
The Coexistence of Antibodies to Neuronal Cell and Synaptic Receptor Proteins, Gangliosides and Selected Neurotropic Pathogens in Neurologic Disorders in Children

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
4.1. Infectious Agents
4.2. ANA and ANCA
4.3. Antiganglioside Antibodies
4.4. Antineural Antibodies
4.5. Onconeural Antibodies
4.6. Anti-NMDAr Autoantibodies
4.7. Radiologic Findings
4.8. Electroencephalography
4.9. Place of Living
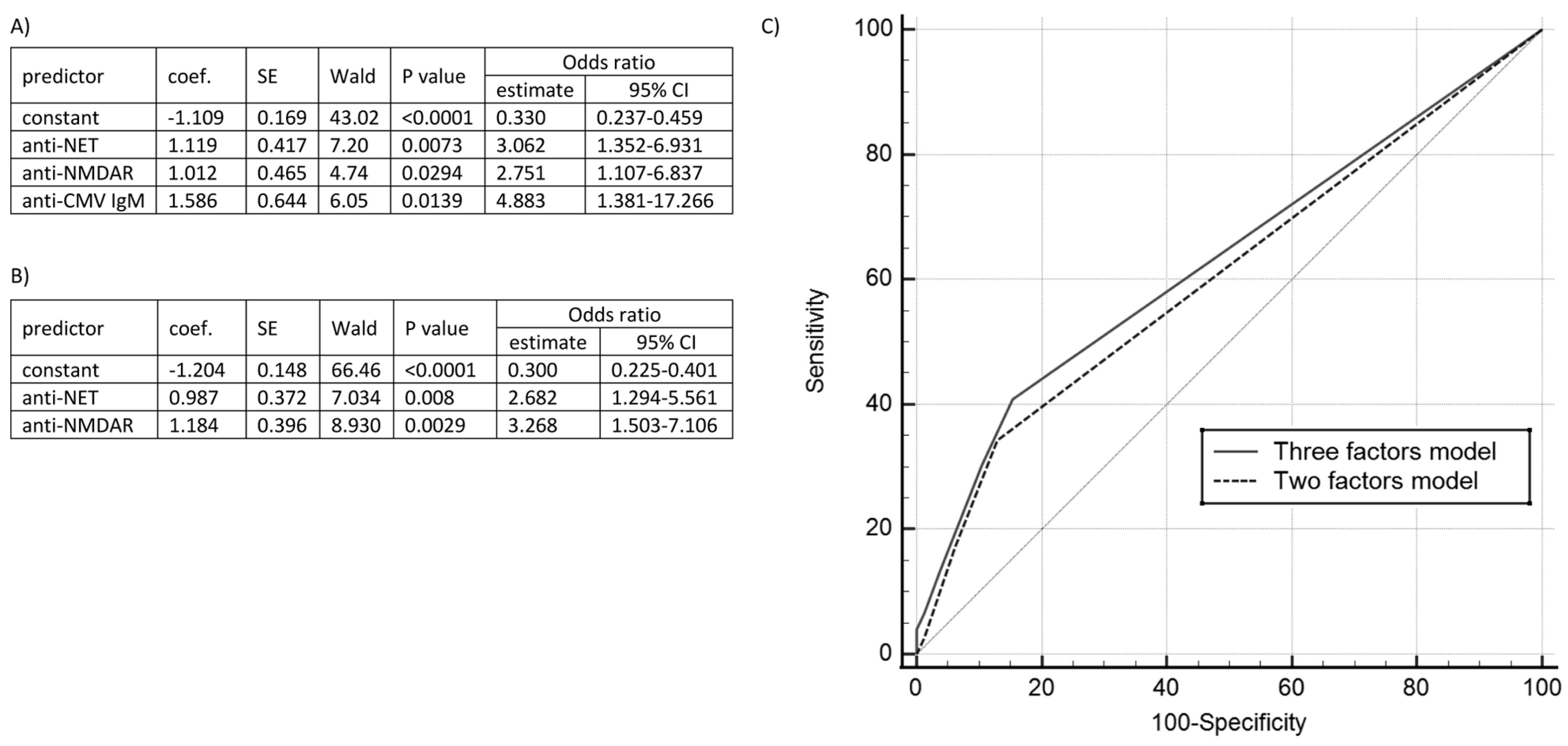
4.10. Logistic Regression Models
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zheng, J.; Shen, J.; Wang, A.; Liu, L.; Xiong, J.; Li, X.; Xiao, Y.; Li, J.; Mao, D.; Liu, L. Clinical Characteristics of Anti-N-Methyl-D-Aspartate Receptor Encephalitis in Children. Zhong Nan Da Xue Xue Bao Yi Xue Ban 2020, 45, 47–54. [Google Scholar] [CrossRef]
- Venkatesan, A.; Jagdish, B. Imaging in Encephalitis. Semin. Neurol. 2019, 39, 312–321. [Google Scholar] [CrossRef]
- Adam, P.; Táaborský, L.; Sobek, O.; Hildebrand, T.; Kelbich, P.; Průocha, M.; Hyánek, J. Cerebrospinal Fluid. In Advances in Clinical Chemistry; Elsevier: Amsterdam, The Netherlands, 2001; Volume 36, pp. 1–62. ISBN 978-0-12-010336-2. [Google Scholar]
- Dalmau, J.; Graus, F. Antibody-Mediated Encephalitis. N. Engl. J. Med. 2018, 378, 840–851. [Google Scholar] [CrossRef] [Green Version]
- Murphy, T.K.; Gerardi, D.M.; Leckman, J.F. Pediatric Acute-Onset Neuropsychiatric Syndrome. Psychiatr. Clin. N. Am. 2014, 37, 353–374. [Google Scholar] [CrossRef]
- Allen, A.J.; Leonard, H.L.; Swedo, S.E. Case Study: A New Infection-Triggered, Autoimmune Subtype of Pediatric OCD and Tourette’s Syndrome. J. Am. Acad. Child Adolesc. Psychiatry 1995, 34, 307–311. [Google Scholar] [CrossRef]
- Swedo, S.E.; Leonard, H.L.; Garvey, M.; Mittleman, B.; Allen, A.J.; Perlmutter, S.; Lougee, L.; Dow, S.; Zamkoff, J.; Dubbert, B.K. Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal Infections: Clinical Description of the First 50 Cases. Am. J. Psychiatry 1998, 155, 264–271. [Google Scholar] [CrossRef]
- Swedo, S.E.; Leckman, J.F.; Rose, N.R. From Research Subgroup to Clinical Syndrome: Modifying the PANDAS Criteria to Describe PANS (Pediatric Acute-Onset Neuropsychiatric Syndrome). Pediatr. Ther. 2012, 2, 113. [Google Scholar] [CrossRef]
- Mrozowska-Nyckowska, K.; Zbrzeźniak, J.; Paradowska-Stankiewicz, I. Meningitis and Encephalitis in Poland in 2020. Przegl. Epidemiol. 2022, 76, 371–384. [Google Scholar] [CrossRef]
- Figlerowicz, M.; Mazur-Melewska, K.; Kemnitz, P.; Mania, A. Pediatric Postviral Autoimmune Disorders of the CNS. Future Virol. 2020, 15, 307–315. [Google Scholar] [CrossRef]
- Yiş, U.; Kurul, S.H.; Çakmakçı, H.; Dirik, E. Mycoplasma Pneumoniae: Nervous System Complications in Childhood and Review of the Literature. Eur. J. Pediatr. 2008, 167, 973–978. [Google Scholar] [CrossRef]
- Lin, W.-C.; Lee, P.-I.; Lu, C.-Y.; Hsieh, Y.-C.; Lai, H.-P.; Lee, C.-Y.; Huang, L.-M. Mycoplasma Pneumoniae Encephalitis in Childhood. J. Microbiol. Immunol. Infect. Wei Mian Yu Gan Ran Za Zhi 2002, 35, 173–178. [Google Scholar]
- Salloum, S.; Goenka, A.; Ey, E. Mycoplasma Pneumoniae-Associated Transverse Myelitis Presenting as Asymmetric Flaccid Paralysis. Clin. Pract. 2019, 9, 75–77. [Google Scholar] [CrossRef] [Green Version]
- Fallon, B.A.; Keilp, J.; Prohovnik, I.; Heertum, R.V.; Mann, J.J. Regional Cerebral Blood Flow and Cognitive Deficits in Chronic Lyme Disease. J. Neuropsychiatry Clin. Neurosci. 2003, 15, 326–332. [Google Scholar] [CrossRef]
- Herbert, M.R.; Ziegler, D.A.; Deutsch, C.K.; O’Brien, L.M.; Lange, N.; Bakardjiev, A.; Hodgson, J.; Adrien, K.T.; Steele, S.; Makris, N.; et al. Dissociations of Cerebral Cortex, Subcortical and Cerebral White Matter Volumes in Autistic Boys. Brain 2003, 126, 1182–1192. [Google Scholar] [CrossRef] [Green Version]
- Bransfield, R.C.; Wulfman, J.S.; Harvey, W.T.; Usman, A.I. The Association between Tick-Borne Infections, Lyme Borreliosis and Autism Spectrum Disorders. Med. Hypotheses 2008, 70, 967–974. [Google Scholar] [CrossRef]
- Mazur-Melewska, K.; Breńska, I.; Jończyk-Potoczna, K.; Kemnitz, P.; Pieczonka-Ruszkowska, I.; Mania, A.; Służewski, W.; Figlerowicz, M. Neurologic Complications Caused by Epstein-Barr Virus in Pediatric Patients. J. Child Neurol. 2016, 31, 700–708. [Google Scholar] [CrossRef]
- Valayi, S.; Eftekharian, M.M.; Taheri, M.; Alikhani, M.Y. Evaluation of Antibodies to Cytomegalovirus and Epstein-Barr Virus in Patients with Autism Spectrum Disorder. Hum. Antibodies 2018, 26, 165–169. [Google Scholar] [CrossRef]
- Slawinski, B.L.; Talge, N.; Ingersoll, B.; Smith, A.; Glazier, A.; Kerver, J.; Paneth, N.; Racicot, K. Maternal Cytomegalovirus Sero-Positivity and Autism Symptoms in Children. Am. J. Reprod. Immunol. 2018, 79, e12840. [Google Scholar] [CrossRef]
- Mohammad, S.S.; Sinclair, K.; Pillai, S.; Merheb, V.; Aumann, T.D.; Gill, D.; Dale, R.C.; Brilot, F. Herpes Simplex Encephalitis Relapse with Chorea Is Associated with Autoantibodies to N-Methyl-D-Aspartate Receptor or Dopamine-2 Receptor. Mov. Disord. 2014, 29, 117–122. [Google Scholar] [CrossRef]
- Barbagallo, M.; Vitaliti, G.; Pavone, P.; Romano, C.; Lubrano, R.; Falsaperla, R. Pediatric Autoimmune Encephalitis. J. Pediatr. Neurosci. 2017, 12, 130–134. [Google Scholar] [CrossRef]
- Hilário, M.O.E.; Len, C.A.; Roja, S.C.; Terreri, M.T.; Almeida, G.; Andrade, L.E.C. Frequency of Antinuclear Antibodies in Healthy Children and Adolescents. Clin. Pediatr. 2004, 43, 637–642. [Google Scholar] [CrossRef]
- Mostafa, G.A.; El-Sherif, D.F.; Al-Ayadhi, L.Y. Systemic Auto-Antibodies in Children with Autism. J. Neuroimmunol. 2014, 272, 94–98. [Google Scholar] [CrossRef]
- Wanleenuwat, P.; Iwanowski, P.; Kozubski, W. Antiganglioside Antibodies in Neurological Diseases. J. Neurol. Sci. 2020, 408, 116576. [Google Scholar] [CrossRef]
- Antoine, J.-C.; Camdessanché, J.-P.; Ferraud, K.; Caudie, C. Antiganglioside Antibodies in Paraneoplastic Peripheral Neuropathies. J. Neurol. Neurosurg. Psychiatry 2004, 75, 1765–1767. [Google Scholar] [CrossRef] [Green Version]
- Kaida, K.; Ariga, T.; Yu, R.K. Antiganglioside Antibodies and Their Pathophysiological Effects on Guillain-Barre Syndrome and Related Disorders—A Review. Glycobiology 2009, 19, 676–692. [Google Scholar] [CrossRef] [Green Version]
- Koszewicz, M.; Michalak, S.; Bilinska, M.; Budrewicz, S.; Zaborowski, M.; Slotwinski, K.; Podemski, R.; Ejma, M. Is Peripheral Paraneoplastic Neurological Syndrome Possible in Primary Brain Tumors? Brain Behav. 2016, 6, e00465. [Google Scholar] [CrossRef] [Green Version]
- Michalak, S.; Gruszczyńska, A.; Popławska, K.; Żurawicz, P.; Kozubski, W. Clinical significance of anti-MAG, anti-myelin and anti-neuroendothelium antibodies. Neuroskop 2011, 13, 100–105. [Google Scholar]
- Tanaka, Y.; Tsukada, N.; Koh, C.-S.; Yanagisawa, N. Anti-Endothelial Cell Antibodies and Circulating Immune Complexes in the Sera of Patients with Multiple Sclerosis. J. Neuroimmunol. 1987, 17, 49–59. [Google Scholar] [CrossRef]
- Annunziata, P.; Cioni, C.; Moschini, F.; Riccucci, A.; Guazzi, G.C. Serum Anti-Brain Endothelium Antibodies and Cognitive Assessment in Patients with Binswanger’s Encephalopathy. J. Neurol. Sci. 1995, 128, 96–102. [Google Scholar] [CrossRef]
- Troxell, R.M.; Christy, A. Atypical Pediatric Demyelinating Diseases of the Central Nervous System. Curr. Neurol. Neurosci. Rep. 2019, 19, 95. [Google Scholar] [CrossRef]
- Li, J.; Xu, Y.; Ren, H.; Zhu, Y.; Peng, B.; Cui, L. Autoimmune GFAP Astrocytopathy after Viral Encephalitis: A Case Report. Mult. Scler. Relat. Disord. 2018, 21, 84–87. [Google Scholar] [CrossRef]
- Flanagan, E.P.; Hinson, S.R.; Lennon, V.A.; Fang, B.; Aksamit, A.J.; Morris, P.P.; Basal, E.; Honorat, J.A.; Alfugham, N.B.; Linnoila, J.J.; et al. Glial Fibrillary Acidic Protein Immunoglobulin G as Biomarker of Autoimmune Astrocytopathy: Analysis of 102 Patients: Autoimmune GFAP Astrocytopathy. Ann. Neurol. 2017, 81, 298–309. [Google Scholar] [CrossRef]
- Ambrosius, W.; Michalak, S.; Kozubski, W.; Kalinowska, A. Myelin Oligodendrocyte Glycoprotein Antibody-Associated Disease: Current Insights into the Disease Pathophysiology, Diagnosis and Management. Int. J. Mol. Sci. 2020, 22, 100. [Google Scholar] [CrossRef]
- López-Chiriboga, A.S.; Majed, M.; Fryer, J.; Dubey, D.; McKeon, A.; Flanagan, E.P.; Jitprapaikulsan, J.; Kothapalli, N.; Tillema, J.-M.; Chen, J.; et al. Association of MOG-IgG Serostatus With Relapse After Acute Disseminated Encephalomyelitis and Proposed Diagnostic Criteria for MOG-IgG–Associated Disorders. JAMA Neurol. 2018, 75, 1355–1363. [Google Scholar] [CrossRef] [Green Version]
- Sakamoto, Y.; Shimizu, T.; Tobisawa, S.; Isozaki, E. Chronic Demyelinating Neuropathy with Anti-Myelin-Associated Glycoprotein Antibody without Any Detectable M-Protein. Neurol. Sci. 2017, 38, 2165–2169. [Google Scholar] [CrossRef]
- Gövert, F.; Leypoldt, F.; Junker, R.; Wandinger, K.-P.; Deuschl, G.; Bhatia, K.P.; Balint, B. Antibody-Related Movement Disorders—A Comprehensive Review of Phenotype-Autoantibody Correlations and a Guide to Testing. Neurol. Res. Pract. 2020, 2, 6. [Google Scholar] [CrossRef] [Green Version]
- Kunstreich, M.; Kreth, J.H.; Oommen, P.T.; Schaper, J.; Karenfort, M.; Aktas, O.; Tibussek, D.; Distelmaier, F.; Borkhardt, A.; Kuhlen, M. Paraneoplastic Limbic Encephalitis with SOX1 and PCA2 Antibodies and Relapsing Neurological Symptoms in an Adolescent with Hodgkin Lymphoma. Eur. J. Paediatr. Neurol. 2017, 21, 661–665. [Google Scholar] [CrossRef]
- Dalmau, J.; Rosenfeld, M.R. Paraneoplastic Syndromes of the CNS. Lancet Neurol. 2008, 7, 327–340. [Google Scholar] [CrossRef] [Green Version]
- Donfrancesco, R.; Nativio, P.; Di Benedetto, A.; Villa, M.P.; Andriola, E.; Melegari, M.G.; Cipriano, E.; Di Trani, M. Anti-Yo Antibodies in Children With ADHD: First Results About Serum Cytokines. J. Atten. Disord. 2020, 24, 1497–1502. [Google Scholar] [CrossRef] [Green Version]
- Saiz, A.; Blanco, Y.; Sabater, L.; González, F.; Bataller, L.; Casamitjana, R.; Ramió-Torrentà, L.; Graus, F. Spectrum of Neurological Syndromes Associated with Glutamic Acid Decarboxylase Antibodies: Diagnostic Clues for This Association. Brain J. Neurol. 2008, 131, 2553–2563. [Google Scholar] [CrossRef] [Green Version]
- Lascano, A.M.; Vargas, M.I.; Lalive, P.H. Diagnostic Tools for Immune Causes of Encephalitis. Clin. Microbiol. Infect. 2019, 25, 431–436. [Google Scholar] [CrossRef] [Green Version]
- Guasp, M.; Módena, Y.; Armangue, T.; Dalmau, J.; Graus, F. Clinical Features of Seronegative, but CSF Antibody-Positive, Anti-NMDA Receptor Encephalitis. Neurol.-Neuroimmunol. Neuroinflamm. 2020, 7, e659. [Google Scholar] [CrossRef] [Green Version]
- Dalmau, J.; Tüzün, E.; Wu, H.; Masjuan, J.; Rossi, J.E.; Voloschin, A.; Baehring, J.M.; Shimazaki, H.; Koide, R.; King, D.; et al. Paraneoplastic Anti-N-Methyl-D-Aspartate Receptor Encephalitis Associated with Ovarian Teratoma. Ann. Neurol. 2007, 61, 25–36. [Google Scholar] [CrossRef] [Green Version]
- Jurek, B.; Chayka, M.; Kreye, J.; Lang, K.; Kraus, L.; Fidzinski, P.; Kornau, H.; Dao, L.; Wenke, N.K.; Long, M.; et al. Human Gestational N-methyl-d-aspartate Receptor Autoantibodies Impair Neonatal Murine Brain Function. Ann. Neurol. 2019, 86, 656–670. [Google Scholar] [CrossRef] [Green Version]
- Endres, D.; Maier, V.; Leypoldt, F.; Wandinger, K.-P.; Lennox, B.; Pollak, T.A.; Nickel, K.; Maier, S.; Feige, B.; Domschke, K.; et al. Autoantibody-Associated Psychiatric Syndromes: A Systematic Literature Review Resulting in 145 Cases. Psychol. Med. 2022, 52, 1135–1146. [Google Scholar] [CrossRef]
- Scheffer, I.E.; Berkovic, S.; Capovilla, G.; Connolly, M.B.; French, J.; Guilhoto, L.; Hirsch, E.; Jain, S.; Mathern, G.W.; Moshé, S.L.; et al. ILAE Classification of the Epilepsies: Position Paper of the ILAE Commission for Classification and Terminology. Epilepsia 2017, 58, 512–521. [Google Scholar] [CrossRef] [Green Version]
- Kotsopoulos, I.A.W.; Van Merode, T.; Kessels, F.G.H.; De Krom, M.C.T.F.M.; Knottnerus, J.A. Systematic Review and Meta-Analysis of Incidence Studies of Epilepsy and Unprovoked Seizures. Epilepsia 2002, 43, 1402–1409. [Google Scholar] [CrossRef]
- Attilakos, A.; Fotis, L.; Dinopoulos, A.; Alexopoulos, H.; Theofilopoulou, A.V.; Tzioufas, A.G.; Mastroyianni, S.; Karalexi, M.; Garoufi, A. Antiphospholipid and Antinuclear Antibodies in Children with Idiopathic Epilepsy: A 2-Year Prospective Study. J. Clin. Neurol. 2020, 16, 140–144. [Google Scholar] [CrossRef]
- Vassos, E.; Agerbo, E.; Mors, O.; Pedersen, C.B. Urban–Rural Differences in Incidence Rates of Psychiatric Disorders in Denmark. Br. J. Psychiatry 2016, 208, 435–440. [Google Scholar] [CrossRef]
- Chen, C.-Y.; Liu, C.-Y.; Su, W.-C.; Huang, S.-L.; Lin, K.-M. Factors Associated With the Diagnosis of Neurodevelopmental Disorders: A Population-Based Longitudinal Study. Pediatrics 2007, 119, e435–e443. [Google Scholar] [CrossRef]
- Hviid, A.; Melbye, M. The Epidemiology of Viral Meningitis Hospitalization in Childhood. Epidemiology 2007, 18, 695–701. [Google Scholar] [CrossRef] [PubMed]
- Dubey, D.; Pittock, S.J.; Kelly, C.R.; McKeon, A.; Lopez-Chiriboga, A.S.; Lennon, V.A.; Gadoth, A.; Smith, C.Y.; Bryant, S.C.; Klein, C.J.; et al. Autoimmune Encephalitis Epidemiology and a Comparison to Infectious Encephalitis: Autoimmune Encephalitis. Ann. Neurol. 2018, 83, 166–177. [Google Scholar] [CrossRef] [PubMed]
- Graus, F.; Vogrig, A.; Muñiz-Castrillo, S.; Antoine, J.-C.G.; Desestret, V.; Dubey, D.; Giometto, B.; Irani, S.R.; Joubert, B.; Leypoldt, F.; et al. Updated Diagnostic Criteria for Paraneoplastic Neurologic Syndromes. Neurol.—Neuroimmunol. Neuroinflamm. 2021, 8, e1014. [Google Scholar] [CrossRef] [PubMed]
- Lubarski, K.; Mania, A.; Michalak, S.; Osztynowicz, K.; Mazur-Melewska, K.; Figlerowicz, M. The Clinical Spectrum of Autoimmune-Mediated Neurological Diseases in Paediatric Population. Brain Sci. 2022, 12, 584. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| CNS Infections (n = 42) | PANDAS (n = 34) | Autoimmune and Demyelinating Diseases (n = 139) | PDD (n = 48) | Epilepsy (n = 88) | Other (n = 157) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| diagnosis | n | ass. symptoms | n | diagnosis | n | diagnosis | n | diagnosis | n | diagnosis | n |
| Neuroborreliosis | 4 | tics | 27 | Neuropathies | 44 | Autism | 37 | generalised idiopathic: | 58 | involuntary movements diagnostics | 41 |
| meningitis: | 12 | OCD | 10 | - GBS | 13 | Asperger syndrome | 3 | - tonic-clonic | 15 | headache | 22 |
| - HHV-7 | 2 | anxiety disorder | 3 | - mononeuropathies | 6 | Other PDD | 8 | - polymorphic | 11 | dissociative and emotional disorders | 21 |
| - HSV-1 + N. meningitidis | 1 | psychomotor delay | 4 | - CIDP | 5 | - absence | 8 | movement disorders | 11 | ||
| - Influenza A virus | 1 | seizures | 3 | - postinfectious neuropathies | 5 | - myoclonic | 8 | - tetraplegia | 1 | ||
| - unidentified agent | 8 | visual symptoms | 3 | - axonal neuropathy | 10 | - other generalised seizures | 16 | - dizziness, imbalance | 8 | ||
| encephalitis: | 12 | - other and undescribed | 5 | focal idiopathic: | 19 | - ataxia and gait impairment | 2 | ||||
| - VZV | 4 | CNS inflammation: | 44 | - with generalisation | 12 | neoplasms and paraneoplastic syndromes | 9 | ||||
| - HSV-1 | 2 | - encephalitis | 31 | - simple focal | 7 | - ALL | 3 | ||||
| - HHV-6 | 1 | - cerebellitis | 4 | symptomatic | 11 | - spinal tumour | 2 | ||||
| - Influenza A virus | 1 | - ADEM | 3 | - Neuroblastoma suspicion, OMS | 2 | ||||||
| - rotavirus | 1 | - encephalomyelitis | 2 | - brain stem tumour | 1 | ||||||
| - enterovirus | 1 | - encephalomeningitis | 1 | - thalamic tumour | 1 | ||||||
| - unidentified agent | 2 | - myelitis | 1 | psychomotor delay | 9 | ||||||
| cerebellitis and ataxia: | 5 | - acute demyelinating episode | 1 | vision disorders | 9 | ||||||
| - VZV | 1 | - Rasmussen syndrome | 1 | neuromuscular or muscular disease | 7 | ||||||
| - M. pneumoniae | 1 | Optic nerve inflammation | 7 | CNS diagnostics in systemic rheumatologic diseases | 6 | ||||||
| - unidentified agent | 3 | PANS | 7 | stroke or TIA | 5 | ||||||
| meningocerebellitis: | 2 | PITAND | 6 | other— differential diagnosis | 17 | ||||||
| - EBV | 1 | MS | 6 | - gastroenterological symptoms | 4 | ||||||
| - enterovirus | 1 | Myasthenia | 1 | - appendicitis | 1 | ||||||
| encephalomeningitis: | 3 | Other: | 24 | - MRI abnormalities | 4 | ||||||
| - S. pneumoniae | 1 | - CNS demyelination | 14 | - Idiopathic scoliosis | 1 | ||||||
| - unidentified agent | 2 | - involuntary movement disorder reactive to IVIG | 7 | - febrile seizures | 2 | ||||||
| panencephalitis | 1 | - progressive encephalopathy | 1 | - heat-illness | 1 | ||||||
| Cerebral toxocariasis | 1 | - MS diagnostics | 1 | - transient neurological symptoms | 2 | ||||||
| M. pneumoniae-induced: | 2 | - autoimmune mediated development delay suspicion | 1 | - respiratory abnormalities, dyspnoea | 1 | ||||||
| - tic disorder | 1 | - inborn error of metabolism suspicion | 1 | ||||||||
| - OMS | 1 | ||||||||||
| All (n = 508) Median (IQR) | CNS Infections (n = 42) Median (IQR) | PANDAS (n = 34) Median (IQR) | Autoimmune and Demyelinating Diseases (n = 139) Median (IQR) | PDD (n = 48) Median (IQR) | Epilepsy (n = 88) Median (IQR) | Other (n = 157) Median (IQR) | |
|---|---|---|---|---|---|---|---|
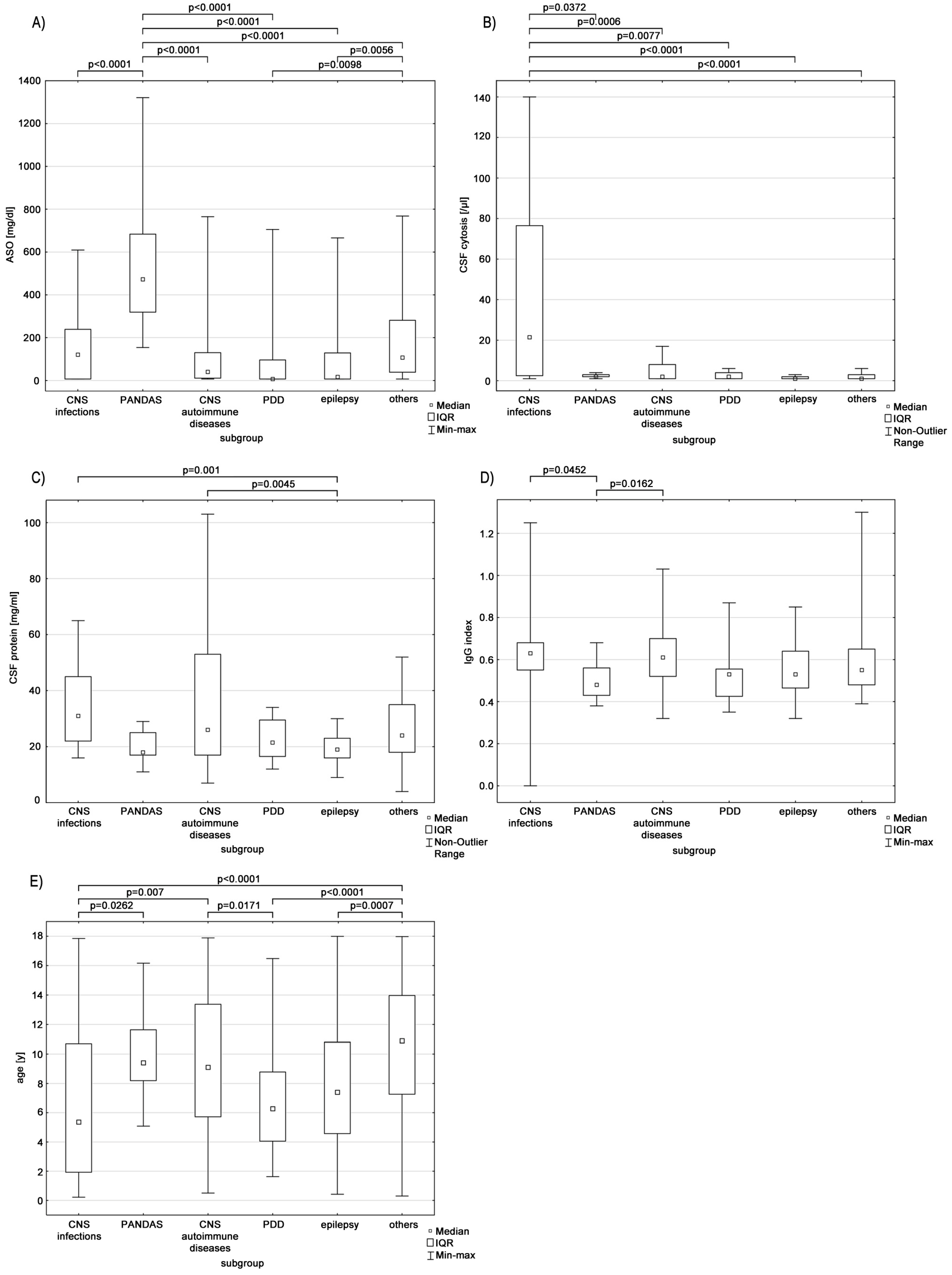
| age (y/a) | 8.9 (5.4–12.7) | 5.4 bcf (1.9–10.7) | 9.4 a (8.2–11.6) | 9.1 ad (5.7–13.4) | 6.3 cf (4.1–8.8) | 7.4 f (4.6–10.8) | 10.9 ade (7.3–14) |
| CSF protein (mg/dL) | 24 (17–38) | 31 e (22–45) | 18 (17–25) | 26 e (17–53) | 21.5 (16.5–29.5) | 19 ac (16–23) | 24 (18–35) |
| CSF cytosis (/µL) | 2 (1–6) | 22 bcdef (3–77) | 2 a (2–3) | 2 a (1–8) | 2 a (1–4) | 1 a (1–2) | 1 a (1–3) |
| IgG index | 0.57 (0.49–0.67) | 0.63 b (0.55–0.68) | 0.48 ac (0.43–0.56) | 0.61 b (0.52–0.70) | 0.53 (0.43–0.56) | 0.53 (0.47–0.64) | 0.55 (0.48–0.65) |
| ASO (IU/mL) | 74 (7–268) | 120.5 b (7–239) | 472.5 acdef (319–684) | 40 (11–130) | 7 bf (7–96) | 17 bf (7–129) | 107 bde (39–281) |
| Without Division n (%) | Subgroups | |||||||
|---|---|---|---|---|---|---|---|---|
| CNS Infections n (%) | PANDAS n (%) | Autoimmune and Demyelinating Diseases n (%) | PDD n (%) | Epilepsy n (%) | Other n (%) | |||
| sex | female | 215 (42.3) | 16 (38.1) | 6 (17.6) | 60 (43.2) | 12 (25) | 54 (61.4) * | 67 (42.7%) |
| male | 293 (57.7) | 26 (61.9) | 28 (82.4) * | 79 (56.8) | 36 (75) * | 34 (38.6) | 90 (57.3%) | |
| living place | rural | 208 (40.9) | 27 (64.3) * | 12 (35.3) | 57 (41) | 13 (27.1) | 35 (39.8) | 64 (40.8%) |
| urban | 300 (59.1) | 15 (35.7) | 22 (64.7) | 82 (59) | 35 (72.9) * | 53 (60.2) | 93 (59.2%) | |
| IgG index ≥0.75 | 43/216 (19.9%) | 6/27 (24) | 0/17 (0) ** | 23/93 (24.7) | 1/12 (8.3) | 3/20 (15) | 10/49 (20.4) | |
| anti-MAG Ab | 15/463 (3.2%) | 0/38 (0) | 3/32 (9.4) | 5/123 (4.1) | 0/45 (0) | 1/85 (1.2) | 6/140 (4.3) | |
| anti-myelin Ab | 27/463 (5.8%) | 4/38 (10.5) | 2/32 (6.3) | 8/123 (6.5) | 0/45 (0) | 5/85 (5.9) | 8/140 (5.7) | |
| anti-NET Ab | 46/463 (9.9%) | 1/38 (2.6) | 3/32 (9.4) | 19/123 (15.4) * | 4/45 (8.9) | 11/85 (12.9) | 8/140 (5.7) ** | |
| anti-GFAP Ab | 27/463 (5.8%) | 2/38 (5.3) | 4/32 (12.5) | 6/123 (4.9) | 4/45 (8.9) | 6/85 (7.1) | 5/140 (3.6) | |
| serum anti-NMDAr Ab | 32/343 (9.3%) | 1/32 (3.1) | 1/31 (3.2) | 18/95 (18.9) * | 3/32 (9.4) | 4/60 (6.7) | 5/93 (5.4) | |
| ANA | 114/310 (36.8%) | 10/24 (41.7) | 10/27 (37) | 36/93 (38.7) | 6/29 (20.7) | 18/45 (40) | 34/92 (37) | |
| MRI/CT lesions | 148/439 (33.7%) | 11/41 (26.8) | 7/28 (25) | 56/125 (44.8) * | 6/38 (15.8) | 28/80 (35) | 40/127 (31.5) | |
| Without Division n (%) | Subgroups | ||||||
|---|---|---|---|---|---|---|---|
| CNS Infections n (%) | PANDAS n (%) | Autoimmune and Demyelinating Diseases n (%) | PDD n (%) | Epilepsy n (%) | Other n (%) | ||
| anti-HSV-1 IgG Ab | 103/230 (44.8) | 11/32 (34.4) | 7/14 (50) | 40/84 (47.6) | 9/18 (50) | 16/38 (57.1) | 20/54 (37) |
| anti-HSV-1 IgM Ab | 8/226 (3.5) | 4/32 (12.5) * | 0/14 (0) | 3/85 (3.5) | 0/14 (0) | 1/28 (3.6) | 0/53 (0) |
| anti-HSV-2 IgG Ab | 8/229 (3.5) | 1/32 (3.1) | 1/13 (7.7) | 4/84 (4.8) | 0/18 (0) | 0/28 (0) | 2/54 (3.7) |
| anti-HSV-2 IgM Ab | 1/224 (0.4) | 0/32 (0) | 0/13 (0) | 1/85 (1.2) | 0/14 (0) | 0/28 (0) | 0/52 (0) |
| anti-VCA EBV IgG Ab | 222/367 (60.5) | 18/33 (54.5) | 14/24 (58.3) | 69/112 (61.6) | 20/37 (54.1) | 37/58 (63.8) | 64/103 (62.1) |
| anti-VCA EBV IgM Ab | 33/368 (9) | 3/33 (9.1) | 1/24 (4.2) | 13/112 (11.6) | 2/37 (5.4) | 5/59 (8.5) | 9/103 (8.7) |
| EBNA IgG Ab | 194/348 (55.7) | 15/31 (48.4) | 13/24 (54.2) | 58/104 (55.8) | 19/37 (51.4) | 32/55 (58.2) | 57/97 (58.8) |
| anti-CMV IgG Ab | 159/377 (42.2) | 5/33 (15.2) ** | 12/26 (46.2) | 44/99 (40.4) | 16/36 (44.4) | 30/62 (48.4) | 52/111 (46.8) |
| anti-CMV IgM Ab | 15/377 (4) | 0/33 (0) | 0/25 (0) | 10/108 (9.3)* | 0/36 (0) | 0/62 (0) | 5/113 (4.4) |
| anti-B. burgdorferi IgG Ab | 14/378 (3.7) | 2/34 (5.9) | 2/30 (6.7) | 7/118 (5.9) | 0/31 (0) | 1/55 (1.8) | 2/110 (1.8) |
| anti-B. burgdorferi IgM Ab | 30/380 (7.9) | 8/34 (23.5) * | 0/30 (0) | 11/119 (9.2) | 1/31 (3.2) | 2/56 (3.6) | 8/110 (7.3) |
| anti-M. pneumoniae IgG Ab | 74/366 (20.2) | 7/36 (19.4) | 8/28 (28.6) | 16/110 (14.5) | 2/30 (6.7) | 11/62 (17.7) | 30/100 (30) * |
| anti-M. pneumoniae IgM Ab | 17/368 (4.6) | 3/36 (8.3) | 1/28 (3.6) | 7/111 (6.3) | 0/31 (0) | 0/62 (0) | 6/100 (6) |
| anti-M. pneumoniae IgA Ab | 10/360 (2.8) | 1/35 (2.9) | 0/28 (0) | 3/109 (2.8) | 0/29 (0) | 1/62 (1.6) | 5/97 (5.2) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lubarski, K.; Mania, A.; Michalak, S.; Osztynowicz, K.; Mazur-Melewska, K.; Figlerowicz, M. The Coexistence of Antibodies to Neuronal Cell and Synaptic Receptor Proteins, Gangliosides and Selected Neurotropic Pathogens in Neurologic Disorders in Children. Diagnostics 2023, 13, 1274. https://doi.org/10.3390/diagnostics13071274
Lubarski K, Mania A, Michalak S, Osztynowicz K, Mazur-Melewska K, Figlerowicz M. The Coexistence of Antibodies to Neuronal Cell and Synaptic Receptor Proteins, Gangliosides and Selected Neurotropic Pathogens in Neurologic Disorders in Children. Diagnostics. 2023; 13(7):1274. https://doi.org/10.3390/diagnostics13071274
Chicago/Turabian StyleLubarski, Karol, Anna Mania, Sławomir Michalak, Krystyna Osztynowicz, Katarzyna Mazur-Melewska, and Magdalena Figlerowicz. 2023. "The Coexistence of Antibodies to Neuronal Cell and Synaptic Receptor Proteins, Gangliosides and Selected Neurotropic Pathogens in Neurologic Disorders in Children" Diagnostics 13, no. 7: 1274. https://doi.org/10.3390/diagnostics13071274