
Long-Term Tacrolimus Blood Trough Level and Patient Survival in Adult Liver Transplantation

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
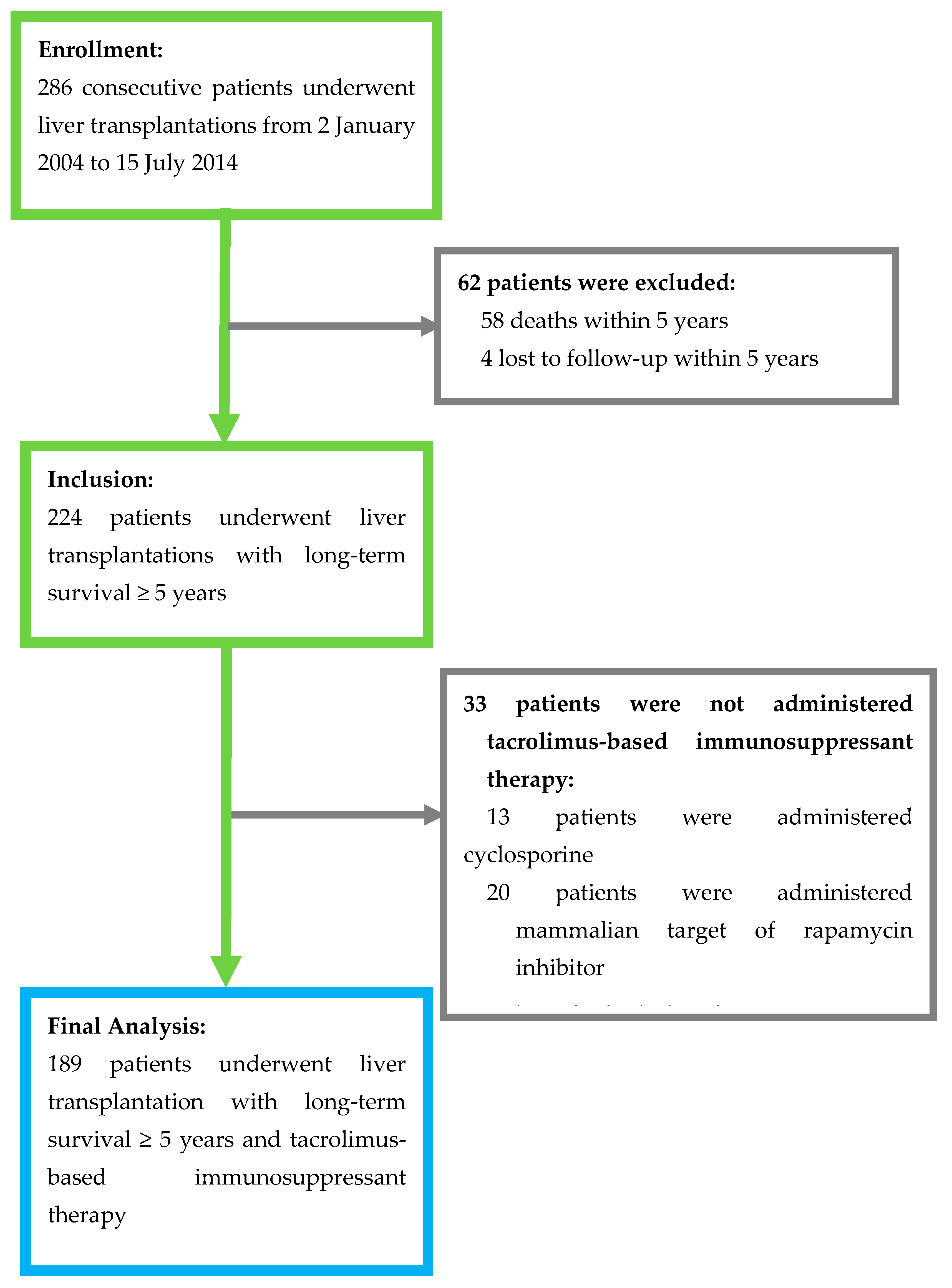
3.1. Patients’ Demographic and Clinical Characteristics
3.2. Predictors of Patients’ Long-Term Survival
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Adam, R.; Karam, V.; Delvart, V.; O’Grady, J.; Mirza, D.; Klempnauer, J.; Burroughs, A. Evolution of indications and results of liver transplantation in Europe. A report from the European Liver Transplant Registry (ELTR). J. Hepatol. 2012, 57, 675–688. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fung, J.; Kelly, D.; Kadry, Z.; Patel-Tom, K.; Eghtesad, B. Immunosuppression in liver transplantation: Beyond calcineurin inhibitors. Liver Transpl. 2005, 11, 267–280. [Google Scholar] [CrossRef] [PubMed]
- European Association for the Study of the Liver. Electronic address EEE. EASL Clinical Practice Guidelines: Liver transplantation. J. Hepatol. 2016, 64, 433–485. [Google Scholar] [CrossRef] [PubMed]
- Wiesner, R.H.; Fung, J.J. Present state of immunosuppressive therapy in liver transplant recipients. Liver Transpl. 2011, 17 (Suppl. 3), S1–S9. [Google Scholar] [CrossRef] [PubMed]
- McAlister, V.C.; Haddad, E.; Renouf, E.; Malthaner, R.A.; Kjaer, M.S.; Gluud, L.L. Cyclosporin versus tacrolimus as primary immunosuppressant after liver transplantation: A meta-analysis. Am. J. Transplant. 2006, 6, 1578–1585. [Google Scholar] [CrossRef]
- O’Grady, J.G.; Hardy, P.; Burroughs, A.K.; Elbourne, D.; UK and Ireland Liver Transplant Study Group. Randomized controlled trial of tacrolimus versus microemulsified cyclosporin (TMC) in liver transplantation: Poststudy surveillance to 3 years. Am. J. Transplant. 2007, 7, 137–141. [Google Scholar] [CrossRef]
- Gonwa, T.A.; Mai, M.L.; Melton, L.B.; Hays, S.R.; Goldstein, R.M.; Levy, M.F. End-stage renal disease (ESRD) after orthotopic liver transplantation (OLTX) using calcineurin-based immunotherapy: Risk of development and treatment. Transplantation 2001, 72, 1934–1939. [Google Scholar] [CrossRef]
- Dantal, J.; Soulillou, J.P. Immunosuppressive drugs and the risk of cancer after organ transplantation. N. Engl. J. Med. 2005, 352, 1371–1373. [Google Scholar] [CrossRef]
- Halloran, P.F. Immunosuppressive drugs for kidney transplantation. N. Engl. J. Med. 2004, 351, 2715–2729. [Google Scholar] [CrossRef] [Green Version]
- Watt, K.D.; Pedersen, R.A.; Kremers, W.K.; Heimbach, J.K.; Charlton, M.R. Evolution of causes and risk factors for mortality post-liver transplant: Results of the NIDDK long-term follow-up study. Am. J. Transplant. 2010, 10, 1420–1427. [Google Scholar] [CrossRef]
- Benitez, C.; Londono, M.C.; Miquel, R.; Manzia, T.M.; Abraldes, J.G.; Lozano, J.J. Prospective multicenter clinical trial of immunosuppressive drug withdrawal in stable adult liver transplant recipients. Hepatology 2013, 58, 1824–1835. [Google Scholar] [CrossRef] [PubMed]
- Londono, M.C.; Rimola, A.; O’Grady, J.; Sanchez-Fueyo, A. Immunosuppression minimization vs. complete drug withdrawal in liver transplantation. J. Hepatol. 2013, 59, 872–879. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lucey, M.R.; Terrault, N.; Ojo, L.; Hay, J.E.; Neuberger, J.; Blumberg, E. Long-term management of the successful adult liver transplant: 2012 practice guideline by the American Association for the Study of Liver Diseases and the American Society of Transplantation. Liver Transpl. 2013, 19, 3–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neuberger, J.M.; Bechstein, W.O.; Kuypers, D.R.; Burra, P.; Citterio, F.; De Geest, S.; Duvoux, C.; Jardine, A.G.; Kamar, N.; Krämer, B.K.; et al. Practical Recommendations for Long-term Management of Modifiable Risks in Kidney and Liver Transplant Recipients: A Guidance Report and Clinical Checklist by the Consensus on Managing Modifiable Risk in Transplantation (COMMIT) Group. Transplantation 2017, 101 (Suppl. 2), S1–S56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Charlton, M.; Levitsky, J.; Aqel, B.; O’Grady, J.; Hemibach, J.; Rinella, M.; Saliba, F. International Liver Transplantation Society Consensus Statement on Immunosuppression in Liver Transplant Recipients. Transplantation 2018, 102, 727–743. [Google Scholar] [CrossRef]
- Hu, F.C. My Stepwise: Stepwise Variable Selection Procedures for Regression Analysis. R Package, Version 0.1.0. Available online: https://CRAN.R-project.org/package=My.stepwise (accessed on 12 October 2020).
- Nagelkerke, N. A note on a general definition of the coefficient of determination. Biometrika 1991, 78, 691–692. [Google Scholar] [CrossRef]
- Moore, D.F. Applied Survival Analysis Using R; Springer International Publishing: Cham, Switzerland, 2016; pp. 84–85. [Google Scholar]
- Rodriguez-Peralvarez, M.; Germani, G.; Papastergiou, V.; Tsochatzis, E.; Thalassinos, E.; Luong, T.V. Early tacrolimus exposure after liver transplantation: Relationship with moderate/severe acute rejection and long-term outcome. J. Hepatol. 2013, 58, 262–270. [Google Scholar] [CrossRef]
- Khalaf, H.; Mourad, W.; El-Sheikh, Y.; Abdo, A.; Helmy, A.; Medhat, Y. Liver transplantation for autoimmune hepatitis: A single-center experience. Transplant. Proc. 2007, 39, 1166–1170. [Google Scholar] [CrossRef]
- Grassi, A.; Ballardini, G. Post-liver transplant hepatitis C virus recurrence: An unresolved thorny problem. World J. Gastroenterol. 2014, 20, 11095–11115. [Google Scholar] [CrossRef]
- Moini, M.; Schilsky, M.L.; Tichy, E.M. Review on immunosuppression in liver transplantation. World J. Hepatol. 2015, 7, 1355–1368. [Google Scholar] [CrossRef]
- Adams, D.H.; Neuberger, J.M. Patterns of graft rejection following liver transplantation. J. Hepatol. 1990, 10, 113–119. [Google Scholar] [CrossRef]
- Mor, E.; Gonwa, T.A.; Husberg, B.S.; Goldstein, R.M.; Klintmalm, G.B. Late-onset acute rejection in orthotopic liver transplantation--associated risk factors and outcome. Transplantation 1992, 54, 821–824. [Google Scholar] [CrossRef] [PubMed]
- Thurairajah, P.H.; Carbone, M.; Bridgestock, H.; Thomas, P.; Hebbar, S.; Gunson, B.K.; Shah, T.; Neuberger, J. Late acute liver allograft rejection; a study of its natural history and graft survival in the current era. Transplantation 2013, 95, 955–959. [Google Scholar] [CrossRef] [PubMed]
- Song, J.L.; Gao, W.; Zhong, Y.; Yan, L.N.; Yang, J.Y.; Wen, T.F.; Yang, J. Minimizing tacrolimus decreases the risk of new-onset diabetes mellitus after liver transplantation. World J. Gastroenterol. 2016, 22, 2133–2141. [Google Scholar] [CrossRef] [PubMed]
- Li, H.Y.; Li, B.; Wei, Y.G.; Yan, L.N.; Wen, T.F.; Zhao, J.C. Higher tacrolimus blood concentration is related to hyperlipidemia in living donor liver transplantation recipients. Dig. Dis. Sci. 2012, 57, 204–209. [Google Scholar] [CrossRef] [PubMed]
- Jia, J.J.; Lin, B.Y.; He, J.J.; Geng, L.; Kadel, D.; Wang, L.; Yu, D.-D.; Shen, T.; Yang, Z.; Ye, Y.-F.; et al. “Minimizing tacrolimus” strategy and long-term survival after liver transplantation. World J. Gastroenterol. 2014, 20, 11363–11369. [Google Scholar] [CrossRef] [PubMed]
- Saliba, F.; Duvoux, C.; Gugenheim, J.; Kamar, N.; Dharancy, S.; Salame, E. Efficacy and Safety of Everolimus and Mycophenolic Acid with Early Tacrolimus Withdrawal after Liver Transplantation: A Multicenter Randomized Trial. Am. J. Transplant. 2017, 17, 1843–1852. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Girlanda, R.; Rela, M.; Williams, R.; O’Grady, J.G.; Heaton, N.D. Long-term outcome of immunosuppression withdrawal after liver transplantation. Transplant. Proc. 2005, 37, 1708–1709. [Google Scholar] [CrossRef]
- Oike, F.; Yokoi, A.; Nishimura, E.; Ogura, Y.; Fujimoto, Y.; Kasahara, M. Complete withdrawal of immunosuppression in living donor liver transplantation. Transplant. Proc. 2002, 34, 1521. [Google Scholar] [CrossRef]
- Mazariegos, G.V.; Reyes, J.; Marino, I.R.; Demetris, A.J.; Flynn, B.; Irish, W.; Starzl, T.E. Weaning of immunosuppression in liver transplant recipients. Transplantation 1997, 63, 243–249. [Google Scholar] [CrossRef] [Green Version]
- Takatsuki, M.; Uemoto, S.; Inomata, Y.; Egawa, H.; Kiuchi, T.; Fujita, S.; Hayashi, M.; Kanematsu, T.; Tanaka, K. Weaning of immunosuppression in living donor liver transplant recipients. Transplantation 2001, 72, 449–454. [Google Scholar] [CrossRef] [PubMed]
- Tisone, G.; Orlando, G.; Cardillo, A.; Palmieri, G.; Manzia, T.M.; Baiocchi, L. Complete weaning off immunosuppression in HCV liver transplant recipients is feasible and favourably impacts on the progression of disease recurrence. J. Hepatol. 2006, 44, 702–709. [Google Scholar] [CrossRef] [PubMed]
- Boudjema, K.; Camus, C.; Saliba, F.; Calmus, Y.; Salame, E.; Pageaux, G.; Ducerf, C.; Duvoux, C.; Mouchel, C.; Renault, A.; et al. Reduced-dose tacrolimus with mycophenolate mofetil vs. standard-dose tacrolimus in liver transplantation: A randomized study. Am. J. Transplant. 2011, 11, 965–976. [Google Scholar] [CrossRef] [PubMed]
- Fischer, L.; Saliba, F.; Kaiser, G.M.; De Carlis, L.; Metselaar, H.J.; De Simone, P. Three-year Outcomes in De Novo Liver Transplant Patients Receiving Everolimus with Reduced Tacrolimus: Follow-Up Results from a Randomized, Multicenter Study. Transplantation 2015, 99, 1455–1462. [Google Scholar] [CrossRef] [PubMed]
- Imai, D.; Yoshizumi, T.; Sakata, K.; Ikegami, T.; Itoh, S.; Harada, N.; Maehara, Y. Long-Term Outcomes and Risk Factors after Adult Living Donor Liver Transplantation. Transplantation 2018, 102, e382–e391. [Google Scholar] [CrossRef] [PubMed]
- Durand, F. How to improve long-term outcome after liver transplantation? Liver Int. 2018, 38 (Suppl. 1), 134–138. [Google Scholar] [CrossRef] [Green Version]
- Edmunds, C.; Ekong, U.D. Autoimmune Liver Disease Post-Liver Transplantation: A Summary and Proposed Areas for Future Research. Transplantation 2016, 100, 515–524. [Google Scholar] [CrossRef] [Green Version]
- Pruthi, J.; Medkiff, K.A.; Esrason, K.T.; Donovan, J.A.; Yoshida, E.M.; Erb, S.R.; Steinbrecher, U.P.; Fong, T.-L. Analysis of causes of death in liver transplant recipients who survived more than 3 years. Liver Transpl. 2001, 7, 811–815. [Google Scholar] [CrossRef]
- Suraweera, D.; Sundaram, V.; Saab, S. Treatment of Hepatitis C Virus Infection in Liver Transplant Recipients. Gastroenterol. Hepatol. (N. Y.) 2016, 12, 23–30. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | All Patients (n = 189) | Alive (n = 173) | Dead (n = 16) | p Value |
|---|---|---|---|---|
| Gender | 0.7899 | |||
| Male | 121 (64.0) | 110 (90.9) | 11 (9.1) | |
| Female | 68 (36.0) | 63 (92.6) | 5 (7.4) | |
| Age at LT (years) | 52.7 ± 9.6 | 52.6 ± 9.5 | 53.4 ± 10.7 | 0.6672 |
| Body weight at LT (kg) | 64.9 ± 12.2 | 65.0 ± 12.3 | 63.7 ± 12.1 | 0.4459 |
| Blood type | 0.8719 | |||
| O | 79 (41.8) | 73 (92.4) | 6 (7.6) | |
| A | 51 (27.0) | 46 (90.2) | 5 (9.8) | |
| B | 42 (22.2) | 39 (92.9) | 3 (7.1) | |
| AB | 17 (9.0) | 15 (88.2) | 2 (11.8) | |
| Graft type | 1.0000 | |||
| Living donor | 144 (76.2) | 132 (91.7) | 12 (8.3) | |
| Deceased donor | 45 (23.8) | 41 (91.1) | 4 (8.9) | |
| Etiology for LT | ||||
| Liver malignancy (HCC) | 72 (38.1) | 66 (91.7) | 6 (8.3) | 1.0000 |
| Alcoholic cirrhosis | 17 (9.0) | 16 (94.1) | 1 (5.9) | 1.0000 |
| HBV cirrhosis | 100 (52.9) | 92 (92.0) | 8 (8.0) | 1.0000 |
| HCV cirrhosis | 42 (22.2) | 38 (90.5) | 4 (9.5) | 0.7577 |
| Fulminant hepatitis | 23 (12.2) | 23 (100) | 0 (0) | 0.2259 |
| Autoimmune disease | 14 (7.4) | 11 (78.6) | 3 (21.4) | 0.1017 |
| Biliary atresia | 5 (2.6) | 5 (100) | 0 (0) | 1.0000 |
| Other | 10 (5.3) | 9 (90) | 1 (10) | 0.5964 |
| Total bilirubin (mg/dL) | 0.973 ± 0.51 | 0.958 ± 1.53 | 1.133 ± 0.69 | 0.6260 |
| Total bilirubin > 1 mg/dL | 60 (31.7) | 53 (88.3) | 7 (11.7) | 0.2770 |
| Total bilirubin > 2 mg/dL | 11 (5.8) | 9 (81.8) | 2 (18.2) | 0.2360 |
| Creatinine (mg/dL) | 1.391 ± 1.25 | 1.279 ± 0.96 | 2.6 ± 2.74 | 0.0201 * |
| Creatinine > 1.5 mg/dL | 31 (16.4) | 23 (74.2) | 8 (25.8) | 0.0010 * |
| ESRD | 5 (2.6) | 2 (40.0) | 3 (60.0) | 0.0050 * |
| Tacrolimus mean level (ng/mL) | 5.249 ± 1.71 | 5.263 ± 1.53 | 5.096 ± 3.12 | 0.9787 |
| Tacrolimus level < 5 ng/mL | 93 (49.2) | 82 (88.2) | 11 (11.8) | 0.1216 |
| Tacrolimus level < 4 ng/mL | 44 (23.3) | 36 (81.8) | 8 (18.2) | 0.0136 * |
| Tacrolimus level < 3 ng/mL | 11 (5.8) | 9 (81.8) | 2 (18.2) | 0.2356 |
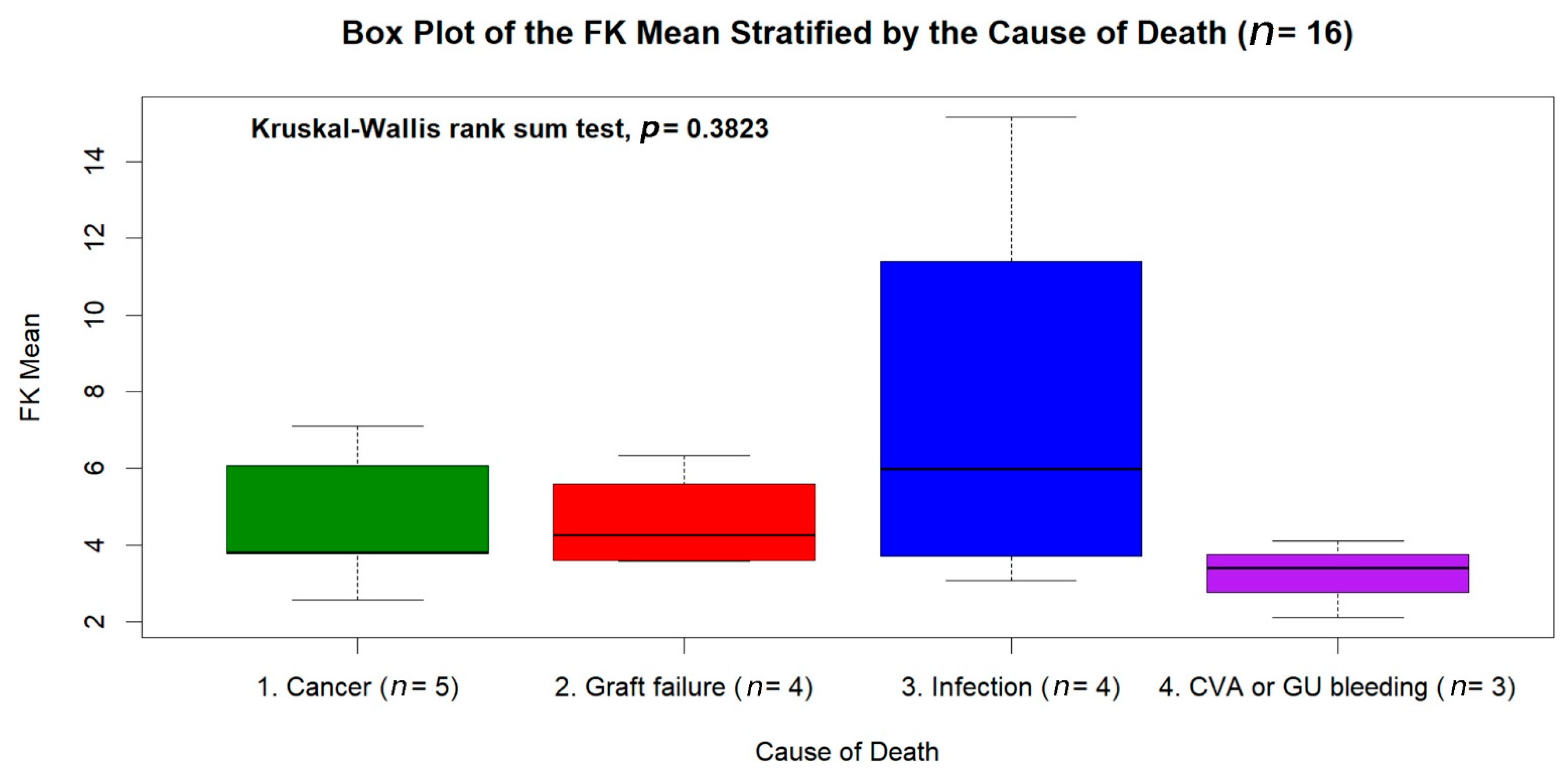
| Causes of Deaths | Number of Subjects |
|---|---|
| Malignancy | 5 (31.25%) |
| De novo: Multiple myeloma, bladder cancer, colon cancer, prostate cancer | 4 |
| Recurrent: Hepatocellular carcinoma | 1 |
| Graft failure | 4 (25.00%) |
| Chronic rejection | 3 |
| Autoimmune hepatitis | 1 |
| Infection | 4 (25.00%) |
| Pneumonia | 3 |
| Urinary tract infection | 1 |
| Cerebral vascular event (intracerebral hemorrhage) | 2 (12.50%) |
| Peptic ulcer bleeding | 1 (6.25%) |
| Covariate 2 | Estimate | Standard Error | Wald’s z Test | p Value | Hazard Ratio (HR) | 95% Confidence Interval (C.I.) |
|---|---|---|---|---|---|---|
| Age at LT ≤ 27.011 years | 5.1286 | 1.3872 | 3.6970 | 0.0002 | 168.7851 | 11.130–2559.512 |
| Autoimmune (including PBC) | 2.0946 | 0.7219 | 2.9015 | 0.0037 | 8.1221 | 1.973–33.431 |
| HCV × Overall survival years | 0.2924 | 0.0914 | 3.1978 | 0.0014 | 1.3397 | 1.120–1.603 |
| Cre > 1.311 × T-Bil > 1.411 mg/dL | 6.8262 | 1.5591 | 4.3784 | <0.0001 | 921.6940 | 43.401–19,573.712 |
| Cre > 1.311 × T-Bil ≤ 0.792 mg/dL | 4.6604 | 1.3294 | 3.5056 | 0.0005 | 105.6778 | 7.805–1430.790 |
| Cre ≤ 1.311 × T-Bil > 0.882 mg/dL | 3.4174 | 1.1871 | 2.8788 | 0.0040 | 30.4913 | 2.977–312.341 |
| Tacrolimus mean ≤ 4.609 or > 10.168 ng/mL | 1.5599 | 0.6479 | 2.4076 | 0.0161 | 4.7581 | 1.336–16.940 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsiao, C.-Y.; Ho, M.-C.; Ho, C.-M.; Wu, Y.-M.; Lee, P.-H.; Hu, R.-H. Long-Term Tacrolimus Blood Trough Level and Patient Survival in Adult Liver Transplantation. J. Pers. Med. 2021, 11, 90. https://doi.org/10.3390/jpm11020090
Hsiao C-Y, Ho M-C, Ho C-M, Wu Y-M, Lee P-H, Hu R-H. Long-Term Tacrolimus Blood Trough Level and Patient Survival in Adult Liver Transplantation. Journal of Personalized Medicine. 2021; 11(2):90. https://doi.org/10.3390/jpm11020090
Chicago/Turabian StyleHsiao, Chih-Yang, Ming-Chih Ho, Cheng-Maw Ho, Yao-Ming Wu, Po-Huang Lee, and Rey-Heng Hu. 2021. "Long-Term Tacrolimus Blood Trough Level and Patient Survival in Adult Liver Transplantation" Journal of Personalized Medicine 11, no. 2: 90. https://doi.org/10.3390/jpm11020090