

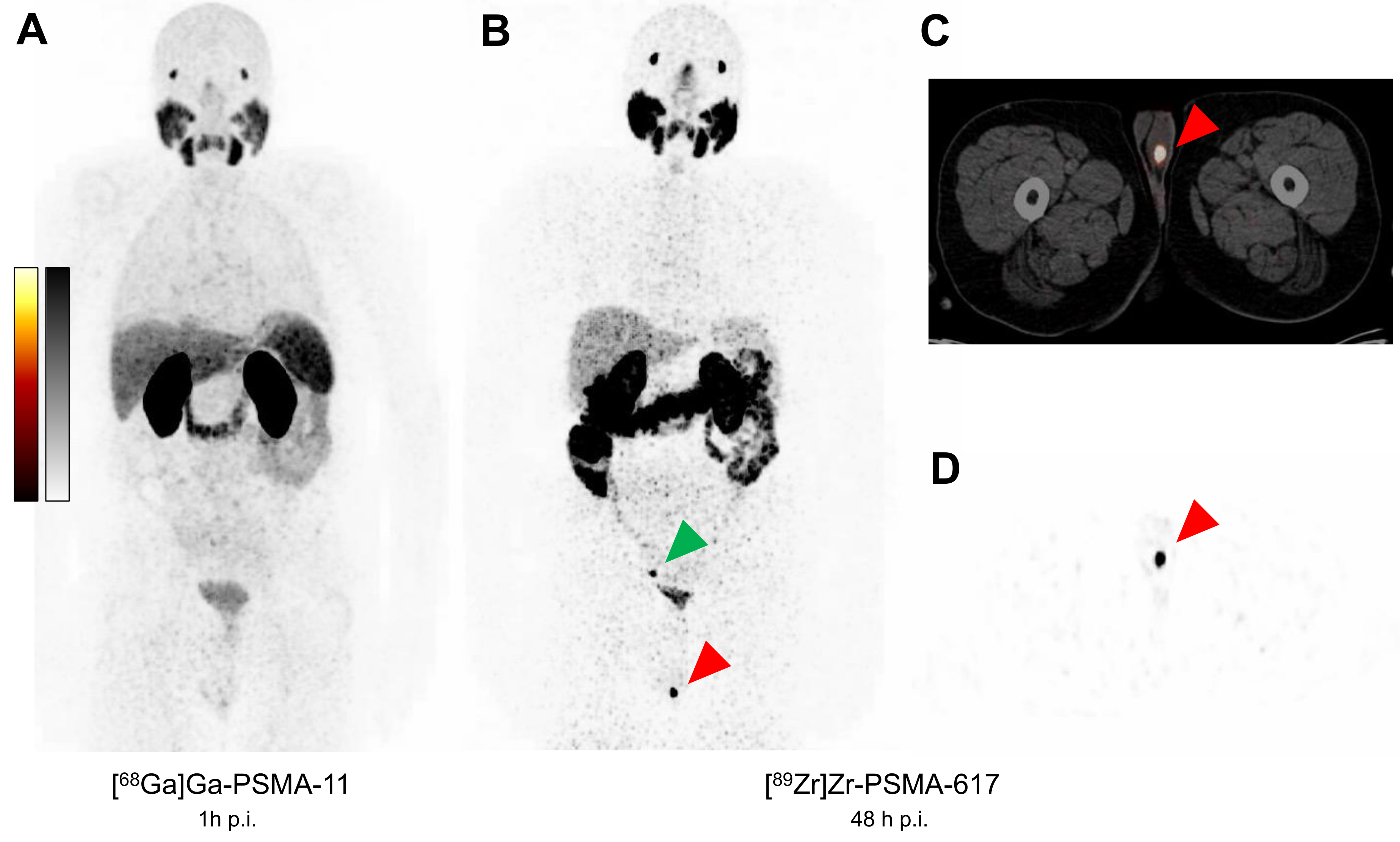
Histologically Confirmed Testicular Metastasis Revealed by [89Zr]Zr-PSMA-617 PET/CT in a Patient with Biochemical Recurrence of Prostate Cancer and Negative Conventional PSMA PET/CT Imaging
 , , ,
, , , {kind=link}
{kind=link}
Abstract
:

Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ghosh, A.; Heston, W.D.W. Tumor Target Prostate Specific Membrane Antigen (PSMA) and Its Regulation in Prostate Cancer. J. Cell. Biochem. 2004, 91, 528–539. [Google Scholar] [CrossRef] [PubMed]
- Hofman, M.S.; Iravani, A.; Nzenza, T.; Murphy, D.G. Advances in Urologic Imaging: Prostate-Specific Membrane Antigen Ligand PET Imaging. Urol. Clin. North. Am. 2018, 45, 503–524. [Google Scholar] [CrossRef] [PubMed]
- Valle, L.; Shabsovich, D.; de Meerleer, G.; Maurer, T.; Murphy, D.G.; Nickols, N.G.; Vapiwala, N.; Calais, J.; Kishan, A.U. Use and Impact of Positron Emission Tomography/Computed Tomography Prior to Salvage Radiation Therapy in Men with Biochemical Recurrence After Radical Prostatectomy: A Scoping Review. Eur. Urol. Oncol. 2021, 4, 339–355. [Google Scholar] [CrossRef] [PubMed]
- Afshar-Oromieh, A.; da Cunha, M.L.; Wagner, J.; Haberkorn, U.; Debus, N.; Weber, W.; Eiber, M.; Holland-Letz, T.; Rauscher, I. Performance of [68Ga]Ga-PSMA-11 PET/CT in Patients with Recurrent Prostate Cancer after Prostatectomy—A Multi-Centre Evaluation of 2533 Patients. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 2925–2934. [Google Scholar] [CrossRef] [PubMed]
- Privé, B.M.; Derks, Y.H.W.; Rosar, F.; Franssen, G.M.; Peters, S.M.B.; Khreish, F.; Bartholomä, M.; Maus, S.; Gotthardt, M.; Laverman, P.; et al. 89Zr-Labeled PSMA Ligands for Pharmacokinetic PET Imaging and Dosimetry of PSMA-617 and PSMA-I&T: A Preclinical Evaluation and First in Man. Eur. J. Nucl. Med. Mol. Imaging 2022, 49, 2064–2076. [Google Scholar] [CrossRef] [PubMed]
- Rosar, F.; Schaefer-Schuler, A.; Bartholomä, M.; Maus, S.; Petto, S.; Burgard, C.; Privé, B.M.; Franssen, G.M.; Derks, Y.H.W.; Nagarajah, J.; et al. [89Zr]Zr-PSMA-617 PET/CT in Biochemical Recurrence of Prostate Cancer: First Clinical Experience from a Pilot Study Including Biodistribution and Dose Estimates. Eur. J. Nucl. Med. Mol. Imaging 2022, 49, 4736–4747. [Google Scholar] [CrossRef] [PubMed]
- Rosar, F.; Bartholomä, M.; Maus, S.; Privé, B.M.; Khreish, F.; Franssen, G.M.; Derks, Y.H.W.; Nagarajah, J.; Ezziddin, S. 89Zr-PSMA-617 PET/CT May Reveal Local Recurrence of Prostate Cancer Unidentified by 68Ga-PSMA-11 PET/CT. Clin. Nucl. Med. 2022, 47, 435–436. [Google Scholar] [CrossRef] [PubMed]
- Dietlein, F.; Kobe, C.; Vázquez, S.M.; Fischer, T.; Endepols, H.; Hohberg, M.; Reifegerst, M.; Neumaier, B.; Schomäcker, K.; Drzezga, A.E.; et al. An 89Zr-Labeled PSMA Tracer for PET/CT Imaging of Prostate Cancer Patients. J. Nucl. Med. 2022, 63, 573–583. [Google Scholar] [CrossRef] [PubMed]
- Gandaglia, G.; Karakiewicz, P.I.; Briganti, A.; Passoni, N.M.; Schiffmann, J.; Trudeau, V.; Graefen, M.; Montorsi, F.; Sun, M. Impact of the Site of Metastases on Survival in Patients with Metastatic Prostate Cancer. Eur. Urol. 2015, 68, 325–334. [Google Scholar] [CrossRef] [PubMed]
- Ruchalski, K.; Kim, H.J.; Douek, M.; Raman, S.; Patel, M.; Sai, V.; Gutierrez, A.; Levine, B.; Fischer, C.; Allen-Auerbach, M.; et al. Pretreatment Visceral Metastases in Castration Resistant Metastatic Prostate Cancer: Role in Prediction versus Actual Site of Disease Progression. Cancer Imaging 2022, 22, 34. [Google Scholar] [CrossRef] [PubMed]
- Gibas, A.; Sieczkowski, M.; Biernat, W.; Matuszewski, M. Isolated Testicular Metastasis of Prostate Cancer after Radical Prostatectomy: Case Report and Literature Review. Urol. Int. 2015, 95, 483–485. [Google Scholar] [CrossRef] [PubMed]
- Smelzo, S.; Mantica, G.; Lucianò, R.; Tenace, N.P.; De Marchi, D.; Pini, G.; Passaretti, G.; Losa, A.; Gaboardi, F. Prostate Cancer Testicular Metastasis: Are They Underestimated? Case Report and Analysis of the Literature. Urologia 2022, 89, 645–647. [Google Scholar] [CrossRef] [PubMed]
- Gupta, N.; Dey, S.; Verma, R.; Belho, E.S. Isolated Testicular Metastasis from Prostate Cancer Detected on Ga-68 PSMA PET/CT Scan. Nucl. Med. Mol. Imaging 2020, 54, 319–323. [Google Scholar] [CrossRef] [PubMed]
- da Cunha, M.L.; de Oliveira Rodrigues, C.; de Araújo, M.P.L.; de Freitas Junior, C.H.; Ferrigno, R. Solitary Testicular Metastasis from Prostate Cancer. A Case Report Diagnosed by PET/CT with PSMA. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 888–889. [Google Scholar] [CrossRef] [PubMed]
- Ege Aktas, G.; Yürüt Çaloğlu, V.; Akdere, H.; Tutuğ, B.B.; Altun, G.D. Biochemical Recurrence of Prostate Cancer Presenting as Solitary Testicular Metastasis on 68Ga-Labeled Prostate-Specific Membrane Antigen Ligand Positron Emission Tomography/Computed Tomography. Clin. Nucl. Med. 2018, 43, 699–700. [Google Scholar] [CrossRef] [PubMed]
- Deeb, I.A.; Khdhir, M.A.; Bulbul, M.; Haidar, M. Solitary Metastasis of Prostatic Adenocarcinoma to the Testicle Detected by 68Ga-Prostate-Specific Membrane Antigen Positron Emission Tomography/Computed Tomography. Indian J. Nucl. Med. 2020, 35, 61–62. [Google Scholar] [CrossRef] [PubMed]
- Weiberg, D.; Radner, H.; Derlin, T.; Thon, W.F. Early Detection of Bilateral Testicular Metastases From Prostatic Adenocarcinoma Using 68Ga-PSMA Ligand PET/CT. Clin. Nucl. Med. 2017, 42, 563–564. [Google Scholar] [CrossRef] [PubMed]
- Kollitsch, L.; Hamann, C.; Knüpfer, S.; Meyer, D.; Kneissl, P.; Jüttner, E.; Osmonov, D. Symptomatic testicular metastasis of acinar adenocarcinoma of the prostate. Urol. A 2020, 59, 1092–1094. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rosar, F.; Burgard, C.; Linxweiler, J.; Wagner, M.; Ezziddin, S. Histologically Confirmed Testicular Metastasis Revealed by [89Zr]Zr-PSMA-617 PET/CT in a Patient with Biochemical Recurrence of Prostate Cancer and Negative Conventional PSMA PET/CT Imaging. Diagnostics 2023, 13, 1352. https://doi.org/10.3390/diagnostics13071352
Rosar F, Burgard C, Linxweiler J, Wagner M, Ezziddin S. Histologically Confirmed Testicular Metastasis Revealed by [89Zr]Zr-PSMA-617 PET/CT in a Patient with Biochemical Recurrence of Prostate Cancer and Negative Conventional PSMA PET/CT Imaging. Diagnostics. 2023; 13(7):1352. https://doi.org/10.3390/diagnostics13071352
Chicago/Turabian StyleRosar, Florian, Caroline Burgard, Johannes Linxweiler, Mathias Wagner, and Samer Ezziddin. 2023. "Histologically Confirmed Testicular Metastasis Revealed by [89Zr]Zr-PSMA-617 PET/CT in a Patient with Biochemical Recurrence of Prostate Cancer and Negative Conventional PSMA PET/CT Imaging" Diagnostics 13, no. 7: 1352. https://doi.org/10.3390/diagnostics13071352