
Effectiveness of Stretching in Post-Stroke Spasticity and Range of Motion: Systematic Review and Meta-Analysis


 , , and
, , and
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Research Strategy
2.2. Eligibility Criteria
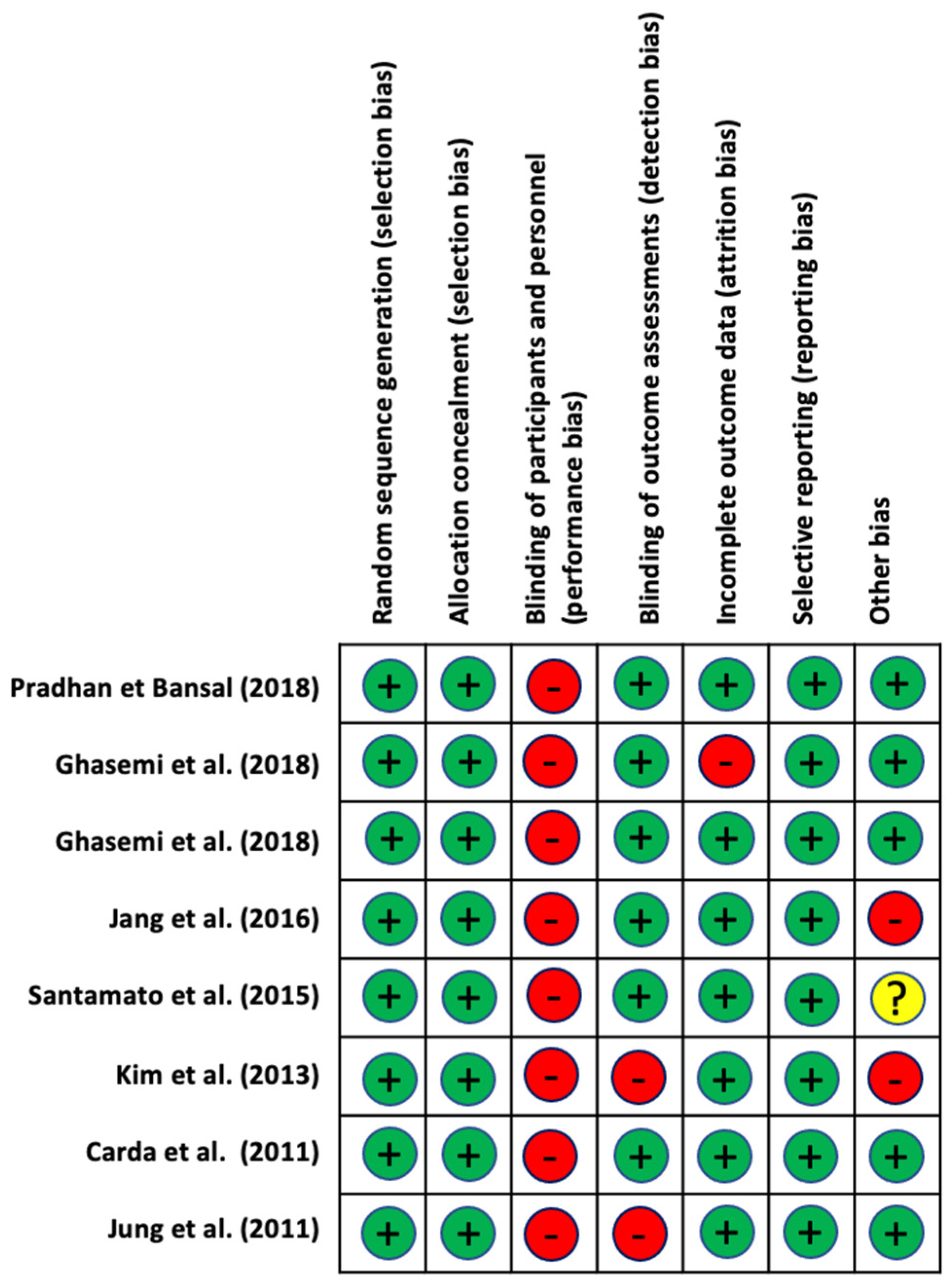
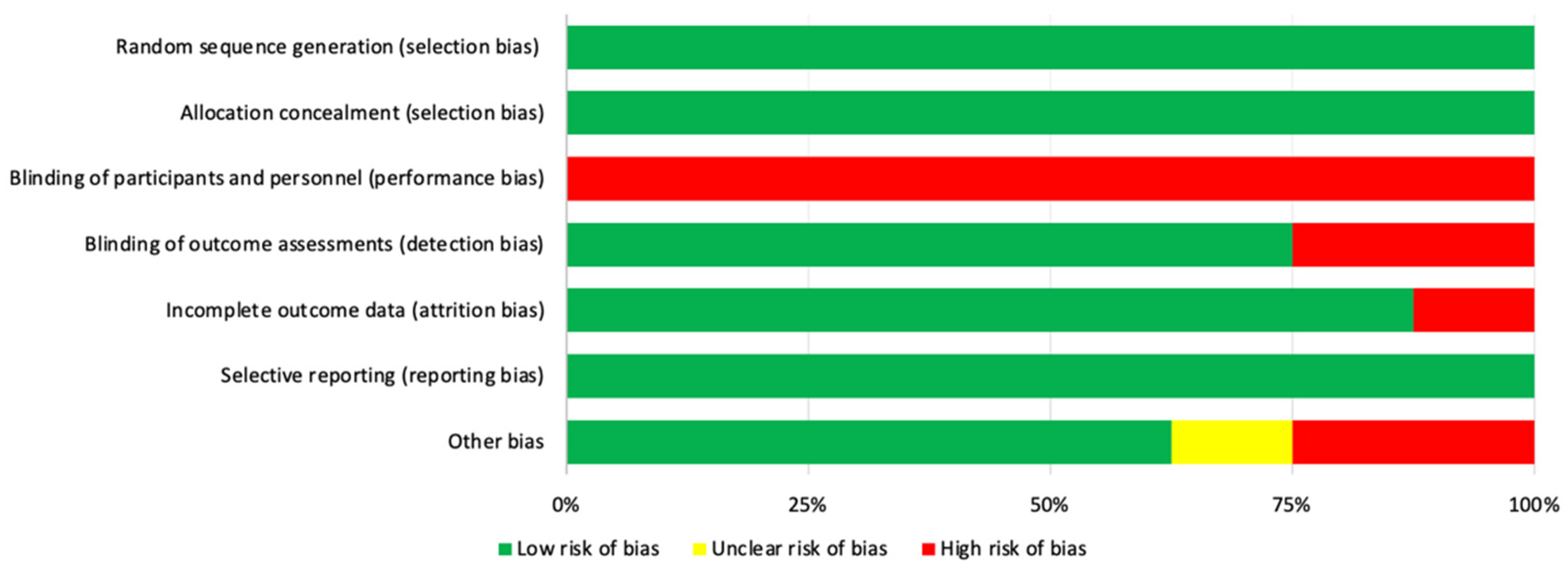
2.3. Assessment of the Methodological Quality and Risk of Bias
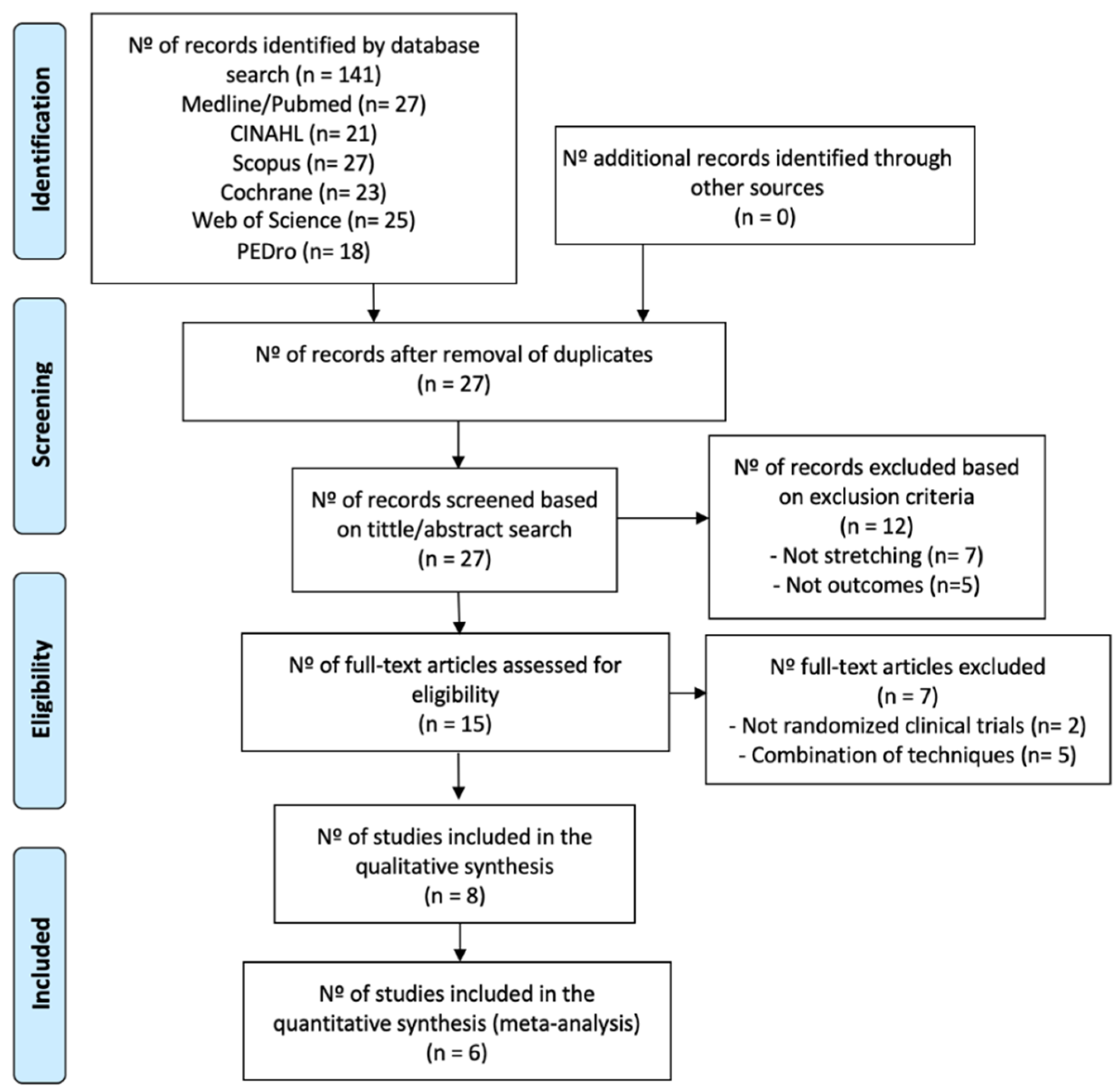
2.4. Selection Process and Data Extraction
2.5. Statistical Analysis
3. Results
3.1. Methodological Quality and Risk of Bias

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Total | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pradhan and Bansal 2018 [40] | 4/10 | - | 0 | 0 | 1 | 0 | 0 | 1 | 0 | 0 | 1 | 1 |
| Ghasemi et al. 2018 [44] | 5/10 | - | 1 | 0 | 1 | 0 | 0 | 1 | 0 | 0 | 1 | 1 |
| Ghasemi et al. 2018 [38] | 6/10 | - | 1 | 0 | 1 | 0 | 0 | 1 | 1 | 0 | 1 | 1 |
| Jang et al. 2016 [45] | 5/10 | - | 1 | 0 | 1 | 0 | 0 | 1 | 0 | 0 | 1 | 1 |
| Santamato et al. 2015 [39] | 8/10 | - | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 1 |
| Kim et al. 2013 [43] | 5/10 | - | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 0 | 1 | 1 |
| Jung et al. 2011 [41] | 4/10 | - | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 1 |
| Carda et al. 2011 [42] | 7/10 | - | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 0 | 1 | 1 |
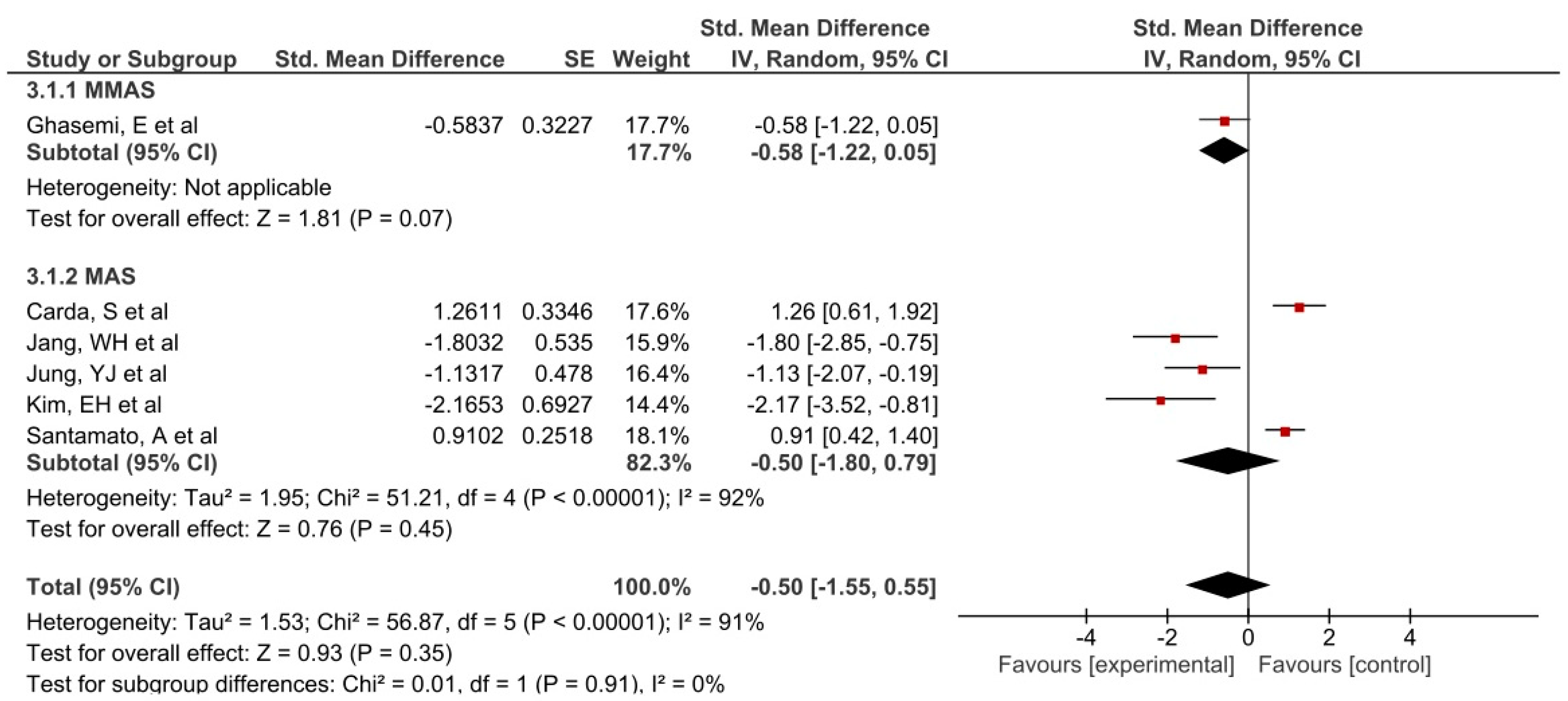
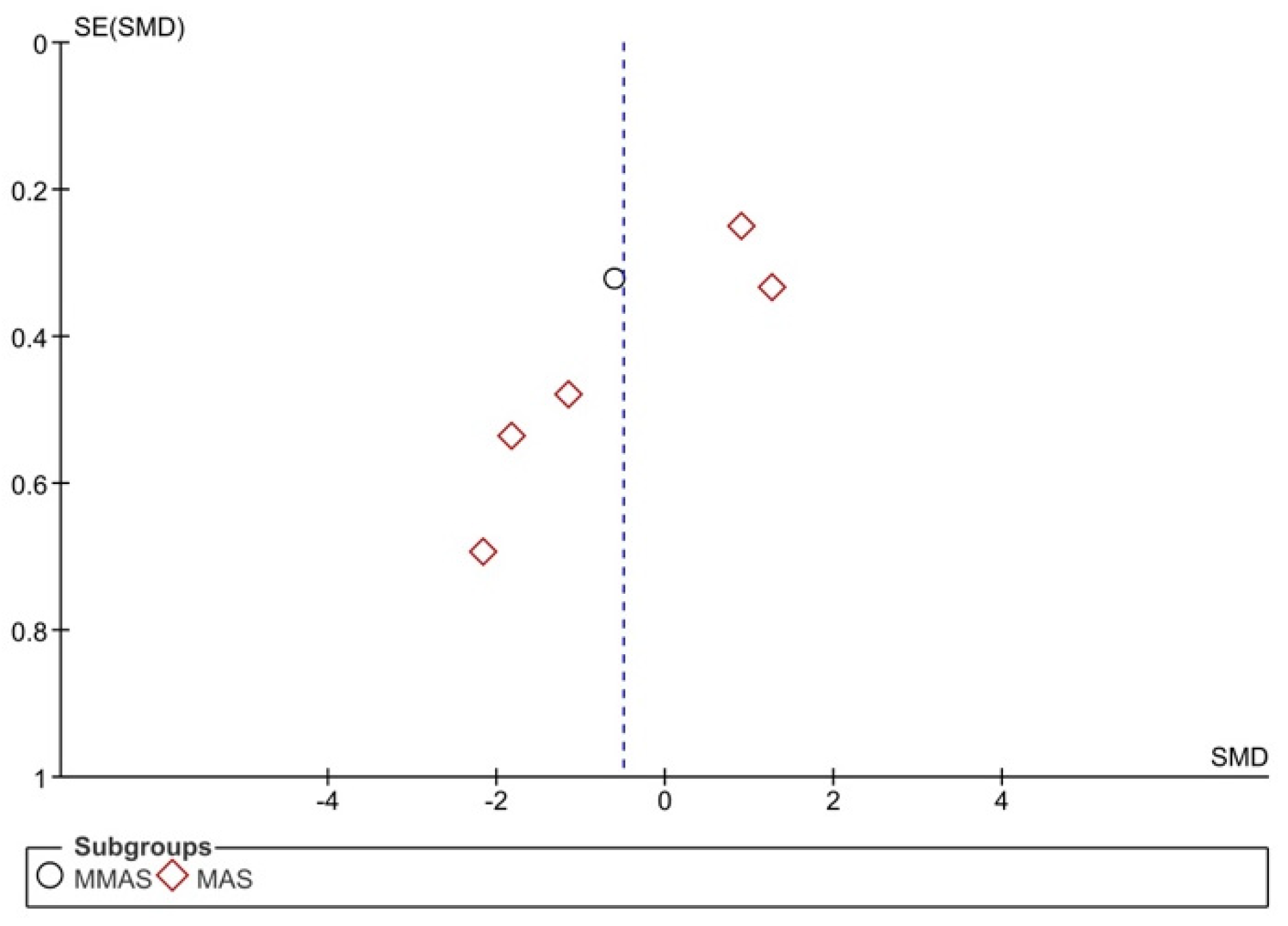
3.2. Synthesis of Results
3.3. Participant Characteristics
3.4. Intervention Characteristics
3.5. Study Groups Included in the Statistical Analysis
Spasticity
3.6. Range of Motion
3.7. Other Outcomes
3.7.1. Activities of Daily Living and Motor Functions
3.7.2. Muscle Strength
3.7.3. Gait
3.7.4. Risk of Fall and Pain
3.7.5. Neural and Mechanical Properties
4. Discussion
4.1. Spasticity
4.2. Range of Motion
4.3. Other Outcomes
4.3.1. Daily Life Activities and Motor Functions
4.3.2. Muscle Strength
4.3.3. Gait
4.3.4. Risk of Fall and Pain
4.3.5. Neural and Mechanical Properties
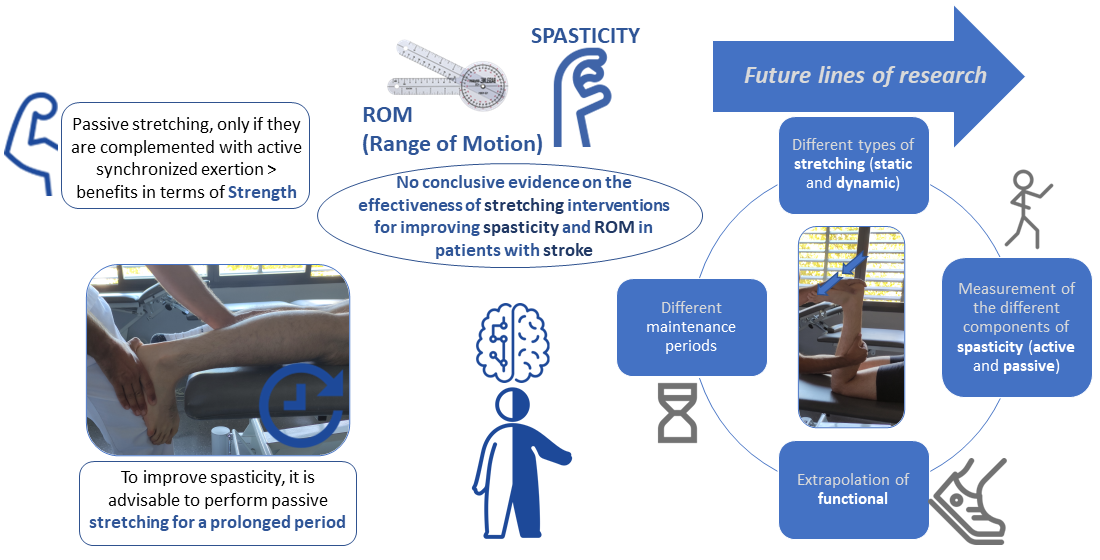
4.4. Study Limitations and Future Research Lines
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- O’Dell, M.W.; Lin, C.-C.D.; Harrison, V. Stroke rehabilitation: Strategies to enhance motor recovery. Annu. Rev. Med. 2009, 60, 55–68. [Google Scholar] [CrossRef] [Green Version]
- Sánchez-Mila, Z.; Salom-Moreno, J.; Fernández-de-Las-Peñas, C. Effects of dry needling on poststroke spasticity, motor function and stability limits: A randomised clinical trial. Acupunct. Med. 2018, 36, 358–366. [Google Scholar] [CrossRef]
- Paul, S.L.; Srikanth, V.K.; Thrift, A.G. The Large and Growing Burden of Stroke. Curr. Drug Targets 2007, 8, 786–793. [Google Scholar] [CrossRef]
- Hilmarsson, A.; Kjartansson, O.; Olafsson, E. Incidence of first stroke: A population study in Iceland. Stroke 2013, 44, 1714–1716. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burke, J.F.; Lisabeth, L.D.; Brown, D.L.; Reeves, M.J.; Morgenstern, L.B. Determining stroke’s rank as a cause of death using multicause mortality data. Stroke 2012, 43, 2207–2211. [Google Scholar] [CrossRef] [Green Version]
- Sommerfeld, D.K.; Eek, E.U.; Svensson, A.K.; Holmqvist, L.W.; von Arbin, M.H. Spasticity After Stroke Its Occurrence and Association With Motor Impairments and Activity Limitations. Stroke 2004, 35, 134–139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lundström, E.; Smits, A.; Borg, J.; Terént, A. Four-fold increase in direct costs of stroke survivors with spasticity compared with stroke survivors without spasticity: The first year after the event. Stroke 2010, 41, 319–324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lance, J.W. The control of muscle tone, reflexes, and movernent: Robert Wartenbeg Lecture. Neurology 1980, 30, 1303–1313. [Google Scholar] [CrossRef] [PubMed]
- Trompetto, C.; Marinelli, L.; Mori, L.; Pelosin, E.; Currà, A.; Molfetta, L.; Abbruzzese, G. Pathophysiology of spasticity: Implications for neurorehabilitation. BioMed Res. Int. 2014, 2014, 354906. [Google Scholar] [CrossRef]
- Crone, C.; Petersen, N.T.; Nielsen, J.E.; Hansen, N.L.; Nielsen, J.B. Reciprocal inhibition and corticospinal transmission in the arm and leg in patients with autosomal dominant pure spastic paraparesis (ADPSP). Brain 2004, 127, 2693–2702. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhakta, B.B.; O’Connor, R.J.; Cozens, J.A. Associated reactions after stroke: A randomized controlled trial of the effect of botulinum toxin type A. J. Rehabil. Med. 2008, 40, 36–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gracies, J.M. Pathophysiology of spastic paresis. I: Paresis and soft tissue changes. Muscle Nerve 2005, 31, 535–551. [Google Scholar] [CrossRef]
- Zijdewind, I.; Thomas, C.K. Motor unit firing during and after voluntary contractions of human thenar muscles weakened by spinal cord injury. J. Neurophysiol. 2003, 89, 2065–2071. [Google Scholar] [CrossRef] [PubMed]
- Wissel, J.; Manack, A.; Brainin, M. Toward an epidemiology of poststroke spasticity. Neurology 2013, 80, S13–S19. [Google Scholar] [CrossRef] [PubMed]
- Bhakta, B.B.; Cozens, J.A.; Chamberlain, M.A.; Bamford, J.M. Impact of botulinum toxin type A on disability and carer burden due to arm spasticity after stroke: A randomised double blind placebo controlled trial. J. Neurol. Neurosurg. Psychiatry 2000, 69, 217–221. [Google Scholar] [CrossRef] [Green Version]
- Hesse, S.; Werner, C. Poststroke Motor Dysfunction and Spasticity: Novel pharmacological and physical treatment strategies. CNS Drugs 2003, 17, 1093–1107. [Google Scholar] [CrossRef]
- Sheean, G. The pathophysiology of spasticity. Eur. J. Neurol. 2002, 9, 3–9. [Google Scholar] [CrossRef]
- Valencia-Chulián, R.; Heredia-Rizo, A.M.; Moral-Munoz, J.A.; Lucena-Anton, D.; Luque-Moreno, C. Dry needling for the management of spasticity, pain, and range of movement in adults after stroke: A systematic review. Complement. Ther. Med. 2020, 52, 102515. [Google Scholar] [CrossRef]
- Kerr, L.; Jewell, V.D.; Jensen, L. Stretching and splinting interventions for poststroke spasticity, hand function, and functional tasks: A systematic review. Am. J. Occup. Ther. 2020, 74. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.; Pei, Z.W.; Xiong, B.D.; Meng, X.M.; Chen, X.L.; Liao, W.J. Use of Kinesio taping in lower-extremity rehabilitation of post-stroke patients: A systematic review and meta-analysis. Complement. Ther. Clin. Pract. 2019, 35, 22–32. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.; Sun, Q.; Wang, H.; Xie, G. Influence of transcutaneous electrical nerve stimulation on spasticity, balance, and walking speed in stroke patients: A systematic review and meta-analysis. J. Rehabil. Med. 2018, 50, 3–7. [Google Scholar] [CrossRef] [Green Version]
- Cabanas-Valdés, R.; Serra-Llobet, P.; Rodriguez-Rubio, P.R.; López-de–Celis, C.; Llauró-Fores, M.; Calvo-Sanz, J. The effectiveness of extracorporeal shock wave therapy for improving upper limb spasticity and functionality in stroke patients: A systematic review and meta-analysis. Clin. Rehabil. 2020, 34, 1141–1156. [Google Scholar] [CrossRef] [PubMed]
- Ortega-Martín, M.E.; Lucena-Antón, D.; Luque-Moreno, C.; Heredia-Rizo, A.M.; Moral-Munoz, J.A. Aplicaciones móviles en el abordaje terapéutico del ictus: Revisión en repositorios comerciales y búsqueda de evidencia [Commercial mobile applications in the therapeutic approach to stroke: Review in main application repositories and scientific evidence]. Rev. Esp. Salud Publica 2019, 93, e201906035. [Google Scholar]
- Luque-Moreno, C.; Ferragut-Garcías, A.; Rodríguez-Blanco, C.; Heredia-Rizo, A.; Oliva-Pascual-Vaca, J.; Kiper, P.; Oliva-Pascual-Vaca, Á. A Decade of Progress Using Virtual Reality for Poststroke Lower Extremity Rehabilitation: Systematic Review of the Intervention Methods. BioMed Res. Int. 2015, 2015, 342529. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bovend’Eerdt, T.J.; Newman, M.; Barker, K.; Dawes, H.; Minelli, C.; Wade, D.T. The Effects of Stretching in Spasticity: A Systematic Review. Arch. Phys. Med. Rehabil. 2008, 89, 1395–1406. [Google Scholar] [CrossRef] [PubMed]
- Freitas, S.R.; Vaz, J.R.; Bruno, P.M.; Andrade, R.; Mil-Homens, P. Stretching Effects: High-intensity & Moderate-duration vs. Low-intensity & Long-duration. Int. J. Sports Med. 2016, 37, 239–244. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Magnusson, S.P.; Simonsen, E.B.; Dyhre-Poulsen, P.; Aagaard, P.; Mohr, T.; Kjaer, M. Viscoelastic stress relaxation during static stretch in human skeletal muscle in the absence of EMG activity. Scand. J. Med. Sci. Sports 1996, 6, 323–328. [Google Scholar] [CrossRef] [PubMed]
- Katalinic, O.M.; Harvey, L.A.; Herbert, R.D. Effectiveness of stretch for the treatment and prevention of contractures in people with neurological conditions: A systematic review. Phys. Ther. 2011, 91, 11–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pin, T.; Dyke, P.; Chan, M. The effectiveness of passive stretching in children with cerebral palsy. Dev. Med. Child Neurol. 2006, 48, 855–862. [Google Scholar] [CrossRef]
- Wallin, D.; Ekblom, B.; Grahn, R.; Nordenborg, T. Improvement of muscle flexibility:A comparison between two techniques. Am. J. Sports Med. 1985, 13, 263–268. [Google Scholar] [CrossRef] [PubMed]
- Fasen, J.M.; O’Connor, A.M.; Schwartz, S.L.; Watson, J.O.; Plastaras, C.T.; Garvan, C.W.; Bulcao, C.; Johnson, S.C.; Akuthota, V. A randomized controlled trial of hamstring stretching: Comparison of four techniques. J. Strength Cond. Res. 2009, 23, 660–667. [Google Scholar] [CrossRef]
- Salazar, A.P.; Pinto, C.; Ruschel Mossi, J.V.; Figueiro, B.; Lukrafka, J.L.; Pagnussat, A.S. Effectiveness of static stretching positioning on post-stroke upper-limb spasticity and mobility: Systematic review with meta-analysis. Ann. Phys. Rehabil. Med. 2019, 62, 274–282. [Google Scholar] [CrossRef] [PubMed]
- Sommerfeld, D.K.; Gripenstedt, U.; Welmer, A.K. Spasticity after stroke: An overview of prevalence, test instruments, and treatments. Am. J. Phys. Med. Rehabil. 2012, 91, 814–820. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; Estarli, M.; Barrera, E.S.A.; et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- da Costa Santos, C.M.; de Mattos Pimenta, C.A.; Nobre, M.R. The PICO strategy for the research question construction and evidence search. Rev. Lat. Am. Enfermagem 2007, 15, 508–511. [Google Scholar] [CrossRef] [Green Version]
- Foley, N.C.; Teasell, R.W.; Bhogal, S.K.; Speechley, M.R. Stroke rehabilitation evidence-based review: Methodology. Top. Stroke Rehabil. 2003, 10, 1–7. [Google Scholar] [CrossRef]
- Higgins, J.P.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- Ghasemi, E.; Khademi-Kalantari, K.; Khalkhali-Zavieh, M.; Rezasoltani, A.; Ghasemi, M.; Baghban, A.A.; Ghasemi, M. The effect of functional stretching exercises on functional outcomes in spastic stroke patients: A randomized controlled clinical trial. J. Bodyw. Mov. Ther. 2018, 22, 1004–1012. [Google Scholar] [CrossRef]
- Santamato, A.; Micello, M.F.; Panza, F.; Fortunato, F.; Picelli, A.; Smania, N.; Logroscino, G.; Fiore, P.; Ranieri, M. Adhesive taping vs. daily manual muscle stretching and splinting after botulinum toxin type A injection for wrist and fingers spastic overactivity in stroke patients: A randomized controlled trial. Clin. Rehabil. 2015, 29, 50–58. [Google Scholar] [CrossRef]
- Pradhan, S.; Bansal, R. Role of corrected-assisted-synchronized-periodic therapy in post-stroke rehabilitation. Neurol. India 2018, 66, 1345–1350. [Google Scholar] [CrossRef]
- Jung, Y.J.; Hong, J.H.; Kwon, H.G.; Song, J.C.; Kim, C.; Park, S.; Ki Kim, Y.; Ahn, S.H.; Jang, S.H. The effect of a stretching device on hand spasticity in chronic hemiparetic stroke patients. NeuroRehabilitation 2011, 29, 53–59. [Google Scholar] [CrossRef]
- Carda, S.; Invernizzi, M.; Baricich, A.; Cisari, C. Casting, taping or stretching after botulinum toxin type A for spastic equinus foot: A single-blind randomized trial on adult stroke patients. Clin. Rehabil. 2011, 25, 1119–1127. [Google Scholar] [CrossRef]
- Kim, E.H.; Chang, M.C.; Seo, J.P.; Jang, S.H.; Song, J.C.; Jo, H.M. The effect of a hand-stretching device during the management of spasticity in chronic hemiparetic stroke patients. Ann. Rehabil. Med. 2013, 37, 235–240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghasemi, E.; Khademi-Kalantari, K.; Khalkhali-Zavieh, M.; Rezasoltani, A.; Ghasemi, M.; Akbarzadeh Baghban, A.; Ghasemi, M. The Effect of Functional Stretching Exercises on Neural and Mechanical Properties of the Spastic Medial Gastrocnemius Muscle in Patients with Chronic Stroke: A Randomized Controlled Trial. J. Stroke Cerebrovasc. Dis. 2018, 27, 1733–1742. [Google Scholar] [CrossRef] [PubMed]
- Jang, W.H.; Kwon, H.C.; Yoo, K.J.; Jang, S.H. The effect of a wrist-hand stretching device for spasticity in chronic hemiparetic stroke patients. Eur. J. Phys. Rehabil. Med. 2016, 52, 65–71. [Google Scholar] [PubMed]
- Gregson, J.M.; Leathley, M.; Moore, A.P.; Sharma, A.K.; Smith, T.L.; Watkins, C.L. Reliability of the tone assessment scale and the modified Ashworth scale as clinical tools for assessing poststroke spasticity. Arch. Phys. Med. Rehabil. 1999, 80, 1013–1016. [Google Scholar] [CrossRef]
- Huang, Y.C.; Chen, P.C.; Tso, H.H.; Yang, Y.C.; Ho, T.L.; Leong, C.P. Effects of kinesio taping on hemiplegic hand in patients with upper limb post-stroke spasticity: A randomized controlled pilot study. Eur. J. Phys. Rehabil. Med. 2019, 55, 551–557. [Google Scholar] [CrossRef]
- Starring, T.D.; Gossman, M.R.; Nicholson, G.G.; Lemons, J. Comparison of cyclic and sustained passive stretching using a mechanical device to increase resting length of hamstring muscles. Phys. Ther. 1988, 68, 314–320. [Google Scholar] [CrossRef]
- Yeh, C.Y.; Chen, J.J.; Tsai, K.H. Quantifying the effectiveness of the sustained muscle stretching treatments in stroke patients with ankle hypertonia. J. Electromyogr. Kinesiol. 2007, 17, 453–461. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.Q.; Chung, S.G.; Bai, Z.; Xu, D.; Van Rey, E.M.; Rogers, M.W.; Johnson, M.E.; Roth, E.J. Intelligent stretching of ankle joints with contracture/spasticity. IEEE Trans. Neural Syst. Rehabil. Eng. 2002, 10, 149–157. [Google Scholar] [CrossRef]
- Brokaw, E.B.; Black, I.; Holley, R.J.; Lum, P.S. Hand Spring Operated Movement Enhancer (HandSOME): A portable, passive hand Exoskeleton for stroke rehabilitation. IEEE Trans. Neural Syst. Rehabil. Eng. 2011, 19, 391–399. [Google Scholar] [CrossRef] [PubMed]
- Bressel, E.; McNair, P.J. The effect of prolonged static and cyclic stretching on ankle joint stiffness, torque relaxation, and gait in people with stroke. Phys. Ther. 2002, 82, 880–887. [Google Scholar] [PubMed] [Green Version]
- Trimble, M.H.; Koceja, D.M. Modulation of the triceps surae h-reflex with training. Int. J. Neurosci. 1994, 76, 293–303. [Google Scholar] [CrossRef] [PubMed]
- Maynard, V.; Bakheit, A.M.; Shaw, S. Comparison of the impact of a single session of isokinetic or isotonic muscle stretch on gait in patients with spastic hemiparesis. Clin. Rehabil. 2005, 19, 146–154. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.L.; Huang, M.H.; Lee, C.L.; Liu, C.W.; Lin, L.J.; Chen, C.H. Effect on spasticity after performance of dynamic-repeated-passive ankle joint motion exercise in chronic stroke patients. Kaohsiung J. Med. Sci. 2006, 22, 610–617. [Google Scholar] [CrossRef] [Green Version]
- Ng, S.S.; Hui-Chan, C.W. The timed up & go test: Its reliability and association with lower-limb impairments and locomotor capacities in people with chronic stroke. Arch. Phys. Med. Rehabil. 2005, 86, 1641–1647. [Google Scholar] [CrossRef]
- Guissard, N.; Duchateau, J. Effect of static stretch training on neural and mechanical properties of the human plantar-flexor muscles. Muscle Nerve 2004, 29, 248–255. [Google Scholar] [CrossRef]
- Tsai, K.H.; Yeh, C.Y.; Chang, H.Y.; Chen, J.J. Effects of a single session of prolonged muscle stretch on spastic muscle of stroke patients. Proc. Natl. Sci. Counc. Repub. China B 2001, 25, 76–81. [Google Scholar] [PubMed]
- Bakheit, A.M.; Maynard, V.; Shaw, S. The effects of isotonic and isokinetic muscle stretch on the excitability of the spinal alpha motor neurones in patients with muscle spasticity. Eur. J. Neurol. 2005, 12, 719–724. [Google Scholar] [CrossRef]
- De Jong, L.D.; Dijkstra, P.U.; Gerritsen, J.; Geurts, A.C.; Postema, K. Combined arm stretch positioning and neuromuscular electrical stimulation during rehabilitation does not improve range of motion, shoulder pain or function in patients after stroke: A randomised trial. J. Physiother. 2013, 59, 245–254. [Google Scholar] [CrossRef] [Green Version]
- Ribeiro, T.; Britto, H.; Oliveira, D.; Silva, E.; Galvão, E.; Lindquist, A. Effects of treadmill training with partial body weight support and the proprioceptive neuromuscular facilitation method on hemiparetic gait: A randomized controlled study. Eur. J. Phys. Rehabil. Med. 2013, 49, 451–461. [Google Scholar] [PubMed]







| Databases | Search |
|---|---|
| Medline/PubMed, CINAHL, Scopus, Cochrane, Web of Science | (“stretch” OR “stretching” OR “stretching exercises” OR “stretching flexibility” OR “mobility” OR “flexibility” OR “range of motion” OR “muscle stretching exercises” OR “passive motion” OR “assisted movement” OR “constraint-induced movement” OR “tissue expansion” OR “tissue expansion devices”) AND (“spasticity” OR “muscle spasticity” OR “pyramidal hypertonia” OR “muscle rigidity” OR “muscle hypertonia”) AND [“stroke”] |
| PEDro | Stretch * spasticity * stroke * |
| Authors (Year) | Sample | Type of Stretching | Age (Average) | Stadium | N Sessions Temporality | Performance of Measurement | Results |
|---|---|---|---|---|---|---|---|
| Pradhan et Bansal (2018) [40] | N = 61 CASP = 31 CT = 30 | CASP = Passive dynamic stretching + active effort TC = Passive dynamic repetitive stretching | 51.15 | Chronicity +6 months | 30 min/session. 6 months. CASP = 6 sessions/day. TC = 2–3 sessions/day. | MAS (0–4), mMRC (0–10), mRS (0–6), Barthel index (0–100) | A significantly greater improvement was obtained in CASP therapy (p < 0.001). However, both improved in all the variables studied. |
| Ghasemi et al. (2018) [44] | N = 45 EG = 30 CT = 15 | Passive static stretching + functional stretching exercises | 56.25 | Chronicity +6 weeks | 30 s/stretch. 3 sessions/week. 4 weeks. | EMG, ultrasound machine. MMAS (0–4), reflex hammer (0–4), goniometer. | Significant improvements in EG tracking were in the angle of penetration (p = 0.006) and muscle thickness (p = 0.030). |
| Ghasemi et al. (2018) [38] | N = 30 EG = 15 CT = 15 | Passive static stretching + functional stretching exercises | 52.27 | Chronicity +3 months | 30 s/stretch. 3 sessions/week. 4 weeks. | MMAS (0–4), reflex hammer (0–4), goniometer. 10 m WTT, TUG, VAS (0–10) | The comparison between the two groups showed significant differences only in spasticity (MMAS p = 0.048) and pain (VAS p = 0.001). |
| Jang et al. (2016) [45] | N = 21 IG = 11 CG = 10 | Passive static stretching with dispositive | 49.1 ± 13.5 | Chronic | 4 min/stretch. 3 stretch/session. 3 sessions/day. 6 days/week. 4 weeks. | MAS, FMA, goniometer | Significant improvements were obtained in the IG in spasticity (MAS) and motor functions (FMA), both observing its follow-up and comparing with the CG (p < 0.05). |
| Santamato et al. (2015) [39] | N = 70 Taping + BTX-A = 35 Stretching + BTX-A = 35 | Passive dynamic stretching + static stretching with splint | 56.9 | Chronicity +6 months | 30 min/session passive dinamic. 30 min/session passive static. 10 days. | MAS (0–4), DAS (0–3) | After two weeks, “taping” obtained a significant reduction in spasticity (MAS p < 0.01), and after one month, it was added the decrease in disability in the upper limb (p < 0.01) compared to “stretching”. |
| Kim et al. (2013) [43] | N = 15 IG = 8 CG = 7 | Passive static stretching with dispositive | 51.2 ± 11.4 | Chronicity +6 months | 10 min/session. 2 sessions/day. 4 weeks. | MAS (0–4) | Comparing both groups, the IG showed a significant decrease in spasticity after treatment (p < 0.001). |
| Jung et al. (2011) [41] | N = 21 IG = 10 CG = 11 | Passive dynamic stretching with dispositive | 46.6 ± 10.9 | Chronicity +6 months | 30 s/stretch. 20 min/session. 2 sessions/day. 6 days/week. 3 weeks. | MAS (0–4) | The IG showed significant improvement during treatment with respect to CG (p < 0.001), but after a week after treatment, spasticity increased again. |
| Carda et al. (2011) [42] | N = 69 Taping + BTX-A = 24 Casting + BTX-A = 27 Stretching + BTX-A = 18 | Passive dynamic stretching | 62.1 | Chronicity +6 months | 30 min/session. 2 sessions/day. 1 week. | MAS, goniometer, 6MWT, 10MWT, FCA, MRC | The comparison between the three groups showed no significant differences (p > 0.05). However, the follow-up of the Stretching group showed improvements in spasticity, PROM, speed, and endurance in the walk. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gomez-Cuaresma, L.; Lucena-Anton, D.; Gonzalez-Medina, G.; Martin-Vega, F.J.; Galan-Mercant, A.; Luque-Moreno, C. Effectiveness of Stretching in Post-Stroke Spasticity and Range of Motion: Systematic Review and Meta-Analysis. J. Pers. Med. 2021, 11, 1074. https://doi.org/10.3390/jpm11111074
Gomez-Cuaresma L, Lucena-Anton D, Gonzalez-Medina G, Martin-Vega FJ, Galan-Mercant A, Luque-Moreno C. Effectiveness of Stretching in Post-Stroke Spasticity and Range of Motion: Systematic Review and Meta-Analysis. Journal of Personalized Medicine. 2021; 11(11):1074. https://doi.org/10.3390/jpm11111074
Chicago/Turabian StyleGomez-Cuaresma, Laura, David Lucena-Anton, Gloria Gonzalez-Medina, Francisco Javier Martin-Vega, Alejandro Galan-Mercant, and Carlos Luque-Moreno. 2021. "Effectiveness of Stretching in Post-Stroke Spasticity and Range of Motion: Systematic Review and Meta-Analysis" Journal of Personalized Medicine 11, no. 11: 1074. https://doi.org/10.3390/jpm11111074