1. Introduction
Cancer starts when healthy cells in the breast change and grow out of control, forming a mass or sheet of cells called a tumor. A tumor may be benign or cancerous. Malignant means a cancerous tumor can grow and spread to other body parts. If a tumor is benign, it can enlarge but not spread. Radiologists must use a computer-aided detection (CAD) system to differentiate between normal and cancerous cell growth [
1]. Arthritis is a form of joint inflammation that causes pain, stiffness, swelling, and limited movement. In India, 15% of the adult population had arthritis in 2015, compared with 22.7% in the United States [
2]. According to medical research, there are around 100 different types of arthritis, with rheumatoid arthritis (RA) and osteoarthritis (OA) being the most frequent [
3]. Medical imaging is a growing field and has several tools and methods for getting information from medical images. Magnetic resonance imaging (MRI) is one of the most extensively employed imaging techniques. MRI image samples are obtained using Brainix and neuroimaging data sources [
4].
Up to 17% of people worldwide have progressive RA, an inflammatory condition. Most of the time, the condition causes inflammation in the joints, which makes them hurt for life, shortens people’s lives, and makes life less enjoyable. Some of the first signs of arthritis are narrowing joint space, breaking cartilage, less synovial fluid, and a torn meniscus. In both men and women, although more typically in middle-aged women, it can also affect organs and systems such as the skin, heart, and lungs [
5]. RA is a long-lasting inflammatory disease that painfully destroys joints. Still, measuring how well a therapy works greatly depends on how the patient and the clinician feel about it. Aggressive disease-modifying therapy can alleviate symptoms and avoid irreversible joint deterioration [
6]. Patients with RA who are getting good medical care may still develop musculoskeletal problems, such as damage to the knee joints that cannot be fixed. Total knee arthroplasty (TKA) surgeries on RA patients may become more common and have more complications as patients age. Pathogenesis, prognosis, and medical treatment for RA of the knee differ from those for OA of the knee, so the expected results of TKA are also different. The advanced knee damage RA causes is not a local problem, but a sign of a systemic problem. These variables influence the outcomes of TKA [
7]. Research into the ways that artificial intelligence (AI), especially machine learning (ML) and deep learning (DL) techniques, could be used in medicine and healthcare is growing quickly. When there is not a good treatment for people with chronic rheumatological disorders such as RA, the second most common autoimmunity, these strategies can be very important for giving good care [
8]. RA, an autoimmune disorder, affects between 0.5 and 1 percent of adults globally. The condition is most prevalent between the ages of 50 and 60, and women are twice as likely as men to develop it. Despite the lack of knowledge of what brings on rheumatoid arthritis, the consequences of this condition can be quite severe [
9].
In 2010, the European League Against Rheumatism (EULAR) made its first suggestions about how to treat RA with biological and synthetic disease-modifying antirheumatic drugs (DMARDs). They gave rheumatologists, patients, payers, and other interested parties a summary of what is known now and what European specialists think based on evidence. Targeted synthetic and biologic DMARDs have transformed the treatment of this disorder. However, there are concerns about applying these novel ideas to clinical practice [
10]. People with RA can now stop irreversible joint damage and, in some cases, heal damaged joints with the help of new drugs, biologics, and intensive treatment plans. Radiographs may reveal subchondral bone sclerosis and osteophyte formation as injured joints heal. The “evaluation of RA by scoring big joint destruction and healing in radiographic imaging” (ARASHI score) says that these changes, called secondary osteoarthritis (OA), are signs of rheumatoid arthritis. Radiographs include them in the definition of structural remodeling of large joints and recommend them as a way to make large joints more stable [
11]. Scientists have used the term “human activity recognition” (HAR) to describe how machines automatically analyze what people do. Healthcare professionals rely heavily on this to promote health and wellness. For example, aged monitoring, exercise supervision, and rehabilitation monitoring all use it. Human activity recognition (HAR) can be used to track and analyze the activity levels of the elderly so that we can detect health issues prematurely [
12]. This semi-supervised hierarchical convolutional neural network (SS-HCNN) aims to get around how hard it is to put images into categories and how the annotations limit what can be done. The concept is to use unsupervised clustering of the low-level characteristics to divide images into a tree-like structure and then train a tree-like network of convolutional neural networks (CNNs) at the root and parent nodes using the generated cluster labels [
13]. This study proposes a probability-based real-parameter encoding operator. The approach also reduces the chromosomal length, saving computation space. The proposed revised GA algorithm passed the two-step validation process. First, a typical DFJSP demonstrated the algorithm’s utility. Second, the algorithm solved a real-world problem. A Taiwanese fastener factory applied historical data to 100 and 200 work orders. The proposed GA method change solved GA encoding problems. They completed the 100 sets of work orders in 102 days and 39 min using the proposed GA, saving 3878 min (150,797 min – 146,919 min = 3878 min) [
14]. The author used the 3D articular bone shapes of the hand joints of people with RA and psoriatic arthritis and healthy controls to train a new neural network.
High-resolution peripheral computed tomography (HR-pQCT) data from the head of the second metacarpal bone were used to make the bone. Using GradCAM, it generated heat maps of problem areas. After training, we gave the neural network patterns of arthritis that could not be categorized as RA, PsA, or HC to figure out what kind of arthritis they were. In 932 HR-pQCT images of 617 patients, hand bone shapes were obtained. The network discriminated HC, RA, and PsA with area-under-receiver-operator curves of 82%, 75%, and 68%, respectively. Heat maps showed bare spots and places where ligaments connect that are likely to erode and form bone spurs. Based on joint form, the neural network identified 86% of UA data as “RA,” 11% as “PsA,” and 3% as “HC” [
15]. The author came up with a new, simple, and computer-generated method for diagnosing knee RA that is based on deep CNNs and automatically measures the severity of RA in knee joints. This network was trained using around 1650 digital X-radiation images of the knee joint from the Optical Knee X-radiation Images Mendeley Collection. We performed the validation procedure for 20% of the data [
16].
The proposed method was based on spatial analysis, and they separated the edges of the skin using a method based on intensity. The thresholding algorithm for segmenting bone regions, the hit-or-miss transformation for segmenting bone lines, and a distance measure for detecting the joint region following localization was followed. The synovial region was then identified using the active contour technique. In arthritic situations, synovitis also develops. We divided this condition into four types based on how much fluid builds up in the synovial area. The various grades were defined and analyzed using deep learning. A deep learning system used a convolutional neural network to determine the exact grade of synovitis and the type of arthritis. The validation produced an average true-positive percentage of 88.52%, ranging from 78.12% to 98.95%. False positives fell by 1.41 percent. These findings demonstrate that the network efficiently differentiates synovial grades [
17]. In a big data set, the machine-learning-based ensemble analytical approach (MLEAA) has two parts: learning and predicting. During the learning phase, Hadoop’s map-reduce technology processes the data, while the highlighted attributes move the prediction stage forward. Three different algorithms, including Ababoost, SVM, and ANN, were used in the proposed MLEAA approach’s prediction phase, and the final predictive value was computed based on the voting system [
18]. There are ways to conduct traditional statistical modeling, but they limit these methods in how much data they can effectively analyze. It is necessary to create thorough, patient-specific prediction models. Techniques such as data mining and machine learning should be used to help make these kinds of models. Although it will be difficult, current technology should allow for the sub-grouping of patients with OA, which could improve clinical judgment and advance precision medicine [
19]. Early knee osteoarthritis detection is presented. Deep-learning-based feature descriptors on X-radiation pictures perform this. Training and testing use the Mendeley Dataset VI. Deep learning-based feature descriptors on X-radiation pictures perform this CNN with LBP and HOG used joint space width to obtain the proposed model feature from the region of interest. KOA was classified using KL, SVM, RF, and KNN. Images were five-fold validated and cross-validated. The method achieved 97.14% cross-validation and 98% five-fold validation accuracy. In the future, it will be possible to combine the proposed method with other models to find diseases above and below the knee more complexly. Feature fusion can detect and classify different diseases [
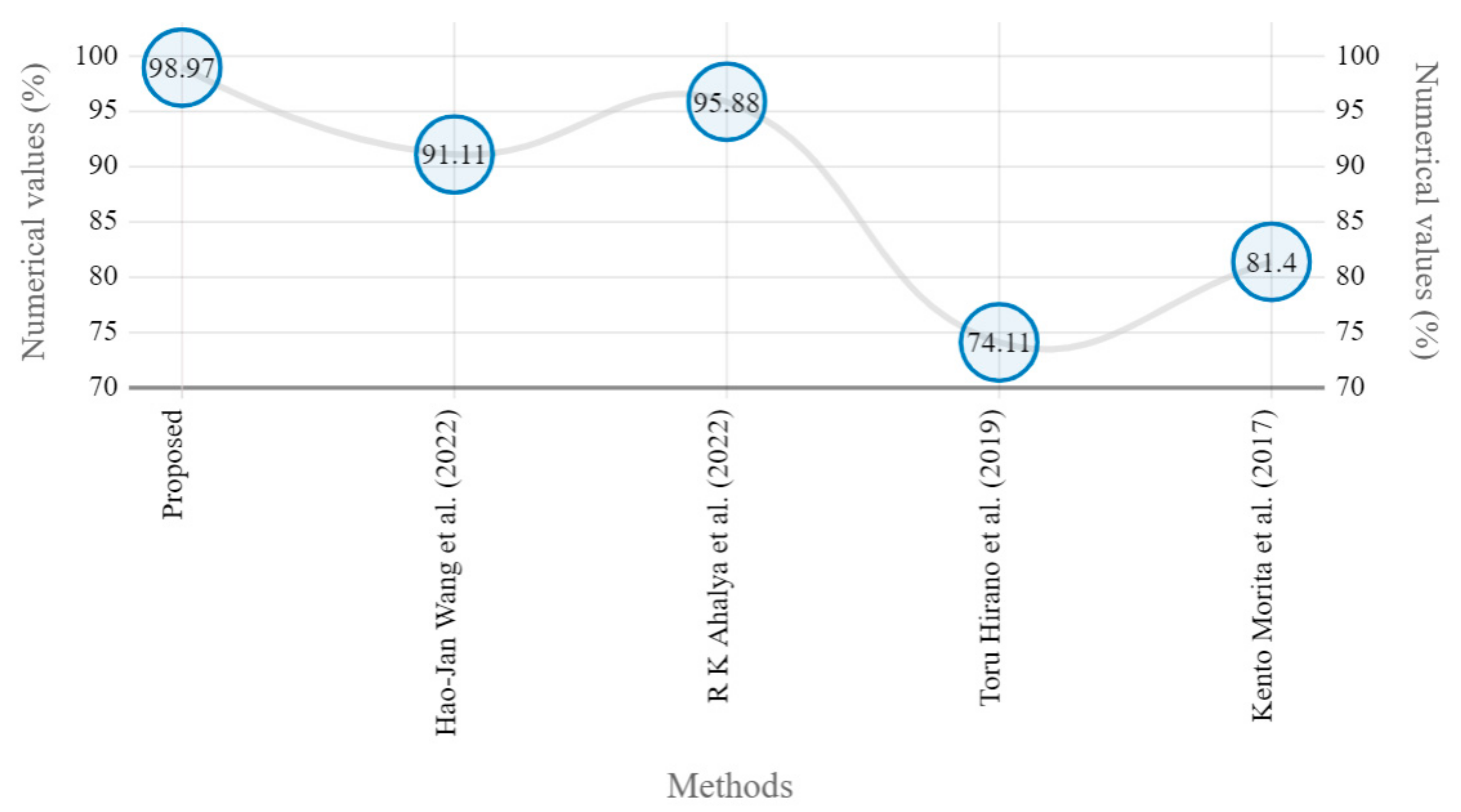
20]. The model contained both a joint-detection step and a joint-evaluation step. There were 216 radiographs taken from 108 RA patients, with 186 assigned to the training/validation dataset and 30 to the test dataset. In the training/validation dataset, pictures of the PIP joints, the thumb’s IP joint, and the MCP joints were manually cropped, evaluated by clinicians for joint space narrowing (JSN), and then augmented. To train and test a deep convolutional neural network for joint evaluation, 11,160 images were used. The joint detection machine learning system was trained using 3720 carefully selected images. Putting these two methods together made a model for figuring out how badly radiographic finger joints damage it. With a sensitivity of 95.3%, the model estimated JSN and erosion for the PIP, thumb IP, and MCP joints. JSN’s accuracy range was 49.6–65.4 percent, while its erosion range was 70–74.1 percent. The correlation between model and clinician scores per image was 0.72 to 0.88 for JSN and 0.54 to 0.56 for erosion [
21].
The proposed system architecture was made up of a CNN layer and a multilayer-based metadata learning layer. This was conducted so that the information was reliable. Sparse coding estimates and metadata-based vector encoding were used for the additional dimension. To keep the geometric format of supervised data [
22], a well-structured k-neighbored network was used to build nearby limitation atoms. This study proposes SVM-based detection of finger joints and mTS score estimation. Using X-radiations of 45 RA patients, the suggested approach recognized finger joints with 81.4% accuracy and evaluated erosion and the JSN score with 50.9% and 64.4% accuracy, respectively [
23]. The proposed model scored JSN and erosion for PIP, thumb IP, and MCP joints with 95.3% sensitivity. JSN had an accuracy range of 49.6–65.4% and an erosion range of 70–74.1%. They correlated the model and clinician scores per image at 0.72–0.88 for JSN and 0.54–0.75 for erosion [
24]. The accuracy of the modified pre-trained GoogleNet model was 89%, whereas that of the proposed custom model was 95%. Google Net had a sensitivity of 84% and a specificity of 90%. Model number three was 95% sensitive and 94% specific. When extracted features from customized models (SIFT + CNN) are compared with those from ML classifiers, the custom3 model performed better [
25]. The suggested method was compared with other fuzzy clustering methods that are already used to show how well it works. We compared the support vector machine (SVM), Decision Tree (DT), rough set data analysis (RSDA), and fuzzy-SVM classification algorithms to find the best way to group things [
26]. The authors aim to create an AI-based computer-aided diagnosis tool that can classify abnormalities by reading chest X-radiations and help doctors make an accurate diagnosis quickly. We used a Google-created convolutional neural network (CNN) called XceptionNet to find those pathologies in the ChestX-radiation-14 data. Additionally, the same data are being used to run other CNN-ResNet algorithms [
27]. At the 100th training iteration, the mean square error and the false recognition rate dropped below 1.1%, suggesting that the LPRNN was trained correctly. Edge preservation index values were above the experimental threshold of 0.48, signal-to-noise ratios (SNRs) were greater than 65 dB, peak SNR ratios were greater than 70 dB, and destruction times were faster [
28]. Principal Component Analysis improved characteristics, while the Co-Active Adaptive Neuro-Fuzzy Expert System sorted images of the brain into glioma or non-glioma groups. The PCA and CANFES classification techniques had a sensitivity (Se) of 97.6%, a specificity of 98.56%, an accuracy of 98.73%, a precision of 98.85%, a false positive rate of 98.11%, and a false negative rate of 98.185 [
29].
Table 1 illustrates the various state-of-the-art methods for knee RA classification.
1.1. Contribution
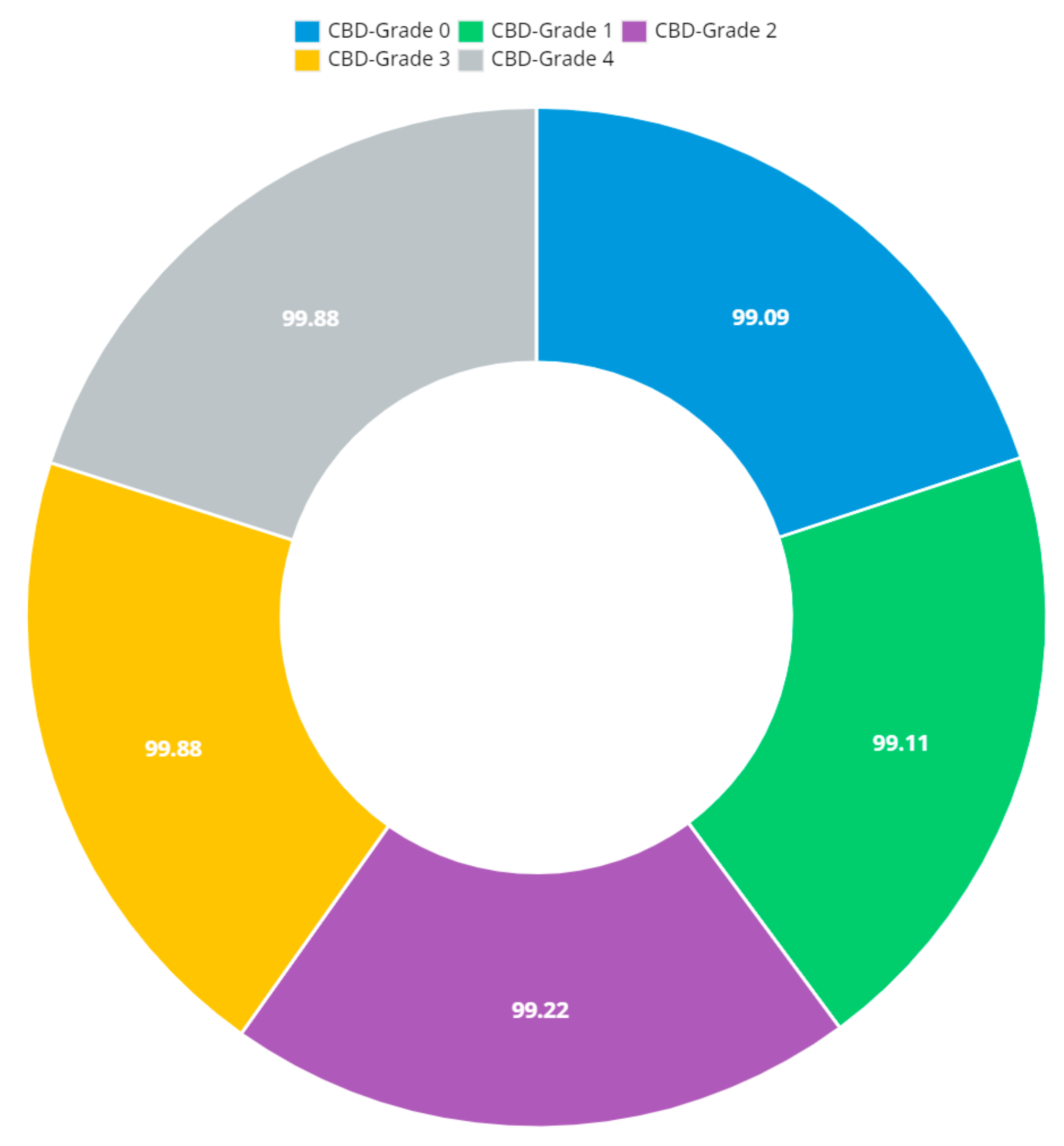
The proposed system predicts the minimal joint space narrow region and knee RA severity grade value.
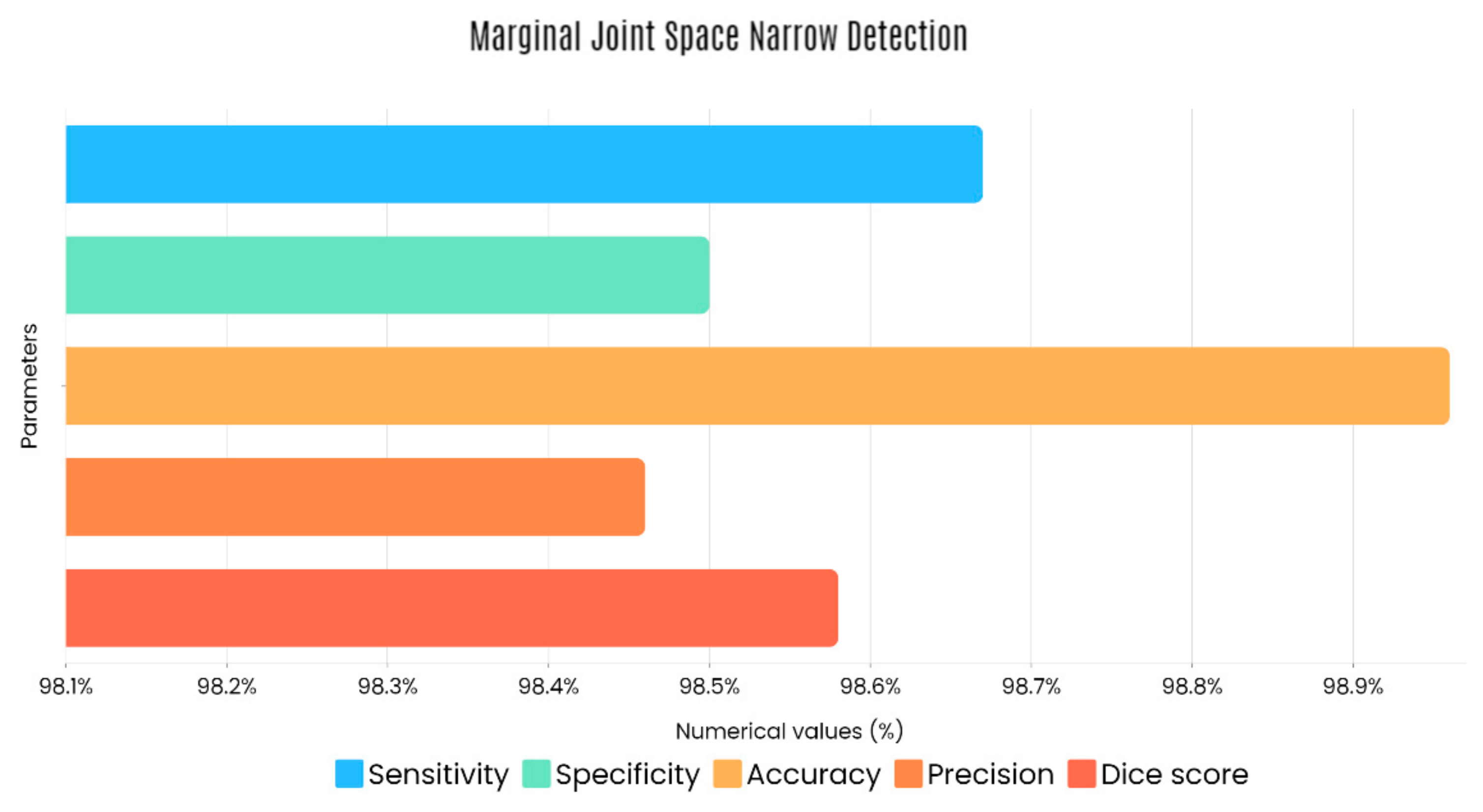
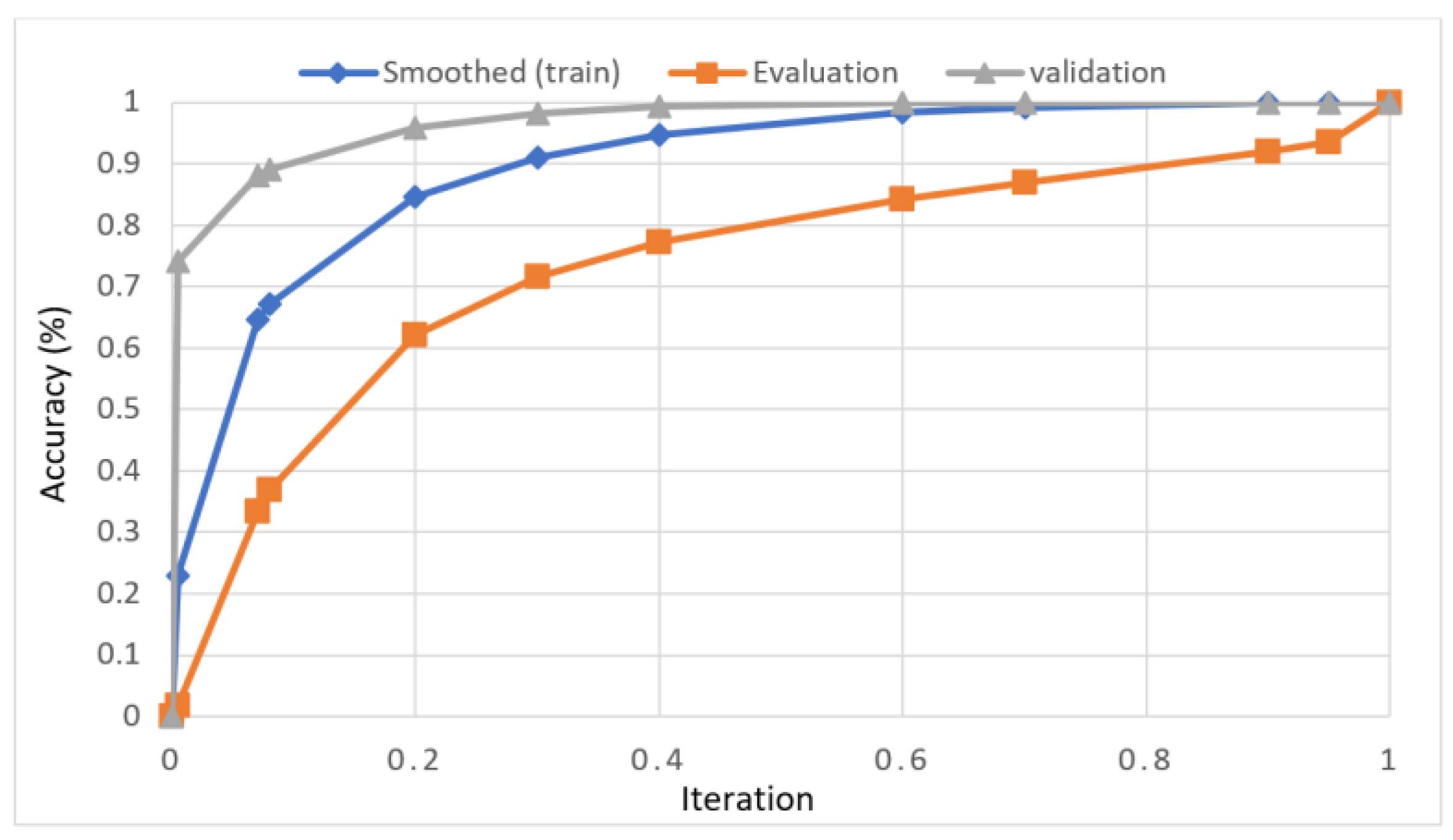
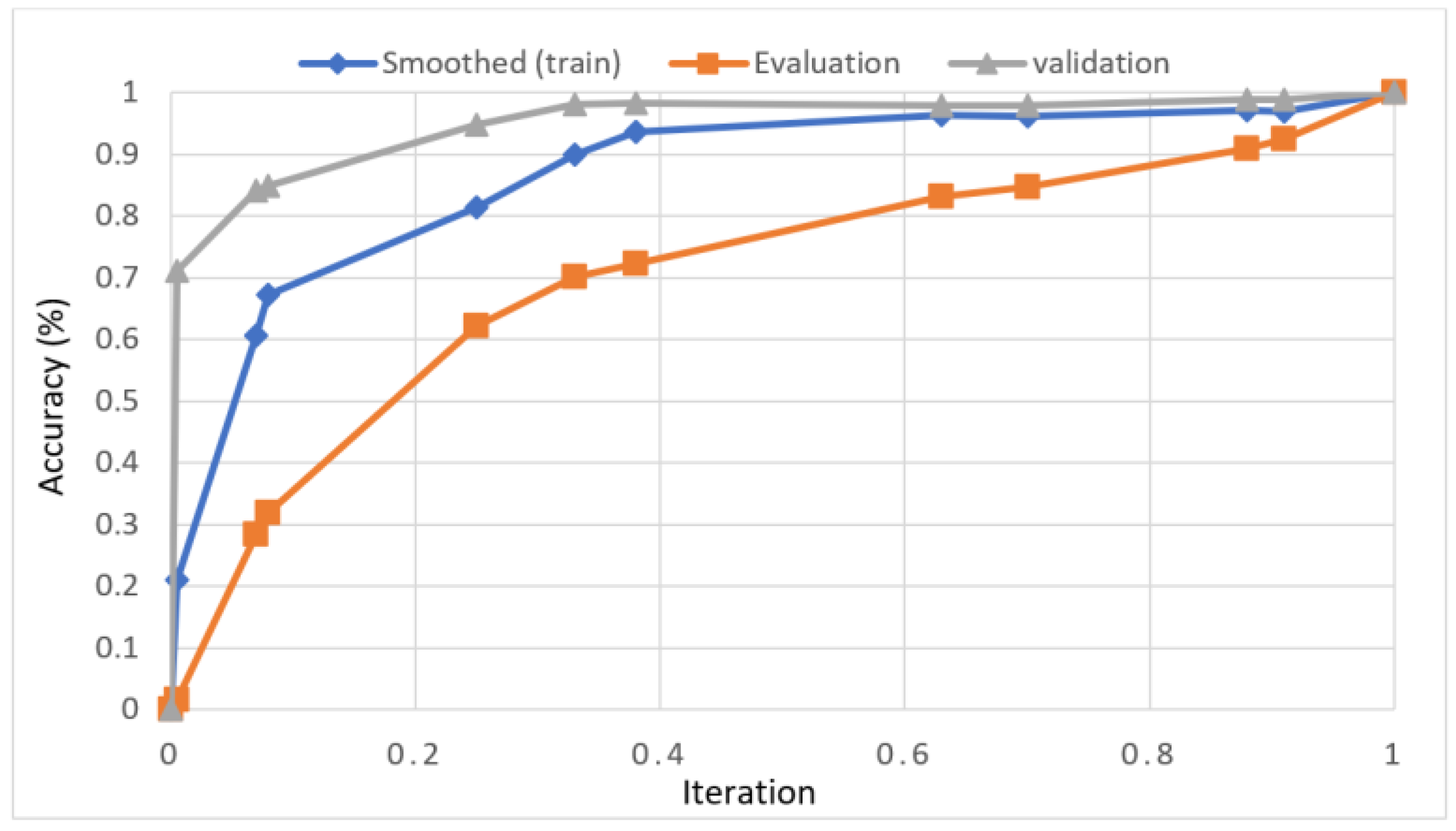
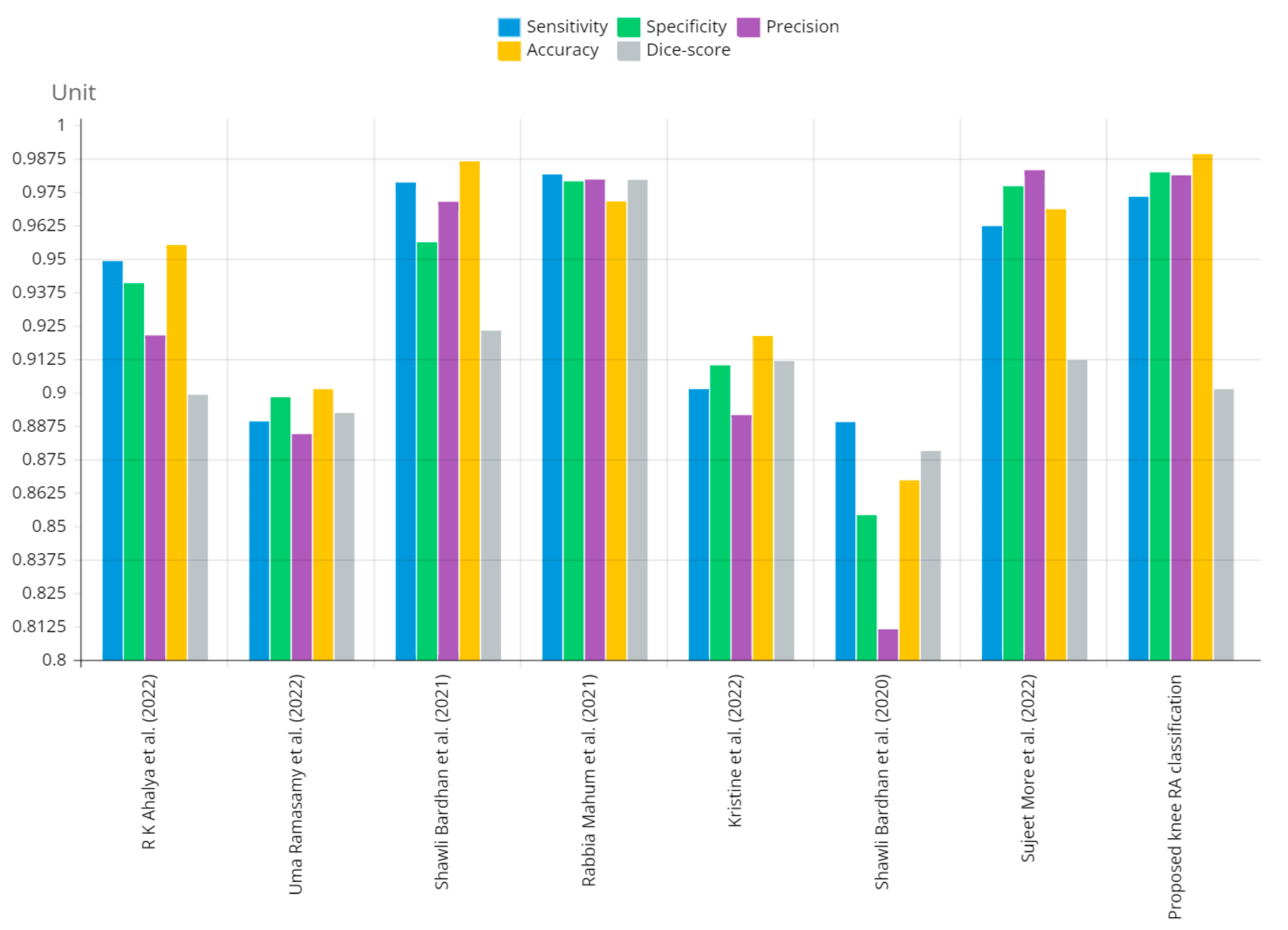
The proposed system’s experimental analysis was carried out using various criteria. The RA severity classification parameters such as sensitivity, specificity, accuracy, precision, and dice score.
Our proposed system classification paradigm outcomes perform better than traditional techniques.
1.2. Organization of Work
Section 1: this paper also discusses the techniques for dataset validation and inflammatory mediator ground truth production and discusses the different state-of-the-art method performances.
Section 2: following the data collection step, pre-processing and segmentation of the thermograms take place.
Section 3: in the last step, the algorithm differentiates between abnormal and normal knee thermograms and then divides aberrant knee thermograms into three distinct categories.
Section 4: provides the RA classification results from various parameters and compares the results of various existing techniques.

 ,
, 













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}