A Qualitative Study to Develop a Privacy and Nondiscrimination Best Practice Framework for Personalized Wellness Programs



Abstract
:1. Introduction
2. Materials and Methods
2.1. Identification and Assessment of Public Stakeholder Concerns
2.2. Interview Guide Development
Legislator/Legislative Staff Interviews
3. Results
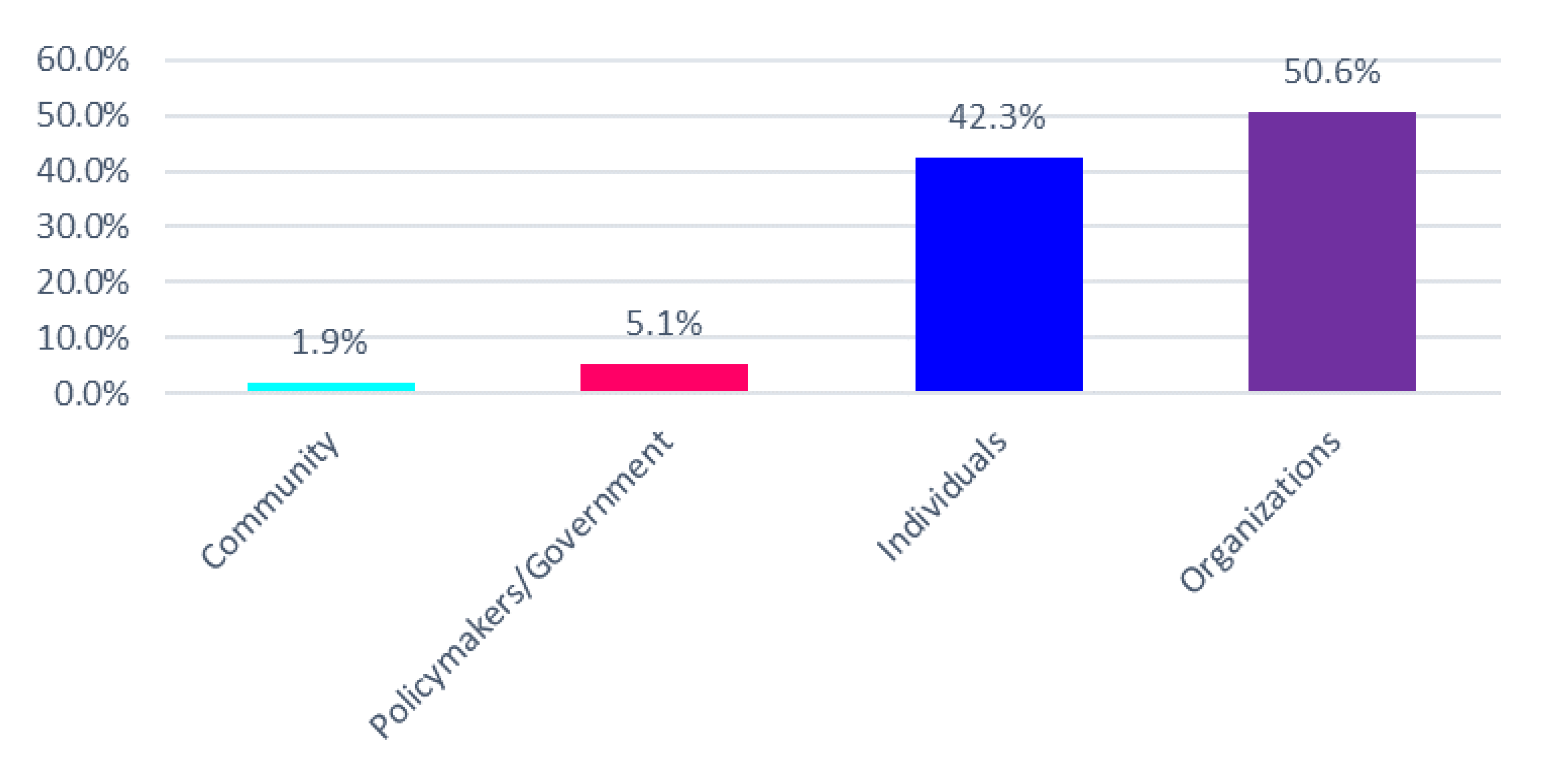
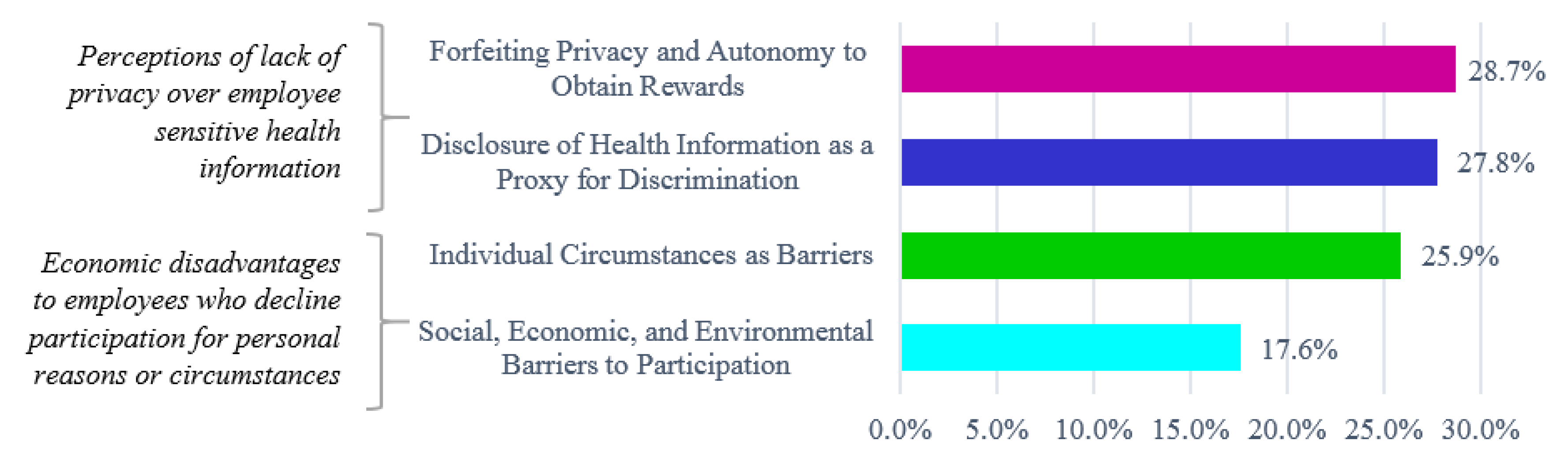
3.1. Assessment of Public Comments, Court Case Documents, and Transcripts of Public Testimony
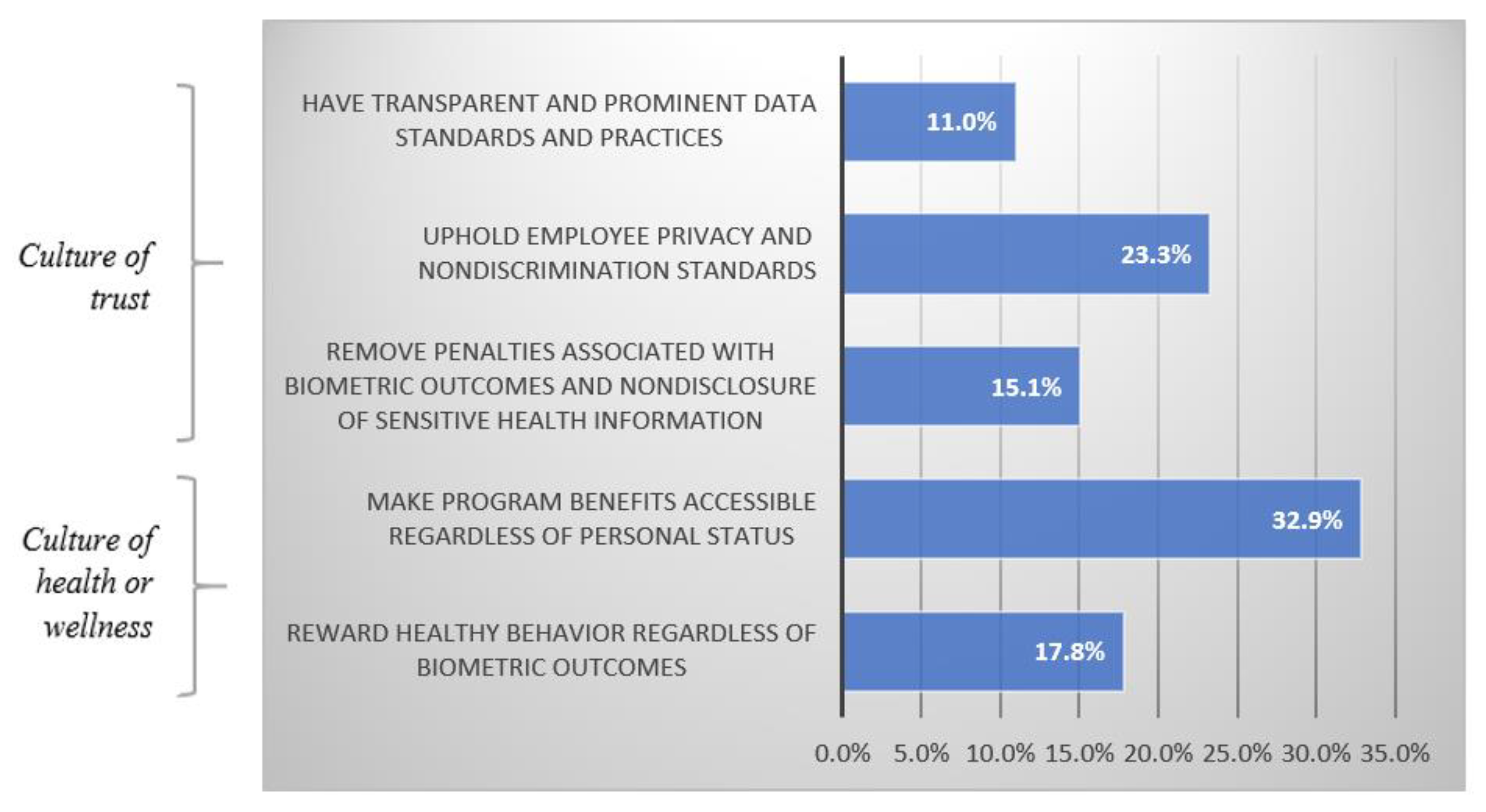
3.2. Determining Privacy and Nondiscrimination Best Practices: Interviews with Legislators and Legislative Staff
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- KFF. Health Insurance Coverage of the Total Population; KFF: Washington, DC, USA; San Francisco, CA, USA, 2019. [Google Scholar]
- Claxton, G.; Rae, M.; Damico, A.; Young, G.; McDermott, D.; Whitmore, H. Health benefits in 2019: Premiums inch higher, employers respond to federal policy. Health Aff. 2019, 38, 1752–1761. [Google Scholar] [CrossRef] [PubMed]
- Does the GDPR Apply to Companies Outside of the EU? Available online: https://gdpr.eu/companies-outside-of-europe/ (accessed on 28 October 2020).
- Anonymous EU Health Programme. Available online: https://ec.europa.eu/health/funding/programme_en (accessed on 26 October 2020).
- Cawley, J.; Price, J.A. A case study of a workplace wellness program that offers financial incentives for weight loss. J. Health Econ. 2013, 32, 794–803. [Google Scholar] [CrossRef] [PubMed]
- Merrill, R.M.; LeCheminant, J.D. Medical cost analysis of a school district worksite wellness program. Prev. Med. Rep. 2016, 3, 159–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, Z.; Baicker, K. Effect of a Workplace Wellness Program on Employee Health and Economic Outcomes: A Randomized Clinical Trial. JAMA 2019, 321, 1491–1501. [Google Scholar] [CrossRef]
- Personalized Medicine Coalition. Wellness in the Workplace: Understanding the Opportunities and Challenges Associated With Employer-Sponsored Genetic Testing Programs for Healthy Patients. In Proceedings of the 16th Annual Personalized Medicine Conference, Boston, MA, USA, 13–14 November 2019. [Google Scholar]
- Kanter, M.; Desrosiers, A. Personalized Wellness Past and Future: Will the Science and Technology Coevolve? Nutr. Today 2019, 54, 174–181. [Google Scholar] [CrossRef]
- Abelson, R. How Healthy Are You? G.O.P. Bill Would Help Employers Find Out. The New York Times, 10 March 2017. [Google Scholar]
- Silverman, R.E. Genetic Testing May Be Coming to Your Office. Wall Str. J. 2015, 16. [Google Scholar]
- Farr, C. Apple Is Offering Free Genetic Tests to All Its Silicon Valley Employees. Available online: https://www.cnbc.com/2019/12/13/apple-teams-with-color-to-offer-free-dna-tests-to-employees.html (accessed on 14 April 2020).
- Helm, A.M.; Georgatos, D. Privacy and mHealth: How Mobile Health “Apps” Fit into a Privacy Framework Not Limited to HIPAA; Social Science Research Network: Rochester, NY, USA, 2014. [Google Scholar]
- Guadarrama, A. Mind the Gap: Addressing Gaps in HIPAA Coverage in the Mobile Health Apps Industry. Hous. L. Rev. 2018, 55, 3876. [Google Scholar]
- Glenn, T.; Monteith, S. Privacy in the Digital World: Medical and Health Data Outside of HIPAA Protections. Curr. Psychiatry Rep. 2014, 16, 494. [Google Scholar] [CrossRef]
- Hudson, K.L.; Pollitz, K. Undermining Genetic Privacy? Employee Wellness Programs and the Law. N. Engl. J. Med. 2017, 377, 1–3. [Google Scholar] [CrossRef]
- Kistler Tiffany Benefits. Wearables Bring Benefits to Wellness Programs But Also Privacy Concerns. Available online: https://ktbenefits.com/2018/04/wearables-bring-benefits-to-wellness-programs-but-also-privacy-concerns/ (accessed on 14 April 2020).
- Wadyka, S. Are Workplace Wellness Programs a Privacy Problem? Available online: https://www.consumerreports.org/health-privacy/are-workplace-wellness-programs-a-privacy-problem/ (accessed on 14 April 2020).
- Steck, M.B. Response to “Workplace Wellness Programs: Educating Patients and Families about Discrimination via Disclosure of Genetic Information”. Clin. J. Oncol. Nurs. 2019, 23, 124. [Google Scholar] [CrossRef] [PubMed]
- Gersema, E. Americans Willing to Make Major Lifestyle Changes to Save Money on Health Care, Study Finds. Available online: https://pressroom.usc.edu/americans-willing-to-make-major-lifestyle-changes-to-save-money-on-health-care-study-finds/ (accessed on 14 April 2020).
- Lebo, H. Digital Future Project. Available online: https://www.digitalcenter.org/digital-future-project/ (accessed on 8 September 2020).
- Keith, K. HHS Proposes New Wellness Demonstration Projects. Health Affairs. Available online: https://www.healthaffairs.org/do/10.1377/hblog20191001.231439/full/ (accessed on 14 April 2020).
- Tie, Y.C.; Birks, M.; Francis, K. Grounded theory research: A design framework for novice researchers. SAGE Open Med. 2019. [Google Scholar] [CrossRef] [Green Version]
- Taormina, R.J.; Sun, R. Antecedents and Outcomes of Psychological Insecurity and Interpersonal Trust Among Chinese People. Psychol. Thought 2015, 8, 173–188. [Google Scholar] [CrossRef] [Green Version]
- Feng, Z.; Vlachantoni, A.; Liu, X.; Jones, K. Social trust, interpersonal trust and self-rated health in China: A multi-level study. Int. J. Equity Health 2016, 15, 180. [Google Scholar] [CrossRef] [Green Version]
- Acosta, J.D.; Whitley, M.D.; May, L.W.; Dubowitz, T.; Williams, M.V.; Chandra, A. Stakeholder Perspectives on a Culture of Health: Key findings. Rand Health Q. 2017, 6, 6. [Google Scholar]
- Chandra, A.; Acosta, J.; Carman, K.G.; Dubowitz, T.; Leviton, L.; Martin, L.T.; Miller, C.; Nelson, C.; Orleans, T.; Tait, M.; et al. Building a National Culture of Health. Rand Health Q. 2017, 6, 3. [Google Scholar]
- Nash, D.B.; Fabius, R.J.; Skoufalos, A.; Clarke, J.L.; Horowitz, M.R. Population Health: Creating a Culture of Wellness; Jones & Bartlett Publishers: Burlington, MA, USA, 2016; ISBN 978-1-284-04792-9. [Google Scholar]
- McDonald, W.S.; Wagner, J.K.; Deverka, P.A.; Woods, L.A.; Peterson, J.F.; Williams, M.S. Genetic testing and employer-sponsored wellness programs: An overview of current vendors, products, and practices. Mol. Genet. Genom. Med. 2020, 8, e1414. [Google Scholar] [CrossRef]
- Roberts, J.L. Will the Recent Workplace Wellness Bill Really Undermine Employee Health Privacy? Available online: https://blog.petrieflom.law.harvard.edu/2017/03/15/will-the-recent-workplace-wellness-bill-really-undermine-employee-health-privacy/ (accessed on 14 April 2020).
- Foxx, V. Text—H.R.1313—115th Congress (2017–2018): Preserving Employee Wellness Programs Act. Available online: https://www.congress.gov/bill/115th-congress/house-bill/1313/text (accessed on 14 April 2020).
- Slaughter, L.M. The Genetic Information Nondiscrimination Act: Why Your Personal Genetics are Still Vulnerable to Discrimination. Surg. Clin. N. Am. 2008, 88, 723–738. [Google Scholar] [CrossRef]
- Genetic Privacy: Genetic Secrets: Protecting Privacy and Confidentiality in the Genetic Era. JAMA 1998, 280, 938. [CrossRef]
- Sokhansanj, B.A. Beyond Protecting Genetic Privacy: Understanding Genetic Discrimination through its Disparate Impact on Racial Minorities. Colum. J. Race L. 2012, 2, 279–309. [Google Scholar] [CrossRef]
- Norman-Bloodsaw v. Lawrence Berkeley Lab. Available online: https://casetext.com/case/norman-bloodsaw-v-lawrence-berkeley-lab (accessed on 14 April 2020).
- Robbins, R. I Tried 5 Genetic Tests to Boost My Fitness. The Result? Fiasco. STAT. 2016. Available online: https://www.statnews.com/2016/11/03/genetic-testing-fitness-nutrition/ (accessed on 14 April 2020).
- Wolfe, J. Note: Coerced into Health: Workplace Wellness Programs and Their Threat to Genetic Privacy—Minnesota Law Review. Available online: https://www.minnesotalawreview.org/wp-content/uploads/2019/01/9Wolfe_MLR.pdf (accessed on 14 April 2020).
- Horwitz, J.R.; Kelly, B.D.; DiNardo, J.E. Wellness Incentives in the Workplace: Cost Savings Through Cost Shifting To Unhealthy Workers. Health Aff. 2013, 32, 468–476. [Google Scholar] [CrossRef] [PubMed]
- Pomeranz, J.L. Participatory Workplace Wellness Programs: Reward, Penalty, and Regulatory Conflict. Milbank Q. 2015, 93, 301–318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Madison, K.M. The Risks of Using Workplace Wellness Programs to Foster a Culture of Health. Health Aff. 2016, 35, 2068–2074. [Google Scholar] [CrossRef] [PubMed]
- Webber, L.S.; Johnson, C.C.; Rose, D.; Rice, J.C. Development of ACTION! Wellness Program for Elementary School Personnel. Obesity 2007, 15, 48S–56S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fink, J.; Rich, J.; Smith, D.; Singh, M.; Sutton, K.; Mueller, G.; Ihrke, D.; Skalla, J.; Cisler, R. Weight Loss Associated With Employee Income in an Incentivized Employee Wellness Program. J. Occup. Environ. Med. 2016, 58, 1181–1184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bélisle-Pipon, J.-C.; Vayena, E.; Green, R.C.; Cohen, I.G. Genetic testing, insurance discrimination and medical research: What the United States can learn from peer countries. Nat. Med. 2019, 25, 1198–1204. [Google Scholar] [CrossRef]
- Shabani, M.; Borry, P. Rules for processing genetic data for research purposes in view of the new EU General Data Protection Regulation. Eur. J. Hum. Genet. 2018, 26, 149–156. [Google Scholar] [CrossRef]
- Rothstein, M.A.; Roberts, J.L.; Guidotti, T.L. Limiting Occupational Medical Evaluations Under the Americans with Disabilities Act and the Genetic Information Nondiscrimination Act; Social Science Research Network: Rochester, NY, USA, 2015. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Reward healthy behavior regardless of biometric outcomes (Culture of health or wellness) |
| “You know, I think that in life in general, you need skin in the game of whatever. And so, I think that there needs to be incentives and—but people are going to have to have responsibility as well. So, it depends on program-to-program. To speak as a whole, you can’t do that. But I generally believe that you should be rewarded for good behavior.” |
| “Well, regardless of the evidence, I still think it’s a good thing to do to encourage people to take better care of themselves, and maybe it doesn’t save the company any money to develop these programs, but I still think, again, just for the individual that it’s a good thing to do, because hopefully people will be healthier, and of course you can’t argue with that. That’s better for the individual and their families and those kind of things. So, I mean, I wasn’t aware that there was very little evidence, but I still think it’s a good thing for the person, and it’s a nice thing for the company to offer. You can’t always give more money, but there’s other things you can do like wellness programs or a extra holiday, that kind of thing, so I still think it’s good for the culture of the organization when they talk about what are great places to work.” |
| Make program benefits accessible, regardless of personal status (Culture of health or wellness) |
| “If you have insurance through your employer, and many people do, a lot of people don’t, so if your employer is providing insurance that’s wonderful. I hope we get to a place where we’re no longer employer-based insurance, but the reality we live in is a lot of people have employer-based insurance. The insurance should be offered, and that’s it. The door closes. The cost match of the insurance is the cost match of the insurance. Then you get into pregnancy, you get into people recovering from surgery. All those things start affecting your ability to participate in a wellness program. You click in, you click off. Who’s going to measure that? What are you going to do? So, the cost of your health insurance should be across the board the same for all employees, and employers should never be able to look into your mental health records, your physical health records.” |
| “I can see the thing about employees wanting to participate and needing to participate because of the incentive, but I could also see a lot of employees that might work a second job and might have childcare issues and might have a 100 and so reasons why they can’t if it’s after work or if it’s during work. Their jobs might not be good, so, I mean, I think that the best way to do it is to have a wellness program in a workplace that is free, accessible to everybody without going through all of that.” |
| “I think the employer should provide both the time and the means to participate in the wellness programs. I don’t think they should be required to be completed outside of the work areas-- hours or outside of the work areas so if it involves going to a gym, the gym should be on site and it should be during work hours. I don’t think it should be a burden on the employee.” |
| “I think that if employers are going to offer a wellness program, then it should be conducive to the workplace and where their employees are. It should not be a burden to employees, and I believe many people probably feel similarly in that respect… So really trying to make it seamless and truly integrated within the workplace would be ideal for a wellness program. Something that could be accomplished in the office or wherever the workplace is and that there’s an understanding between employer and employee that the facilities or the whatever the activities are associated with the program can be done during work hours.” |
| Remove penalties associated with biometric outcomes and nondisclosure of sensitive health information (Culture of trust) |
| “I think you probably hit it spot-on in terms of running the risk of coercion… obviously employers have a justification for being invested in their employees’ wellness. It makes sense, especially if they’re providing healthcare. At the same time, you really need to ensure through the incentives you’re crafting around these that it truly is a voluntary program and that the employees are protected so that the incentives are not so great that then it flips to be almost punitive if they are not participating, and so it’s definitely finding that balance and attenuating the program to ensure that there are the right guardrails around the program and the employees.” |
| “Well, I mean, I do think people are responsible for their health, but I think it’s their personal choice, so, again, going back to how wellness programs are set-up, I think it should be set-up in an incentive-type way to encourage people to do it, but if people choose not to do it, I mean, that’s their choice. I don’t think you should make people do it. I think about myself, how I gain and lose the same 10 to 15 pounds every year, and I only lose the weight, but I have my mind really set toward it, and I’m really determined that even if someone pushes me into it if I’m not determined it’s not going to happen, just like people who have a drinking problem or smoking, trying to quit smoking, that they have to first want to do it, and then it’s still hard. And I think someone that’s pregnant, I mean, even though some people that are pregnant still exercise or whatever, but it’s still a choice, so I don’t think people should be penalized.” |
| Uphold employee privacy and nondiscrimination standards (Culture of trust) |
| “So I think that there’s a careful line that we have to ensure that at a policy level when we look at regulations around employee wellness programs that we don’t cross a line into essentially what would be medical underwriting from an employer standpoint, and, you know, the ACA did a lot in terms of progress for medical underwriting, but now that we’re in this new era of employee wellness and more open data and more accessible data, I think we really need to be mindful that it is being used in the right way and wouldn’t be used in a discriminatory fashion, wouldn’t be used to cherry pick employees in hiring process potentially or promotional process, and that it isn’t, you know, it isn’t used, again, against employees. That it wouldn’t be turned into a punitive measure.” |
| “You know, of course I believe in respecting one’s privacy, and I think that’s a true balance somewhere in between so that employees are able to keep their privacy but be able to participate in the wellness programs. What the answer is to get there, I think that’s where you have so much debate within the agencies and also within Congress. So-- but I think… for the most part, I believe that you need to have a balance of respecting employees’ privacy and still be able to utilize the programs.” |
| “…I think that’s a difficult one. I mean, if you have a large pool of employees, potentially if you’re not giving the names of employees but just giving statistics, it might be easier, but, you know, in smaller workplaces, it might become very evident which employee you’re talking about when you’re looking at some of those metrics. Yeah, I think that’s something that the workarounds on that might be a little more difficult.” |
| Have transparent and prominent data standards and practices (Culture of trust) |
| “…To whom does the health data belong? Is it the company who’s making the assessment or does it belong to the employee or the employer? Is it shared? So, making all of those elements clear, that’s not a very straightforward process right now. I mean, companies don’t have standards that cross across each company, or what have you.” |
| “Well, I definitely think before an employee gets involved in a wellness program there has to be some type of contractual agreement around the issue of privacy and how the information gets used. Now, of course because of hackings, cybersecurity and those kind of things there’s always a chance that your information can get out, but when you get a credit card there’s that chance also, but I think there has to be agreements set-up in the beginning about how and why that information can be used in the privacy document.” |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hendricks-Sturrup, R.M.; Cerminara, K.L.; Lu, C.Y. A Qualitative Study to Develop a Privacy and Nondiscrimination Best Practice Framework for Personalized Wellness Programs. J. Pers. Med. 2020, 10, 264. https://doi.org/10.3390/jpm10040264
Hendricks-Sturrup RM, Cerminara KL, Lu CY. A Qualitative Study to Develop a Privacy and Nondiscrimination Best Practice Framework for Personalized Wellness Programs. Journal of Personalized Medicine. 2020; 10(4):264. https://doi.org/10.3390/jpm10040264
Chicago/Turabian StyleHendricks-Sturrup, Rachele M., Kathy L. Cerminara, and Christine Y. Lu. 2020. "A Qualitative Study to Develop a Privacy and Nondiscrimination Best Practice Framework for Personalized Wellness Programs" Journal of Personalized Medicine 10, no. 4: 264. https://doi.org/10.3390/jpm10040264