80) | 138.30(134.67, 141.27) | 0.01 |
| TC (mmol/L) | 3.14(2.50, 3.91) | 3.21(2.55, 4.00) | 2.64(2.00, 3.17) | <0.001 |
| TG (mmol/L) | 0.88(0.66, 1.24) | 0.88(0.66, 1.22) | 0.94(0.64, 1.30) | 0.4 |
| HDL-C (mg/dL) | 0.87(0.52, 1.17) | 0.90(0.62, 1.21) | 0.47(0.21, 0.78) | <0.001 |
| LDL-C (mg/dL) | 1.60(1.18, 2.16) | 1.65(1.26, 2.20) | 1.21(0.89, 1.85) | <0.001 |
| Pre-ALB (mg/dL) | 73.35(48.00, 104.65) | 76.55(50.98, 108.20) | 58.90(39.93, 83.30) | <0.001 |
| PT (s) | 15.50(13.70, 17.90) | 15.20(13.50, 17.30) | 18.30(15.60, 22.02) | <0.001 |
| LnINR | 0.30(0.17, 0.45) | 0.28(0.17, 0.42) | 0.48(0.30, 0.68) | <0.001 |
| MELD | 9.89(6.16, 14.83) | 9.41(5.77, 13.37) | 17.11(9.87, 23.73) | <0.001 |
| MELD-Na | 10.43(5.54, 16.46) | 9.62(5.10, 14.94) | 18.07(10.30, 25.39) | <0.001 |
| ALBI | −1.53 ± 0.66 | −1.59 ± 0.64 | −1.14 ± 0.62 | <0.001 |
| Dataset | Algorithm | AUC | Accuracy | Sensitivity | Specificity |
|---|---|---|---|---|---|
| Training | GBM | 0.900 | 0.876 | 0.597 | 0.926 |
| XGBoost | 0.938 | 0.915 | 0.647 | 0.963 | |
| LR | 0.662 | 0.852 | 0.555 | 0.905 | |
| RF | 0.807 | 0.833 | 0.513 | 0.890 | |
| DL | 1.000 | 0.999 | 1.000 | 0.999 | |
| Stacking | 0.956 | 0.922 | 0.655 | 0.969 | |
| MELD | 0.806 | 0.784 | 0.736 | 0.793 | |
| MELD-Na | 0.791 | 0.797 | 0.669 | 0.820 | |
| ALBI | 0.739 | 0.649 | 0.752 | 0.630 | |
| Validation | GBM | 0.886 | 0.857 | 0.412 | 0.919 |
| XGBoost | 0.888 | 0.879 | 0.471 | 0.935 | |
| LR | 0.673 | 0.821 | 0.353 | 0.886 | |
| RF | 0.866 | 0.821 | 0.294 | 0.894 | |
| DL | 0.830 | 0.850 | 0.471 | 0.902 | |
| Stacking | 0.850 | 0.871 | 0.294 | 0.951 | |
| MELD | 0.778 | 0.864 | 0.588 | 0.902 | |
| MELD-Na | 0.782 | 0.857 | 0.588 | 0.894 | |
| ALBI | 0.662 | 0.536 | 0.824 | 0.496 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yu, C.; Li, Y.; Yin, M.; Gao, J.; Xi, L.; Lin, J.; Liu, L.; Zhang, H.; Wu, A.; Xu, C.; et al. Automated Machine Learning in Predicting 30-Day Mortality in Patients with Non-Cholestatic Cirrhosis. J. Pers. Med. 2022, 12, 1930. https://doi.org/10.3390/jpm12111930
Yu C, Li Y, Yin M, Gao J, Xi L, Lin J, Liu L, Zhang H, Wu A, Xu C, et al. Automated Machine Learning in Predicting 30-Day Mortality in Patients with Non-Cholestatic Cirrhosis. Journal of Personalized Medicine. 2022; 12(11):1930. https://doi.org/10.3390/jpm12111930
Chicago/Turabian StyleYu, Chenyan, Yao Li, Minyue Yin, Jingwen Gao, Liting Xi, Jiaxi Lin, Lu Liu, Huixian Zhang, Airong Wu, Chunfang Xu, and et al. 2022. "Automated Machine Learning in Predicting 30-Day Mortality in Patients with Non-Cholestatic Cirrhosis" Journal of Personalized Medicine 12, no. 11: 1930. https://doi.org/10.3390/jpm12111930