
The Diagnostic Challenge of Osteoid Osteoma in the Bones of the Hand—A Case Series
 ,
,
Abstract
:1. Introduction
2. Methods
3. Results
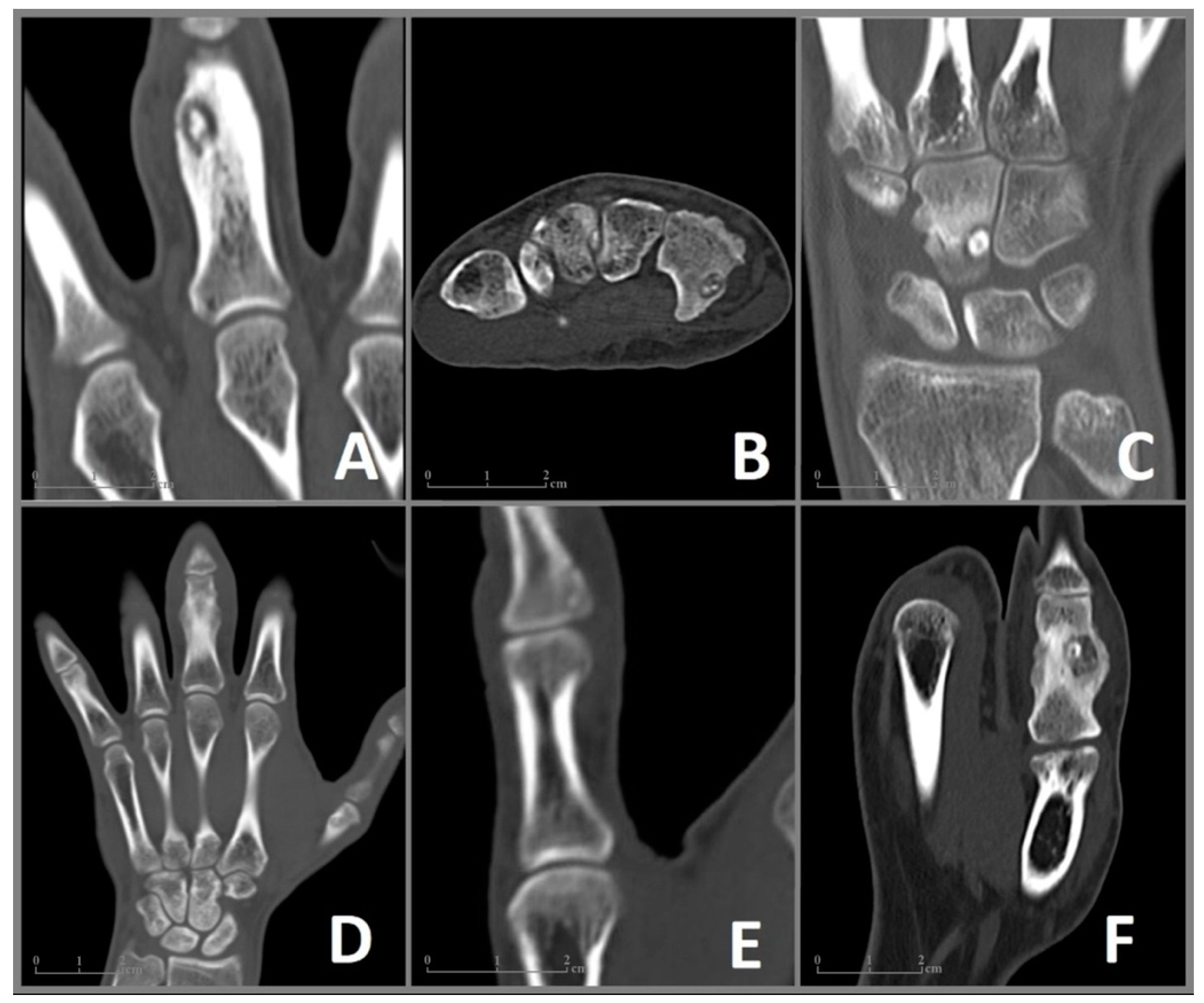
3.1. Case 1
3.2. Case 2
3.3. Case 3
3.4. Case 4
3.5. Case 5
3.6. Case 6
3.7. Summary of the Patient Cohort
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jaffe, H.L. Osteoid Osteoma: A benign osteoblastic tumor composed of osteoid and atypical bone. Arch. Surg. 1935, 31, 709–728. [Google Scholar] [CrossRef]
- Hakim, D.N.; Pelly, T.; Kulendran, M.; Caris, J.A. Benign tumours of the bone: A review. J. Bone Oncol. 2015, 4, 37–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lam, Y. Bone Tumors: Benign Bone Tumors. FP Essent. 2020, 493, 11–21. [Google Scholar] [PubMed]
- Klei, M.H.; Shankman, S. Osteoid osteoma: Radiologic and pathologic correlation. Skelet. Radiol. 1992, 21, 23–31. [Google Scholar]
- Jordan, R.W.; Koç, T.; Chapman, A.W.; Taylor, H.P. Osteoid osteoma of the foot and ankle—A systematic review. Foot. Ankle Surg. 2015, 21, 228–234. [Google Scholar] [CrossRef]
- Erdogan, O.; Gurkan, V. Hand osteoid osteoma: Evaluation of diagnosis and treatment. Eur. J. Med. Res. 2019, 24, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kotnis, N.; James, S.L. Imaging features of osteoid osteoma of the phalanges. Skelet. Radiol. 2015, 44, 1461–1466. [Google Scholar] [CrossRef]
- Rolvien, T.; Krause, M.; Zustin, J.; Yastrebov, O.; Oheim, R.; Barvencik, F.; Frosch, K.-H.; Amling, M. Intra-articular osteoid osteoma accompanied by extensive bone marrow edema. A clinical and micro-morphological analysis. J. Bone Oncol. 2019, 18, 100256. [Google Scholar] [CrossRef]
- Simon, M.J.K.; Pogoda, P.; Hövelborn, F.; Krause, M.; Zustin, J.; Amling, M.; Barvencik, F. Incidence, histopathologic analysis and distribution of tumours of the hand. BMC Musculoskelet. Disord. 2014, 15, 182. [Google Scholar] [CrossRef] [Green Version]
- Liu, E.H.; Stone, N.; Alowami, S.O.; Thoma, A. Proximal Phalanx Osteoid Osteoma: A Case Report and Literature Review. Plast. Reconstr. Surg. Glob. Open. 2017, 5, e1332. [Google Scholar] [CrossRef]
- Themistocleous, G.S.; Chloros, G.D.; Mavrogenis, A.F.; Khaldi, L.; Papagelopoulos, P.J.; Efstathopoulos, D.G. Unusual presentation of osteoid osteoma of the scaphoid. Arch. Orthop. Trauma Surg. 2005, 125, 482–485. [Google Scholar] [CrossRef] [PubMed]
- De Smet, L.; Fabry, G. Clubbing of single digit: An unusual cause. Clin. Rheumatol. 1996, 15, 310–311. [Google Scholar] [CrossRef] [PubMed]
- Levy, Y.; Rosenheck, S.; Greiff, M.; Torok, G. Osteoid osteoma of the distal phalanx of the thumb. Acta. Orthop. Scand. 1979, 50 Pt 1, 667–669. [Google Scholar] [CrossRef] [PubMed]
- Andalib, A.; Sajadie-Khajouei, S. Osteoid osteoma of distal phalanx: A rare disorder and review of literature. J. Res. Med. Sci. 2013, 18, 264–266. [Google Scholar] [PubMed]
- Rolvien, T.; Zustin, J.; Mussawy, H.; Schmidt, T.; Pogoda, P.; Ueblacker, P. Intra-articular osteoid osteoma as a differential diagnosis of diffuse mono-articular joint pain. BMC Musculoskelet. Disord. 2016, 17, 455. [Google Scholar] [CrossRef] [Green Version]
- Taylor, S.A.; Trehan, S.K.; Crivello, K.M.; Schneider, R.; Wolfe, S.W. Osteoid osteoma of the triquetrum: A case of four-year delay in diagnosis. HSS J. 2014, 10, 191–196. [Google Scholar] [CrossRef] [Green Version]
- Vlaic, J.; Lamot, L.; Šimunić, S.; Harjacek, M.; Bojic, D. Unusual localization and presentation of osteoid osteoma mimicking juvenile spondyloarthritis: A case report. BMC Musculoskelet. Disord. 2019, 20, 17. [Google Scholar] [CrossRef]
- Katolik, L.I. Osteoid osteoma of the scaphoid presenting with radiocarpal arthritis: A case report. Hand 2009, 4, 187–190. [Google Scholar] [CrossRef] [Green Version]
- Rajeev, A.; Ali, M.; Ralte, A.; Chakaravathy, J. Osteoid osteoma as an unusual cause of wrist pain—A case report and review of literature. Int. J. Surg. Case. Rep. 2014, 5, 896–898. [Google Scholar] [CrossRef] [Green Version]
- Ge, S.M.; Marwan, Y.; Abduljabbar, F.H.; Morelli, M.; Turcotte, R.E. Arthroscopic management of intra- and juxta-articular osteoid osteoma of the upper extremity: A systematic review of the literature. Eur. J. Orthop. Surg. Traumatol. 2020, 30, 1333–1344. [Google Scholar] [CrossRef]
- Franceschi, F.; Marinozzi, A.; Papalia, R.; Longo, U.G.; Gualdi, G.; Denaro, E. Intra- and juxta-articular osteoid osteoma: A diagnostic challenge: Misdiagnosis and successful treatment: A report of four cases. Arch. Orthop. Trauma. Surg. 2006, 126, 660–667. [Google Scholar] [CrossRef]
- Boscainos, P.J.; Cousins, G.R.; Kulshreshtha, R.; Oliver, T.B.; Papagelopoulos, P.J. Osteoid osteoma. Orthopedics 2013, 36, 792–800. [Google Scholar] [CrossRef] [PubMed]
- Ayas, M.S.; Gül, O.; Okutan, A.E.; Kerimoğlu, S.; Yıldız, M.; Turhan, A.U.; Aynacı, O. Effectiveness and reliability of traditional open surgery in atypical localizations of osteoid osteoma. Jt. Dis. Relat. Surg. 2020, 31, 541–547. [Google Scholar] [CrossRef] [PubMed]
- Burger, I.M.; McCarthy, E.F. Phalangeal osteoid osteomas in the hand: A diagnostic problem. Clin. Orthop. Relat. Res. 2004, 427, 198–203. [Google Scholar] [CrossRef] [PubMed]
- Soler, J.M.; Pizà, G.; Aliaga, F. Special characteristics of osteoid osteoma in the proximal phalanx. J. Hand Surg. Br. 1997, 22, 793–797. [Google Scholar] [CrossRef] [PubMed]
- Hamdi, M.F.; Tarhouni, L.; Daghfous, M.; Bergaoui, N.; Baccari, S. Osteoid osteoma of the phalanx and metacarpal bone: Report of 17 cases. Musculoskelet. Surg. 2015, 99, 61–65. [Google Scholar] [CrossRef]
- Davies, M.; Cassar-Pullicino, V.N.; McCall, I.W.; Tyrrell, P.N. The diagnostic accuracy of MR imaging in osteoid osteoma. Skelet. Radiol. 2002, 31, 559–569. [Google Scholar] [CrossRef]
- Lisanti, M.; Rosati, M.; Spagnolli, G.; Luppichini, G. Osteoid osteoma of the carpus. Case reports and a review of the literature. Acta Orthop. Belg. 1996, 62, 195–199. [Google Scholar]
- Mahajan, S.; Chandra, R.; Mohan Lal, Y. “Nora lesion”—Bizarre parosteal osteochondromatous proliferation. J. Clin. Orthop. Trauma. 2012, 3, 119–121. [Google Scholar] [CrossRef] [Green Version]
- Martínez Álvarez, S.; Azorín Cuadrillero, D.L.; Little, K.J. Bizarre Parosteal Osteochondromatous Proliferation (Nora Lesion) in Pediatric Phalanges. J. Hand Surg. Am. 2021, 46, 344.e1–344.e9. [Google Scholar] [CrossRef]
- Suresh, S. Nora’s lesion of the second toe. Indian J. Orthop. 2010, 44, 342–344. [Google Scholar] [CrossRef] [PubMed]
- Schlur, C.; Bachy, M.; Wajfisz, A.; Ducou le Pointe, H.; Josset, P.; Vialle, R. Osteoid osteoma mimicking Brodie’s abscess in a 13-year-old girl. Pediatr. Int. 2013, 55, e29–e31. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, P.; Sobti, A. A Brodie’s Abscess of Femoral Neck Mimicking Osteoid Osteoma: Diagnostic Approach and Management Strategy. Ethiop. J. Health. Sci. 2016, 26, 81–84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanrıverdi, B.; Salık, A.E.; Çetingök, H.; Edipoğlu, E.; Bilgili, M.G.; Güven, K.; Saçan, F. Multidisciplinary approach in the treatment of osteoid osteoma with radiofrequency ablation. Jt. Dis. Relat. Surg. 2020, 31, 255–259. [Google Scholar] [CrossRef] [PubMed]
- Kuyumcu, G.; Ilaslan, H.; Sundaram, M.; Schils, J.P. Osteoid osteoma of the hand and foot in children successfully treated with radiofrequency neurotomy probes. Skelet. Radiol. 2017, 46, 1561–1565. [Google Scholar] [CrossRef]
- Michaelides, M.; Drakonaki, E.; Petridou, E.; Pantziara, M.; Ioannides, C. Osteoid osteoma of the scaphoid bone associated with flexor carpi radialis calcific tendinitis and treated with CT-guided RF ablation. Skelet. Radiol. 2018, 47, 1449–1453. [Google Scholar] [CrossRef]
- Rosenthal, D.I.; Hornicek, F.J.; Torriani, M.; Gebhardt, M.C.; Mankin, H.J. Osteoid osteoma: Percutaneous treatment with radiofrequency energy. Radiology 2003, 229, 171–175. [Google Scholar] [CrossRef]
- Franceschini, N.; Lam, S.W.; Cleton-Jansen, A.M.; Bovée, J.V. What’s new in bone forming tumours of the skeleton? Virchows Arch. 2020, 476, 147–157. [Google Scholar] [CrossRef] [Green Version]
- Amary, M.F.; Markert, E.; Berisha, F.; Ye, H.; Gerrand, C.; Cool, P.; Tirabosco, R.; Lindsay, D.; Pillay, N.; O’Donnell, P.; et al. FOS Expression in Osteoid Osteoma and Osteoblastoma: A Valuable Ancillary Diagnostic Tool. Am. J. Surg. Pathol. 2019, 43, 1661–1667. [Google Scholar] [CrossRef]
- Lam, S.W.; Cleven, A.H.G.; Kroon, H.M.; Bruijn, I.H.B.-D.; Szuhai, K.; Bovée, J.V.M.G. Utility of FOS as diagnostic marker for osteoid osteoma and osteoblastoma. Virchows Arch. 2020, 476, 455–463. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case Number | 1 | 2 | 3 | 4 | 5 | 6 |
|---|---|---|---|---|---|---|
| age/gender | 35/m | 27/m | 22/m | 27/m | 24/m | 29/m |
| side | left | right | left | left | right | left |
| bone | prox. phalanx | hamate | capitate | prox. phalanx | dist. phalanx | prox. phalanx |
| localization | intracortical | intracortical | juxta-articular | juxta-articular | intracortical | intracortical |
| time to diagnosis (months) | 62 | 7 | 18 | 12 | 12 | 12 |
| Detection OO in imaging Xray/CT/MRI | −/+/+ | −/+/− | +/+/+ | −/+/− | −/+/+ | +/+/+ |
| widest nidus diameter (mm) | 9 | 6 | 7 | 10 | 6 | 9 |
| pain/night pain/improvement due to NSAID | +/+/+ | +/+/− | +/+/+ | +/0/0 | +/+/+ | +/+/+ |
| swelling/deformity/motoric deficites | +/+/− | −/−/− | −/−/+ | +/+/+ | +/+/- | +/+/+ |
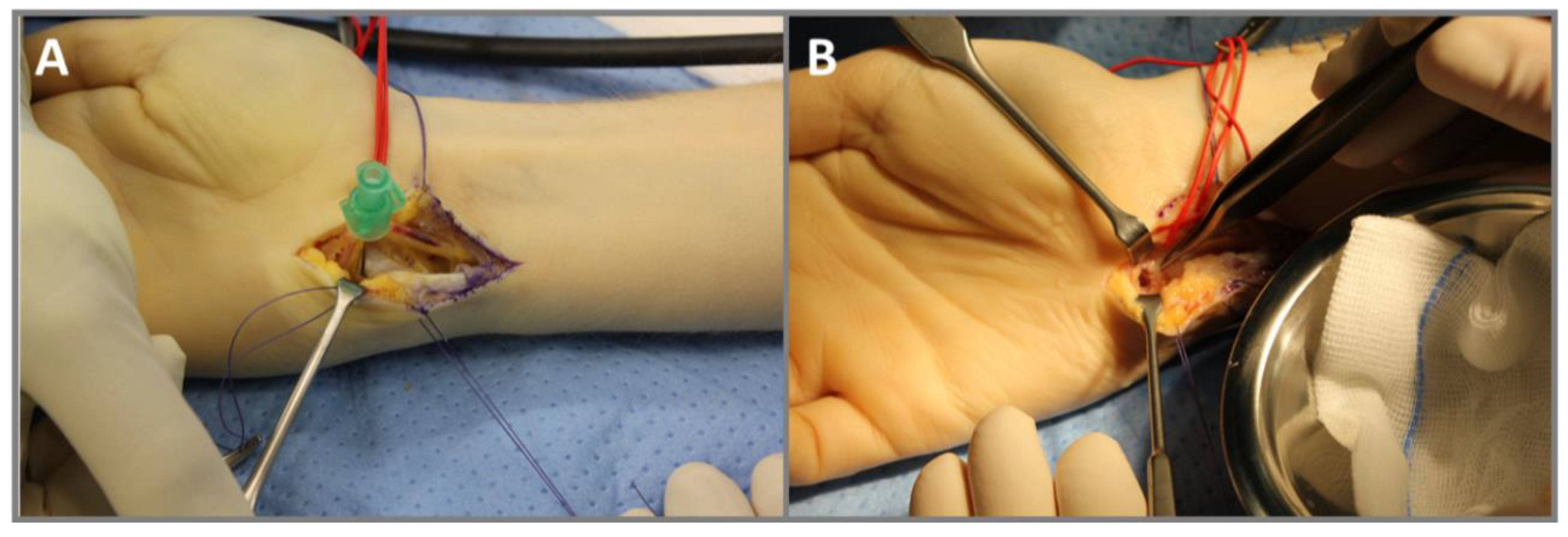
| treatment | en bloc | curretage | curretage | curretage | curretage | curretage |
| follow-up (months) | 78 | 4 | 14 | 16 | 16 | 4 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Meyer, J.; Priemel, M.; Rolvien, T.; Frosch, K.-H.; Schlickewei, C.; Yarar-Schlickewei, S. The Diagnostic Challenge of Osteoid Osteoma in the Bones of the Hand—A Case Series. Diagnostics 2023, 13, 1279. https://doi.org/10.3390/diagnostics13071279
Meyer J, Priemel M, Rolvien T, Frosch K-H, Schlickewei C, Yarar-Schlickewei S. The Diagnostic Challenge of Osteoid Osteoma in the Bones of the Hand—A Case Series. Diagnostics. 2023; 13(7):1279. https://doi.org/10.3390/diagnostics13071279
Chicago/Turabian StyleMeyer, Jasmin, Matthias Priemel, Tim Rolvien, Karl-Heinz Frosch, Carsten Schlickewei, and Sinef Yarar-Schlickewei. 2023. "The Diagnostic Challenge of Osteoid Osteoma in the Bones of the Hand—A Case Series" Diagnostics 13, no. 7: 1279. https://doi.org/10.3390/diagnostics13071279