
The Benefits and Challenges of the Multimodal Treatment in Advanced/Metastatic Malignant Melanoma
 , , , and
, , , and {kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
3. Discussion
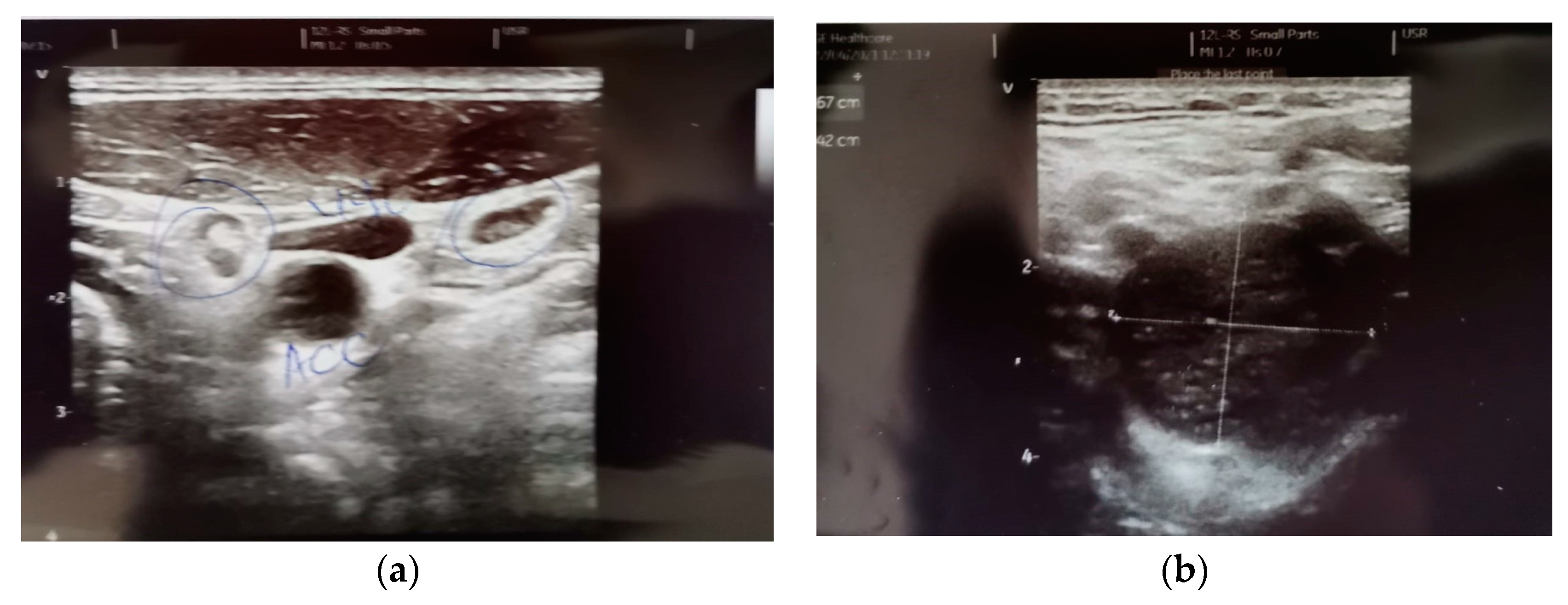
- The description, in all of the imaging investigations carried out initially, but also in the reassessment of the treatment, of a left latero-cervical adenopathy, stages II-III, with dimensional progression under treatment with BRAF/MEK inhibitors and Nivolumab—histopathologically and immunohistochemically invalidated during the surgical verification—schwannoma;
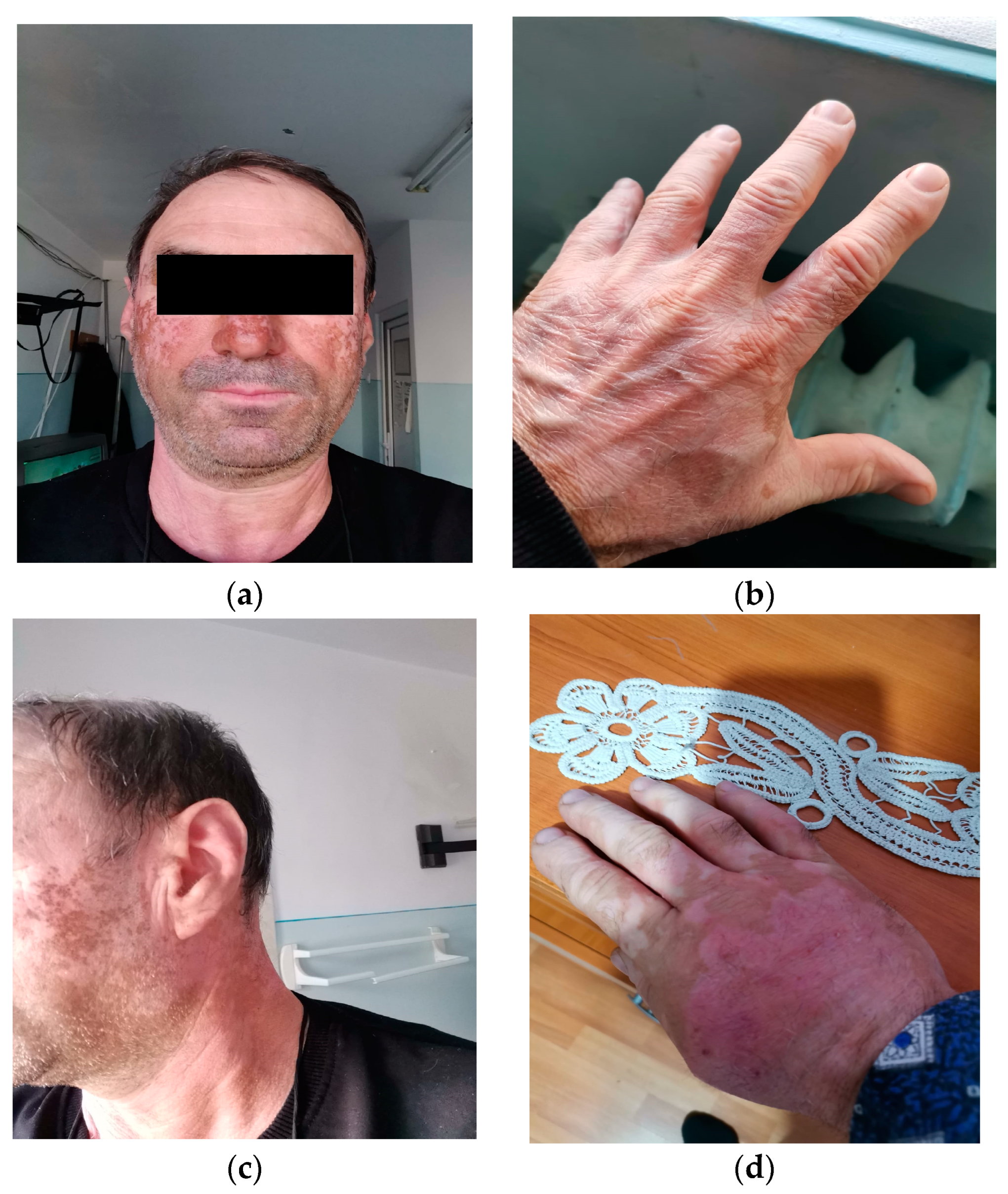
- The development of a “vitiligo”-like cutaneous lesion with evolution at a distance, during the treatment with Nivolumab;
- A 3rd degree severity skin reaction when BRAF/MEK inhibitors were reintroduced into the treatment—an allergic reaction to treatment vs. an adverse skin reaction;
- An imaging response of intrathoracic ganglia to the treatment with Dacarbazine, after the progression of these lesions under targeted treatment and immune checkpoint inhibitors;
- Throughout the evolution of the disease, a single cerebral secondary determination occurred, thus challenging the therapeutic decision.
- Highly increased clinical effectiveness;
- Combined therapies (e.g., BRAF/MEK inhibitors) that increase clinical tolerance and decrease toxicity;
- Active interventions in advanced disease in order to increase the disease-free interval with the approval of new therapies for adjuvant purposes (e.g., Nivolumab, Pembrolizumab, Dabrafenib/Trametinib);
- Therapeutic diversity with the possibility of disease attack, in case of progression under a therapeutic option, in patients with good performance status;
- Increased survival until disease progression, increased overall survival, lasting benefit of the treatment.
- The development of new algorithms in the sequential administration of these therapeutic agents;
- The establishment of the best interval of the disease for the initiation of the specific treatment—adjuvant/“follow-up”;
- The multidisciplinary approach to the disease—in establishing the sequence of the specific oncological treatments—surgery, systemic treatment, radiotherapy;
- The selection of patients for whom certain treatments bring maximum benefit;
- The early and correct diagnosis and the control of the adverse reactions of the new therapies by the multidisciplinary team.
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Borik-Heil, L.; Endler, G.; Parson, W.; Zuckermann, A.; Schnaller, L.; Uyanik-Ünal, K.; Jaksch, P.; Böhmig, G.; Cejka, D.; Staufer, K.; et al. Cumulative UV Exposure or a Modified SCINEXA™-Skin Aging Score Do Not Play a Substantial Role in Predicting the Risk of Developing Keratinocyte Cancers after Solid Organ Transplantation—A Case Control Study. Cancers 2023, 15, 864. [Google Scholar] [CrossRef] [PubMed]
- Juszko-Piekut, M.; Mozdzierz, A.; Koosza, Z.; Krolikowska-Jeruzalska, M.; Wawro-Bielecka, P.; Kowalska-Ziomek, G.; Olczyk, D.; Stojko, J. Incidence of melanoma and non-melanoma skin cancer in the inhabitants of the Upper Silesia, Poland. In Highlights in Skin Cancer; Vereecken, P., Ed.; IntechOpen: London, UK, 2013; Available online: https://www.intechopen.com/chapters/43189 (accessed on 15 January 2023).
- Memon, A.; Bannister, P.; Rogers, I.; Sundin, J.; Al-Ayadhy, B.; James, P.; Mcnally, R. Changing epidemiology and age-specific incidence of cutaneous malignant melanoma in England: An analysis of the national cancer registration data by age, gender and anatomical site, 1981–2018. Lancet Reg. Health Eur. 2021, 2, 100024. [Google Scholar] [CrossRef] [PubMed]
- Islami, F.; Ward, E.M.; Sung, H.; Cronin, K.A.; Tangka, F.K.L.; Sherman, R.L.; Zhao, J.; Anderson, R.N.; Henley, S.J.; Yabroff, K.R.; et al. Annual Report to the Nation on the Status of Cancer, Part 1: National Cancer Statistics. J. Natl. Cancer Inst. 2021, 113, 1648–1669. [Google Scholar] [CrossRef] [PubMed]
- Morton, D.L.; Essner, R.; Kirkwood, J.M.; Wollman, R.C. History of melanoma. In Holland-Frei Cancer Medicine, 6th ed.; BC Decker: Hamilton, ON, USA, 2003. Available online: https://www.ncbi.nlm.nih.gov/books/NBK13962/ (accessed on 15 March 2023).
- Rebecca, V.W.; Sondak, V.K.; Smalley, K.S. A brief history of melanoma: From mummies to mutations. Melanoma Res. 2012, 22, 114–122. [Google Scholar] [CrossRef] [PubMed]
- Srivastava, N.; McDermott, D. Update on benefit of immunotherapy and targeted therapy in melanoma: The changing landscape. Cancer Manag. Res. 2014, 6, 279–289. [Google Scholar] [CrossRef] [PubMed]
- Skudalski, L.; Waldman, R.; Kerr, P.E.; Grant-Kels, J.M. Melanoma: An update on systemic therapies. J. Am. Acad. Dermatol. 2022, 86, 515–524. [Google Scholar] [CrossRef]
- Monroy-Garcia, A.; de Lourdes Mora-Garcia, M.; Hernandez- Montes, J. Cancer immunology and novel strategies for immunotherapy. In Molecular Oncology: Principles and Recent Advances; Bentham Science Publisher: Sharjah, UAE, 2012; Volume 1, pp. 130–147. ISBN 978-1-60805-016-1. [Google Scholar] [CrossRef]
- Yu, R.; Zhu, B.; Chen, D. Type I interferon-mediated tumor immunity and its role in immunotherapy. Cell. Mol. Life Sci. 2022, 79, 191. [Google Scholar] [CrossRef]
- Tarhini, A.A.; Gogas, H.; Kirkwood, J.M. IFN-α in the treatment of melanoma. J. Immunol. 2012, 189, 3789–3793. [Google Scholar] [CrossRef]
- Buchbinder, E.I.; Desai, A. CTLA-4 and PD-1 Pathways: Similarities, Differences, and Implications of Their Inhibition. Am. J. Clin. Oncol. 2016, 39, 98–106. [Google Scholar] [CrossRef]
- Fellner, C. Ipilimumab (yervoy) prolongs survival in advanced melanoma: Serious side effects and a hefty price tag may limit its use. Pharm. Ther. 2012, 37, 503–530. [Google Scholar]
- Mireștean, C.C.; Iancu, R.I.; Iancu, D.T. Immunotherapy and Radiotherapy as an Antitumoral Long-Range Weapon—A Partnership with Unsolved Challenges: Dose, Fractionation, Volumes, Therapeutic Sequence. Curr. Oncol. 2022, 29, 7388–7395. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, R.J.; Flaherty, K.T. BRAF in Melanoma: Pathogenesis, Diagnosis, Inhibition, and Resistance. J. Skin Cancer 2011, 2011, 423239. [Google Scholar] [CrossRef] [PubMed]
- Eroglu, Z.; Ribas, A. Combination therapy with BRAF and MEK inhibitors for melanoma: Latest evidence and place in therapy. Ther. Adv. Med. Oncol. 2016, 8, 48–56. [Google Scholar] [CrossRef] [PubMed]
- Loras, A.; Gil-Barrachina, M.; Marqués-Torrejón, M.Á.; Perez-Pastor, G.; Martinez-Cadenas, C. UV-Induced Somatic Mutations Driving Clonal Evolution in Healthy Skin, Nevus, and Cutaneous Melanoma. Life 2022, 12, 1339. [Google Scholar] [CrossRef]
- Ronchi, A.; Montella, M.; Zito Marino, F.; Caraglia, M.; Grimaldi, A.; Argenziano, G.; Moscarella, E.; Brancaccio, G.; Troiani, T.; Napolitano, S.; et al. Predictive Evaluation on Cytological Sample of Metastatic Melanoma: The Role of BRAF Immunocytochemistry in the Molecular Era. Diagnostics 2021, 11, 1110. [Google Scholar] [CrossRef]
- Palamaris, K.; Moutafi, M.; Gakiopoulou, H.; Theocharis, S. Histone Deacetylase (HDAC) Inhibitors: A Promising Weapon to Tackle Therapy Resistance in Melanoma. Int. J. Mol. Sci. 2022, 23, 3660. [Google Scholar] [CrossRef]
- Kim, K.B.; Kefford, R.; Pavlick, A.C.; Infante, J.R.; Ribas, A.; Sosman, J.A.; Fecher, L.A.; Millward, M.; McArthur, G.A.; Hwu, P.; et al. Phase II study of the MEK1/MEK2 inhibitor Trametinib in patients with metastatic BRAF-mutant cutaneous melanoma previously treated with or without a BRAF inhibitor. J. Clin. Oncol. 2013, 31, 482–489. [Google Scholar] [CrossRef]
- Crist, J.; Hodge, J.R.; Frick, M.; Leung, F.P.; Hsu, E.; Gi, M.T.; Venkatesh, S.K. Magnetic Resonance Imaging Appearance of Schwannomas from Head to Toe: A Pictorial Review. J. Clin. Imaging Sci. 2017, 7, 38. [Google Scholar] [CrossRef]
- Tamas, T.; Dinu, C.; Lenghel, L.M.; Boțan, E.; Tamas, A.; Stoia, S.; Leucuta, D.C.; Bran, S.; Onisor, F.; Băciuț, G.; et al. High-Frequency Ultrasound in Diagnosis and Treatment of Non-Melanoma Skin Cancer in the Head and Neck Region. Diagnostics 2023, 13, 1002. [Google Scholar] [CrossRef]
- Skolnik, A.D.; Loevner, L.A.; Sampathu, D.M.; Newman, J.G.; Lee, J.Y.; Bagley, L.J.; Learned, K.O. Cranial Nerve Schwannomas: Diagnostic Imaging Approach. Radiographics 2016, 36, 1463–1477. [Google Scholar] [CrossRef]
- Monson, K.; Dewey, B.; Ugorowski, M.; Broski, S. 18F-FDG PET/CT Imaging Features of Benign Schwannomas. J. Nucl. Med. 2019, 60, 2053. [Google Scholar]
- Lommerts, J.E.; Bekkenk, M.W.; Luiten, R.M. Vitiligo induced by immune checkpoint inhibitors in melanoma patients: An expert opinion. Expert Opin. Drug Saf. 2021, 20, 883–888. [Google Scholar] [CrossRef] [PubMed]
- Guida, M.; Strippoli, S.; Maule, M.; Quaglino, P.; Ramondetta, A.; Chiaron Sileni, V.; Antonini Cappellini, G.; Queirolo, P.; Ridolfi, L.; Del Vecchio, M.; et al. Immune checkpoint inhibitor associated vitiligo and its impact on survival in patients with metastatic melanoma: An Italian Melanoma Intergroup study. ESMO Open 2021, 6, 100064. [Google Scholar] [CrossRef] [PubMed]
- Tietze, J.K.; Forschner, A.; Loquai, C.; Mitzel-Rink, H.; Zimmer, L.; Meiss, F.; Rafei-Shamsabadi, D.; Utikal, J.; Bergmann, M.; Meier, F.; et al. The efficacy of re-challenge with BRAF inhibitors after previous progression to BRAF inhibitors in melanoma: A retrospective multicenter study. Oncotarget 2018, 9, 34336–34346. [Google Scholar] [CrossRef] [PubMed]
- Zaremba, A.; Eggermont, A.M.M.; Robert, C.; Dummer, R.; Ugurel, S.; Livingstone, E.; Ascierto, P.A.; Long, G.V.; Schadendorf, D.; Zimmer, L. The concepts of rechallenge and retreatment with immune checkpoint blockade in melanoma patients. Eur. J. Cancer 2021, 155, 268–280. [Google Scholar] [CrossRef] [PubMed]
- Torres-Navarro, I.; de Unamuno-Bustos, B.; Botella-Estrada, R. Systematic review of BRAF/MEK inhibitors-induced Severe Cutaneous Adverse Reactions (SCARs). J. Eur. Acad. Dermatol. Venereol. 2021, 35, 607–614. [Google Scholar] [CrossRef] [PubMed]
- Janavicius, M.; Lachej, N.; Anglickiene, G.; Vincerzevskiene, I.; Brasiuniene, B. Outcomes of Treatment for Melanoma Brain Metastases. J. Skin Cancer 2020, 2020, 7520924. [Google Scholar] [CrossRef]
- Costa Svedman, F.; Das, I.; Tuominen, R.; Darai Ramqvist, E.; Höiom, V.; Egyhazi Brage, S. Proliferation and Immune Response Gene Signatures Associated with Clinical Outcome to Immunotherapy and Targeted Therapy in Metastatic Cutaneous Malignant Melanoma. Cancers 2022, 14, 3587. [Google Scholar] [CrossRef]
- Tawbi, H.A.; Boutros, C.; Kok, D.; Robert, C.; McArthur, G. New Era in the Management of Melanoma Brain Metastases. Am. Soc. Clin. Oncol. Educ. Book 2018, 38, 741–750. [Google Scholar] [CrossRef]
- Fetcko, K.; Lukas, R.V.; Watson, G.A.; Zhang, L.; Dey, M. Survival and complications of stereotactic radiosurgery: A systematic review of stereotactic radiosurgery for newly diagnosed and recurrent high-grade gliomas. Medicine 2017, 96, e8293. [Google Scholar] [CrossRef]
- Goldinger, S.M.; Buder-Bakhaya, K.; Lo, S.N.; Forschner, A.; McKean, M.; Zimmer, L.; Khoo, C.; Dummer, R.; Eroglu, Z.; Buchbinder, E.I.; et al. Chemotherapy after immune checkpoint inhibitor failure in metastatic melanoma: A retrospective multicentre analysis. Eur. J. Cancer 2022, 162, 22–33. [Google Scholar] [CrossRef] [PubMed]
- Tone, M.; Izumo, T.; Awano, N.; Kuse, N.; Inomata, M.; Jo, T.; Yoshimura, H.; Miyamoto, S.; Kunitoh, H. Treatment effect and safety profile of salvage chemotherapy following immune checkpoint inhibitors in lung cancer. Lung. Cancer Manag. 2019, 4, LMT12. [Google Scholar] [CrossRef] [PubMed]
- Heinhuis, K.M.; Ros, W.; Kok, M.; Steeghs, N.; Beijnen, J.H.; Schellens, J.H.M. Enhancing antitumor response by combining immune checkpoint inhibitors with chemotherapy in solid tumors. Ann. Oncol. 2019, 30, 219–235. [Google Scholar] [CrossRef] [PubMed]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stoian, A.-R.; Rahnea-Nita, G.; Ciuhu, A.-N.; Gales, L.; Anghel, R.-M.; Rebegea, L.-F.; Rahnea-Nita, R.-A.; Andronache, L.-F.; Soare, I.; Stoleriu, G. The Benefits and Challenges of the Multimodal Treatment in Advanced/Metastatic Malignant Melanoma. Diagnostics 2023, 13, 1635. https://doi.org/10.3390/diagnostics13091635
Stoian A-R, Rahnea-Nita G, Ciuhu A-N, Gales L, Anghel R-M, Rebegea L-F, Rahnea-Nita R-A, Andronache L-F, Soare I, Stoleriu G. The Benefits and Challenges of the Multimodal Treatment in Advanced/Metastatic Malignant Melanoma. Diagnostics. 2023; 13(9):1635. https://doi.org/10.3390/diagnostics13091635
Chicago/Turabian StyleStoian, Alexandru-Rares, Gabriela Rahnea-Nita, Anda-Natalia Ciuhu, Laurentia Gales, Rodica-Maricela Anghel, Laura-Florentina Rebegea, Roxana-Andreea Rahnea-Nita, Liliana-Florina Andronache, Ioana Soare, and Gabriela Stoleriu. 2023. "The Benefits and Challenges of the Multimodal Treatment in Advanced/Metastatic Malignant Melanoma" Diagnostics 13, no. 9: 1635. https://doi.org/10.3390/diagnostics13091635