
Modern MRI Diagnostics of Upper-Extremity-Related Nerve Injuries—A Prospective Multi-Center Study Protocol for Diagnostics and Follow Up of Peripheral Nerve Injuries
 , , , and
, , , and
Abstract
:1. Background
2. Aim of the Study
- Peripheral nerve lesions of the trunk nerves of the upper extremity (60 patients);
- Applicability and nerve visualization in patients with internal plate osteosynthesis of humeral fractures (20 patients).
3. Methods
4. Participants
| Inclusion criteria: | General:
|
| Exclusion criteria |
|
| Absolute contraindications to MRI |
|
| In the case of a relative contraindication, only after the patient has been informed and the radiologist performing the procedure has given their consent |
|
5. Interventions
6. Objective
7. Primary Research Question
8. Secondary Research Question
9. Hypotheses
10. Design
11. Outcomes—Investigations
12. Statistical Considerations and Sample Size
13. Randomization
14. Statistical Methods
15. Timeframe—Recruiting Plan
16. Discussion
17. Trial Status
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
List of Abbreviations
| DASH | Disability of the Arm, Shoulder and Hand |
| DASS | Depression, Anxiety and Stress Score |
| DRF | clinical report form |
| DTI | diffusion tensor imaging |
| FA | fractional anisotropy |
| IES-R | Impact of Event Scale—short |
| MRI | magnetic resonance imaging |
| MRN | magnetic resonance neurography |
| SF-36 | Short Form 36 |
References
- Ciaramitaro, P.; Mondelli, M.; Logullo, F.; Grimaldi, S.; Battiston, B.; Sard, A.; Scarinzi, C.; Migliaretti, G.; Faccani, G.; Cocito, D.; et al. Traumatic peripheral nerve injuries: Epidemiological findings, neuropathic pain and quality of life in 158 patients. J. Peripher. Nerv. Syst. 2010, 15, 120–127. [Google Scholar] [CrossRef] [PubMed]
- Kouyoumdjian, J.A. Peripheral nerve injuries: A retrospective survey of 456 cases. Muscle Nerve 2006, 34, 785–788. [Google Scholar] [CrossRef] [PubMed]
- Robinson, L.R. Traumatic injury to peripheral nerves. Suppl. Clin. Neurophysiol. 2004, 57, 173–186. [Google Scholar] [CrossRef]
- Dahlin, L.B. The Role of Timing in Nerve Reconstruction. Int. Rev. Neurobiol. 2013, 109, 151–164. [Google Scholar] [CrossRef]
- Dydyk, A.M.; Negrete, G.; Cascella, M. Median Nerve Injury; StatPearls Publishing: Treasure Island, FL, USA, 2020. [Google Scholar]
- Grinsell, D.; Keating, C.P. Peripheral Nerve Reconstruction after Injury: A Review of Clinical and Experimental Therapies. BioMed Res. Int. 2014, 2014, 698256. [Google Scholar] [CrossRef] [PubMed]
- Bergmeister, K.D.; Große-Hartlage, L.; Daeschler, S.C.; Rhodius, P.; Böcker, A.; Beyersdorff, M.; Kern, A.O.; Kneser, U.; Harhaus, L. Acute and long-term costs of 268 peripheral nerve injuries in the upper extremity. PLoS ONE 2020, 15, e0229530. [Google Scholar] [CrossRef] [PubMed]
- Mackinnon, S.E. Pathophysiology of nerve compression. Hand Clin. 2002, 18, 231–241. [Google Scholar] [CrossRef]
- Tinel, J. “Tingling” signs with peripheral nerve injuries. 1915. J. Hand Surg. 2005, 30, 87–89. [Google Scholar] [CrossRef] [PubMed]
- Cocks, K.; Torgerson, D. Sample size calculations for pilot randomized trials: A confidence interval approach. J. Clin. Epidemiol. 2013, 66, 197–201. [Google Scholar] [CrossRef] [PubMed]
- Eng, J. Sample size estimation: How many individuals should be studied? Radiology 2003, 227, 309–313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sandvik, L.; Erikssen, J.; Mowinckel, P.; Rødland, E.A. A Method for determining the size of internal pilot studies. Stat. Med. 1996, 15, 1587–1590. [Google Scholar] [CrossRef]
- Bender, R.; Lange, S. Adjusting for multiple testing--when and how? J. Clin. Epidemiol. 2001, 54, 343–349. [Google Scholar] [CrossRef]
- Gordon, T. Nerve Regeneration: Understanding Biology and Its Influence on Return of Function After Nerve Transfers. Hand Clin. 2016, 32, 1031–1117. [Google Scholar] [CrossRef] [PubMed]
- Wood, M.D.; Kemp, S.W.; Weber, C.; Borschel, G.H.; Gordon, T. Outcome measures of peripheral nerve regeneration. Ann. Anat. Anat. Anz. Off. Organ Anat. Ges. 2011, 193, 321–333. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Wu, P.; Chawla, A.; Spinner, R.J.; Yu, C.; Yaszemski, M.J.; Windebank, A.J. Key changes in denervated muscles and their impact on regeneration and reinnervation. Neural Regen. Res. 2014, 9, 1796–1809. [Google Scholar] [CrossRef]
- Bendszus, M.; Stoll, G. Technology Insight: Visualizing peripheral nerve injury using MRI. Nat. Clin. Pract. Cardiovasc. Med. 2005, 1, 45–53. [Google Scholar] [CrossRef] [PubMed]
- Filler, A.G.; Howe, F.A.; Hayes, C.E.; Kliot, M.; Winn, H.R.; Tsuruda, J.S.; Hayes, C.E.; Howe, F.A.; Griffiths, J.R.; Bell, B.A. Magnetic resonance neurography. Lancet 1993, 341, 659–661. [Google Scholar] [CrossRef]
- Bäumer, P.; Pham, M.; Ruetters, M.; Heiland, S.; Heckel, A.; Radbruch, A.; Bendszus, M.; Weiler, M. Peripheral Neuropathy: Detection with Diffusion-Tensor Imaging. Radiology 2014, 273, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Raz, E.; Cercignani, M.; Sbardella, E.; Totaro, P.; Pozzilli, C.; Bozzali, M.; Pantano, P. Clinically Isolated Syndrome Suggestive of Multiple Sclerosis: Voxelwise Regional Investigation of White and Gray Matter. Radiology 2010, 254, 227–234. [Google Scholar] [CrossRef]
- Reiman, E.M.; Jagust, W.J. Brain imaging in the study of Alzheimer’s disease. NeuroImage 2012, 61, 505–516. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Standardized Clinical Examination | |
|---|---|
| Clinical report form for anamnesis | Standardized questionnaires for medical anamnesis and follow-up examinations |
| Clinical report form for sensory motor functioning testing | The results of the following tests are recorded:
|
| Technical Examinations | |
| Electrophysiology Neurosonography MR neurography | Measurement is performed by trained neurologists affiliated to the trauma center and comprises the following procedures:
Measurement performed by a trained radiologist at center C. |
| Standardized Questionnaires | |
| Short Form 36 (SF-36) Morfeld et al., 2011 | The SF-36 is a well-established self-reported measure of health-related quality of life. In addition to the general state of health, the content of the SF-36 is the occurrence of pain and the impairment in everyday life due to mental health problems. The values can vary between 0 and 100 points; lower values reflect poorer well-being, higher values reflect better well-being. |
| Impact of Event Scale—Revised (IES-R) Horowitz et al., 1979 | The IES-R is a 22-item self-disclosure questionnaire that assesses the subjective distress caused by traumatic events. Respondents are asked to identify a specific stressful life event and then indicate how much they were worried or disturbed by it in the last 7 days. The items are rated on a scale from 0 (“not”) to 4 (“extreme”). The IES contains three subscales: intrusion, avoidance, and hyperarousal. |
| Disabilities of Arm, Shoulder, and Hand Scale (DASH) Germann et al., 2003 | The German version of the DASH is regarded as the standard for the subjective assessment of limitations in the functionality of the upper extremities. The questionnaire consists of 30 items, scoring from 1 to 5. Optionally, there is a sports and music module (4 items) and a work and occupation module (4 items). Using an algorithm, the raw data are transformed into a DASH score between 0 (no restrictions) and 100 (maximum restrictions). |
| PainDETECT Freynhagen et al., 2006 | The PainDETECT tool was developed by the German Research Association for Neuropathic Pain. It allows screening for the presence of neuropathic pain. It comprises 9 questions and records the intensity, pattern, and quality of pain. Its sensitivity and specificity are over 80 percent. |
| Depression–Anxiety–Stress Scale (DASS21-G) Nilges and Essau, 2015 | The DASS is a self-disclosure questionnaire that assesses depression, anxiety, and stress without confounding somatic factors. The short version DASS 21G consists of three scales, depression, anxiety, and stress, each with 7 items scoring from “0—did not apply to me at all” to “3—applied very much to me or most of the time”. |
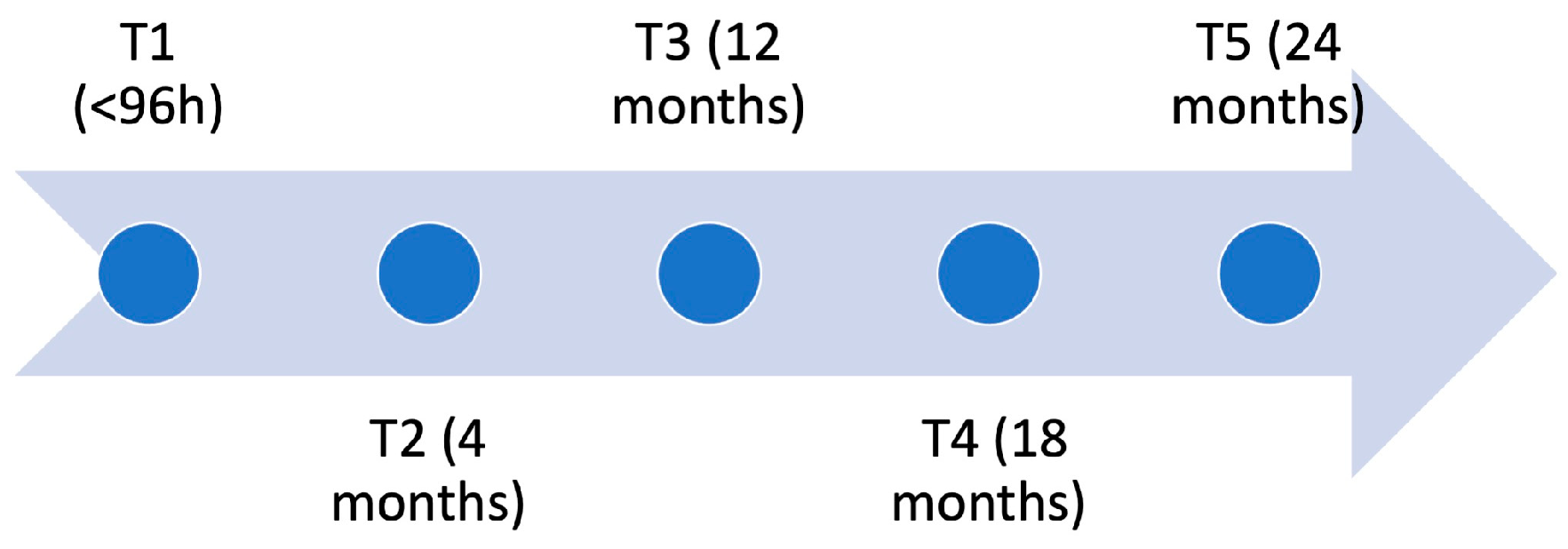
| T1 within 96 h after Injury | T2 4 Months after Injury | T3 12 Months after Injury | T4 18 Months after Injury | T5 24 Months after Injury (only Injuries Proximal to the Elbow) | |
|---|---|---|---|---|---|
| CRF anamnesis | X | X | X | X | X |
| Sensory and motor function testing | only healthy site | X | X | X | X |
| Technical examination | |||||
| Electrophysiology | X | X | X | X | |
| MR neurography | X | X | X | X | X |
| Neurosonography | X | X | X | X | X |
| Questionnaires | |||||
| SF-36 | X | X | X | X | X |
| IES-R | X | X | X | X | X |
| DASH | X | X | X | X | X |
| PainDETECT | X | X | X | X | X |
| DASS | X | X | X | X | X |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aman, M.; Schwarz, D.; Stolle, A.; Bergmeister, K.D.; Boecker, A.H.; Daeschler, S.; Bendszus, M.; Kneser, U.; Harhaus, L. Modern MRI Diagnostics of Upper-Extremity-Related Nerve Injuries—A Prospective Multi-Center Study Protocol for Diagnostics and Follow Up of Peripheral Nerve Injuries. J. Pers. Med. 2022, 12, 1548. https://doi.org/10.3390/jpm12101548
Aman M, Schwarz D, Stolle A, Bergmeister KD, Boecker AH, Daeschler S, Bendszus M, Kneser U, Harhaus L. Modern MRI Diagnostics of Upper-Extremity-Related Nerve Injuries—A Prospective Multi-Center Study Protocol for Diagnostics and Follow Up of Peripheral Nerve Injuries. Journal of Personalized Medicine. 2022; 12(10):1548. https://doi.org/10.3390/jpm12101548
Chicago/Turabian StyleAman, Martin, Daniel Schwarz, Annette Stolle, Konstantin Davide Bergmeister, Arne H. Boecker, Simeon Daeschler, Martin Bendszus, Ulrich Kneser, and Leila Harhaus. 2022. "Modern MRI Diagnostics of Upper-Extremity-Related Nerve Injuries—A Prospective Multi-Center Study Protocol for Diagnostics and Follow Up of Peripheral Nerve Injuries" Journal of Personalized Medicine 12, no. 10: 1548. https://doi.org/10.3390/jpm12101548