XGBoost Improves Classification of MGMT Promoter Methylation Status in IDH1 Wildtype Glioblastoma

 ,
, 
Abstract
:1. Introduction
2. Results
2.1. Patient Characteristics
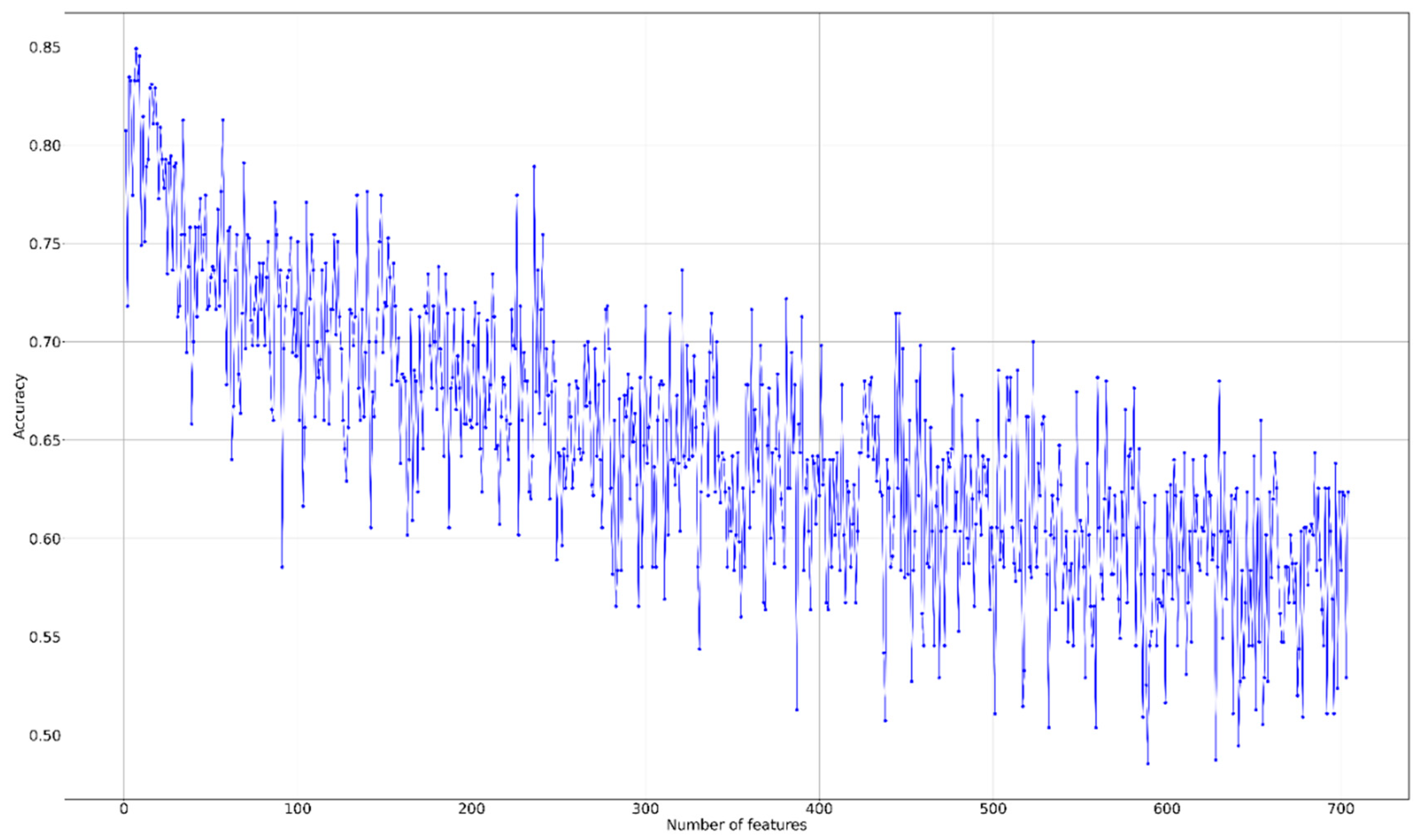
2.2. Feature Selection and Radiomics Signature Building
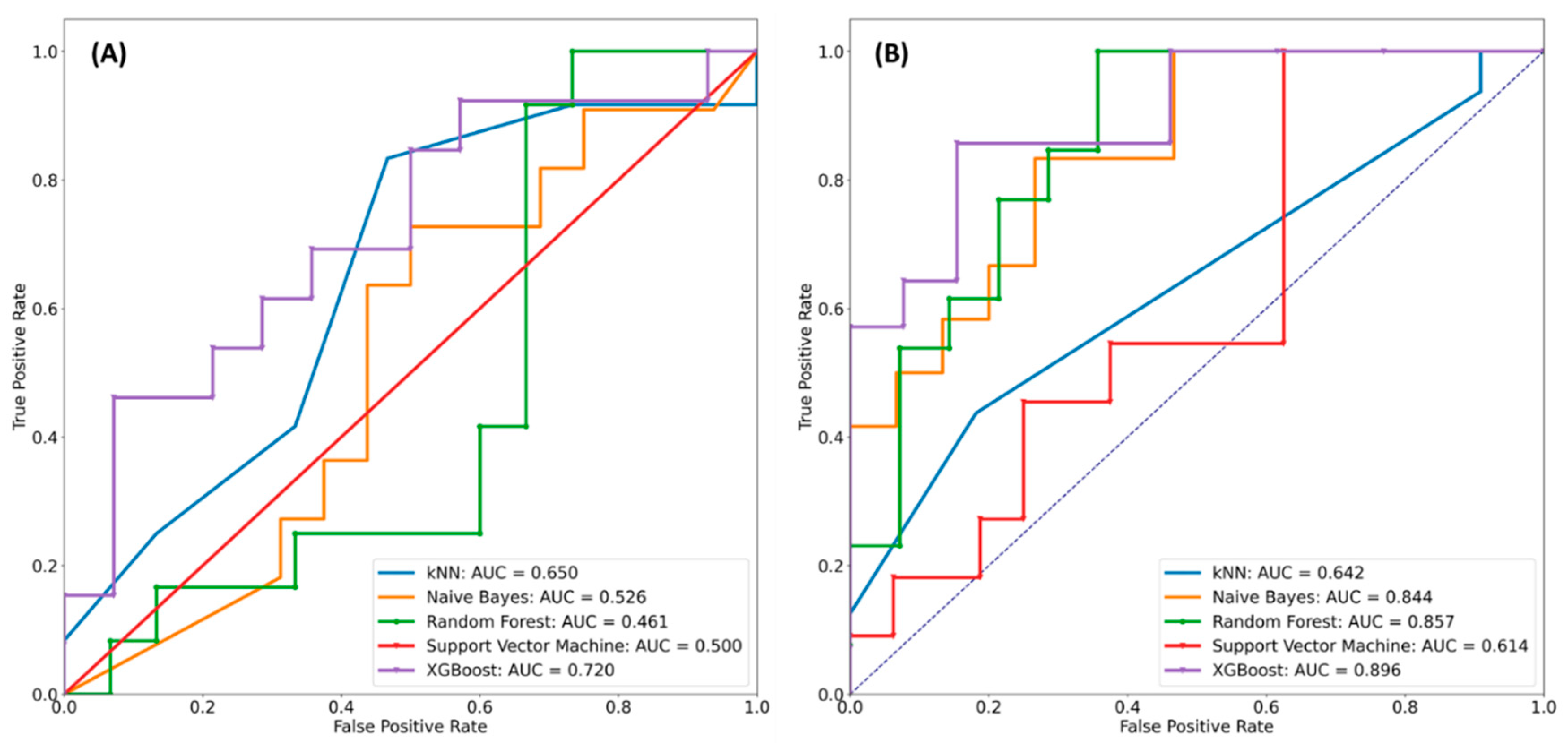
2.3. Supervised Learning Classification
2.4. Comparison with Previous Radiomics Studies in Terms of Prediction of O6-Methylguanine-DNA Methyltransferase (MGMT) Status
3. Discussion
4. Materials and Methods
4.1. Patient Cohort
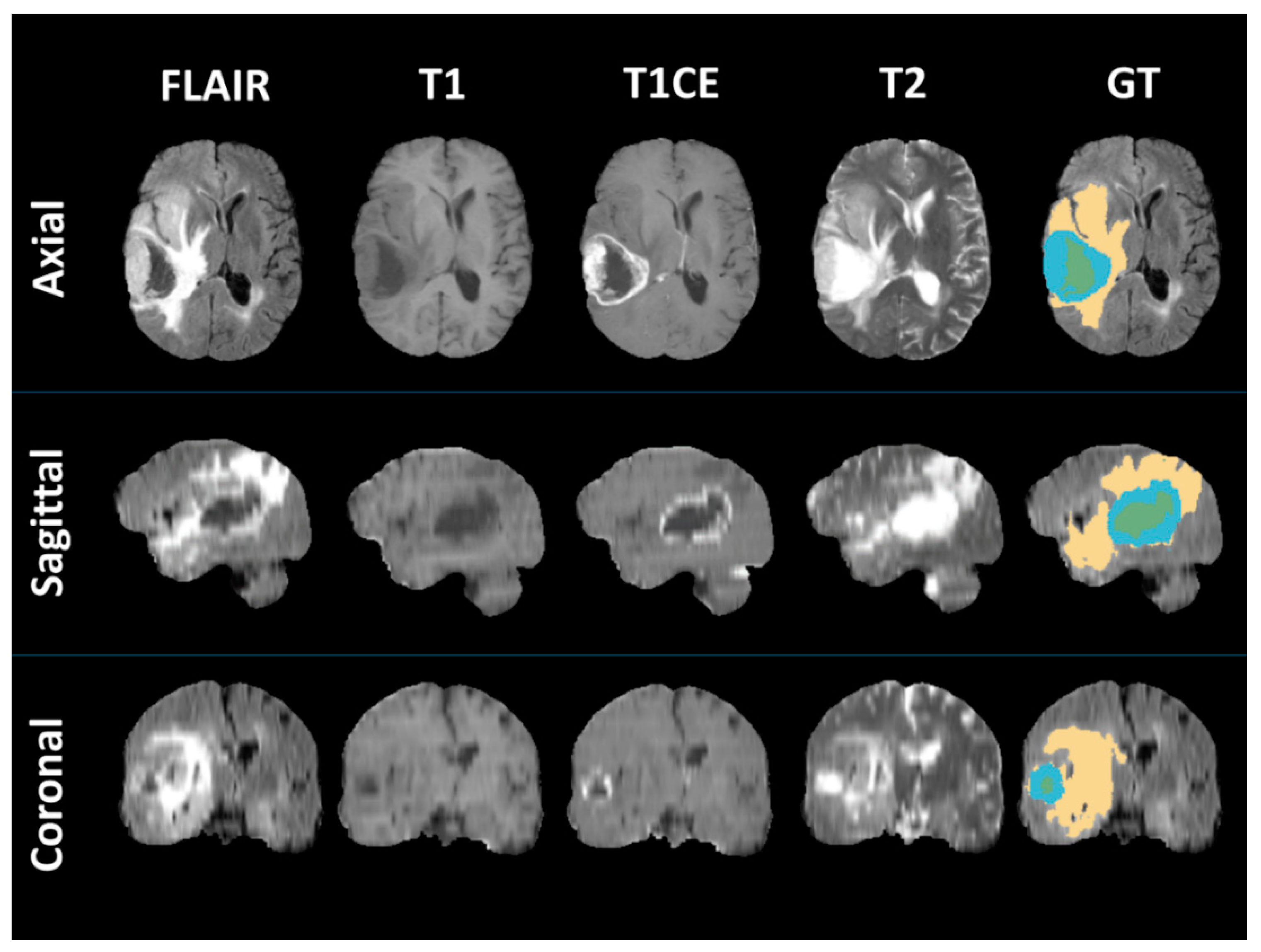
4.2. MRI Segmentation and Radiomics Features
4.3. Radiomics Feature Selection
4.4. Machine Learning
4.5. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Hanif, F.; Muzaffar, K.; Perveen, K.; Malhi, S.M.; Simjee, S.U. Glioblastoma multiforme: A review of its epidemiology and pathogenesis through clinical presentation and treatment. Asian Pac. J. Cancer Prev. 2017, 18, 3–9. [Google Scholar]
- Hau, P.; Stupp, R.; Hegi, M.E. MGMT methylation status: The advent of stratified therapy in glioblastoma? Dis. Mark. 2007, 23, 159242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lao, J.; Chen, Y.; Li, Z.C.; Li, Q.; Zhang, J.; Liu, J.; Zhai, G. A deep learning-based radiomics model for prediction of survival in glioblastoma multiforme. Sci. Rep. 2017, 7, 10353. [Google Scholar] [CrossRef]
- Lambin, P.; Leijenaar, R.T.; Deist, T.M.; Peerlings, J.; De Jong, E.E.; Van Timmeren, J.; Sanduleanu, S.; Larue, R.T.; Even, A.J.; Jochems, A. Radiomics: The bridge between medical imaging and personalized medicine. Nat. Rev. Clin. Oncol. 2017, 14, 749–762. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Liu, Z.; He, L.; Chen, X.; Pan, D.; Ma, Z.; Liang, C.; Tian, J.; Liang, C. Radiomics signature: A potential biomarker for the prediction of disease-free survival in early-stage (I or II) non—Small cell lung cancer. Radiology 2016, 281, 947–957. [Google Scholar] [CrossRef] [PubMed]
- Coroller, T.P.; Grossmann, P.; Hou, Y.; Velazquez, E.R.; Leijenaar, R.T.; Hermann, G.; Lambin, P.; Haibe-Kains, B.; Mak, R.H.; Aerts, H.J. CT-based radiomic signature predicts distant metastasis in lung adenocarcinoma. Radiother. Oncol. 2015, 114, 345–350. [Google Scholar] [CrossRef]
- Kickingereder, P.; Bonekamp, D.; Nowosielski, M.; Kratz, A.; Sill, M.; Burth, S.; Wick, A.; Eidel, O.; Schlemmer, H.P.; Radbruch, A.; et al. Radiogenomics of glioblastoma: Machine learning–based classification of molecular characteristics by using multiparametric and multiregional mr imaging features. Radiology 2016, 281, 907–918. [Google Scholar] [CrossRef] [Green Version]
- Li, Z.-C.; Bai, H.; Sun, Q.; Li, Q.; Liu, L.; Zou, Y.; Chen, Y.; Liang, C.; Zheng, H. Multiregional radiomics features from multiparametric MRI for prediction of MGMT methylation status in glioblastoma multiforme: A multicentre study. Eur. Radiol. 2018, 28, 3640–3650. [Google Scholar] [CrossRef]
- Xi, Y.-b.; Guo, F.; Xu, Z.L.; Li, C.; Wei, W.; Tian, P.; Liu, T.T.; Liu, L.; Chen, G.; Ye, J.; et al. Radiomics signature: A potential biomarker for the prediction of MGMT promoter methylation in glioblastoma. J. Magn. Reson. Imaging 2018, 47, 1380–1387. [Google Scholar] [CrossRef]
- Wei, J.; Yang, G.; Hao, X.; Gu, D.; Tan, Y.; Wang, X.; Dong, D.; Zhang, S.; Wang, L.; Zhang, H.; et al. multi-sequence and habitat-based MRI radiomics signature for preoperative prediction of MGMT promoter methylation in astrocytomas with prognostic implication. Eur. Radiol. 2019, 29, 877–888. [Google Scholar] [CrossRef] [Green Version]
- Korfiatis, P.; Kline, T.L.; Coufalova, L.; Lachance, D.H.; Parney, I.F.; Carter, R.E.; Buckner, J.C.; Erickson, B.J. MRI texture features as biomarkers to predict MGMT methylation status in glioblastomas. Med. Phys. 2016, 43, 2835–2844. [Google Scholar] [CrossRef] [PubMed]
- Jiang, S.; Jiang, S.; Rui, Q.; Wang, Y.; Heo, H.Y.; Zou, T.; Yu, H.; Zhang, Y.; Wang, X.; Du, Y.; et al. Discriminating MGMT promoter methylation status in patients with glioblastoma employing amide proton transfer-weighted MRI metrics. Eur. Radiol. 2018, 28, 2115–2123. [Google Scholar] [CrossRef] [PubMed]
- Kong, Z.; Jiang, C.; Zhu, R.; Feng, S.; Wang, Y.; Li, J.; Chen, W.; Liu, P.; Zhao, D.; Ma, W.; et al. 18F-FDG-PET-based Radiomics signature predicts MGMT promoter methylation status in primary diffuse glioma. Cancer Imaging 2019, 19, 58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Han, S.; Liu, Y.; Cai, S.J.; Qian, M.; Ding, J.; Larion, M.; Gilbert, M.R.; Yang, C. IDH mutation in glioma: Molecular mechanisms and potential therapeutic targets. Br. J. Cancer 2020, 122, 1580–1589. [Google Scholar] [CrossRef]
- Deng, L.; Xiong, P.; Luo, Y.; Bu, X.; Qian, S.; Zhong, W.; Lv, S. Association between IDH1/2 mutations and brain glioma grade. Oncol. Lett. 2018, 16, 5405–5409. [Google Scholar] [CrossRef] [Green Version]
- Jiang, C.; Kong, Z.; Liu, S.; Feng, S.; Zhang, Y.; Zhu, R.; Chen, W.; Wang, Y.; Lyu, Y.; You, H.; et al. Fusion radiomics features from conventional MRI Predict mgmt promoter methylation status in lower grade gliomas. Eur. J. Radiol. 2019, 121, 108714. [Google Scholar] [CrossRef]
- Crisi, G.; Filice, S. Predicting MGMT promoter methylation of glioblastoma from dynamic susceptibility contrast perfusion: A radiomic approach. J. Neuroimaging 2020. [Google Scholar] [CrossRef]
- Levner, I.; Drabycz, S.; Roldan, G.; De Robles, P.; Cairncross, J.G.; Mitchell, R. Predicting MGMT methylation status of glioblastomas from MRI texture. In Proceeding of the Medical Image Computing and Computer-Assisted Intervention—MICCAI 2009, London, UK, 20–24 September 2009; Springer: Berlin/Heidelberg, Germany, 2009. [Google Scholar]
- Sung Soo, A.; Shin, N.Y.; Chang, J.H.; Kim, S.H.; Kim, E.H.; Kim, D.W.; Lee, S.K. Prediction of methylguanine methyltransferase promoter methylation in glioblastoma using dynamic contrast-enhanced magnetic resonance and diffusion tensor imaging. J. Neurosurg. JNS 2014, 121, 367–373. [Google Scholar]
- Sasaki, T.; Kinoshita, M.; Fujita, K.; Fukai, J.; Hayashi, N.; Uematsu, Y.; Okita, Y.; Nonaka, M.; Moriuchi, S.; Uda, T.; et al. Radiomics and MGMT promoter methylation for prognostication of newly diagnosed glioblastoma. Sci. Rep. 2019, 9, 14435. [Google Scholar] [CrossRef]
- Clark, K.; Vendt, B.; Smith, K.; Freymann, J.; Kirby, J.; Koppel, P.; Moore, S.; Phillips, S.; Maffitt, D.; Pringle, M.; et al. The Cancer Imaging Archive (TCIA): Maintaining and operating a public information repository. J. Digit. Imaging 2013, 26, 1045–1057. [Google Scholar] [CrossRef] [Green Version]
- Batchala, P.P.; Muttikkal, T.J.E.; Donahue, J.H.; Patrie, J.T.; Schiff, D.; Fadul, C.E.; Mrachek, E.K.; Lopes, M.B.; Jain, R.; Patel, S.H. Neuroimaging-based classification algorithm for predicting 1p/19q-codeletion status in IDH-mutant lower grade gliomas. Am. J. Neuroradiol. 2019, 40, 426–432. [Google Scholar] [CrossRef] [Green Version]
- Hsieh, K.L.-C.; Chen, C.-Y.; Lo, C.-M. Radiomic model for predicting mutations in the isocitrate dehydrogenase gene in glioblastomas. Oncotarget 2017, 8, 45888. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bangalore Yogananda, C.G.; Shah, B.R.; Vejdani-Jahromi, M.; Nalawade, S.S.; Murugesan, G.K.; Yu, F.F.; Pinho, M.C.; Wagner, B.C.; Mickey, B.; Patel, T.R. A novel fully automated MRI-based deep-learning method for classification of IDH mutation status in brain gliomas. Neuro Oncol. 2019, 22, 402–411. [Google Scholar]
- González, S.R.; Zemmoura, I.; Tauber, C. Deep convolutional neural network to predict 1p19q co-deletion and IDH1 mutation status from MRI in low grade gliomas. In Proceedings of the 10th International Conference on Pattern Recognition Systems (ICPES-2019), Tours, France, 8–10 July 2019; p. 2. [Google Scholar]
- Radke, J.; Koch, A.; Pritsch, F.; Schumann, E.; Misch, M.; Hempt, C.; Lenz, K.; Löbel, F.; Paschereit, F.; Heppner, F.L.; et al. Predictive MGMT status in a homogeneous cohort of IDH wildtype glioblastoma patients. Acta Neuropathol. Commun. 2019, 7, 89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brennan, C.W.; Verhaak, R.G.; McKenna, A.; Campos, B.; Noushmehr, H.; Salama, S.R.; Zheng, S.; Chakravarty, D.; Sanborn, J.Z.; Berman, S.H. The somatic genomic landscape of glioblastoma. Cell 2013, 155, 462–477. [Google Scholar]
- Bady, P.; Sciuscio, D.; Diserens, A.C.; Bloch, J.; Van Den Bent, M.J.; Marosi, C.; Dietrich, P.Y.; Weller, M.; Mariani, L.; Heppner, F.L.; et al. MGMT methylation analysis of glioblastoma on the Infinium methylation BeadChip identifies two distinct CpG regions associated with gene silencing and outcome, yielding a prediction model for comparisons across datasets, tumor grades, and CIMP-status. Acta Neuropathol. 2012, 124, 547–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Menze, B.H.; Jakab, A.; Bauer, S.; Kalpathy-Cramer, J.; Farahani, K.; Kirby, J.; Burren, Y.; Porz, N.; Slotboom, J.; Wiest, R.; et al. The multimodal brain tumor image segmentation benchmark (BRATS). IEEE Trans. Med. Imaging 2015, 34, 1993–2024. [Google Scholar] [CrossRef]
- Bakas, S.; Akbari, H.; Sotiras, A.; Bilello, M.; Rozycki, M.; Kirby, J.S.; Freymann, J.B.; Farahani, K.; Davatzikos, C. Advancing the cancer genome atlas glioma MRI collections with expert segmentation labels and radiomic features. Sci. Data 2017, 4, 170117. [Google Scholar] [CrossRef] [Green Version]
- Gooya, A.; Pohl, K.M.; Bilello, M.; Cirillo, L.; Biros, G.; Melhem, E.R.; Davatzikos, C. GLISTR: Glioma image segmentation and registration. IEEE Trans. Med. Imaging 2012, 31, 1941–1954. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.-W.; Lin, C.-J. Combining SVMs with various feature selection strategies. In Feature Extraction; Guyon, I., Nikravesh, M., Gunn, S., Zadeh, L.A., Eds.; Springer: Berlin, Germany, 2006; pp. 315–324. [Google Scholar]
- Deo Rahul, C. Machine learning in medicine. Circulation 2015, 132, 1920–1930. [Google Scholar]
- Blumenthal, D.T.; Artzi, M.; Liberman, G.; Bokstein, F.; Aizenstein, O.; Bashat, D.B. Classification of high-grade glioma into tumor and nontumor components using support vector machine. Am. J. Neuroradiol. 2017, 38, 908. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Havaei, M.; Farley, D.; Biard, A.; Courville, A.; Bengio, Y.; Pal, C.; Jodoin, P.M.; Larochelle, H. Brain tumor segmentation with deep neural networks. Med. Image Anal. 2017, 35, 18–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kunimatsu, A.; Kunimatsu, N.; Yasaka, K.; Akai, H.; Kamiya, K.; Watadani, T.; Mori, H.; Abe, O. Machine learning-based texture analysis of contrast-enhanced mr imaging to differentiate between glioblastoma and primary central nervous system lymphoma. Magn. Reson. Med. Sci. 2019, 18, 44–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papp, L.; Pötsch, N.; Grahovac, M.; Schmidbauer, V.; Woehrer, A.; Preusser, M.; Mitterhauser, M.; Kiesel, B.; Wadsak, W.; Beyer, T.; et al. Glioma survival prediction with combined analysis of in vivo 11C-MET PET features, ex vivo features, and patient features by supervised machine learning. J. Nuclear Med. 2018, 59, 892–899. [Google Scholar]
- Le, N.-Q.-K.; Ho, Q.-T.; Ou, Y.-Y. Incorporating deep learning with convolutional neural networks and position specific scoring matrices for identifying electron transport proteins. J. Comput. Chem. 2017, 38, 2000–2006. [Google Scholar] [CrossRef] [PubMed]
- Do, D.T.; Le, T.Q.T.; Le, N.Q.K. Using deep neural networks and biological subwords to detect protein S-sulfenylation sites. Brief. Bioinform. 2020. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Methylated (n = 26) | Unmethylated (n = 27) | |
|---|---|---|
| Age (mean ± SD, years) | 53 ± 16.43 | 60.83 ± 12.12 |
| Gender | ||
| Male | 8 | 19 |
| Female | 18 | 8 |
| TCGA subtype | ||
| Classical | 6 | 8 |
| Mesenchymal | 9 | 8 |
| Neural | 1 | 2 |
| Proneural | 6 | 9 |
| Methylation class | ||
| CL_1 | 1 | 4 |
| CL_2 | 8 | 9 |
| CL_3 | 6 | 5 |
| CL_4 | 4 | 5 |
| CL_6 | 3 | 4 |
| No. | Feature Name | Modality | Matrix | Type |
|---|---|---|---|---|
| 1 | HISTO_ET_T2_Bin6 | T2 | First Order | Histogram |
| 2 | TEXTURE_GLRLM_ED_T2_GLV | T2 | GLRLM | Texture |
| 3 | TEXTURE_GLSZM_NET_FLAIR_ZP | FLAIR | GLSZM | Wavelet Texture |
| 4 | TEXTURE_GLSZM_NET_FLAIR_SZE | FLAIR | GLSZM | Wavelet Texture |
| 5 | TEXTURE_GLSZM_NET_FLAIR_ZSN | FLAIR | GLSZM | Wavelet Texture |
| 6 | TEXTURE_GLSZM_NET_T1_ZSN | T1 | GLSZM | Wavelet Texture |
| 7 | TEXTURE_GLSZM_NET_T1_SZE | T1 | GLSZM | Wavelet Texture |
| 8 | HISTO_ED_T2_Bin5 | T2 | First Order | Histogram |
| 9 | TEXTURE_GLSZM_NET_T1_ZP | T1 | GLSZM | Wavelet Texture |
| Learning Algorithm | Hyperparameter Range | Optimal Value |
|---|---|---|
| K-nearest neighbors (kNN) | n_neighbors = [1, 2, 3, .., 30] | 1 |
| weights = [uniform, distance] | uniform | |
| metric = [euclidean, manhattan, minkowski] | minkowski | |
| Random Forest | max_depth = [10, 20, 30, 40, 50, …, 100, 110, None] | None |
| max_features = [‘auto’, ‘sqrt’] | sqrt | |
| min_samples_leaf = [1, 2, 3, 4, 5] | 1 | |
| min_samples_split = [2, 4, 6, 8, 10, 12] | 10 | |
| n_estimators = [100, 200, 300, 400, 500, 600, …, 2000] | 2000 | |
| Support vector machine (SVM) | C = [0.001, 0.01, 0.1, 1, 10] | 0.001 |
| gamma = [0.001, 0.01, 0.1, 1] | 0.1 | |
| kernel = [rbf, linear, poly, sigmoid] | poly | |
| eXtreme Gradient Boosting (XGBoost) | min_child_weight = [1, 2, 3, 4, 5, 6, 7, 8, 9, 10] | 1 |
| gamma = [0.5, 1, 1.5, 2, 2.5, 3, 3.5, 4, 4.5, 5] | 2.5 | |
| subsample = [0, 0.2, 0.4, 0.6, 0.8, 1] | 0.6 | |
| colsample_bytree = [0, 0.2, 0.4, 0.6, 0.8, 1] | 0.4 | |
| max_depth = [10, 20, 30, 40, 50, …, 100, 110, None] | 50 | |
| n_estimators = [100, 200, 300, 400, 500, 600, …, 2000] | 200 |
| Biomarkers | Classifiers | Sensitivity | Specificity | Accuracy | |
|---|---|---|---|---|---|
| Jiang et al. | 15 features | Mann–Whitney test | 0.821 | 0.857 | 0.886 |
| Levner et al. | 8 features | L1-regularized neural networks | 0.854 | 0.9 | 0.877 |
| Xi et al. | 63 features | Support vector machine | 0.888 | 0.838 | 0.866 |
| Crisi et al. | 14 features | Multilayer perceptron | 0.75 | 0.85 | - |
| Ahn et al. | - | Mann–Whitney U-test | 0.563 | 0.852 | - |
| Korfiatis et al. | 4 features | Support vector machine | 0.803 | 0.813 | - |
| Sasaki et al. | 5 features | LASSO | 0.67 | 0.66 | 0.67 |
| Our study | 9 features | XGBoost | 0.88 | 0.887 | 0.887 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Le, N.Q.K.; Do, D.T.; Chiu, F.-Y.; Yapp, E.K.Y.; Yeh, H.-Y.; Chen, C.-Y. XGBoost Improves Classification of MGMT Promoter Methylation Status in IDH1 Wildtype Glioblastoma. J. Pers. Med. 2020, 10, 128. https://doi.org/10.3390/jpm10030128
Le NQK, Do DT, Chiu F-Y, Yapp EKY, Yeh H-Y, Chen C-Y. XGBoost Improves Classification of MGMT Promoter Methylation Status in IDH1 Wildtype Glioblastoma. Journal of Personalized Medicine. 2020; 10(3):128. https://doi.org/10.3390/jpm10030128
Chicago/Turabian StyleLe, Nguyen Quoc Khanh, Duyen Thi Do, Fang-Ying Chiu, Edward Kien Yee Yapp, Hui-Yuan Yeh, and Cheng-Yu Chen. 2020. "XGBoost Improves Classification of MGMT Promoter Methylation Status in IDH1 Wildtype Glioblastoma" Journal of Personalized Medicine 10, no. 3: 128. https://doi.org/10.3390/jpm10030128