
Valid and Reproducible Quantitative Assessment of Cardiac Volumes by Echocardiography in Patients with Valvular Heart Diseases—Possible or Wishful Thinking?


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Questions and Potential Consequences Arising from These Volume Differences between Echocardiography and CMR
- ○
- Do these methodological discrepancies between both imaging modalities really exist?
- ○
- If LV volumes determined by echocardiography and CMR under comparable circulatory conditions are not similar, how can the problem of underestimation of cardiac volumes by echocardiography or overestimation by CMR be explained?
- ○
- In addition, if echocardiography is always reputed to measure smaller LV volumes than CMR, how can the data of some previous trials [25], in which comparable or bigger LV volume values have been determined by echocardiography, be explained?
- ○
- In contrast, if LV volumes determined by echocardiography and CMR under circulatory comparable conditions are similar, are physiological aspects during image acquisition the reason for potential irrelevant differences?
- ○
- If the assessment of comparable cardiac volumes is possible, does the underestimation of cardiac volumes by echocardiography then constitute a methodological failure?
- ○
- Assuming that cardiac volumes are underestimated by echocardiography in the past, what are the clinical implications?
- (1)
- both modalities measure the same target values if both methods are used properly;
- (2)
- echocardiography generally underestimates cardiac volumes implying that cardiac volumes generally cannot be properly assessed by echocardiography.
3. Phantom Studies: The True Volumes and the Volumes Determined by Echocardiography Are Comparable
4. Clinical Studies: Different Imaging Modalities Result in Different Cardiac Volumes—Most Notably an Underestimation by Echocardiography Compared with CMR
5. Normal Values of Cardiac Volumes in Echocardiographic Recommendations
6. Implications Derived from the Current Underestimation of Cardiac Volumes by Echocardiography in Patients with Valvular Heart Diseases
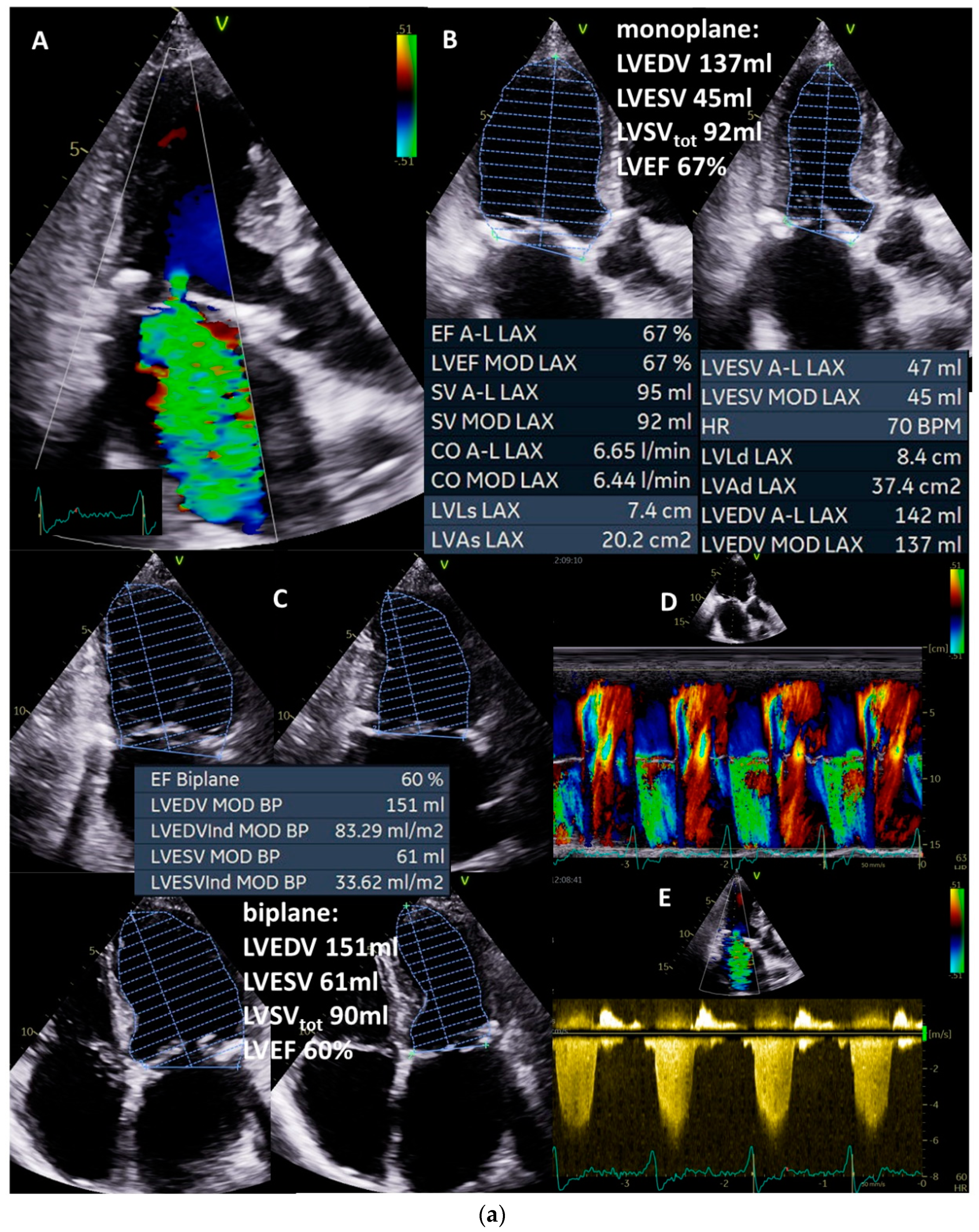
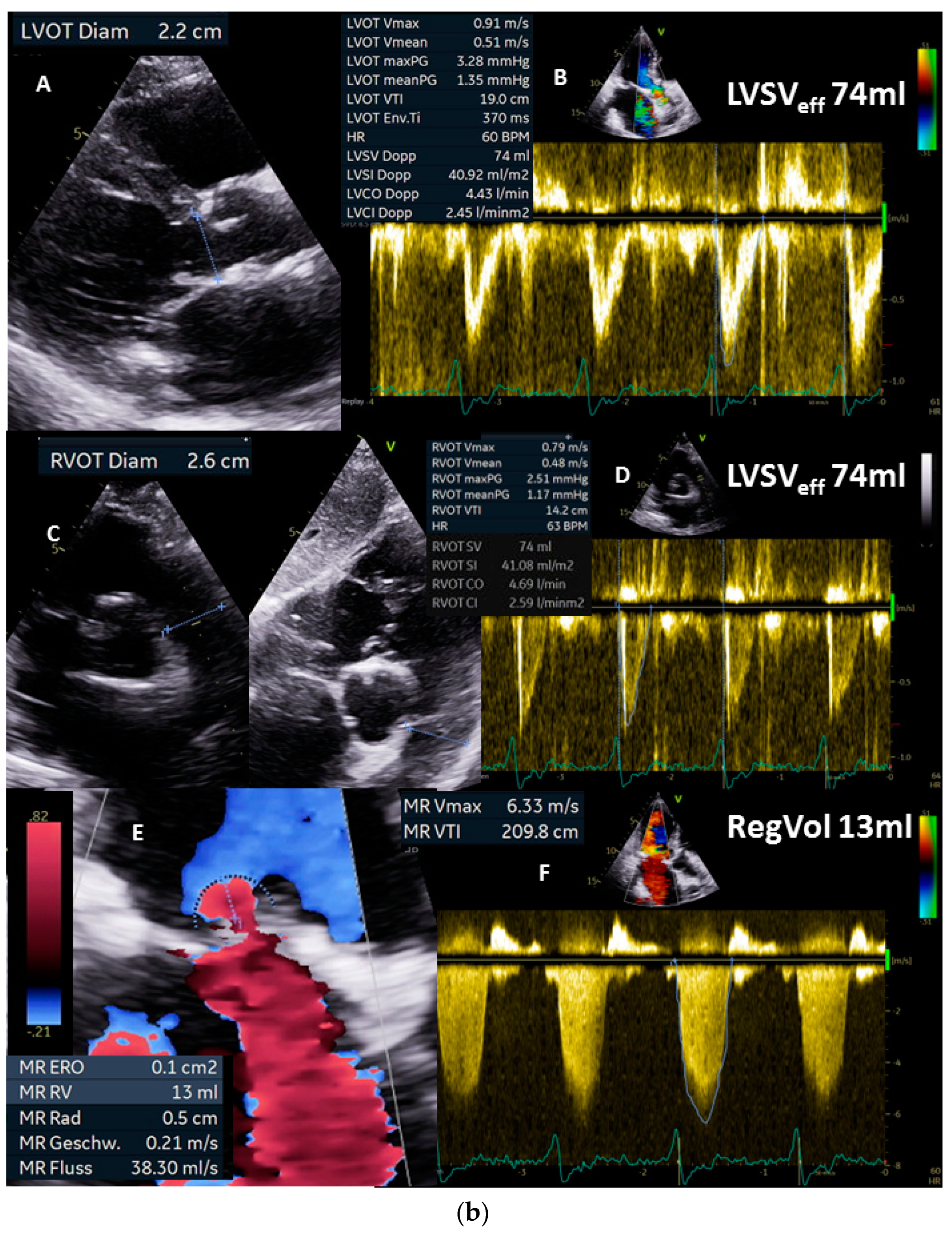
7. How to Plausibly Analyze the Severity of Mitral Regurgitation—A Case Report (Figure 4)


8. Future Implications
- (1)
- The actual, integrative approach is too error prone to be continued in this form. It should be replaced or supplemented by a definitive quantitative approach comparable to CMR.
- (2)
- Valid quantitative assessment by echocardiography is feasible once echocardiography and data analysis are performed with methodological and technical considerations in mind.
- (3)
- Unfortunately, implementation of this approach cannot generally be considered for real-world conditions.
- (4)
- Cardiac volumes, particularly total and effective LVSV and RegVol, should be checked for plausibility and valid hemodynamics.
- (5)
- Apparently, incorrect former echocardiographic data of cardiac volume measurements should not be considered in future meta-analyses.
- (6)
- New studies about normal ranges of cardiac volumes measured by echocardiography and validated by CMR are necessary.
- (7)
- The echocardiographic algorithm for analysis of VHD, particularly valvular regurgitations, should be revised to include hemodynamically valid CO and CI.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Vahanian, A.; Beyersdorf, F.; Praz, F.; Milojevic, M.; Baldus, S.; Bauersachs, J.; Capodanno, D.; Conradi, L.; De Bonis, M.; De Paulis, R.; et al. 2021 ESC/EACTS Guidelines for the Management of Valvular Heart Disease: Developed by the Task Force for the Management of Valvular Heart Disease of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS). Rev. Española Cardiol. (Engl. Ed.) 2022, 75, 524. [Google Scholar] [CrossRef] [PubMed]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef] [PubMed]
- Lancellotti, P.; Tribouilloy, C.; Hagendorff, A.; Popescu, B.A.; Edvardsen, T.; Pierard, L.A.; Badano, L.; Zamorano, J.L.; On behalf of the Scientific Document Committee of the European Association of Cardiovascular Imaging. Recommendations for the Echocardiographic Assessment of Native Valvular Regurgitation: An Executive Summary from the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2013, 14, 611–644. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for Cardiac Chamber Quantification by Echocardiography in Adults: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 233–271. [Google Scholar] [CrossRef] [PubMed]
- Zoghbi, W.A.; Adams, D.; Bonow, R.O.; Enriquez-Sarano, M.; Foster, E.; Grayburn, P.A.; Hahn, R.T.; Han, Y.; Hung, J.; Lang, R.M.; et al. Recommendations for Noninvasive Evaluation of Native Valvular Regurgitation. J. Am. Soc. Echocardiogr. 2017, 30, 303–371. [Google Scholar] [CrossRef]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the Management of Arterial Hypertension. Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef] [Green Version]
- Teichholz, L.E.; Kreulen, T.; Herman, M.V.; Gorlin, R. Problems in Echocardiographic Volume Determinations: Echocardiographic-Angiographic Correlations in the Presence or Absence of Asynergy. Am. J. Cardiol. 1976, 37, 7–11. [Google Scholar] [CrossRef]
- Quinones, M.A.; Waggoner, A.D.; Reduto, L.A.; Nelson, J.G.; Young, J.B.; Winters, W.L.; Ribeiro, L.G.; Miller, R.R. A New, Simplified and Accurate Method for Determining Ejection Fraction with Two-Dimensional Echocardiography. Circulation 1981, 64, 744–753. [Google Scholar] [CrossRef] [Green Version]
- De Castro, S.; Caselli, S.; Maron, M.; Pelliccia, A.; Cavarretta, E.; Maddukuri, P.; Cartoni, D.; Di Angelantonio, E.; Kuvin, J.T.; Patel, A.R.; et al. Left Ventricular Remodelling Index (LVRI) in Various Pathophysiological Conditions: A Real-Time Three-Dimensional Echocardiographic Study. Heart 2005, 93, 205–209. [Google Scholar] [CrossRef]
- Ostenfel, E.; Flachskampf, F.A. Assessment of Right Ventricular Volumes and Ejection Fraction by Echocardiography: From Geometric Approximations to Realistic Shapes. Echo Res. Pract. 2015, 2, R1–R11. [Google Scholar] [CrossRef] [Green Version]
- Rudski, L.G.; Lai, W.W.; Afilalo, J.; Hua, L.; Handschumacher, M.D.; Chandrasekaran, K.; Solomon, S.D.; Louie, E.K.; Schiller, N.B. Guidelines for the Echocardiographic Assessment of the Right Heart in Adults: A Report from the American Society of Echocardiography. J. Am. Soc. Echocardiogr. 2010, 23, 685–713. [Google Scholar] [CrossRef]
- Milan, A.; Magnino, C.; Veglio, F. Echocardiographic Indexes for the Non-Invasive Evaluation of Pulmonary Hemodynamics. J. Am. Soc. Echocardiogr. 2010, 23, 225–239. [Google Scholar] [CrossRef] [PubMed]
- Hagendorff, A.; Knebel, F.; Helfen, A.; Stöbe, S.; Haghi, D.; Ruf, T.; Lavall, D.; Knierim, J.; Altiok, E.; Brandt, R.; et al. Echocardiographic Assessment of Mitral Regurgitation: Discussion of Practical and Methodologic Aspects of Severity Quantification to Improve Diagnostic Conclusiveness. Clin. Res. Cardiol. 2021, 110, 1704–1733. [Google Scholar] [CrossRef] [PubMed]
- Mor-Avi, V.; Sugeng, L.; Weinert, L.; MacEneaney, P.; Caiani, E.G.; Koch, R.; Salgo, I.S.; Lang, R.M. Fast Measurement of Left Ventricular Mass with Real-Time Three-Dimensional Echocardiography: Comparison with Magnetic Resonance Imaging. Circulation 2004, 110, 1814–1818. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pouleur, A.-C.; le Polain de Waroux, J.-B.; Pasquet, A.; Gerber, B.L.; Gerard, O.; Allain, P.; Vanoverschelde, J.-L.J. Assessment of Left Ventricular Mass and Volumes by Three-Dimensional Echocardiography in Patients with or without Wall Motion Abnormalities: Comparison against Cine Magnetic Resonance Imaging. Heart 2008, 94, 1050–1057. [Google Scholar] [CrossRef] [Green Version]
- Shimada, Y.J.; Shiota, T. A Meta-Analysis and Investigation for the Source of Bias of Left Ventricular Volumes and Function by Three-Dimensional Echocardiography in Comparison with Magnetic Resonance Imaging. Am. J. Cardiol. 2011, 107, 126–138. [Google Scholar] [CrossRef]
- Dorosz, J.L.; Lezotte, D.C.; Weitzenkamp, D.A.; Allen, L.A.; Salcedo, E.E. Performance of 3-Dimensional Echocardiography in Measuring Left Ventricular Volumes and Ejection Fraction. J. Am. Coll. Cardiol. 2012, 59, 1799–1808. [Google Scholar] [CrossRef] [Green Version]
- Rigolli, M.; Anandabaskaran, S.; Christiansen, J.P.; Whalley, G.A. Bias Associated with Left Ventricular Quantification by Multimodality Imaging: A Systematic Review and Meta-Analysis. Open Heart 2016, 3, e000388. [Google Scholar] [CrossRef] [Green Version]
- Kitano, T.; Nabeshima, Y.; Otsuji, Y.; Negishi, K.; Takeuchi, M. Accuracy of Left Ventricular Volumes and Ejection Fraction Measurements by Contemporary Three-Dimensional Echocardiography with Semi- and Fully Automated Software: Systematic Review and Meta-Analysis of 1,881 Subjects. J. Am. Soc. Echocardiogr. 2019, 32, 1105–1115.e5. [Google Scholar] [CrossRef]
- Wu, V.C.-C.; Kitano, T.; Chu, P.-H.; Takeuchi, M. Left Ventricular Volume and Ejection Fraction Measurements by Fully Automated 3D Echocardiography Left Chamber Quantification Software versus CMR: A Systematic Review and Meta-Analysis. J. Cardiol. 2023, 81, 19–25. [Google Scholar] [CrossRef]
- Simpson, R.; Bromage, D.; Dancy, L.; McDiarmid, A.; Monaghan, M.; McDonagh, T.; Sado, D. Comparing Echocardiography and Cardiac Magnetic Resonance Measures of Ejection Fraction: Implications for HFMRF Research. In Proceedings of the British Cardiovascular Imaging Meeting 2018, Edinburgh, UK, 2–4 May 2018; p. A3. [Google Scholar]
- Wood, P.W.; Choy, J.B.; Nanda, N.C.; Becher, H. Left Ventricular Ejection Fraction and Volumes: It Depends on the Imaging Method. Echocardiography 2014, 31, 87–100. [Google Scholar] [CrossRef] [Green Version]
- Zhao, L.; Lu, A.; Tian, J.; Huang, J.; Ma, X. Effects of Different LVEF Assessed by Echocardiography and CMR on the Diagnosis and Therapeutic Decisions of Cardiovascular Diseases. Front. Physiol. 2020, 11, 679. [Google Scholar] [CrossRef] [PubMed]
- Klaeboe, L.G.; Edvardsen, T. Echocardiographic Assessment of Left Ventricular Systolic Function. J. Echocardiogr. 2019, 17, 10–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Demir, H.; Tan, Y.Z.; Kozdag, G.; Isgoren, S.; Anik, Y.; Ural, D.; Demirci, A.; Berk, F. Comparison of Gated SPECT, Echocardiography and Cardiac Magnetic Resonance Imaging for the Assessment of Left Ventricular Ejection Fraction and Volumes. Ann. Saudi Med. 2007, 27, 415–420. [Google Scholar] [CrossRef]
- Wolfe, E.R.; Delp, E.J.; Meyer, C.R.; Bookstein, F.L.; Buda, A.J. Accuracy of Automatically Determined Borders in Digital Two-Dimensional Echocardiography Using a Cardiac Phantom. IEEE Trans. Med. Imaging 1987, 6, 292–296. [Google Scholar] [CrossRef] [PubMed]
- Siu, S.C.; Rivera, J.M.; Handschumacher, M.D.; Weyman, A.E.; Levine, R.A.; Picard, M.H. Three-Dimensional Echocardiography: The Influence of Number of Component Images on Accuracy of Left Ventricular Volume Quantitation. J. Am. Soc. Echocardiogr. 1996, 9, 147–155. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, L.D.; Léger, C.; Debrun, D.; Thérain, F.; Visser, J.; Busemann Sokole, E. Validation of a Volumic Reconstruction in 4-d Echocardiography and Gated Spect Using a Dynamic Cardiac Phantom. Ultrasound Med. Biol. 2003, 29, 1151–1160. [Google Scholar] [CrossRef]
- Mårtensson, M.; Winter, R.; Cederlund, K.; Ripsweden, J.; Mir-Akbari, H.; Nowak, J.; Brodin, L.-Å. Assessment of Left Ventricular Volumes Using Simplified 3-D Echocardiography and Computed Tomography—A Phantom and Clinical Study. Cardiovasc. Ultrasound 2008, 6, 26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Dell, W.G. Accuracy of Left Ventricular Cavity Volume and Ejection Fraction for Conventional Estimation Methods and 3D Surface Fitting. JAHA 2019, 8, e009124. [Google Scholar] [CrossRef] [Green Version]
- Mor-Avi, V.; Jenkins, C.; Kühl, H.P.; Nesser, H.-J.; Marwick, T.; Franke, A.; Ebner, C.; Freed, B.H.; Steringer-Mascherbauer, R.; Pollard, H.; et al. Real-Time 3-Dimensional Echocardiographic Quantification of Left Ventricular Volumes. JACC Cardiovasc. Imaging 2008, 1, 413–423. [Google Scholar] [CrossRef] [Green Version]
- Bellenger, N. Comparison of Left Ventricular Ejection Fraction and Volumes in Heart Failure by Echocardiography, Radionuclide Ventriculography and Cardiovascular Magnetic Resonance. Are They Interchangeable? Eur. Heart J. 2000, 21, 1387–1396. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malm, S.; Frigstad, S.; Sagberg, E.; Larsson, H.; Skjaerpe, T. Accurate and Reproducible Measurement of Left Ventricular Volume and Ejection Fraction by Contrast Echocardiography. J. Am. Coll. Cardiol. 2004, 44, 1030–1035. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jenkins, C.; Moir, S.; Chan, J.; Rakhit, D.; Haluska, B.; Marwick, T.H. Left Ventricular Volume Measurement with Echocardiography: A Comparison of Left Ventricular Opacification, Three-Dimensional Echocardiography, or Both with Magnetic Resonance Imaging. Eur. Heart J. 2008, 30, 98–106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greupner, J.; Zimmermann, E.; Grohmann, A.; Dübel, H.-P.; Althoff, T.; Borges, A.C.; Rutsch, W.; Schlattmann, P.; Hamm, B.; Dewey, M. Head-to-Head Comparison of Left Ventricular Function Assessment with 64-Row Computed Tomography, Biplane Left Cineventriculography, and Both 2- and 3-Dimensional Transthoracic Echocardiography. J. Am. Coll. Cardiol. 2012, 59, 1897–1907. [Google Scholar] [CrossRef] [Green Version]
- Hoffmann, R.; Barletta, G.; von Bardeleben, S.; Vanoverschelde, J.L.; Kasprzak, J.; Greis, C.; Becher, H. Analysis of Left Ventricular Volumes and Function: A Multicenter Comparison of Cardiac Magnetic Resonance Imaging, Cine Ventriculography, and Unenhanced and Contrast-Enhanced Two-Dimensional and Three-Dimensional Echocardiography. J. Am. Soc. Echocardiogr. 2014, 27, 292–301. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Lossnitzer, D.; Katus, H.A.; Buss, S.J. Comparison of Left Ventricular Volumes and Ejection Fraction by Monoplane Cineventriculography, Unenhanced Echocardiography and Cardiac Magnetic Resonance Imaging. Int. J. Cardiovasc. Imaging 2012, 28, 1003–1010. [Google Scholar] [CrossRef]
- Ünlü, S.; Duchenne, J.; Mirea, O.; Pagourelias, E.D.; Bézy, S.; Cvijic, M.; Beela, A.S.; Thomas, J.D.; Badano, L.P.; Voigt, J.-U.; et al. Impact of Apical Foreshortening on Deformation Measurements: A Report from the EACVI-ASE Strain Standardization Task Force. Eur. Heart J. Cardiovasc. Imaging 2019, 21, 337–343. [Google Scholar] [CrossRef]
- Jenkins, C.; Bricknell, K.; Chan, J.; Hanekom, L.; Marwick, T.H. Comparison of Two- and Three-Dimensional Echocardiography with Sequential Magnetic Resonance Imaging for Evaluating Left Ventricular Volume and Ejection Fraction over Time in Patients with Healed Myocardial Infarction. Am. J. Cardiol. 2007, 99, 300–306. [Google Scholar] [CrossRef]
- Jenkins, C.; Bricknell, K.; Hanekom, L.; Marwick, T.H. Reproducibility and Accuracy of Echocardiographic Measurements of Left Ventricular Parameters Using Real-Time Three-Dimensional Echocardiography. J. Am. Coll. Cardiol. 2004, 44, 878–886. [Google Scholar] [CrossRef] [Green Version]
- Kühl, H.P.; Schreckenberg, M.; Rulands, D.; Katoh, M.; Schäfer, W.; Schummers, G.; Bücker, A.; Hanrath, P.; Franke, A. High-Resolution Transthoracic Real-Time Three-Dimensional Echocardiography. J. Am. Coll. Cardiol. 2004, 43, 2083–2090. [Google Scholar] [CrossRef] [Green Version]
- Sugeng, L.; Mor-Avi, V.; Weinert, L.; Niel, J.; Ebner, C.; Steringer-Mascherbauer, R.; Schmidt, F.; Galuschky, C.; Schummers, G.; Lang, R.M.; et al. Quantitative Assessment of Left Ventricular Size and Function: Side-by-Side Comparison of Real-Time Three-Dimensional Echocardiography and Computed Tomography with Magnetic Resonance Reference. Circulation 2006, 114, 654–661. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Macron, L.; Lim, P.; Bensaid, A.; Nahum, J.; Dussault, C.; Mitchell-Heggs, L.; Dubois-Randé, J.-L.; Deux, J.-F.; Gueret, P. Single-Beat Versus Multibeat Real-Time 3D Echocardiography for Assessing Left Ventricular Volumes and Ejection Fraction: A Comparison Study with Cardiac Magnetic Resonance. Circ. Cardiovasc. Imaging 2010, 3, 450–455. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shibayama, K.; Watanabe, H.; Iguchi, N.; Sasaki, S.; Mahara, K.; Umemura, J.; Sumiyoshi, T. Evaluation of Automated Measurement of Left Ventricular Volume by Novel Real-Time 3-Dimensional Echocardiographic System: Validation with Cardiac Magnetic Resonance Imaging and 2-Dimensional Echocardiography. J. Cardiol. 2013, 61, 281–288. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Squeri, A.; Censi, S.; Reverberi, C.; Gaibazzi, N.; Baldelli, M.; Binno, S.M.; Properzi, E.; Bosi, S. Three-Dimensional Echocardiography in Various Types of Heart Disease: A Comparison Study of Magnetic Resonance Imaging and 64-Slice Computed Tomography in a Real-World Population. J. Echocardiogr. 2017, 15, 18–26. [Google Scholar] [CrossRef]
- Zhao, D.; Quill, G.M.; Gilbert, K.; Wang, V.Y.; Houle, H.C.; Legget, M.E.; Ruygrok, P.N.; Doughty, R.N.; Pedrosa, J.; D’hooge, J.; et al. Systematic Comparison of Left Ventricular Geometry Between 3D-Echocardiography and Cardiac Magnetic Resonance Imaging. Front. Cardiovasc. Med. 2021, 8, 728205. [Google Scholar] [CrossRef]
- Miller, C.A.; Pearce, K.; Jordan, P.; Argyle, R.; Clark, D.; Stout, M.; Ray, S.G.; Schmitt, M. Comparison of Real-Time Three-Dimensional Echocardiography with Cardiovascular Magnetic Resonance for Left Ventricular Volumetric Assessment in Unselected Patients. Eur. Heart J. Cardiovasc. Imaging 2012, 13, 187–195. [Google Scholar] [CrossRef]
- Moceri, P.; Doyen, D.; Bertora, D.; Cerboni, P.; Ferrari, E.; Gibelin, P. Real Time Three-Dimensional Echocardiographic Assessment of Left Ventricular Function in Heart Failure Patients: Underestimation of Left Ventricular Volume Increases with the Degree of Dilatation: Limits of RT3DE in Heart Failure Patients. Echocardiography 2012, 29, 970–977. [Google Scholar] [CrossRef]
- Stoebe, S.; Metze, M.; Jurisch, D.; Tayal, B.; BoA, K.S.; Laufs, U.; Pfeiffer, D.; Hagendorff, A. Analysis of Chronic Aortic Regurgitation by 2D and 3D Echocardiography and Cardiac MRI. Echo Res. Pract. 2018, 5, 51–62. [Google Scholar] [CrossRef] [Green Version]
- Chukwu, E.O.; Barasch, E.; Mihalatos, D.G.; Katz, A.; Lachmann, J.; Han, J.; Reichek, N.; Gopal, A.S. Relative Importance of Errors in Left Ventricular Quantitation by Two-Dimensional Echocardiography: Insights from Three-Dimensional Echocardiography and Cardiac Magnetic Resonance Imaging. J. Am. Soc. Echocardiogr. 2008, 21, 990–997. [Google Scholar] [CrossRef]
- Castel, A.L.; Toledano, M.; Tribouilloy, C.; Delelis, F.; Mailliet, A.; Marotte, N.; Guerbaai, R.A.; Levy, F.; Graux, P.; Ennezat, P.-V.; et al. Assessment of Left Ventricular Size and Function by 3-Dimensional Transthoracic Echocardiography: Impact of the Echocardiography Platform and Analysis Software. Am. Heart J. 2018, 202, 127–136. [Google Scholar] [CrossRef]
- Muraru, D.; Cecchetto, A.; Cucchini, U.; Zhou, X.; Lang, R.M.; Romeo, G.; Vannan, M.; Mihaila, S.; Miglioranza, M.H.; Iliceto, S.; et al. Intervendor Consistency and Accuracy of Left Ventricular Volume Measurements Using Three-Dimensional Echocardiography. J. Am. Soc. Echocardiogr. 2018, 31, 158–168.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kenny, J.; Plappert, T.; Doubilet, P.; Salzman, D.; Sutton, M.G. Effects of Heart Rate on Ventricular Size, Stroke Volume, and Output in the Normal Human Fetus: A Prospective Doppler Echocardiographic Study. Circulation 1987, 76, 52–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, K.; Monaghan, M.J.; Kenny, A.; Rana, B.; Steeds, R.; Mackay, C.; va der Westhuizen, D. 3D Echocardiography: Benefits and Steps to Wider Implementation. Br. J. Cardiol. 2018, 25, 63–68. [Google Scholar] [CrossRef]
- Kwon, S.H.; Gopal, A.S. 3D and 4D Ultrasound: Current Progress and Future Perspectives. Curr. Cardiovasc. Imaging Rep. 2017, 10, 43. [Google Scholar] [CrossRef] [Green Version]
- Wu, V.; Takeuchi, M. Three-Dimensional Echocardiography: Current Status and Real-Life Applications. Acta Cardiol. Sin. 2017, 33, 107–118. [Google Scholar] [CrossRef] [PubMed]
- Lang, R.M.; Addetia, K.; Narang, A.; Mor-Avi, V. 3-Dimensional Echocardiography. JACC Cardiovasc. Imaging 2018, 11, 1854–1878. [Google Scholar] [CrossRef] [PubMed]
- Baldea, S.M.; Velcea, A.E.; Rimbas, R.C.; Andronic, A.; Matei, L.; Calin, S.I.; Muraru, D.; Badano, L.P.; Vinereanu, D. 3-D Echocardiography Is Feasible and More Reproducible than 2-D Echocardiography for In-Training Echocardiographers in Follow-up of Patients with Heart Failure with Reduced Ejection Fraction. Ultrasound Med. Biol. 2021, 47, 499–510. [Google Scholar] [CrossRef]
- Mancuso, F.J.N.; Moises, V.A.; Almeida, D.R.; Poyares, D.; Storti, L.J.; Brito, F.S.; Tufik, S.; de Paola, A.A.V.; Carvalho, A.C.C.; Campos, O. Prognostic Value of Real-Time Three-Dimensional Echocardiography Compared to Two-Dimensional Echocardiography in Patients with Systolic Heart Failure. Int. J. Cardiovasc. Imaging 2018, 34, 553–560. [Google Scholar] [CrossRef]
- Muraru, D.; Baldea, S.M.; Genovese, D.; Tomaselli, M.; Heilbron, F.; Gavazzoni, M.; Radu, N.; Sergio, C.; Baratto, C.; Perelli, F.; et al. Association of Outcome with Left Ventricular Volumes and Ejection Fraction Measured with Two- and Three-Dimensional Echocardiography in Patients Referred for Routine, Clinically Indicated Studies. Front. Cardiovasc. Med. 2022, 9, 1065131. [Google Scholar] [CrossRef]
- Maeder, M.T.; Karapanagiotidis, S.; Dewar, E.M.; Kaye, D.M. Accuracy of Echocardiographic Cardiac Index Assessment in Subjects with Preserved Left Ventricular Ejection Fraction. Echocardiography 2015, 32, 1628–1638. [Google Scholar] [CrossRef]
- Zhang, Y.; Wang, Y.; Shi, J.; Hua, Z.; Xu, J. Cardiac Output Measurements via Echocardiography versus Thermodilution: A Systematic Review and Meta-Analysis. PLoS ONE 2019, 14, e0222105. [Google Scholar] [CrossRef] [PubMed]
- Rusinaru, D.; Bohbot, Y.; Djelaili, F.; Delpierre, Q.; Altes, A.; Serbout, S.; Kubala, M.; Maréchaux, S.; Tribouilloy, C. Normative Reference Values of Cardiac Output by Pulsed-Wave Doppler Echocardiography in Adults. Am. J. Cardiol. 2021, 140, 128–133. [Google Scholar] [CrossRef] [PubMed]
- Knutsen, K.M.; Otterstad, J.E.; Frøland, G.; Stugaard, M.; Michelsen, S. Determination of Cardiac Output by Doppler Echocardiography InApparently Healthy, Non-Athletic Men Aged 20-70 Years. Am. J. Noninvas. Cardiol. 1989, 3, 36–41. [Google Scholar] [CrossRef]
- Kou, S.; Caballero, L.; Dulgheru, R.; Voilliot, D.; De Sousa, C.; Kacharava, G.; Athanassopoulos, G.D.; Barone, D.; Baroni, M.; Cardim, N.; et al. Echocardiographic Reference Ranges for Normal Cardiac Chamber Size: Results from the NORRE Study. Eur. Heart J. Cardiovasc. Imaging 2014, 15, 680–690. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bernard, A.; Addetia, K.; Dulgheru, R.; Caballero, L.; Sugimoto, T.; Akhaladze, N.; Athanassopoulos, G.D.; Barone, D.; Baroni, M.; Cardim, N.; et al. 3D Echocardiographic Reference Ranges for Normal Left Ventricular Volumes and Strain: Results from the EACVI NORRE Study. Eur. Heart J. Cardiovasc. Imaging 2017, 18, 475–483. [Google Scholar] [CrossRef] [PubMed]
- Muraru, D.; Badano, L.P.; Peluso, D.; Dal Bianco, L.; Casablanca, S.; Kocabay, G.; Zoppellaro, G.; Iliceto, S. Comprehensive Analysis of Left Ventricular Geometry and Function by Three-Dimensional Echocardiography in Healthy Adults. J. Am. Soc. Echocardiogr. 2013, 26, 618–628. [Google Scholar] [CrossRef] [PubMed]
- Muraru, D.; Badano, L.P.; Piccoli, G.; Gianfagna, P.; Del Mestre, L.; Ermacora, D.; Proclemer, A. Validation of a Novel Automated Border-Detection Algorithm for Rapid and Accurate Quantitation of Left Ventricular Volumes Based on Three-Dimensional Echocardiography. Eur. Heart J. Cardiovasc. Imaging 2010, 11, 359–368. [Google Scholar] [CrossRef] [Green Version]
- Le Ven, F.; Bibeau, K.; De Larochellière, É.; Tizón-Marcos, H.; Deneault-Bissonnette, S.; Pibarot, P.; Deschepper, C.F.; Larose, É. Cardiac Morphology and Function Reference Values Derived from a Large Subset of Healthy Young Caucasian Adults by Magnetic Resonance Imaging. Eur. Heart J. Cardiovasc. Imaging 2016, 17, 981–990. [Google Scholar] [CrossRef]
- Tamborini, G.; Marsan, N.A.; Gripari, P.; Maffessanti, F.; Brusoni, D.; Muratori, M.; Caiani, E.G.; Fiorentini, C.; Pepi, M. Reference Values for Right Ventricular Volumes and Ejection Fraction with Real-Time Three-Dimensional Echocardiography: Evaluation in a Large Series of Normal Subjects. J. Am. Soc. Echocardiogr. 2010, 23, 109–115. [Google Scholar] [CrossRef]
- Maffessanti, F.; Muraru, D.; Esposito, R.; Gripari, P.; Ermacora, D.; Santoro, C.; Tamborini, G.; Galderisi, M.; Pepi, M.; Badano, L.P. Age-, Body Size-, and Sex-Specific Reference Values for Right Ventricular Volumes and Ejection Fraction by Three-Dimensional Echocardiography: A Multicenter Echocardiographic Study in 507 Healthy Volunteers. Circ. Cardiovasc. Imaging 2013, 6, 700–710. [Google Scholar] [CrossRef] [Green Version]
- Baumgartner, H.; Hung, J.; Bermejo, J.; Chambers, J.B.; Edvardsen, T.; Goldstein, S.; Lancellotti, P.; LeFevre, M.; Miller, F.; Otto, C.M. Recommendations on the Echocardiographic Assessment of Aortic Valve Stenosis: A Focused Update from the European Association of Cardiovascular Imaging and the American Society of Echocardiography. Eur. Heart J. Cardiovasc. Imaging 2017, 18, 254–275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baumgartner, H.; Kratzer, H.; Helmreich, G.; Kuehn, P. Determination of Aortic Valve Area by Doppler Echocardiography Using the Continuity Equation: A Critical Evaluation. Cardiology 1990, 77, 101–111. [Google Scholar] [CrossRef] [PubMed]
- Zoghbi, W.A.; Farmer, K.L.; Soto, J.G.; Nelson, J.G.; Quinones, M.A. Accurate Noninvasive Quantification of Stenotic Aortic Valve Area by Doppler Echocardiography. Circulation 1986, 73, 452–459. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anavekar, N.S.; Oh, J.K. Doppler Echocardiography: A Contemporary Review. J. Cardiol. 2009, 54, 347–358. [Google Scholar] [CrossRef] [Green Version]
- Lancellotti, P.; Magne, J.; Donal, E.; Davin, L.; O’Connor, K.; Rosca, M.; Szymanski, C.; Cosyns, B.; Piérard, L.A. Clinical Outcome in Asymptomatic Severe Aortic Stenosis. J. Am. Coll. Cardiol. 2012, 59, 235–243. [Google Scholar] [CrossRef]
- Uretsky, S.; Gillam, L.; Lang, R.; Chaudhry, F.A.; Argulian, E.; Supariwala, A.; Gurram, S.; Jain, K.; Subero, M.; Jang, J.J.; et al. Discordance between Echocardiography and MRI in the Assessment of Mitral Regurgitation Severity. J. Am. Coll. Cardiol. 2015, 65, 1078–1088. [Google Scholar] [CrossRef] [Green Version]
- Uretsky, S.; Argulian, E.; Narula, J.; Wolff, S.D. Use of Cardiac Magnetic Resonance Imaging in Assessing Mitral Regurgitation. J. Am. Coll. Cardiol. 2018, 71, 547–563. [Google Scholar] [CrossRef]
- Uretsky, S.; Aldaia, L.; Marcoff, L.; Koulogiannis, K.; Argulian, E.; Lasam, G.; Gillam, L. Concordance and Discordance of Echocardiographic Parameters Recommended for Assessing the Severity of Mitral Regurgitation. Circ. Cardiovasc. Imaging 2020, 13, e010278. [Google Scholar] [CrossRef]
- Uretsky, S.; Animashaun, I.B.; Sakul, S.; Aldaia, L.; Marcoff, L.; Koulogiannis, K.; Argulian, E.; Rosenthal, M.; Wolff, S.D.; Gillam, L.D. American Society of Echocardiography Algorithm for Degenerative Mitral Regurgitation. JACC Cardiovasc. Imaging 2022, 15, 747–760. [Google Scholar] [CrossRef]
- Hahn, R.T. Disproportionate Emphasis on Proportionate Mitral Regurgitation—Are There Better Measures of Regurgitant Severity? JAMA Cardiol. 2020, 5, 377. [Google Scholar] [CrossRef]
- Doenst, T.; Bargenda, S.; Kirov, H.; Moschovas, A.; Tkebuchava, S.; Safarov, R.; Diab, M.; Faerber, G. Cardiac Surgery 2018 Reviewed. Clin. Res. Cardiol. 2019, 108, 974–989. [Google Scholar] [CrossRef] [PubMed]
- Kamoen, V.; Calle, S.; De Buyzere, M.; Timmermans, F. Proportionate or Disproportionate Secondary Mitral Regurgitation: How to Untangle the Gordian Knot? Heart 2020, 106, 1719–1725. [Google Scholar] [CrossRef] [PubMed]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hagendorff, A.; Kandels, J.; Metze, M.; Tayal, B.; Stöbe, S. Valid and Reproducible Quantitative Assessment of Cardiac Volumes by Echocardiography in Patients with Valvular Heart Diseases—Possible or Wishful Thinking? Diagnostics 2023, 13, 1359. https://doi.org/10.3390/diagnostics13071359
Hagendorff A, Kandels J, Metze M, Tayal B, Stöbe S. Valid and Reproducible Quantitative Assessment of Cardiac Volumes by Echocardiography in Patients with Valvular Heart Diseases—Possible or Wishful Thinking? Diagnostics. 2023; 13(7):1359. https://doi.org/10.3390/diagnostics13071359
Chicago/Turabian StyleHagendorff, Andreas, Joscha Kandels, Michael Metze, Bhupendar Tayal, and Stephan Stöbe. 2023. "Valid and Reproducible Quantitative Assessment of Cardiac Volumes by Echocardiography in Patients with Valvular Heart Diseases—Possible or Wishful Thinking?" Diagnostics 13, no. 7: 1359. https://doi.org/10.3390/diagnostics13071359