
Circulating and Salivary NGF and BDNF Levels in SARS-CoV-2 Infection: Potential Predictor Biomarkers of COVID-19 Disease—Preliminary Data
 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics and Study Population
2.2. Biosample Handling and Laboratory Tests
2.3. Statistical Analysis: Packages and Visual Representation
3. Results
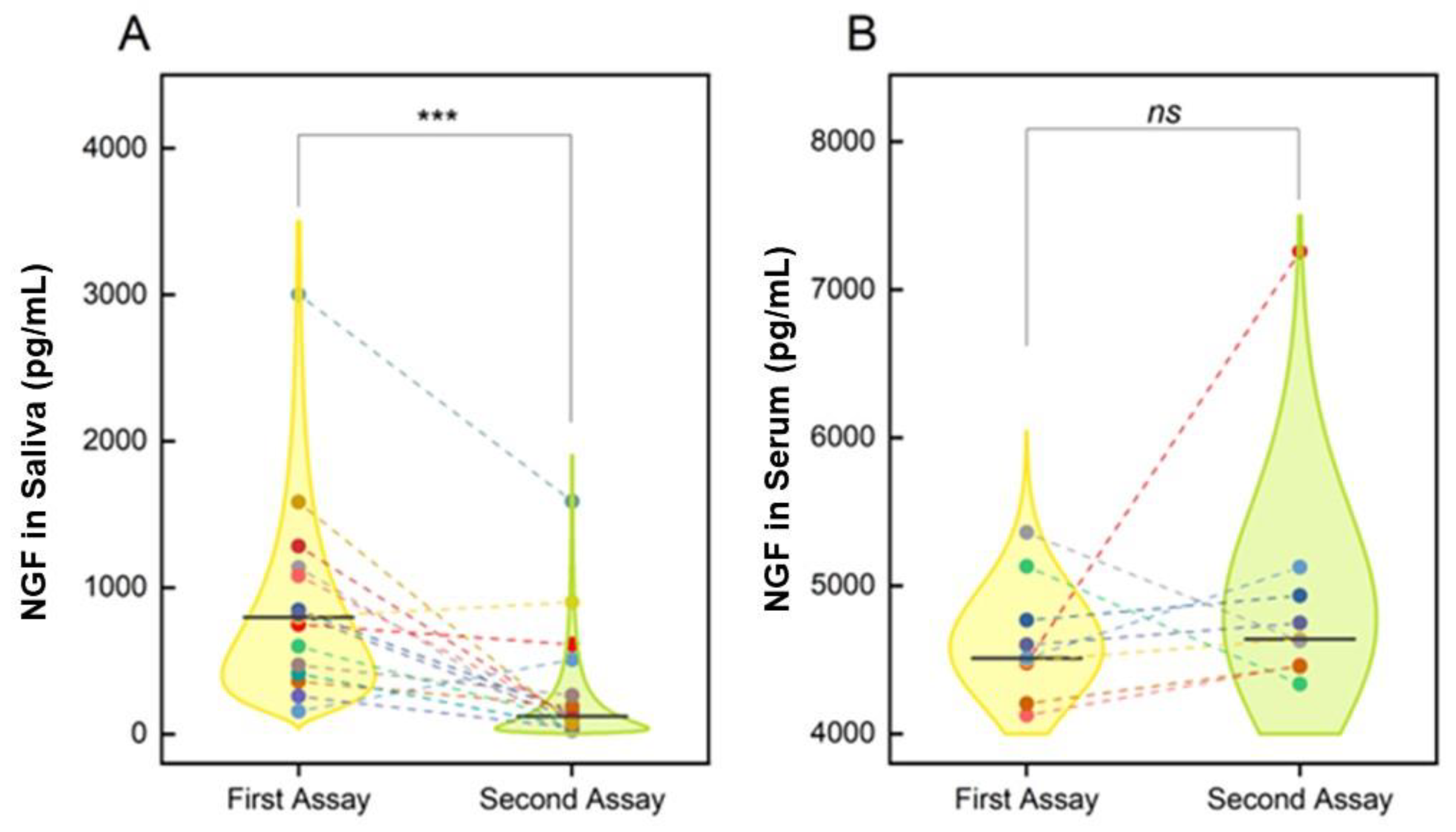
3.1. COVID-19 and NGF Levels
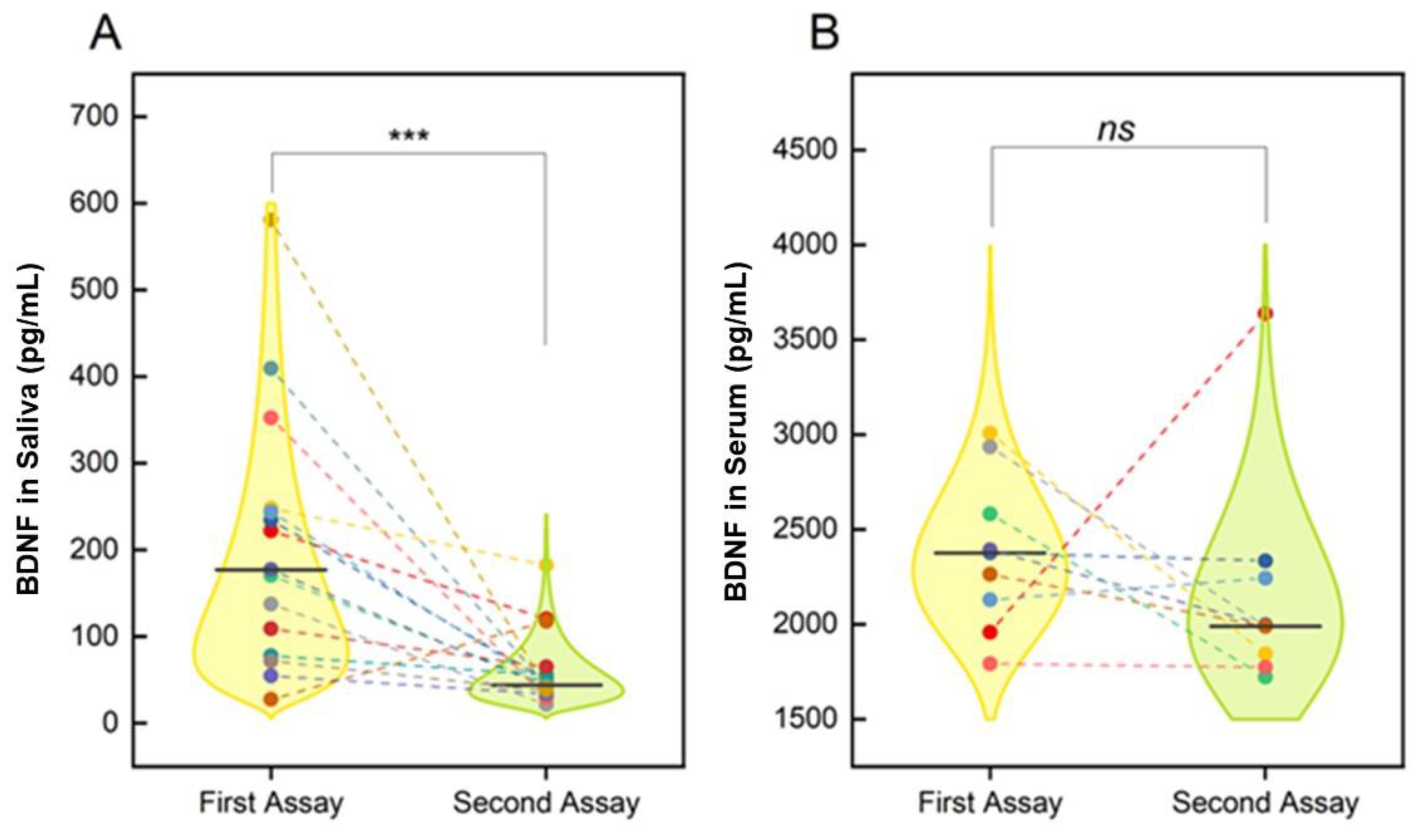
3.2. COVID-19 and Changes in Salivary and Circulating Levels of BDNF
3.3. Demographic and Biochemical Comparisons
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhang, Y.; Huang, Z.; Zhu, J.; Li, C.; Fang, Z.; Chen, K.; Zhang, Y. An updated review of SARS-CoV-2 detection methods in the context of a novel coronavirus pandemic. Bioeng. Transl. Med. 2022, e10356. [Google Scholar] [CrossRef] [PubMed]
- Aleem, A.; Akbar Samad, A.B.; Slenker, A.K. Emerging Variants of SARS-CoV-2 And Novel Therapeutics Against Coronavirus (COVID-19). In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Tian, S.; Xiong, Y.; Liu, H.; Niu, L.; Guo, J.; Liao, M.; Xiao, S.Y. Pathological study of the 2019 novel coronavirus disease (COVID-19) through postmortem core biopsies. Mod. Pathol. 2020, 33, 1007–1014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, J.J.; Dong, X.; Cao, Y.Y.; Yuan, Y.D.; Yang, Y.B.; Yan, Y.Q.; Akdis, C.A.; Gao, Y.D. Clinical characteristics of 140 patients infected with SARS-CoV-2 in Wuhan, China. Allergy 2020, 75, 1730–1741. [Google Scholar] [CrossRef] [PubMed]
- Cafiero, C.; Rosapepe, F.; Palmirotta, R.; Re, A.; Ottaiano, M.P.; Benincasa, G.; Perone, R.; Varriale, E.; D’Amato, G.; Cacciamani, A.; et al. Angiotensin System Polymorphisms’ in SARS-CoV-2 Positive Patients: Assessment between Symptomatic and Asymptomatic Patients: A Pilot Study. Pharm. Pers. Med. 2021, 14, 621–629. [Google Scholar] [CrossRef]
- Cafiero, C.; Palmirotta, R.; Micera, A.; Ottaiano, M.P.; Re, A.; Pedata, F.; Costagliola, D.; Ponticelli, D.; Pisconti, S.; Schiavone, B.; et al. SARS-CoV-2 infection after vaccination in Italian health care workers: A case report. Natl. Acad. Sci. Lett. 2022, 45, 249–254. [Google Scholar] [CrossRef] [PubMed]
- Ng, R.; Vargas, G.; Jashar, D.T.; Morrow, A.; Malone, L.A. Neurocognitive and Psychosocial Characteristics of Pediatric Patients With Post-Acute/Long-COVID: A Retrospective Clinical Case Series. Arch. Clin. Neuropsychol. 2022, acac056. [Google Scholar] [CrossRef] [PubMed]
- Yong, S.J. Long COVID or post-COVID-19 syndrome: Putative pathophysiology, risk factors, and treatments. Infect. Dis. 2021, 53, 737–754. [Google Scholar] [CrossRef]
- Higgins, V.; Sohaei, D.; Diamandis, E.P.; Prassas, I. COVID-19: From an acute to chronic disease? Potential long-term health consequences. Crit. Rev. Clin. Lab. Sci. 2021, 58, 297–310. [Google Scholar] [CrossRef]
- Aloe, L.; Rocco, M.L.; Balzamino, B.O.; Micera, A. Nerve Growth Factor: A Focus on Neuroscience and Therapy. Curr. Neuropharmacol. 2015, 13, 294–303. [Google Scholar] [CrossRef] [Green Version]
- Lang, U.E.; Gallinat, J.; Danker-Hopfe, H.; Bajbouj, M.; Hellweg, R. Nerve growth factor serum concentrations in healthy human volunteers: Physiological variance and stability. Neurosci. Lett. 2003, 344, 13–16. [Google Scholar] [CrossRef]
- Martocchia, A.; Sigala, S.; Proietti, A.; D’Urso, R.; Spano, P.F.; Missale, C.; Falaschi, P. Sex-related variations in serum nerve growth factor concentration in humans. Neuropeptides 2002, 36, 391–395. [Google Scholar] [CrossRef]
- Skaper, S.D. Nerve growth factor: A neuroimmune crosstalk mediator for all seasons. Immunology 2017, 151, 1–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oddone, F.; Roberti, G.; Micera, A.; Busanello, A.; Bonini, S.; Quaranta, L.; Agnifili, L.; Manni, G. Exploring Serum Levels of Brain Derived Neurotrophic Factor and Nerve Growth Factor Across Glaucoma Stages. PLoS ONE 2017, 12, e0168565. [Google Scholar] [CrossRef] [Green Version]
- Liu, P.; Li, S.; Tang, L. Nerve Growth Factor: A Potential Therapeutic Target for Lung Diseases. Int. J. Mol. Sci. 2021, 22, 9112. [Google Scholar] [CrossRef]
- Torcia, M.; Bracci-Laudiero, L.; Lucibello, M.; Nencioni, L.; Labardi, D.; Rubartelli, A.; Cozzolino, F.; Aloe, L.; Garaci, E. Nerve growth factor is an autocrine survival factor for memory B lymphocytes. Cell 1996, 85, 345–356. [Google Scholar] [CrossRef] [Green Version]
- Nam, J.W.; Chung, J.W.; Kho, H.S.; Chung, S.C.; Kim, Y.K. Nerve growth factor concentration in human saliva. Oral Dis. 2007, 13, 187–192. [Google Scholar] [CrossRef] [PubMed]
- Zappella, M.; Biamonte, F.; Balzamino, B.O.; Manieri, R.; Cortes, M.; Santucci, D.; Di Stasio, E.; Rizzuto, M.; Micera, A. Relaxation Response in Stressed Volunteers: Psychometric Tests and Neurotrophin Changes in Biological Fluids. Front. Psychiatry 2021, 12, 655453. [Google Scholar] [CrossRef]
- Aloe, L.; Bracci-Laudiero, L.; Alleva, E.; Lambiase, A.; Micera, A.; Tirassa, P. Emotional stress induced by parachute jumping enhances blood nerve growth factor levels and the distribution of nerve growth factor receptors in lymphocytes. Proc. Natl. Acad. Sci. USA 1994, 91, 10440–10444. [Google Scholar] [CrossRef] [Green Version]
- Cirulli, F.; Alleva, E. The NGF saga: From animal models of psychosocial stress to stress-related psychopathology. Front. Neuroendocrinol. 2009, 30, 379–395. [Google Scholar] [CrossRef] [PubMed]
- Minnone, G.; De Benedetti, F.; Bracci-Laudiero, L. NGF and Its Receptors in the Regulation of Inflammatory Response. Int. J. Mol. Sci. 2017, 18, 1028. [Google Scholar] [CrossRef] [PubMed]
- Bohmwald, K.; Andrade, C.A.; Mora, V.P.; Muñoz, J.T.; Ramírez, R.; Rojas, M.F.; Kalergis, A.M. Neurotrophin Signaling Impairment by Viral Infections in the Central Nervous System. Int. J. Mol. Sci. 2022, 23, 5817. [Google Scholar] [CrossRef]
- Ulrich-Lai, Y.M.; Herman, J.P. Neural regulation of endocrine and autonomic stress responses. Nat. Rev. Neurosci. 2009, 10, 397–409. [Google Scholar] [CrossRef] [Green Version]
- Borba, E.M.; Duarte, J.A.; Bristot, G.; Scotton, E.; Camozzato, A.L.; Chaves, M.L. Brain-derived neurotrophic factor serum levels and hippocampal volume in mild cognitive impairment and dementia due to Alzheimer disease. Dement Geriatr. Cogn. Dis. Extra. 2016, 91, 559–567. [Google Scholar] [CrossRef]
- Mozafarihashjin, M.; Togha, M.; Ghorbani, Z.; Farbod, A.; Rafiee, P.; Martami, F. Assessment of peripheral biomarkers potentially involved in episodic and chronic migraine: A case-control study with a focus on NGF, BDNF, VEGF, and PGE2. J. Headache Pain. 2022, 23, 3. [Google Scholar] [CrossRef]
- Boukhatem, I.; Fleury, S.; Welman, M.; Le Blanc, J.; Thys, C.; Freson, K.; Best, M.G.; Würdinger, T.; Allen, B.G.; Lordkipanidzé, M. The brain-derived neurotrophic factor prompts platelet aggregation and secretion. Blood Adv. 2021, 5, 3568–3580. [Google Scholar] [CrossRef]
- Fujimura, H.; Altar, C.A.; Chen, R.; Nakamura, T.; Nakahashi, T.; Kambayashi, J.; Sun, B.; Tandon, N.N. Brain-derived neurotrophic factor is stored in human platelets and released by agonist stimulation. Thromb. Haemost. 2002, 87, 728–773. [Google Scholar] [CrossRef] [Green Version]
- Kniewallner, K.M.; Grimm, N.; Humpel, C. Platelet-derived nerve growth factor supports the survival of cholinergic neurons in organotypic rat brain slices. Neurosci. Lett. 2014, 574, 64–69. [Google Scholar] [CrossRef] [Green Version]
- Cafiero, C.; Micera, A.; Re, A.; Postiglione, L.; Cacciamani, A.; Schiavone, B.; Benincasa, G.; Palmirotta, R. Could Small Neurotoxins-Peptides be expressed during SARS-CoV-2 Infection? Curr. Genom. 2021, 22, 557–563. [Google Scholar] [CrossRef]
- Aghagoli, G.; Gallo Marin, B.; Katchur, N.J.; Chaves-Sell, F.; Asaad, W.F.; Murphy, S.A. Neurological Involvement in COVID-19 and Potential Mechanisms: A Review. Neurocrit. Care 2021, 34, 1062–1071. [Google Scholar] [CrossRef]
- Needham, E.J.; Ren, A.L.; Digby, R.J.; Norton, E.J.; Ebrahimi, S.; Outtrim, J.G.; Chatfield, D.A.; Manktelow, A.E.; Leibowitz, M.M.; Newcombe, V.; et al. Cambridge NeuroCOVID Group the CITIID-NIHR COVID-19 BioResource Collaboration and Cambridge NIHR Clinical Research Facility. Brain injury in COVID-19 is associated with dysregulated innate and adaptive immune responses. Brain 2022, awac321. [Google Scholar] [CrossRef]
- Azoulay, D.; Shehadeh, M.; Chepa, S.; Shaoul, E.; Baroum, M.; Horowitz, N.A.; Kaykov, E. Recovery from SARS-CoV-2 infection is associated with serum BDNF restoration. J. Infect. 2020, 81, e79–e81. [Google Scholar] [CrossRef]
- Iannitelli, A.; Tirassa, P.; Fiore, M.; Pacitti, F.; Quartini, A.; Rosso, P.; Fico, E.; Garavini, A.; Pompili, A.; Vitali, M.; et al. Gender differences in ultradian serum levels of NGF and BDNF correlate with psychophysical traits in healthy humans. Riv. Psichiatr. 2021, 56, 314–320. [Google Scholar]
- Petrella, C.; Nenna, R.; Petrarca, L.; Tarani, F.; Paparella, R.; Mancino, E.; Di Mattia, G.; Conti, M.G.; Matera, L.; Bonci, E.; et al. Serum NGF and BDNF in Long-COVID-19 Adolescents: A Pilot Study. Diagnostics 2022, 12, 1162. [Google Scholar] [CrossRef]
- Dergaa, I.; Abubaker, M.; Souissi, A.; Mohammed, A.R.; Varma, A.; Musa, S.; Al Naama, A.; Mkaouer, B.; Ben Saad, H. Age and clinical signs as predictors of COVID-19 symptoms and cycle threshold value. Libyan J. Med. 2022, 17, 2010337. [Google Scholar] [CrossRef]
- Napodano, C.; Callà, C.; Fiorita, A.; Marino, M.; Taddei, E.; Di Cesare, T.; Passali, G.C.; Di Santo, R.; Stefanile, A.; Fantoni, M.; et al. Salivary Biomarkers in COVID-19 Patients: Towards a Wide-Scale Test for Monitoring Disease Activity. J. Pers. Med. 2021, 11, 385. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing [Internet]. Vienna, Austria. 2016. Available online: https://www.R-project.org/2016 (accessed on 28 September 2022).
- Sjoberg, D.D.; Whiting, K.; Curry, M.; Lavery, J.A.; Larmarange, J. Reproducible Summary Tables with the gtsummary Package. R J. 2021, 13, 570–580. [Google Scholar] [CrossRef]
- Morici, N.; Podda, G.; Birocchi, S.; Bonacchini, L.; Merli, M.; Trezzi, M.; Massaini, G.; Agostinis, M.; Carioti, G.; Saverio Serino, F.; et al. Enoxaparin for thromboprophylaxis in hospitalized COVID-19 patients: The X-COVID-19 Randomized Trial. Eur. J. Clin. Investig. 2022, 52, e13735. [Google Scholar] [CrossRef]
- Dobryakova, Y.V.; Spivak, Y.S.; Zaichenko, M.I.; Koryagina, A.A.; Markevich, V.A.; Stepanichev, M.Y.; Bolshakov, A.P. Intrahippocampal Adeno-Associated Virus-Mediated Overexpression of Nerve Growth Factor Reverses 192IgG-Saporin-Induced Impairments of Hippocampal Plasticity and Behavior. Front. Neurosci. 2021, 15, 745050. [Google Scholar] [CrossRef]
- Lambiase, A.; Coassin, M.; Costa, N.; Lauretti, P.; Micera, A.; Ghinelli, E.; Aloe, L.; Rama, P.; Bonini, S. Topical treatment with nerve growth factor in an animal model of herpetic keratitis. Graefe’s archive for clinical and experimental ophthalmology. Graefes Arch. Clin. Exp. Ophthalmol. 2008, 246, 121–127. [Google Scholar] [CrossRef]
- Tirassa, P.; Rosso, P.; Iannitelli, A. Ocular Nerve Growth Factor (NGF) and NGF Eye Drop Application as Paradigms to Investigate NGF Neuroprotective and Reparative Actions. Methods Mol. Biol. 2018, 1727, 19–38. [Google Scholar]
- Micera, A.; Puxeddu, I.; Aloe, L.; Levi-Schaffer, F. New insights on the involvement of Nerve Growth Factor in allergic inflammation and fibrosis. Cytokine Growth Factor Rev. 2003, 14, 369–374. [Google Scholar] [CrossRef]
- Micera, A.; Lambiase, A.; Stampachiacchiere, B.; Bonini, S.; Bonini, S.; Levi-Schaffer, F. Nerve growth factor and tissue reair remodeling: trkA(NGFR) and p75(NTR), two receptors one fate. Cytokine Growth Factor Rev. 2007, 18, 245–256. [Google Scholar] [CrossRef]
- Esposito, G.; Balzamino, B.O.; Bruno, L.; Cacciamani, A.; Micera, A. NGF in Inflammatory and Neurodegenerative Diseases of the Eye: New Findings Supporting Neuroprotection and Proper Tissue Remodeling in Vitreoretinal Disorders. Adv. Exp. Med. Biol. 2021, 1331, 265–273. [Google Scholar]
- Santucci, D.; Racca, A.; Alleva, E. When Nerve Growth Factor Met Behavior. Adv. Exp. Med. Biol. 2021, 1331, 205–214. [Google Scholar]
- Minuzzi, L.G.; Seelaender, M.; Silva, B.; Cunha, E.; Deus, M.C.; Vasconcellos, F.; Marqueze, L.; Gadotti, A.C.; Baena, C.P.; Pereira, T.; et al. COVID-19 Outcome Relates With Circulating BDNF, According to Patient Adiposity and Age. Front. Nutr. 2021, 8, 784429. [Google Scholar] [CrossRef]
- Asgarzadeh, A.; Fouladi, N.; Asghariazar, V.; Sarabi, S.F.; Khiavi, H.A.; Mahmoudi, M.; Safarzadeh, E. Serum Brain-Derived Neurotrophic Factor (BDNF) in COVID-19 Patients and its Association with the COVID-19 Manifestations. J. Mol. Neurosci. 2022, 72, 1820–1830. [Google Scholar] [CrossRef]
- Usai, C.; Gibbons, J.M.; Pade, C.; Li, W.; Jacobs, S.R.M.; McKnight, Á.; Kennedy, P.T.F.; Gill, U.S. The β-NGF/TrkA Signalling Pathway Is Associated With the Production of Anti-Nucleoprotein IgG in Convalescent COVID-19. Front. Immunol. 2022, 12, 813300. [Google Scholar] [CrossRef]
- Aloe, L. Nerve growth factor and neuroimmune responses: Basic and clinical observations. Arch. Physiol. Biochem. 2001, 109, 354–356. [Google Scholar] [CrossRef]
- Staff, J.F.; Harding, A.H.; Morton, J.; Jones, K.; Guice, E.A.; McCormick, T. Investigation of saliva as an alternative matrix to blood for the biological monitoring of inorganic lead. Toxicol. Lett. 2014, 231, 270–276. [Google Scholar] [CrossRef] [Green Version]
- Biondi, M.; Iannitelli, A. COVID-19 and stress in the pandemic: “sanity is not statistical”. Riv. Psichiatr. 2020, 55, 1e–6e. [Google Scholar]
- Mostafa, M.; Barhoum, A.; Sehit, E.; Gewaid, H.; Mostafa, E.; Omran, M.M.; Abdalla, M.S.; Abdel-Haleem, F.M.; Altintas, Z.; Forster, R.J. Current trends in COVID-19 diagnosis and its new variants in physiological fluids: Surface antigens, antibodies, nucleic acids, and RNA sequencing. Trends Analyt. Chem. 2022, 157, 116750. [Google Scholar] [CrossRef]
- Drago, F.; Gozzo, L.; Li, L.; Stella, A.; Cosmi, B. Use of Enoxaparin to Counteract COVID-19 Infection and Reduce Thromboembolic Venous Complications: A Review of the Current Evidence. Front. Pharmacol. 2020, 11, 579886. [Google Scholar] [CrossRef]
- Aurikko, J.P.; Ruotolo, B.T.; Grossmann, J.G.; Moncrieffe, M.C.; Stephens, E.; Leppänen, V.M.; Robinson, C.V.; Saarma, M.; Bradshaw, R.A.; Blundell, T.L. Characterization of symmetric complexes of nerve growth factor and the ectodomain of the pan-neurotrophin receptor, p75NTR. J. Biol. Chem. 2005, 280, 33453–33460. [Google Scholar] [CrossRef] [Green Version]
- Cabrera, N.; Díaz-Rodríguez, E.; Becker, E.; Martín-Zanca, D.; Pandiella, A. TrkA receptor ectodomain cleavage generates a tyrosine-phosphorylated cell-associated fragment. J. Cell Biol. 1996, 132, 427–436. [Google Scholar] [CrossRef] [Green Version]
- Ceci, F.M.; Fiore, M.; Gavaruzzi, F.; Angeloni, A.; Lucarelli, M.; Scagnolari, C.; Bonci, E.; Gabanella, F.; Di Certo, M.G.; Barbato, C.; et al. Early Routine Biomarkers of SARS-CoV-2 Morbidity and Mortality: Outcomes from an Emergency Section. Diagnostics 2022, 12, 176. [Google Scholar] [CrossRef]
- Koonin, L.M. Novel coronavirus disease (COVID-19) outbreak: Now is the time to refresh pandemic plans. J. Bus. Contin. Emerg. Plan. 2020, 13, 298–312. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Variables | Characteristics | % 1 |
|---|---|---|
| Gender | F/M | 8/11 (42%/58%) |
| Age | Years | 55 (48, 72) |
| Hospitalization | Days | 19 (13, 42) |
| COVID-19 | Fever at onset | 16 (84%) |
| Dyspnea at onset | 8 (42%) | |
| Asthenia at onset | 6 (32%) | |
| Pneumonia | 15 (79%) | |
| Comorbidities | 0 | 9 (47%) |
| 1 | 6 (32%) | |
| >1 | 4 (21%) | |
| Obesity | 6 (32%) | |
| Hypertension | 5 (26%) | |
| Diabetes | 1 (5.3%) | |
| Life styling | Smoke | 2 (11%) |
| Therapies | Oxygen | 9 (47%) |
| Intensive Care | 6 (32%) | |
| Treatments | Enoxaparin | 19 (100%) |
| Anti-IL-6 | 9 (47%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Biamonte, F.; Re, A.; Balzamino, B.O.; Ciasca, G.; Santucci, D.; Napodano, C.; Nocca, G.; Fiorita, A.; Marino, M.; Basile, U.; et al. Circulating and Salivary NGF and BDNF Levels in SARS-CoV-2 Infection: Potential Predictor Biomarkers of COVID-19 Disease—Preliminary Data. J. Pers. Med. 2022, 12, 1877. https://doi.org/10.3390/jpm12111877
Biamonte F, Re A, Balzamino BO, Ciasca G, Santucci D, Napodano C, Nocca G, Fiorita A, Marino M, Basile U, et al. Circulating and Salivary NGF and BDNF Levels in SARS-CoV-2 Infection: Potential Predictor Biomarkers of COVID-19 Disease—Preliminary Data. Journal of Personalized Medicine. 2022; 12(11):1877. https://doi.org/10.3390/jpm12111877
Chicago/Turabian StyleBiamonte, Filippo, Agnese Re, Bijorn Omar Balzamino, Gabriele Ciasca, Daniela Santucci, Cecilia Napodano, Giuseppina Nocca, Antonella Fiorita, Mariapaola Marino, Umberto Basile, and et al. 2022. "Circulating and Salivary NGF and BDNF Levels in SARS-CoV-2 Infection: Potential Predictor Biomarkers of COVID-19 Disease—Preliminary Data" Journal of Personalized Medicine 12, no. 11: 1877. https://doi.org/10.3390/jpm12111877