
Pre-Analytical Evaluation of Streck Cell-Free DNA Blood Collection Tubes for Liquid Profiling in Oncology

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics Statement
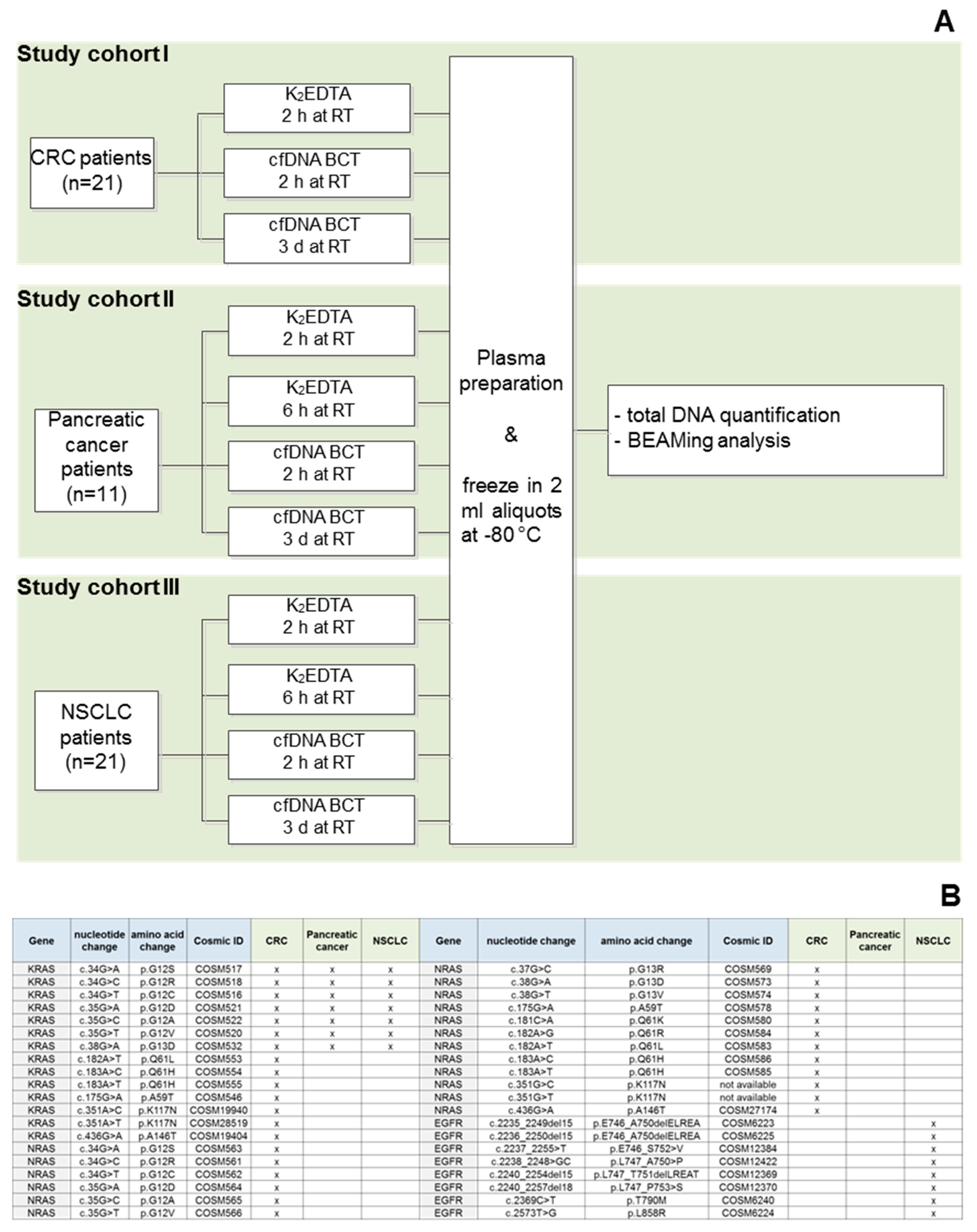
2.2. Blood Collection
2.3. Blood Storage
2.4. Plasma Preparation
2.5. Cell-Free DNA Extraction
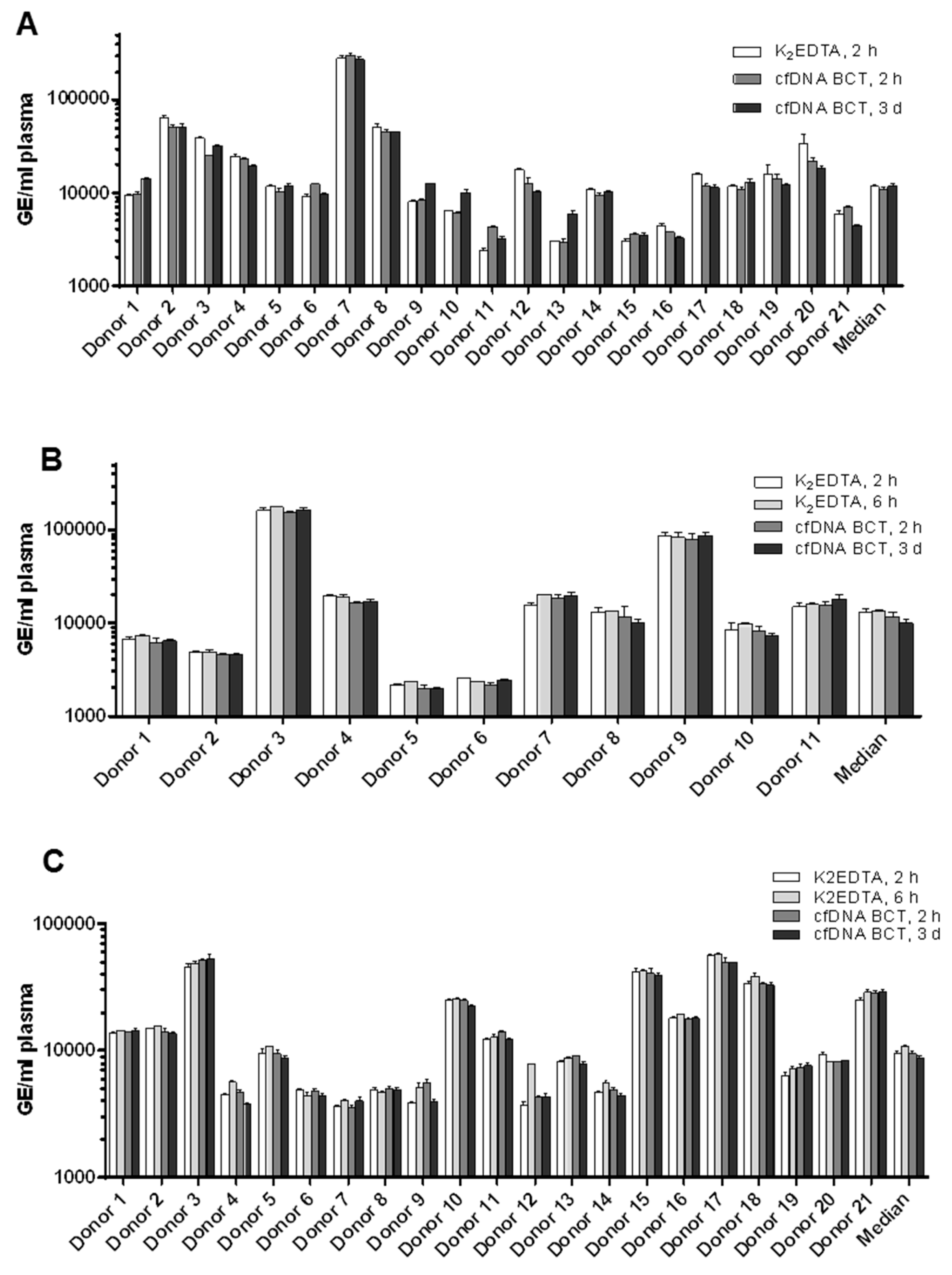
2.6. Cell-Free DNA Quantification
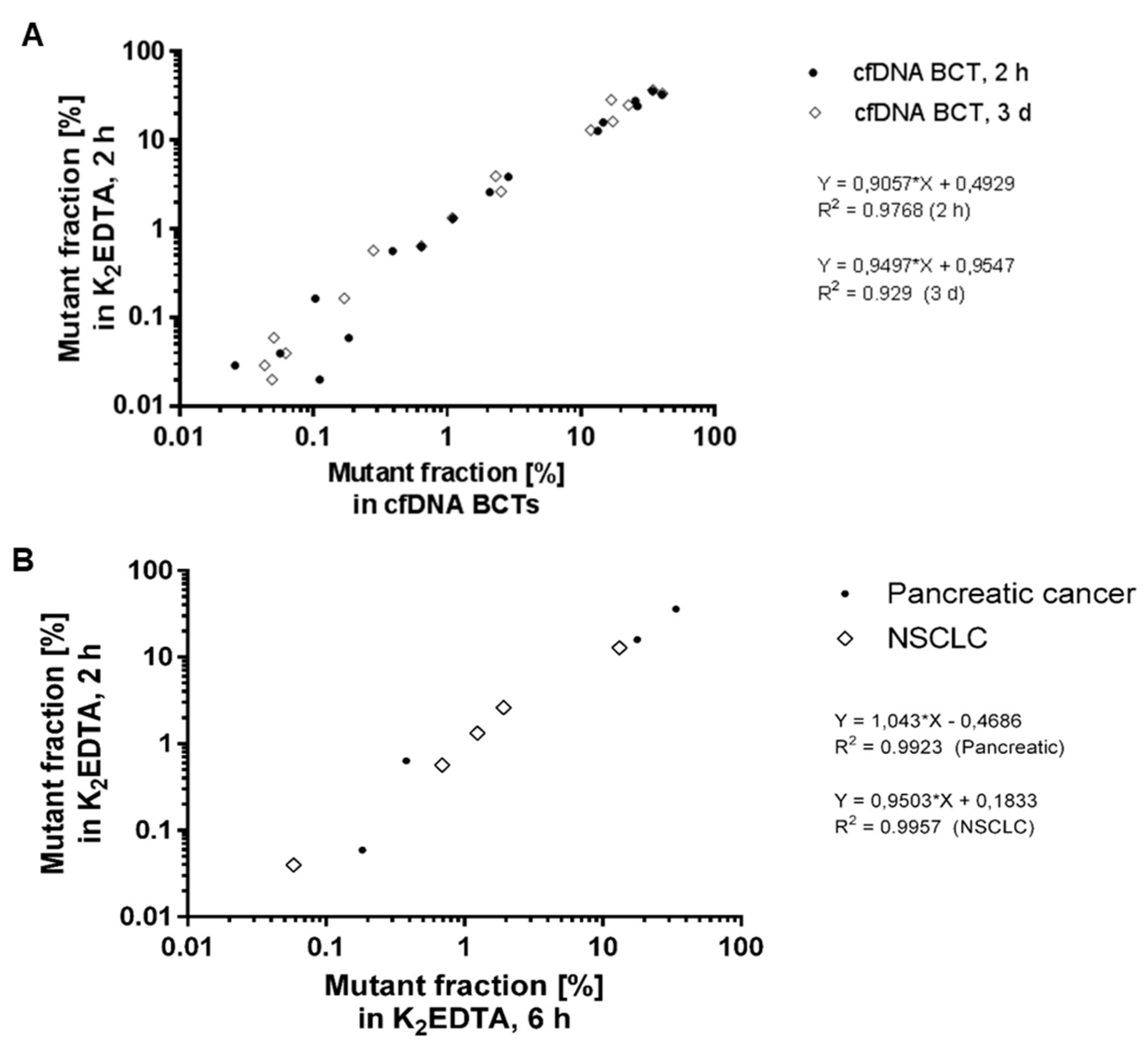
2.7. Mutation Analysis of cfDNA
2.8. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wan, J.C.M.; Massie, C.; Garcia-Corbacho, J.; James, D.; Caldas, C.; Pacey, S.; Baird, R.D.; Rosenfeld, N. Liquid biopsies come of age: Clinical applications of circulating tumour DNA. Nat. Rev. Cancer 2016, 17, 223–238. [Google Scholar] [CrossRef] [PubMed]
- Bronkhorst, A.J.; Ungerer, V.; Oberhofer, A.; Gabriel, S.; Polatoglou, E.; Randeu, H.; Uhlig, C.; Pfister, H.; Mayer, Z.; Holdenrieder, S. New Perspectives on the Importance of Cell-Free DNA Biology. Diagnostics 2022, 12, 2147. [Google Scholar] [CrossRef] [PubMed]
- Tu, M.; Chia, D.; Wei, F.; Wong, D. Liquid biopsy for detection of actionable oncogenic mutations in human cancers and electric field induced release and measurement liquid biopsy (eLB). Analyst 2016, 141, 393–402. [Google Scholar] [CrossRef] [PubMed]
- Medina Diaz, I.; Nocon, A.; Mehnert, D.H.; Fredebohm, J.; Diehl, F.; Holtrup, F. Performance of Streck cfDNA blood collection tubes for liquid biopsy testing. PLoS ONE 2016, 11, e0166354. [Google Scholar] [CrossRef] [PubMed]
- Tsui, D.W.; Barnett, E.; Scher, H.I. Toward Standardization of Preanalytical Procedures for Cell-Free DNA Profiling. Clin. Chem. 2019, 66, 3–5. [Google Scholar] [CrossRef]
- Ungerer, V.; Bronkhorst, A.J.; Holdenrieder, S. Preanalytical variables that affect the outcome of cell-free DNA measurements. Crit. Rev. Clin. Lab. Sci. 2020, 57, 484–507. [Google Scholar] [CrossRef] [PubMed]
- Lampignano, R.; Neumann, M.H.D.; Weber, S.; Kloten, V.; Herdean, A.; Voss, T.; Groelz, D.; Babayan, A.; Tibbesma, M.; Schlumpberger, M.; et al. Multicenter Evaluation of Circulating Cell-Free DNA Extraction and Downstream Analyses for the Development of Standardized (Pre)analytical Work Flows. Clin. Chem. 2020, 66, 149–160. [Google Scholar] [CrossRef]
- Meddeb, R.; Pisareva, E.; Thierry, A.R. Guidelines for the Preanalytical Conditions for Analyzing Circulating Cell-Free DNA. Clin. Chem. 2019, 65, 623–633. [Google Scholar] [CrossRef]
- Norton, S.E.; Luna, K.K.; Lechner, J.M.; Qin, J.; Fernando, M.R. A new blood collection device minimizes cellular DNA release during sample storage and shipping when compared to a standard device. J. Clin. Lab. Anal. 2013, 27, 305–311. [Google Scholar] [CrossRef]
- Norton, S.E.; Lechner, J.M.; Williams, T.; Fernando, M.R. A stabilizing reagent prevents cell-free DNA contamination by cellular DNA in plasma during blood sample storage and shipping as determined by digital PCR. Clin. Biochem. 2013, 46, 1561–1565. [Google Scholar] [CrossRef]
- Barrett, A.N.; Zimmermann, B.G.; Wang, D.; Holloway, A.; Chitty, L.S. Implementing prenatal diagnosis based on cell-free fetal DNA: Accurate identification of factors affecting fetal DNA yield. PLoS ONE 2011, 6, 4–11. [Google Scholar] [CrossRef] [PubMed]
- Jeong, T.-D.; Kim, M.H.; Park, S.; Chung, H.-S.; Lee, J.W.; Chang, J.H.; Huh, J. Effects of Pre-analytical Variables on Cell-free DNA Extraction for Liquid Biopsy. Lab. Med. Online 2019, 9, 45–56. [Google Scholar] [CrossRef]
- Risberg, B.; Tsui, D.W.Y.; Biggs, H.; Ruiz-Valdepenas Martin de Almagro, A.; Dawson, S.J.; Hodgkin, C.; Jones, L.; Parkinson, C.; Piskorz, A.; Marass, F.; et al. Effects of Collection and Processing Procedures on Plasma Circulating Cell-Free DNA from Cancer Patients. J. Mol. Diagn. 2018, 20, 883–892. [Google Scholar] [CrossRef]
- Parpart-Li, S.; Bartlett, B.; Popoli, M.; Adleff, V.; Tucker, L.; Steinberg, R.; Georgiadis, A.; Phallen, J.; Brahmer, J.; Azad, N.; et al. The effect of preservative and temperature on the analysis of circulating tumor DNA. Clin. Cancer Res. 2017, 23, 2471–2477. [Google Scholar] [CrossRef] [PubMed]
- Wong, D.; Moturi, S.; Angkachatchai, V.; Mueller, R.; DeSantis, G.; van den Boom, D.; Ehrich, M. Optimizing blood collection, transport and storage conditions for cell free DNA increases access to prenatal testing. Clin. Biochem. 2013, 46, 1099–1104. [Google Scholar] [CrossRef]
- Fernando, M.R.; Chen, K.; Norton, S.; Krzyzanowski, G.; Bourne, D.; Hunsley, B.; Ryan, W.L.; Bassett, C. A new methodology to preserve the original proportion and integrity of cell-free fetal DNA in maternal plasma during sample processing and storage. Prenat. Diagn. Publ. Affil. Int. Soc. Prenat. Diagn. 2010, 30, 418–424. [Google Scholar] [CrossRef] [PubMed]
- El Messaoudi, S.; Rolet, F.; Mouliere, F.; Thierry, A.R. Circulating cell free DNA: Preanalytical considerations. Clin. Chim. Acta. 2013, 424, 222–230. [Google Scholar] [CrossRef] [PubMed]
- Hrebien, S.; O’Leary, B.; Beaney, M.; Schiavon, G.; Fribbens, C.; Bhambra, A.; Johnson, R.; Garcia-Murillas, I.; Turner, N. Reproducibility of digital PCR assays for circulating tumor DNA analysis in advanced breast cancer. PLoS ONE 2016, 11, e0165023. [Google Scholar] [CrossRef]
- Toro, P.V.; Erlanger, B.; Beaver, J.A.; Cochran, R.L.; VanDenBerg, D.A.; Yakim, E.; Cravero, K.; Chu, D.; Zabransky, D.J.; Wong, H.Y.; et al. Comparison of cell stabilizing blood collection tubes for circulating plasma tumor DNA. Clin. Biochem. 2015, 48, 993–998. [Google Scholar] [CrossRef]
- Kang, Q.; Henry, N.L.; Paoletti, C.; Jiang, H.; Vats, P.; Chinnaiyan, A.M.; Hayes, D.F.; Merajver, S.D.; Rae, J.M.; Tewari, M. Comparative analysis of circulating tumor DNA stability In K3EDTA, Streck, and CellSave blood collection tubes. Clin. Biochem. 2016, 49, 1354–1360. [Google Scholar] [CrossRef]
- Denis, M.G.; Knol, A.-C.; Théoleyre, S.; Vallée, A.; Dréno, B. Efficient detection of BRAF mutation in plasma of patients after long-term storage of blood in cell-free DNA blood collection tubes. Clin. Chem. 2015, 61, 886–888. [Google Scholar] [CrossRef] [PubMed]
- Sherwood, J.L.; Corcoran, C.; Brown, H.; Sharpe, A.D.; Musilova, M.; Kohlmann, A. Optimised pre-analytical methods improve KRAS mutation detection in circulating tumour DNA (ctDNA) from patients with non-small cell lung cancer (NSCLC). PLoS ONE 2016, 11, e0160197. [Google Scholar] [CrossRef] [PubMed]
- Malentacchi, F.; Pizzamiglio, S.; Verderio, P.; Pazzagli, M.; Orlando, C.; Ciniselli, C.M.; Gunther, K.; Gelmini, S. Influence of storage conditions and extraction methods on the quantity and quality of circulating cell-free DNA (ccfDNA): The SPIDIA-DNAplas External Quality Assessment experience. Clin. Chem. Lab. Med. 2015, 53, 1935–1942. [Google Scholar] [CrossRef] [PubMed]
- Fleischhacker, M.; Schmidt, B.; Weickmann, S.; Fersching, D.M.I.; Leszinski, G.S.; Siegele, B.; Stötzer, O.J.; Nagel, D.; Holdenrieder, S. Methods for isolation of cell-free plasma DNA strongly affect DNA yield. Clin. Chim. Acta 2011, 412, 2085–2088. [Google Scholar] [CrossRef] [PubMed]
- Bronkhorst, A.J.; Aucamp, J.; Pretorius, P.J. Cell-free DNA: Preanalytical variables. Clin. Chim. Acta 2015, 450, 243–253. [Google Scholar] [CrossRef]
- Greytak, S.R.; Engel, K.B.; Parpart-Li, S.; Murtaza, M.; Bronkhorst, A.J.; Pertile, M.D.; Moore, H.M. Harmonizing cell-free DNA collection and processing practices through evidence-based guidance. Clin. Cancer Res. 2020, 26, 3104–3109. [Google Scholar] [CrossRef]
- Rago, C.; Huso, D.L.; Diehl, F.; Karim, B.; Liu, G.; Papadopoulos, N.; Samuels, Y.; Velculescu, V.E.; Vogelstein, B.; Kinzler, K.W.; et al. Serial assessment of human tumor burdens in mice by the analysis of circulating DNA. Cancer Res. 2007, 67, 9364–9370. [Google Scholar] [CrossRef]
- Jiang, P.; Lo, Y.M.D. The Long and Short of Circulating Cell-Free DNA and the Ins and Outs of Molecular Diagnostics. Trends Genet. 2016, 32, 360–371. [Google Scholar] [CrossRef]
- Mouliere, F.; Robert, B.; Arnau Peyrotte, E.; Del Rio, M.; Ychou, M.; Molina, F.; Gongora, C.; Thierry, A.R. High fragmentation characterizes tumour-derived circulating DNA. PLoS ONE 2011, 6, e23418. [Google Scholar] [CrossRef]
- Diehl, F.; Li, M.; He, Y.; Kinzler, K.W.; Vogelstein, B.; Dressman, D. BEAMing: Single-molecule PCR on microparticles in water-in-oil emulsions. Nat. Methods 2006, 3, 551–559. [Google Scholar] [CrossRef]
- Van Dessel, L.F.; Beije, N.; Helmijr, J.C.A.; Vitale, S.R.; Kraan, J.; Look, M.P.; de Wit, R.; Sleijfer, S.; Jansen, M.P.H.M.; Martens, J.W.M.; et al. Application of circulating tumor DNA in prospective clinical oncology trials—Standardization of preanalytical conditions. Mol. Oncol. 2017, 11, 295–304. [Google Scholar] [CrossRef] [PubMed]
- Warton, K.; Yuwono, N.L.; Cowley, M.J.; McCabe, M.J.; So, A.; Ford, C.E. Evaluation of Streck BCT and PAXgene Stabilised Blood Collection Tubes for Cell-Free Circulating DNA Studies in Plasma. Mol. Diagn. Ther. 2017, 21, 563–570. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, B.; Reinicke, D.; Reindl, I.; Bork, I.; Wollschläger, B.; Lambrecht, N.; Fleischhacker, M. Liquid biopsy—Performance of the PAXgene® Blood ccfDNA Tubes for the isolation and characterization of cell-free plasma DNA from tumor patients. Clin. Chim. Acta 2017, 469, 94–98. [Google Scholar] [CrossRef]
- Rothwell, D.G.; Smith, N.; Morris, D.; Leong, H.S.; Li, Y.; Hollebecque, A.; Ayub, M.; Carter, L.; Antonello, J.; Franklin, L.; et al. Genetic profiling of tumours using both circulating free DNA and circulating tumour cells isolated from the same preserved whole blood sample. Mol. Oncol. 2016, 10, 566–574. [Google Scholar] [CrossRef]
- Parackal, S.; Zou, D.; Day, R.; Black, M.; Guilford, P. Comparison of Roche Cell-Free DNA collection Tubes® to Streck Cell-Free DNA BCT®s for sample stability using healthy volunteers. Pract. Lab. Med. 2019, 16, e00125. [Google Scholar] [CrossRef] [PubMed]
- Bronkhorst, A.J.; Ungerer, V.; Holdenrieder, S. The emerging role of cell-free DNA as a molecular marker for cancer management. Biomol. Detect. Quantif. 2019, 17, 100087. [Google Scholar] [CrossRef]
- Van der Pol, Y.; Mouliere, F. Toward the Early Detection of Cancer by Decoding the Epigenetic and Environmental Fingerprints of Cell-Free DNA. Cancer Cell 2019, 36, 350–368. [Google Scholar] [CrossRef]
- Oberhofer, A.; Bronkhorst, A.J.; Uhlig, C.; Ungerer, V.; Holdenrieder, S. Tracing the Origin of Cell-Free DNA Molecules through Tissue-Specific Epigenetic Signatures. Diagnostics 2022, 12, 1834. [Google Scholar] [CrossRef]
- Distler, J.; Tetzner, R.; Weiss, G.; Knig, T.; Schlegel, A.; Bagrowski, M. Evaluation of Different Blood Collection Tubes and Blood Storage Conditions for the Preservation and Stability of Cell-Free Circulating DNA for the Analysis of the Methylated mSEPT9 Colorectal Cancer Screening Marker. In Circulating Nucleic Acids in Serum and Plasma–CNAPS IX; Springer International Publishing: New York, NY, USA, 2016; pp. 175–178. [Google Scholar]
- Gahlawat, A.W.; Lenhardt, J.; Witte, T.; Keitel, D.; Kaufhold, A.; Maass, K.K.; Pajtler, K.W.; Sohn, C.; Schott, S. Evaluation of storage tubes for combined analysis of circulating nucleic acids in liquid biopsies. Int. J. Mol. Sci. 2019, 20, 704. [Google Scholar] [CrossRef]
- Heitzer, E.; Haque, I.S.; Roberts, C.E.S.; Speicher, M.R. Current and future perspectives of liquid biopsies in genomics-driven oncology. Nat. Rev. Genet. 2019, 20, 71–88. [Google Scholar] [CrossRef]
- Alidousty, C.; Brandes, D.; Heydt, C.; Wagener, S.; Wittersheim, M.; Schäfer, S.C.; Holz, B.; Merkelbach-Bruse, S.; Büttner, R.; Fassunke, J.; et al. Comparison of Blood Collection Tubes from Three Different Manufacturers for the Collection of Cell-Free DNA for Liquid Biopsy Mutation Testing. J. Mol. Diagn. 2017, 19, 801–804. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cancer Type | Sample ID | Stage | Mutation | Mutant Fraction (%) | Total DNA Amount (GE) | Mutant Molecules |
|---|---|---|---|---|---|---|
| Colorectal | Donor 2, K2EDTA, 2h, RT | IVB | KRAS_g38a | 32.83 | 117553 | 38593 |
| Donor 2, cfDNA BCT, 2h, RT | 41.63 | 93975 | 39119 | |||
| Donor 2, cfDNA BCT, 3d, RT | 40.84 | 94172 | 38457 | |||
| Donor 3, K2EDTA, 2h, RT | IVA | KRAS_g34t | 27.86 | 70947 | 19768 | |
| Donor 3, cfDNA BCT, 2h, RT | 26.24 | 45306 | 11887 | |||
| Donor 3, cfDNA BCT, 3d, RT | 16.87 | 58550 | 9877 | |||
| Donor 5, K2EDTA, 2h, RT | IIA | KRAS_g38a | 0.020 | 21197 | 4,2 | |
| Donor 5, cfDNA BCT, 2h, RT | 0.112 | 18873 | 21 | |||
| Donor 5, cfDNA BCT, 3d, RT | 0.049 | 21505 | 11 | |||
| Donor 7, K2EDTA, 2h, RT | IV | KRAS_g35a | 24.36 | 518814 | 126362 | |
| Donor 7, cfDNA BCT, 2h, RT | 27.25 | 554853 | 151175 | |||
| Donor 7, cfDNA BCT, 3d, RT | 22.70 | 501963 | 113966 | |||
| Donor 7, K2EDTA, 2h, RT | IV | NRAS_g34a | 0.029 | 518814 | 151 | |
| Donor 7, cfDNA BCT, 2h, RT | 0.026 | 554853 | 144 | |||
| Donor 7, cfDNA BCT, 3d, RT | 0.043 | 501963 | 216 | |||
| Donor 10, K2EDTA, 2h, RT | III B | KRAS_a183t | 0.164 | 14514 | 24 | |
| Donor 10, cfDNA BCT, 2h, RT | 0.104 | 14883 | 15 | |||
| Donor 10, cfDNA BCT, 3d, RT | 0.170 | 23001 | 39 | |||
| Donor 18, K2EDTA, 2h, RT | IVB | KRAS_g35t | 3.883 | 28816 | 1119 | |
| Donor 18, cfDNA BCT, 2h, RT | 2.923 | 21746 | 636 | |||
| Donor 18, cfDNA BCT, 3d, RT | 2.306 | 20766 | 479 | |||
| Pancreatic | Donor 18, K2EDTA, 2h, RT | n/a | KRAS_1_g35t | 0.632 | 11550 | 72.9 |
| Donor 18, K2EDTA, 6h, RT | 0.381 | 13338 | 50.8 | |||
| Donor 18, cfDNA BCT, 2h, RT | 0.647 | 10716 | 69.4 | |||
| Donor 18, cfDNA BCT, 3d, RT | 0.641 | 11055 | 70.9 | |||
| Donor 06, K2EDTA, 2h, RT | n/a | KRAS_1_g35t | 0.059 | 4629 | 2.7 | |
| Donor 06, K2EDTA, 6h, RT | 0.183 | 3725 | 6.8 | |||
| Donor 06, cfDNA BCT, 2h, RT | 0.185 | 3269 | 6.1 | |||
| Donor 06, cfDNA BCT, 3d, RT | 0.051 | 3952 | 2.0 | |||
| Donor 07, K2EDTA, 2h, RT | n/a | KRAS_1_g35a | 35.99 | 28001 | 10078.7 | |
| Donor 07, K2EDTA, 6h, RT | 33.87 | 30269 | 10252.7 | |||
| Donor 07, cfDNA BCT, 2h, RT | 35.32 | 33783 | 11930.7 | |||
| Donor 07, cfDNA BCT, 3d, RT | 34.50 | 36337 | 12536.1 | |||
| Donor 09, K2EDTA, 2h, RT | n/a | KRAS_1_g35a | 15.94 | 153645 | 24497.9 | |
| Donor 09, K2EDTA, 6h, RT | 17.82 | 145873 | 25994.9 | |||
| Donor 09, cfDNA BCT, 2h, RT | 15.04 | 140710 | 21155.8 | |||
| Donor 09, cfDNA BCT, 3d, RT | 17.33 | 157914 | 27367.4 | |||
| NSCLC | Donor 03, K2EDTA, 2h, RT | n/a | KRAS_1_g35a | 0.040 | 69619 | 27.6 |
| Donor 03, K2EDTA, 6h, RT | 0.058 | 89446 | 52.2 | |||
| Donor 03, cfDNA BCT, 2h, RT | 0.057 | 93901 | 53.1 | |||
| Donor 03, cfDNA BCT, 3d, RT | 0.062 | 96664 | 59.8 | |||
| Donor 06, K2EDTA, 2h, RT | n/a | KRAS_1_g34t | 0.564 | 8816 | 49.7 | |
| Donor 06, K2EDTA, 6h, RT | 0.690 | 7901 | 54.5 | |||
| Donor 06, cfDNA BCT, 2h, RT | 0.396 | 8656 | 34.3 | |||
| Donor 06, cfDNA BCT, 3d, RT | 0.280 | 7936 | 22.2 | |||
| Donor 08, K2EDTA, 2h, RT | n/a | KRAS_1_g35c | 1.312 | 9025 | 118.4 | |
| Donor 08, K2EDTA, 6h, RT | 1.243 | 8654 | 107.6 | |||
| Donor 08, cfDNA BCT, 2h, RT | 1.120 | 9162 | 102.6 | |||
| Donor 08, cfDNA BCT, 3d, RT | 1.091 | 9005 | 98.2 | |||
| Donor 20, K2EDTA, 2h, RT | n/a | KRAS_1_g35t | 12.71 | 15415 | 1958.9 | |
| Donor 20, K2EDTA, 6h, RT | 13.25 | 14294 | 1893.8 | |||
| Donor 20, cfDNA BCT, 2h, RT | 13.70 | 14570 | 1996.6 | |||
| Donor 20, cfDNA BCT, 3d, RT | 11.87 | 14914 | 1770.7 | |||
| Donor 21, K2EDTA, 2h, RT | n/a | EGFR_19_2236-50D | 2.602 | 45839 | 1192.7 | |
| Donor 21, K2EDTA, 6h, RT | 1.921 | 52731 | 1013.0 | |||
| Donor 21, cfDNA BCT, 2h, RT | 2.116 | 52190 | 1104.1 | |||
| Donor 21, cfDNA BCT, 3d, RT | 2.533 | 53279 | 1349.3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Diaz, I.M.; Nocon, A.; Held, S.A.E.; Kobilay, M.; Skowasch, D.; Bronkhorst, A.J.; Ungerer, V.; Fredebohm, J.; Diehl, F.; Holdenrieder, S.; et al. Pre-Analytical Evaluation of Streck Cell-Free DNA Blood Collection Tubes for Liquid Profiling in Oncology. Diagnostics 2023, 13, 1288. https://doi.org/10.3390/diagnostics13071288
Diaz IM, Nocon A, Held SAE, Kobilay M, Skowasch D, Bronkhorst AJ, Ungerer V, Fredebohm J, Diehl F, Holdenrieder S, et al. Pre-Analytical Evaluation of Streck Cell-Free DNA Blood Collection Tubes for Liquid Profiling in Oncology. Diagnostics. 2023; 13(7):1288. https://doi.org/10.3390/diagnostics13071288
Chicago/Turabian StyleDiaz, Inga Medina, Annette Nocon, Stefanie A. E. Held, Makbule Kobilay, Dirk Skowasch, Abel J. Bronkhorst, Vida Ungerer, Johannes Fredebohm, Frank Diehl, Stefan Holdenrieder, and et al. 2023. "Pre-Analytical Evaluation of Streck Cell-Free DNA Blood Collection Tubes for Liquid Profiling in Oncology" Diagnostics 13, no. 7: 1288. https://doi.org/10.3390/diagnostics13071288