
Idiopathic Pulmonary Hemorrhage in Infancy: A Case Report and Literature Review
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Autopsy Case Report
2.1. Clinical Presentation
2.2. Postmortem Examination
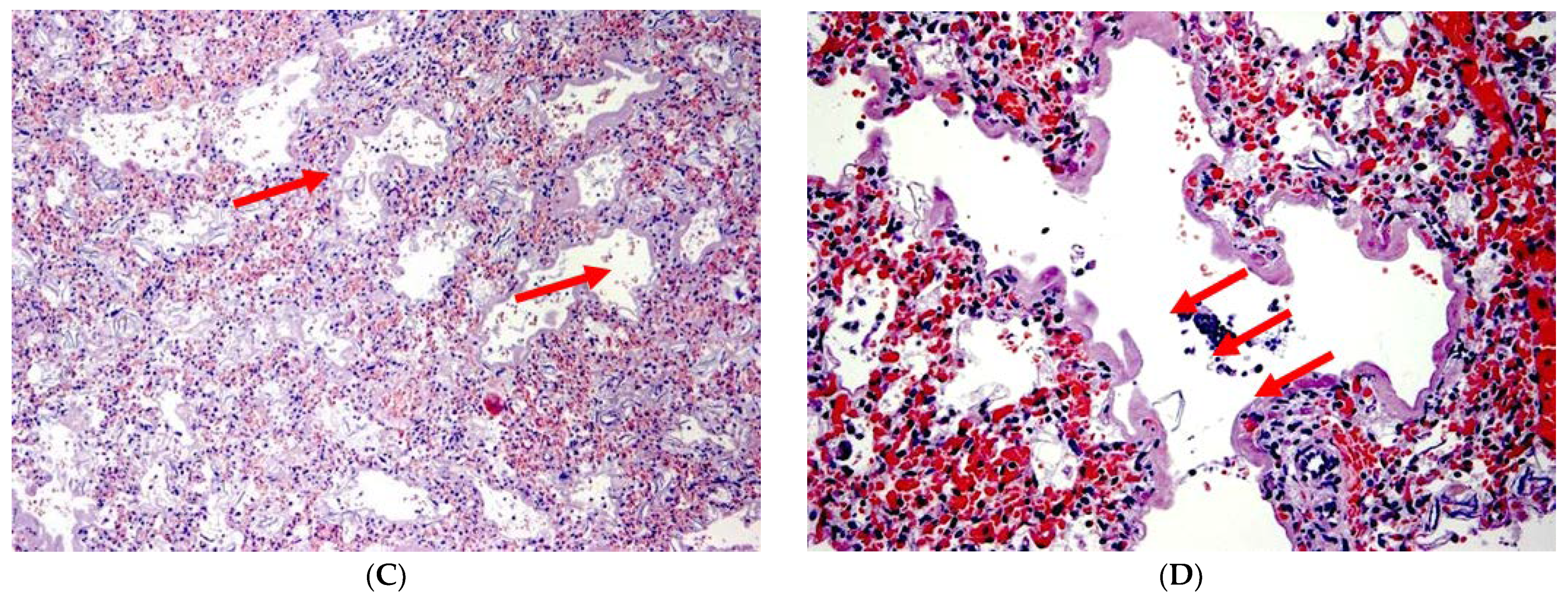
2.3. Histological Evaluation
3. Literature Review
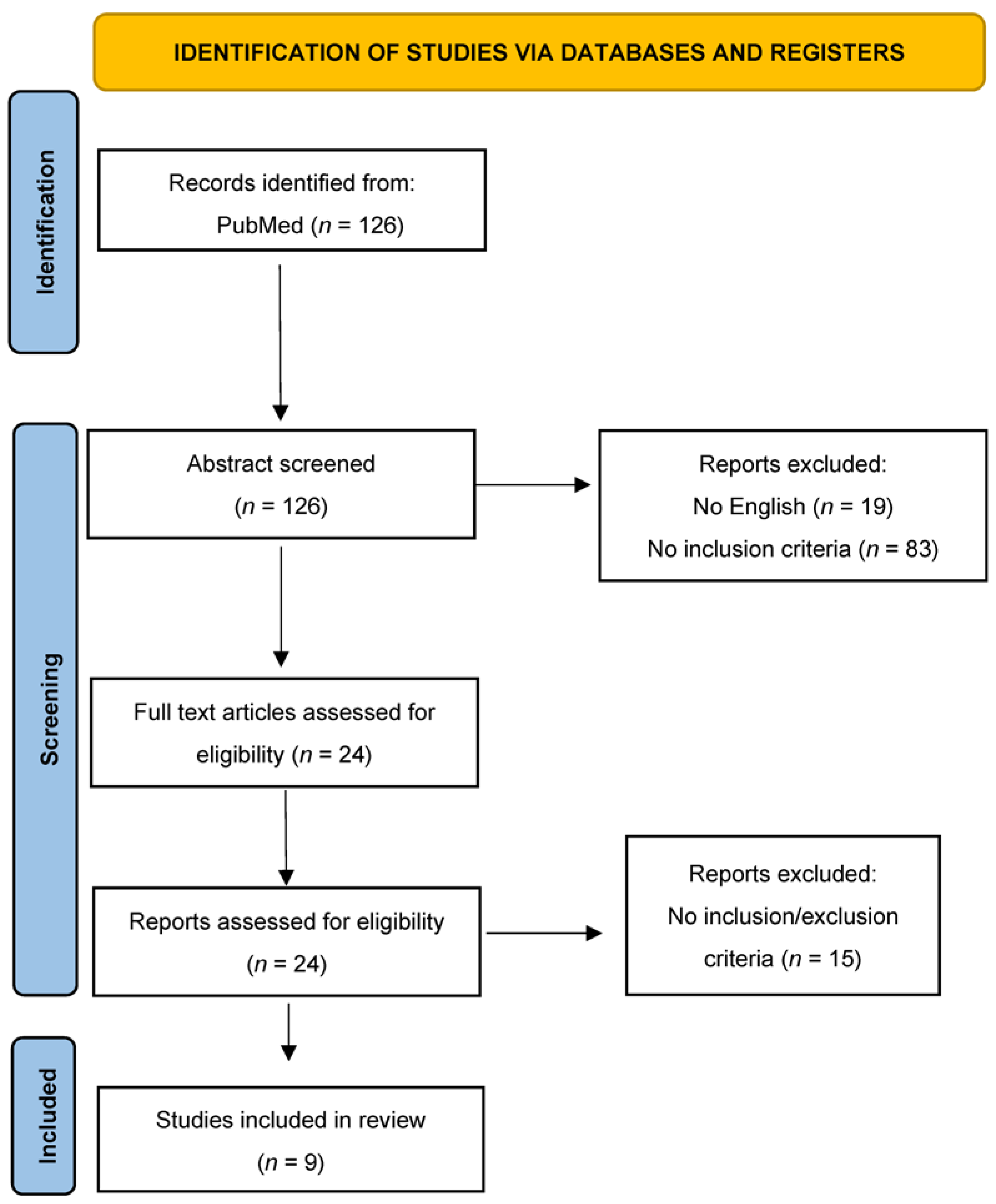
3.1. Materials and Methods
3.2. Results
3.2.1. General Presentation and Clinical Manifestation of AIPHI
3.2.2. Instrumental Analysis and Laboratory Count (When Reported)
3.2.3. Autopsy Data
4. Discussion
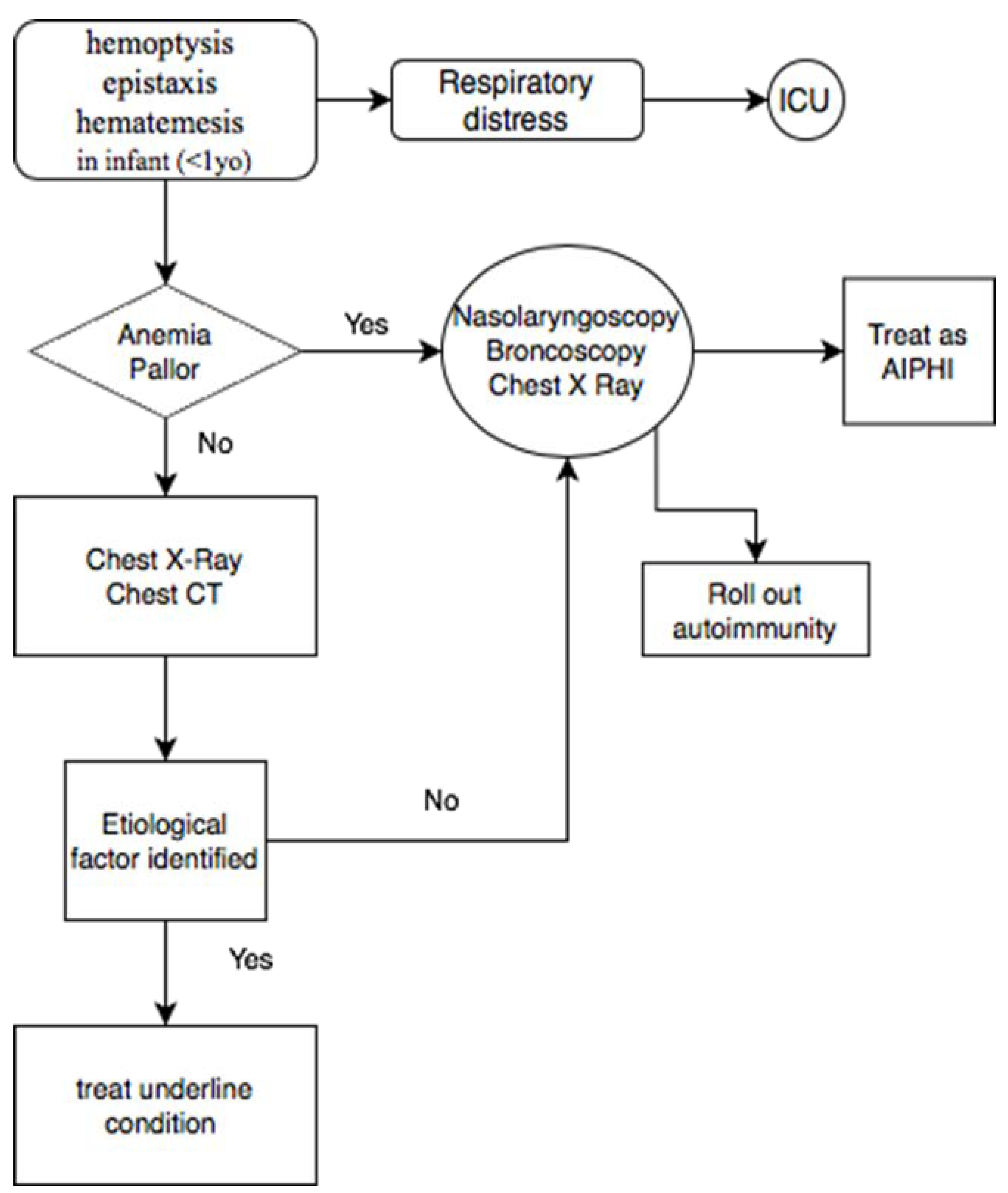
- Previously healthy infant aged <1 year with a gestational age of >32 weeks.
- Abrupt or sudden onset of overt bleeding or obvious evidence of blood in the airway.
- Severe-appearing illness leading to acute respiratory distress or respiratory failure, resulting in hospitalization in a pediatric intensive care unit (PICU) or neonatal intensive care unit (NICU) with intubation and mechanical ventilation.
- Diffuse unilateral or bilateral pulmonary infiltrates visible on CXR or computerized tomography (CT) [33].
- Increased weight of the lungs;
- Interstitial and endoalveolar hemorrhage with a diffuse or nodular pattern;
- Presence of endoalveolar hyaline membranes; (not necessary but possibly found)
- Accumulation of macrophages, siderophages, and hemosiderin as markers of previous bleeding; (not necessary, but possibly found);
- Absence of underlining conditions;
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Welde, M.A.; Sanford, C.B.; Mangum, M.; Paschal, C.; Jnah, A.J. Pulmonary Hemorrhage in the Neonate. Neonatal Netw. 2021, 40, 295–304. [Google Scholar] [CrossRef] [PubMed]
- Barnes, M.E.; Feeney, E.; Duncan, A.; Jassim, S.; MacNamara, H.; O’Hara, J.; Refila, B.; Allen, J.; McCollum, D.; Meehan, J.; et al. Pulmonary haemorrhage in neonates: Systematic review of management. Acta Paediatr. 2021, 111, 236–244. [Google Scholar] [CrossRef] [PubMed]
- Krous, H.F.; Chadwick, A.E.; Haas, E.A.; Stanley, C. Pulmonary intra-alveolar hemorrhage in SIDS and suffocation. J. Forensic Leg. Med. 2007, 14, 461–470. [Google Scholar] [CrossRef]
- Kher, P. Hemorrhagic Disease of Newborn. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK558994/ (accessed on 1 February 2022).
- Pramanik, A.K.; Rangaswamy, N.; Gates, T. Neonatal Respiratory Distress. Pediatr. Clin. N. Am. 2015, 62, 453–469. [Google Scholar] [CrossRef] [PubMed]
- Rocha, G.; Soares, P.; Gonçalves, A.; Silva, A.I.; Almeida, D.; Figueiredo, S.; Pissarra, S.; Costa, S.; Soares, H.; Flôr-De-Lima, F.; et al. Respiratory Care for the Ventilated Neonate. Can. Respir. J. 2018, 2018, 7472964. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reuter, S.; Moser, C.; Baack, M. Respiratory Distress in the Newborn. Pediatr. Rev. 2014, 35, 417–429. [Google Scholar] [CrossRef]
- Polin, R.A.; Carlo, W.A.; Papile, L.-A.; Tan, R.; Kumar, P.; Benitz, W.; Eichenwald, E.; Cummings, J.; Baley, J. Surfactant Replacement Therapy for Preterm and Term Neonates with Respiratory Distress. Pediatrics 2014, 133, 156–163. [Google Scholar] [CrossRef] [Green Version]
- Control, C.D. Prevention (CDC) Acute pulmonary hemorrhage/hemosiderosis among infants—Cleveland, January 1993-November 1994. Morb. Mortal. Wkly. Rep. 1994, 43, 881–883. [Google Scholar]
- CDC. Update: Pulmonary Hemorrhage in Infants. JAMA 2001, 286, 786. [Google Scholar] [CrossRef]
- Zahr, R.A.; Ashfaq, A.; Marron-Corwin, M. Neonatal Pulmonary Hemorrhage. Neoreviews 2012, 13, e302–e306. [Google Scholar] [CrossRef] [Green Version]
- Hanzlick, R. Pulmonary Hemorrhage in Deceased Infants. Am. J. Forensic Med. Pathol. 2001, 22, 188–192. [Google Scholar] [CrossRef]
- Coffin, C.M.; Schechtman, K.; Cole, F.S.; Dehner, L.P. Neonatal and Infantile Pulmonary Hemorrhage: An Autopsy Study with Clinical Correlation. Fetal Pediatr. Pathol. 1993, 13, 583–589. [Google Scholar] [CrossRef]
- Khong, T.Y.; Mooney, E.E.; Ariel, I.; Balmus, N.C.M.; Boyd, T.K.; Brundler, M.-A.; Derricott, H.; Evans, M.J.; Faye-Petersen, O.M.; Gillan, J.E.; et al. Sampling and Definitions of Placental Lesions: Amsterdam Placental Workshop Group Consensus Statement. Arch. Pathol. Lab. Med. 2016, 140, 698–713. [Google Scholar] [CrossRef] [Green Version]
- Fisk, N.; Berry, J.; Jeffrey, I.; Macintosh, M.; Walkinshaw, S.; Sinha, S.; Gawith, A.; Fitchett, M. The Royal College of Obstetricians and Gynaecologists and the Royal College of Pathologists. In Fetal and Perinatal Pathology: Report of a Joint Working Party; RCOG Press: London, UK, 2001. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. PLoS Med. 2021, 18, e1003583. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention (CDC). Acute pulmonary hemorrhage among infants: Chicago, April 1992 to November 1994. MMWR 1995, 44, 67–74. [Google Scholar]
- Pappas, M.D.; Samaik, A.P.; Meert, K.L.; Hasan, R.A.; Lieh-Lai, M.W. selected reports Idiopathic Pulmonary Hemorrhage in Infancy* Clinical Features and Management With High Frequency Ventilation. Chest 1996, 110, 553–555. [Google Scholar] [CrossRef] [PubMed]
- Dearborn, D.G.; Yike, I.; Sorenson, W.G.; Miller, M.J.; Etzei, R.A. Overview of Investigations into Pulmonary Hemorrhage among Infants in Cleveland, Ohio. Environ. Health Perspect. 1999, 107, 495–499. [Google Scholar] [CrossRef] [Green Version]
- Dearborn, D.G. Pulmonary hemorrhage in infants and children. Curr. Opin. Pediatr. 1997, 9, 219–224. [Google Scholar] [CrossRef] [PubMed]
- Vesper, S.J.; Dearborn, D.G.; Yike, I.; Sorenson, W.G.; Haugland, R.A. Hemolysis, Toxicity, and Randomly Amplified Polymorphic DNA Analysis of Stachybotrys chartarum Strains. Appl. Environ. Microbiol. 1999, 65, 3175–3181. [Google Scholar] [CrossRef] [Green Version]
- Saeed, M.M.; Woo, M.S.; Maclaughlin, E.F.; Margetis, M.F.; Keens, T.G. Prognosis in Pediatric Idiopathic Pulmonary Hemosiderosis. Chest 1999, 116, 721–725. [Google Scholar] [CrossRef]
- Chavez, H.; Gomara, R.E.; Plouff, R. A 4-week-old infant with idiopathic pulmonary hemorrhage. Pediatr. Emerg. Care 2000, 16, 42–44. [Google Scholar] [CrossRef]
- Novotny, W.E.; Dixit, A. Pulmonary Hemorrhage in an Infant Following 2 Weeks of Fungal Exposure. Arch. Pediatr. Adolesc. Med. 2000, 154, 271–275. [Google Scholar] [CrossRef] [Green Version]
- Al-Tamemi, S.; Al-Kindi, H. Acute Idiopathic Pulmonary Haemorrhage in a 2 month old Infant Case report and review of the literature. Sultan Qaboos Univ. Med J. 2009, 9, 170–174. [Google Scholar]
- Gutierrez, S.; Shaw, S.; Huseni, S.; Sachdeva, S.; Costello, J.P.; Basu, S.; Nath, D.S.; Klugman, D. Extracorporeal life support for a 5-week-old infant with idiopathic pulmonary hemosiderosis. Eur. J. Pediatr. 2014, 173, 1573–1576. [Google Scholar] [CrossRef] [PubMed]
- Welsh, S.K.; Casey, A.M.; Fishman, M.P. Pulmonary hemorrhage in infancy: A 10-year single-center experience. Pediatr. Pulmonol. 2018, 53, 1559–1564. [Google Scholar] [CrossRef]
- Sato, Y.; Shiota, M.; Sasaki, K.; Hata, A.; Hata, D. Early therapy with corticosteroid and surfactant for acute idiopathic pulmonary hemorrhage in infants: Two case reports. Medicine 2020, 99, e20281. [Google Scholar] [CrossRef]
- Masoumi, H.; Chadwick, A.E.; Haas, E.A.; Stanley, C.; Krous, H.F. Unclassified sudden infant death associated with pulmonary intra-alveolar hemosiderosis and hemorrhage. J. Forensic Leg. Med. 2007, 14, 471–474. [Google Scholar] [CrossRef] [PubMed]
- Homer, R.J. Depositional diseases of the lungs. In Fishman’s Pulmonary Diseases and Disorders; Grippi, M.A., Ed.; McGraw-Hill Medical: New York, NY, USA, 2015. [Google Scholar]
- Leatherman, J.W.; Davies, S.F.; Hoidal, J.R. Alveolar hemorrhage syndromes: Diffuse microvascular lung hemorrhage in immune and idiopathic disorders. Medicine 1984, 63, 343–361. [Google Scholar] [CrossRef] [PubMed]
- In, T.J.T.; Ludwig, S. (Eds.) Textbook of Pediatric Emergency Medicine, 3rd ed.; Williams & Wilkins: Baltimore, MD, USA, 1993; pp. 1336–1362. [Google Scholar]
- Brown, C.M.; Redd, S.C.; Damon, S.A.; Control, C.D. Prevention (CDC) Acute idiopathic pulmonary hemorrhage among infants. Recommendations from the Working Group for Investigation and Surveillance. MMWR Recomm. Rep. 2004, 53, 1–12. [Google Scholar]
- Fracasso, T.; Vennemann, M.; Klöcker, M.; Bajanowski, T.; Brinkmann, B.; Pfeiffer, H. Petechial bleedings in sudden infant death. Int. J. Leg. Med. 2011, 125, 205–210. [Google Scholar] [CrossRef]
- Maiese, A.; Del Duca, F.; Santoro, P.; Pellegrini, L.; De Matteis, A.; La Russa, R.; Frati, P.; Fineschi, V. An Overview on Actual Knowledge About Immunohistochemical and Molecular Features of Vitality, Focusing on the Growing Evidence and Analysis to Distinguish Between Suicidal and Simulated Hanging. Front. Med. 2022, 8, 2925. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, I.; Ernst, L.M. Perinatal Pulmonary Hemorrhage: A Retrospective Autopsy Case Series. Pediatr. Dev. Pathol. 2020, 23, 267–273. [Google Scholar] [CrossRef] [PubMed]
- Wigglesworth, J.S.; Desai, R.; Guerrini, P. Fetal lung hypoplasia: Biochemical and structural variations and their possible significance. Arch. Dis. Child. 1981, 56, 606–615. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gitto, L.; Serinelli, S.; Busardò, F.P.; Panebianco, V.; Bolino, G.; Maiese, A. Can post-mortem computed tomography be considered an alternative for autopsy in deaths due to hemopericardium? J Geriatr Cardiol. 2014, 11, 363–367. [Google Scholar] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n. (Patient) | Reference | Age | Sex | Vital Parameters and Condition at Hospital | Onset Symptoms | Exposure | Other |
|---|---|---|---|---|---|---|---|
| 7 | Chicago Cluster (1992–1994) [17] | 3.0 (0.8–8) m | 4/7 M | Respiratory distress | 4/7 hemoptysis 2/7 epistaxis 1/7 blood leaking from the endotracheal tube | N/A | N/A |
| 6 | Pappas et al. (1996) [18] | Mean 2.3 m (0.9–6) | M | No fever, hypoxemia, respiratory acidosis | One previous infant seizure. 5/6 hemoptysis/hematemesis 1/6 epistaxis | N/A | Transfusion |
| 37 | Dearborn et al. (1999) [19,20,21] Cleveland Cluster | Mean 3.1 m | 9 M 28 F | Tachypnea 30/37 respiratory distress | Acute onset with hemoptysis (18/24), lethargy, respiratory distress, apnea, bradycardia, seizures | 10/37 tobacco smoke exposure 65% Stachybotrys chartarum in patient’s home | 30/37 ventilator support 27/37 transfusion |
| 1 | Saeed et al. (1999) [22] | 7.2 m | F | Not reported | Hemoptysis | N/A | Early prednisone |
| 1 | Chavez et al. (2000) [23] | 27 d | M | Tachypneic, tachycardic (163 bpm), SpO2 79%—O2 therapy with 10 l/min | Hemoptysis, blood leaking from the endotracheal tube | None | Early antibiotics |
| 1 | Novotny et al. (2000) [24] | 40 d | M | Tachypnea (58/min) and respiratory distress SpO2 76%, no fever, PaCO2 of 46 mm Hg, pH, 7.19, and PaO2, 74 mmHg on oxygen therapy | Blood leaking, suctioned from the mouth and posterior pharynx, subcostal retractions, pallor | Acute exposure to environmental tobacco smoke, fungal exposure, Penicillium—Trichoderma | Ampicillin and cefotaxime sodium |
| 1 | Al-Tamemi et al. (2009) [25] | 34 w | M | Shallow breathing, SpO2 84%, bilateral diffuse crackles, respiratory failure, severe metabolic acidosis, and low pCO2 due to hyperventilation | Unresponsive, face and clothing covered with blood | None | Broad-spectrum antibiotics |
| 1 | Gutierrez et al. (2014) [26] | 5 w | M | Respiratory distress, tachycardic and tachypneic | Hematemesis | Not reported | Ceftriaxone Venovenous (VV) extracorporeal membrane oxygenation (ECMO) |
| 4 | Welsh et al. (2018) [27] | 78 d | M | Respiratory distress | Hemoptysis | N/A | N/A |
| 32 d | M | N/A | Hemoptysis | ||||
| 36 d | M | Respiratory distress | N/A | ||||
| 38 d | M | Respiratory distress | Hemoptysis | ||||
| 1 m | F | Hemodynamic Shock | Epistaxis Blood leaking from the endotracheal tube | Not reported | Methylprednisolone surfactant antibiotics |
| Reference | Laboratory Data | Instrumental Analysis | Other |
|---|---|---|---|
| Chicago Cluster (1992–1994) [17] | Not reported | Chest X-ray: bilateral infiltrates | Cultures of blood and urine specimens: negative for bacterial, mycotic, and viral pathogens Bronchoscopy: no source of bleeding |
| Pappas et al. (1996) [18] | Mean Hb 9.8 g/dL (range 7.3–14.7 g/dL) Platelets normal | Chest X-ray: Bilateral infiltrates Echocardiographic evaluation: normal myocardial contractility in all patients | Endotracheal aspirate for hemosiderin-laden macrophages: negative Serum cow’s milk precipitins: negative |
| Dearborn et al. (1999) [19,20,21] Cleveland Cluster | Not reported | Not reported | Bronchoscopy (22/37): hemosiderosis and chronic bleeding >6 months |
| Saeed et al. (1999) [22] | N/A | Chest X-ray: pulmonary infiltrates | N/A |
| Chavez et al. (2000) [23] | WBC 15.9 × 106/mL (53% lymphocytes, 11% monocytes, 28% neutrophils) Platelet 256 × 106/mL | Chest X-ray: bilateral hyperinflation, haziness in the upper lobe and lingula Normal lung perfusion scan | Immunoglobulin panel negative Complement panels negative Viral, bacterial, and fungal cultures negative ANA negative |
| Novotny et al. (2000) [24] | WBC 16 × 106/mL Hb 12.3 g/dL Hematocrit 36% Platelet 624 × 106/mL | Chest X-ray: diffuse bilateral alveolar infiltrates Skeletal survey: no trauma Echocardiogram: negative | Bronchial lavage fluid: hemosiderin and macrophages Antiglomerular basement membrane antibody: negative Antistreptolysin antibody level: normal |
| Al-Tamemi et al. (2009) [25] | Leukocytosis with WBC 22.8 × 106/mL Lymphocytosis [×106/mL] Neutrophil [×106/mL] Platelets 555 × 106/mL Hemoglobin 9.8 g/dL | Chest X-ray: bilateral ground glass appearance Computed tomography (CT) scan: bilateral alveolar opacities | Blood, sputum, urine, and stool cultures: negative Gastric aspirate: negative for hemosiderine |
| Gutierrez et al. (2014) [26] | Not reported | Chest X-ray: dense consolidation throughout the right lung and left lower lobe Echocardiogram: atrial fibrillation | N/A |
| Welsh et al. (2018) [27] | Not reported | 4/4 Chest X-ray and CT not reported | 3/4 flexible bronchoscopy: hemosiderin-laden macrophages |
| Sato et al. (2020) [28] | WBC 35.6 × 106/mL Hb 11.8 g/dL | Chest X-ray: diffuse ground glass opacification of the left lung Echocardiogram: mild pulmonary hypertension but no congenital cardiac malformation Computed tomography (CT) scan: consolidation in the left upper and lower lobes | |
| Worsening anemia | Chest X-ray: widespread ground glass opacification of the bilateral lungs Echocardiogram: negative Computed tomography (CT) scan: consolidation with air bronchogram in both lungs | Coagulation tests: normal |
| N. Cases | Reference | Age | Pulmonary Score (Mean) | Siderophages | Hemorrhage Localization (Lung) |
|---|---|---|---|---|---|
| 1 | Hanzlick et al. (2001) [12] | N/A | 3 | 1/1 | Alveolar and interstitial—Nodular |
| 6 | Masoumi et al. (2007) [29] | 9 m | 3 | 1/6 | Alveolar—Nodular and diffuse |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Del Duca, F.; Maiese, A.; Spina, F.; Visi, G.; La Russa, R.; Santoro, P.; Pignotti, M.S.; Frati, P.; Fineschi, V. Idiopathic Pulmonary Hemorrhage in Infancy: A Case Report and Literature Review. Diagnostics 2023, 13, 1270. https://doi.org/10.3390/diagnostics13071270
Del Duca F, Maiese A, Spina F, Visi G, La Russa R, Santoro P, Pignotti MS, Frati P, Fineschi V. Idiopathic Pulmonary Hemorrhage in Infancy: A Case Report and Literature Review. Diagnostics. 2023; 13(7):1270. https://doi.org/10.3390/diagnostics13071270
Chicago/Turabian StyleDel Duca, Fabio, Aniello Maiese, Federica Spina, Giacomo Visi, Raffaele La Russa, Paola Santoro, Maria Serenella Pignotti, Paola Frati, and Vittorio Fineschi. 2023. "Idiopathic Pulmonary Hemorrhage in Infancy: A Case Report and Literature Review" Diagnostics 13, no. 7: 1270. https://doi.org/10.3390/diagnostics13071270