
Joint Methodology Based on Optical Densitometry and Dynamic Light Scattering for Liver Function Assessment

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
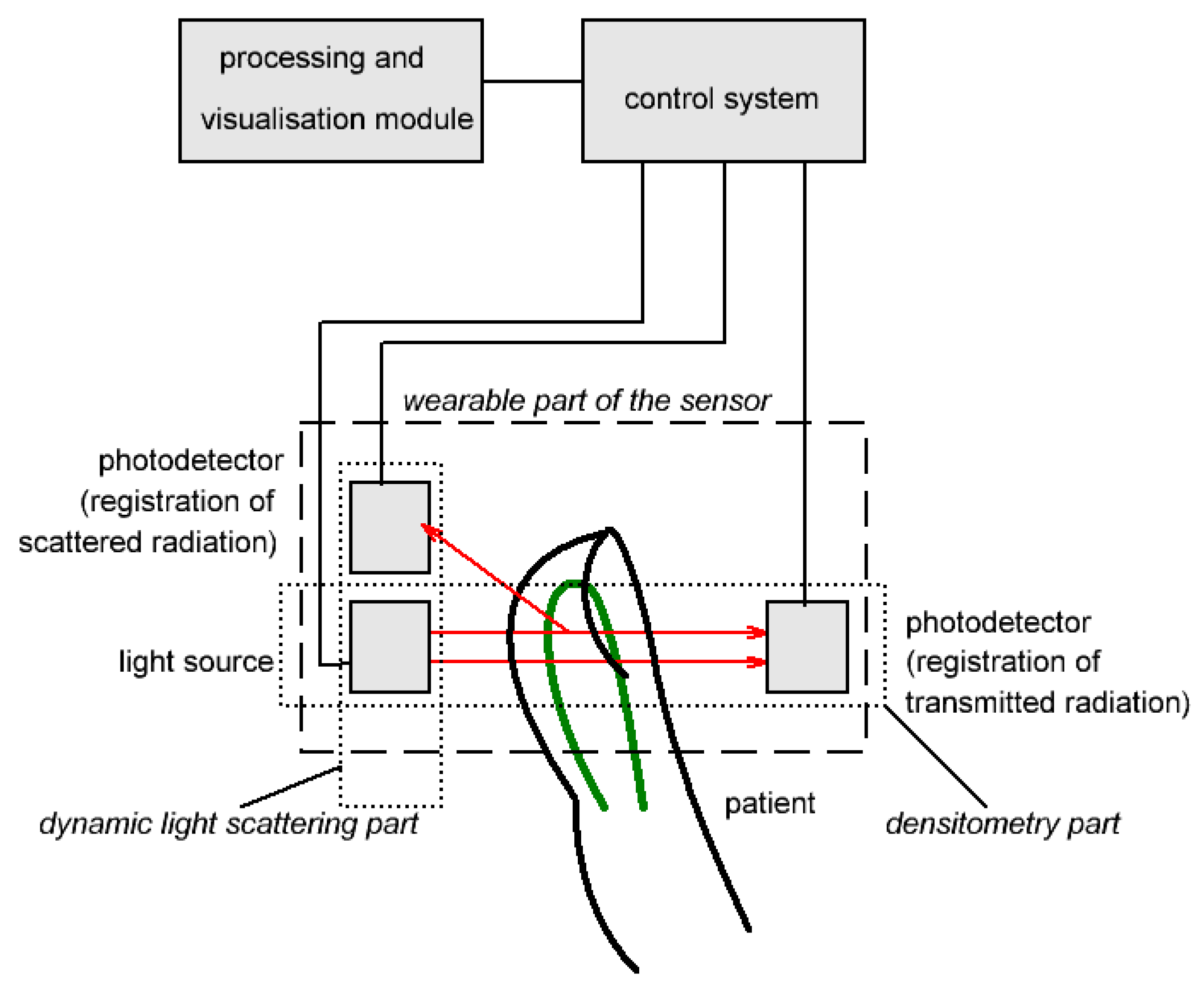
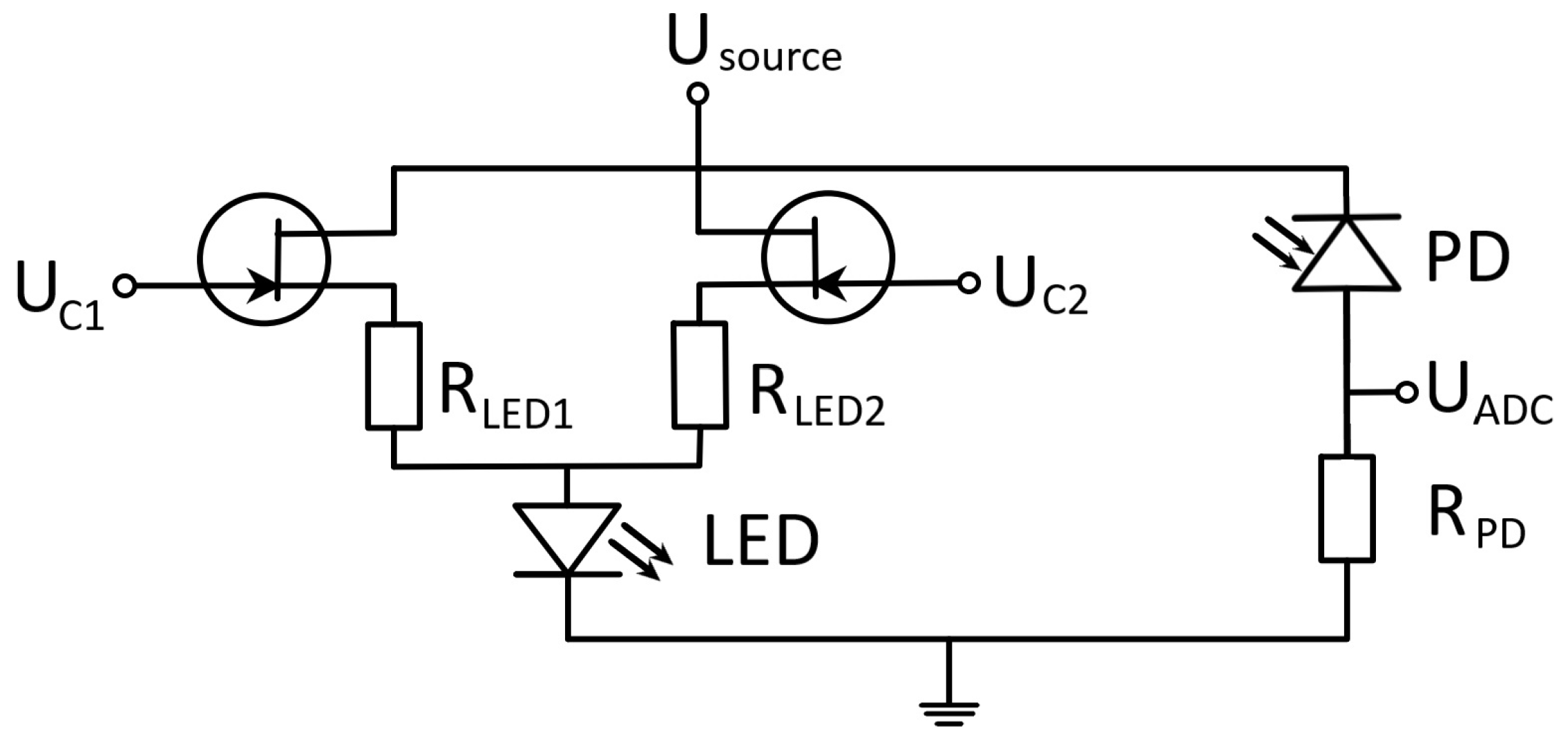
2. Materials and Methods
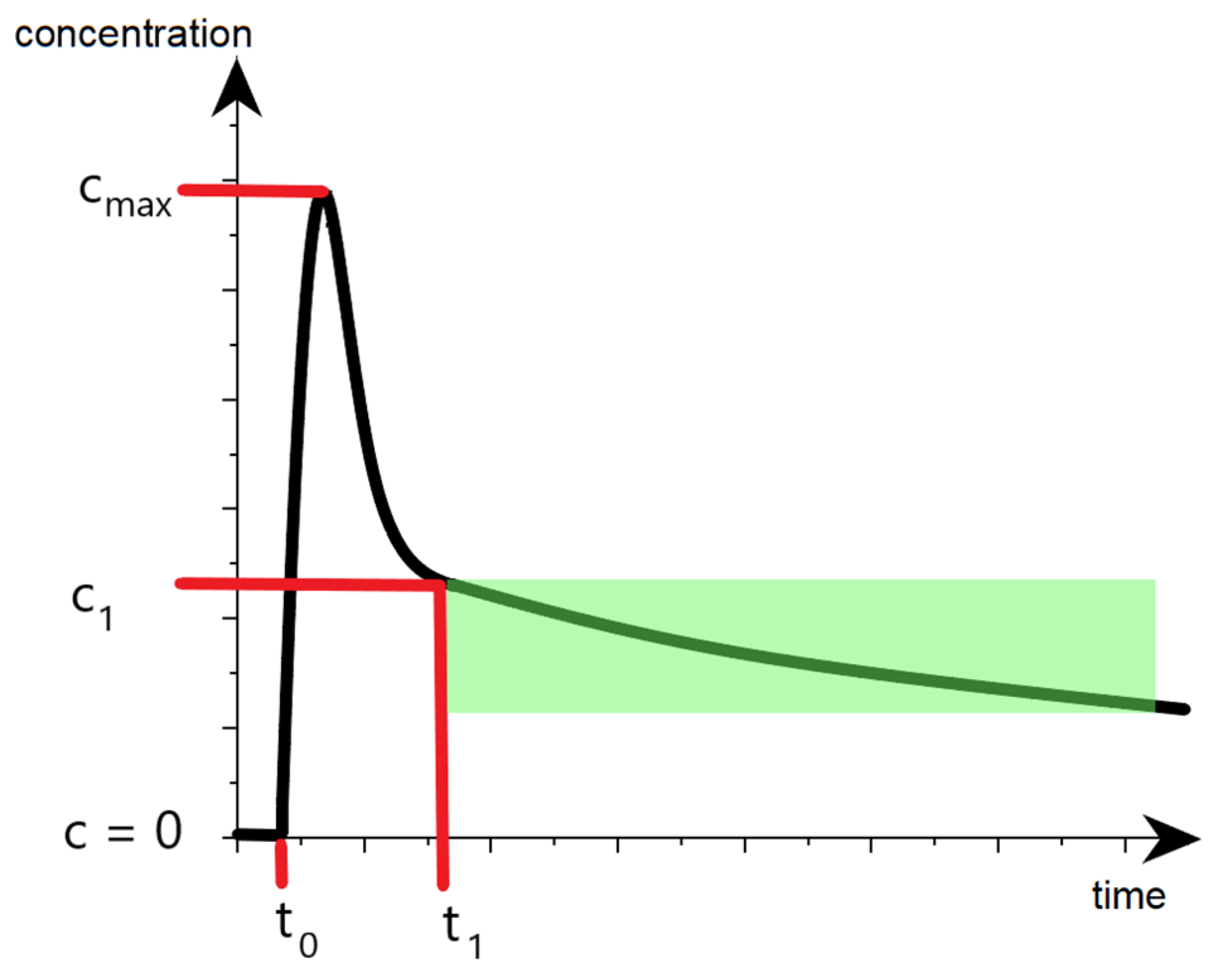
2.1. Optical Densitometry
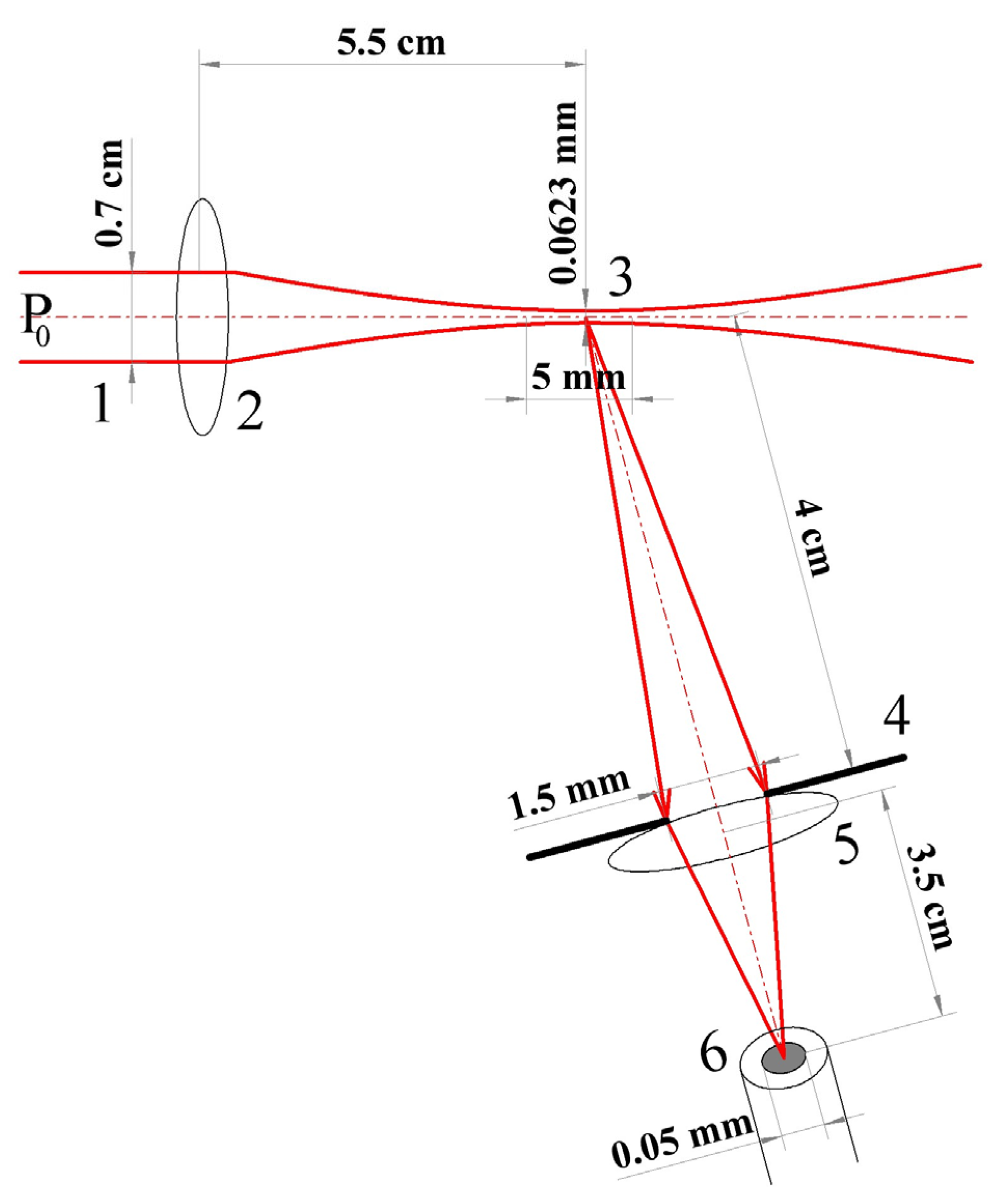
2.2. Dynamic Light Scattering
- laser module λ = 650 nm, p = 5 mW, Δf < 300 GHz, RIN less than −150 dB/Hz (KLM-G650-13-5);
- beam-forming optics (beam diameter in the studied area 1 mm, caustic length 5 mm);
- multimode fiber with a core diameter of 50 µm for scattered light collection and transportation;
- photomultiplier with spectral sensitivity 0.5 · 104 A/W for λ = 650 nm (Hamamatsu H11706-01);
- 14-bit ADC, variable sampling rate up to 50 MHz, input signal range ±10 V (LCard E14-140M).
3. Results
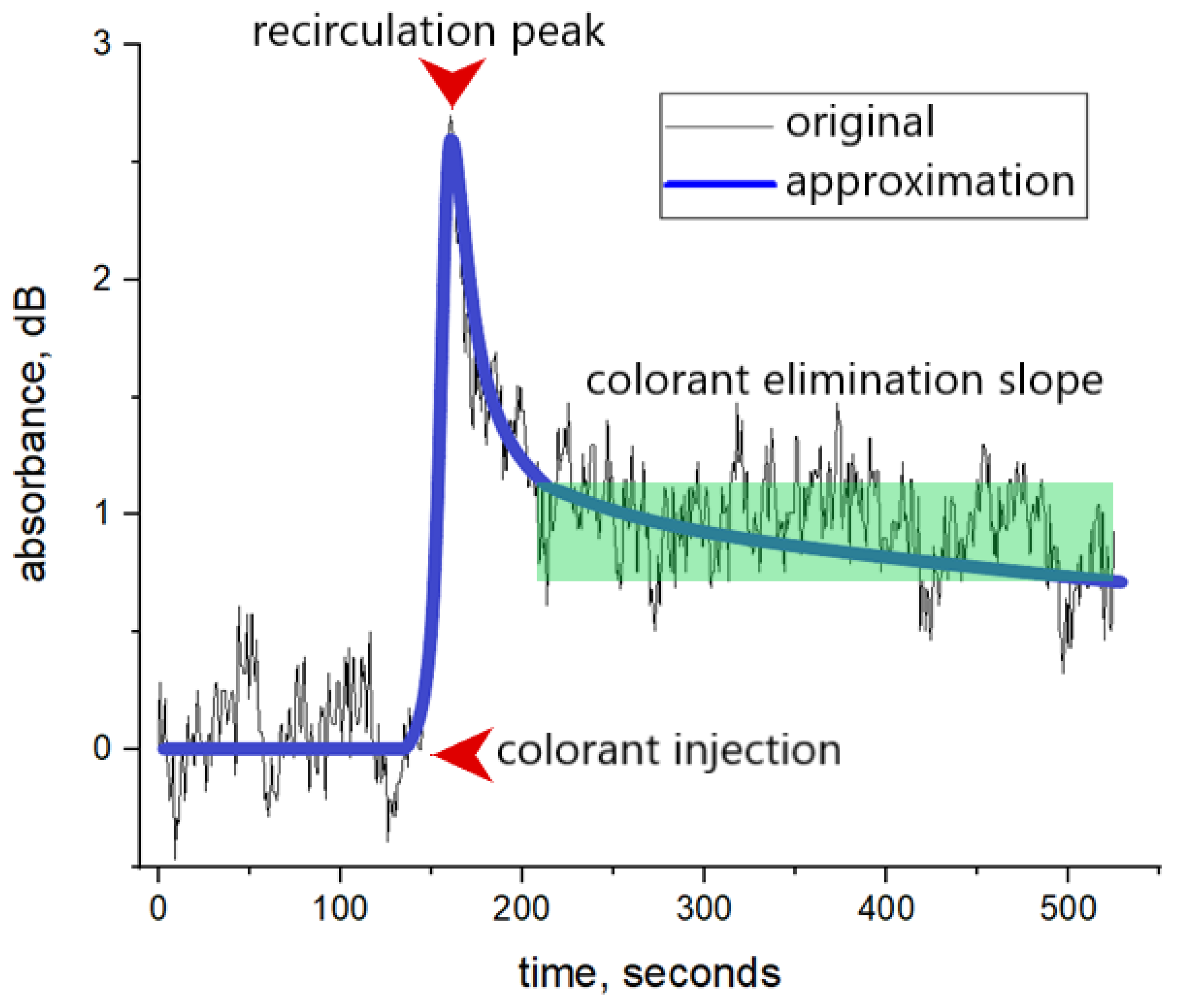
3.1. Optical Densitometry
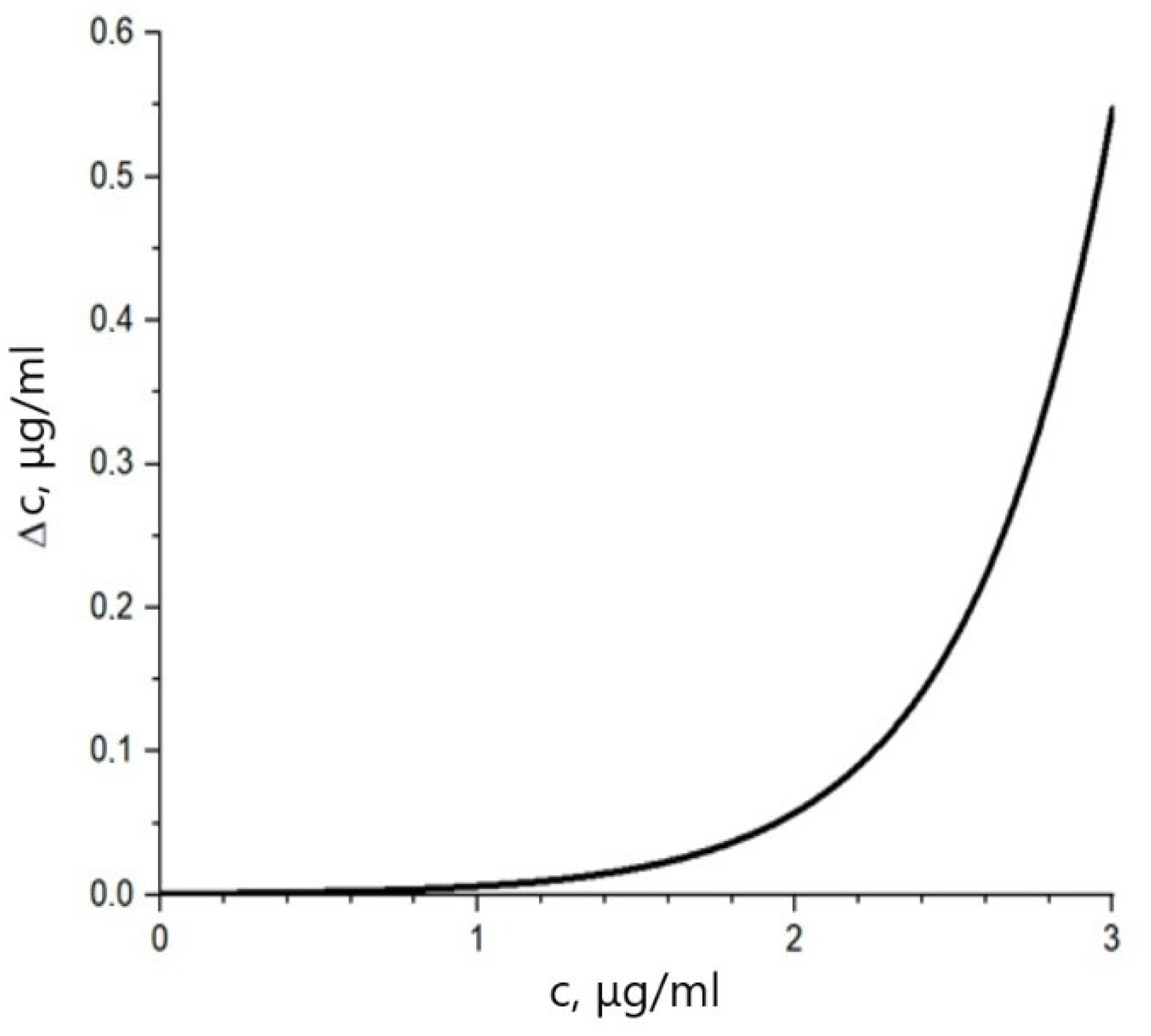
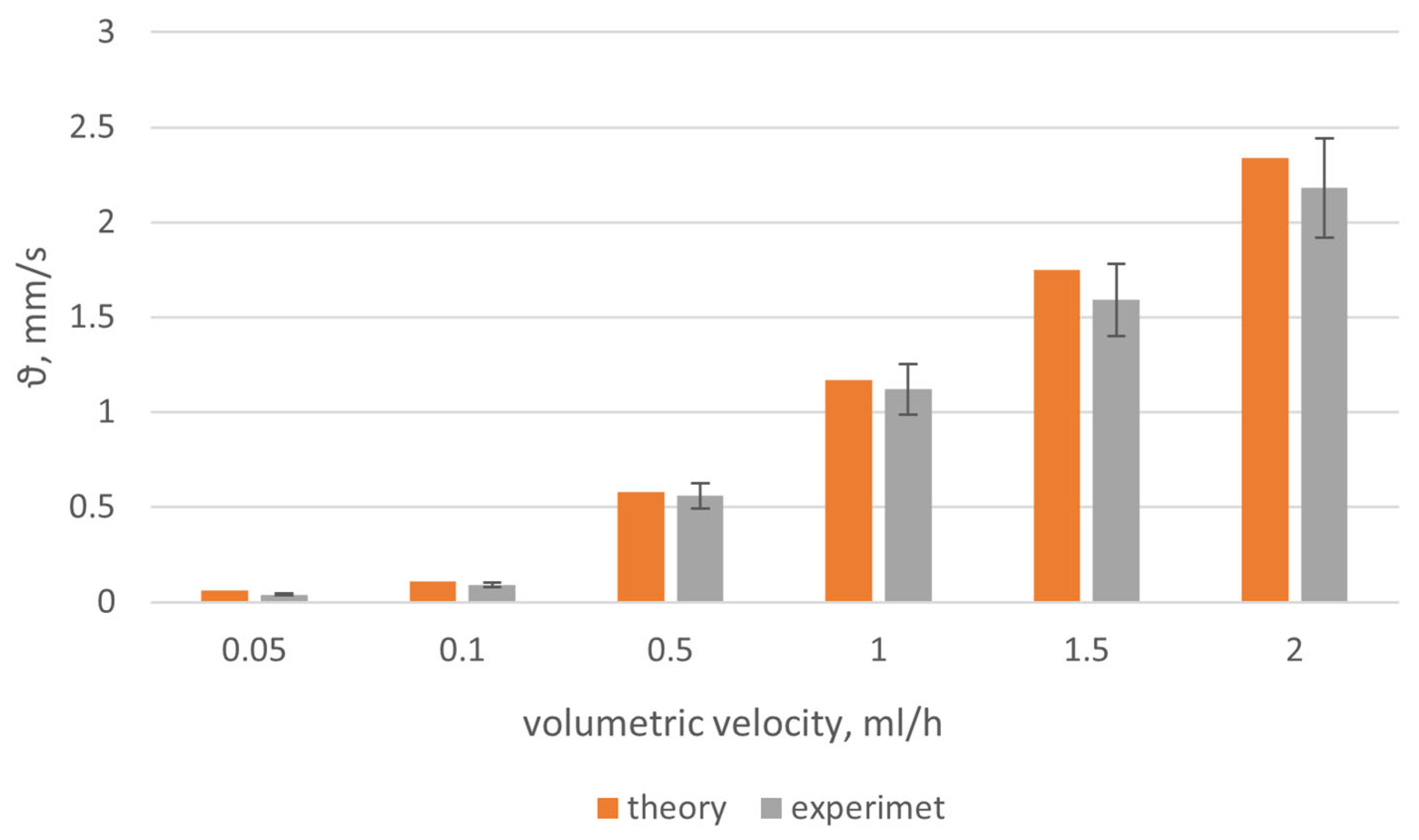
3.2. Dynamic Light Scattering
- a solution with a model suspension was prepared;
- a 20 mL syringe was installed into the dispensing apparatus;
- the capillary was fixed, and the volumetric rates set on the dispensing apparatus in the range of 3 to 30 mL/h. Before the direct measurement, a pause was held for several minutes to allow the flow rate of the solution in the capillary simulator to become constant. Before each change in the set speed, the syringe was removed from the dispenser and shaken to avoid stagnation of microspheres in the syringe and capillary;
- the laser was turned on and the program run to record and process light-scattering data;
- the data necessary for measurements were entered into the computer program: the duration of the measurement, the wavelength of laser radiation, the scattering angle, and the name of the experiment;
- a calibration measurement was launched, in which a short light pulse with a duration of 10 ms was applied to the capillary with the test sample and the laser radiation power was adjusted based on the detected scattering intensity, to determine the level of the dark current of the photodetector;
- the scattering signal was recorded as a function of time, with subsequent calculation of the temporal autocorrelation function of light scattering on the sample;
- the received data was processed (calculating the average value of the flow rate, and standard deviation).
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. WHO Guideline on Use of Ferritin Concentrations to Assess Iron Status in Individuals and Populations; World Health Organization: Geneva, Switzerland, 2020; ISBN 978-92-4-000012-4.
- Sakka, S.G. Assessment of Liver Perfusion and Function by Indocyanine Green in the Perioperative Setting and in Critically Ill Patients. J. Clin. Monit. Comput. 2018, 32, 787–796. [Google Scholar] [CrossRef]
- De Gasperi, A.; Mazza, E.; Prosperi, M. Indocyanine Green Kinetics to Assess Liver Function: Ready for a Clinical Dynamic Assessment in Major Liver Surgery? World, J. Hepatol. 2016, 8, 355. [Google Scholar] [CrossRef]
- Levesque, E.; Martin, E.; Dudau, D.; Lim, C.; Dhonneur, G.; Azoulay, D. Current Use and Perspective of Indocyanine Green Clearance in Liver Diseases. Anaesth. Crit. Care Pain Med. 2016, 35, 49–57. [Google Scholar] [CrossRef]
- Reinhart, M.B.; Huntington, C.R.; Blair, L.J.; Heniford, B.T.; Augenstein, V.A. Indocyanine Green: Historical Context, Current Applications, and Future Considerations. Surg. Innov. 2016, 23, 166–175. [Google Scholar] [CrossRef]
- Hemming, A.W.; Scudamore, C.H.; Shackleton, C.R.; Pudek, M.; Erb, S.R. Indocyanine Green Clearance as a Predictor of Successful Hepatic Resection in Cirrhotic Patients. Am. J. Surg. 1992, 163, 515–518. [Google Scholar] [CrossRef]
- Sagawa, E.; Okubo, H.; Sorin, Y.; Nakadera, E.; Fukada, H.; Igusa, Y.; Kokubu, S.; Miyazaki, A.; Watanobe, I.; Sugo, H.; et al. Use of Finger-Piece Method for Indocyanine Green Clearance Test. Hepatol. Res. 2017, 47, 1235–1240. [Google Scholar] [CrossRef]
- Purcell, R.; Kruger, P.; Jones, M. Indocyanine Green Elimination: A Comparison of the LiMON and Serial Blood Sampling Methods. ANZ J. Surg. 2006, 76, 75–77. [Google Scholar] [CrossRef]
- Takahashi, H.; Shigefuku, R.; Yoshida, Y.; Ikeda, H.; Matsunaga, K.; Matsumoto, N.; Okuse, C.; Sase, S.; Itoh, F.; Suzuki, M. Correlation between Hepatic Blood Flow and Liver Function in Alcoholic Liver Cirrhosis. World J. Gastroenterol. 2014, 20, 17065. [Google Scholar] [CrossRef]
- Karavaev, A.S.; Borovik, A.S.; Borovkova, E.I.; Orlova, E.A.; Simonyan, M.A.; Ponomarenko, V.I.; Skazkina, V.V.; Gridnev, V.I.; Bezruchko, B.P.; Prokhorov, M.D.; et al. Low-Frequency Component of Photoplethysmogram Reflects the Autonomic Control of Blood Pressure. Biophys. J. 2021, 120, 2657–2664. [Google Scholar] [CrossRef]
- Djeldjli, D.; Bousefsaf, F.; Maaoui, C.; Bereksi-Reguig, F.; Pruski, A. Remote Estimation of Pulse Wave Features Related to Arterial Stiffness and Blood Pressure Using a Camera. Biomed. Signal Process. Control 2021, 64, 102242. [Google Scholar] [CrossRef]
- Gilbert Cherrick, B.R.; Stein, S.W.; Leevy, C.M.; Davidson, C.S.; City, J. Indocyanine Green: Observations on Its Physical Properties, Plasma Decay, and Hepatic Extraction. Am. Soc. Clin. Investig. 1960, 39, 592–600. [Google Scholar] [CrossRef] [Green Version]
- Gödje, O.; Höke, K.; Alwin, E.; Felbinger, T.W.; Reuter, D.A.; Reichart, B.; Friedl, R.; Hannekum, A.; Pfeiffer, U.J. Reliability of a New Algorithm for Continuous Cardiac Output: Critical Care Medicine. Crit. Care Med. 2002, 30, 52–58. [Google Scholar] [CrossRef]
- Dremin, V.; Kozlov, I.; Volkov, M.; Margaryants, N.; Potemkin, A.; Zherebtsov, E.; Dunaev, A.; Gurov, I. Dynamic Evaluation of Blood Flow Microcirculation by Combined Use of the Laser Doppler Flowmetry and High-Speed Videocapillaroscopy Methods. J. Biophotonics 2019, 12, e201800317. [Google Scholar] [CrossRef] [Green Version]
- Mayerhöfer, T.G.; Pahlow, S.; Popp, J. The Bouguer-Beer-Lambert Law: Shining Light on the Obscure. ChemPhysChem 2020, 21, 2029–2046. [Google Scholar] [CrossRef]
- Kolokolnikov, I.; Savchenko, E.; Velichko, E. Spectrophotometry Setup for Solute Concentration Determination. In Proceedings of the 2020 IEEE International Conference on Electrical Engineering and Photonics (EExPolytech), Polytech 2020, St. Petersburg, Russia, 15–16 October 2020; pp. 258–260. [Google Scholar] [CrossRef]
- Savchenko, E.; Kolokolnikov, I.; Velichko, E.; Osovskikh, V.; Kiseleva, L.; Musakulova, Z. Design of Liver Functional Reserve Estimation Technique Based on Optical Densitometry. Diagnostics 2020, 10, 599. [Google Scholar] [CrossRef]
- Savchenko, E.A.; Velichko, E.N. The Use of Speckle Correlation Analysis to Determine Blood Flow Velocity. Opt. Spectrosc. 2020, 128, 998–1003. [Google Scholar] [CrossRef]
- Berne, B.; Pecora, R. Dynamic Light Scattering: With Applications to Chemistry, Biology, and Physics; Courier Corporation: Gloucester, MA, USA, 2000. [Google Scholar]
- Tuchin, V. V Handbook of Optical Biomedical Diagnostics; SPIE-The International Society for Optical Engineering: Bellingham, WA, USA, 2002; ISBN 0-8194-4238-0. [Google Scholar]
- Lijima, T.; Aoyagi, T.; Iwao, Y.; Masuda, J.; Fuse, M.; Kobayashi, N.; Sankawa, H. Cardiac Output and Circulating Blood Volume Analysis by Pulse Dye-Densitometry. J. Clin. Monit. 1997, 13, 81–89. [Google Scholar] [CrossRef]
- Gelt, T.D.; Borsukov, A.V. Advanced technique of laser Doppler imaging for the diagnostics of intensity of peripheral microcirculation changes in patients with diffused liver diseases. Acta Biomed. Sci. 2015, 1, 11–17. (In Russia) [Google Scholar]
- Saez, A.M.O.; Mosel, F.; Nürnberger, J.; Rushentsova, U.; Gössl, M.; Mitchell, A.; Schäfers, R.F.; Philipp, T.; Wenzel, R.R. Laser Doppler imager (LDI) scanner and intradermal injection for in vivo pharmacology in human skin microcirculation: Responses to acetylcholine, endothelin-1 and their repeatability. Br. J. Clin. Pharmacol. 2005, 59, 511–519. [Google Scholar] [CrossRef] [Green Version]
- Nemeth, N.; Peto, K.; Magyar, Z.; Klarik, Z.; Varga, G.; Oltean, M.; Mantas, A.; Czigany, Z.; Tolba, R.H. Hemorheological and microcirculatory factors in liver ischemia-reperfusion injury—An update on pathophysiology, molecular mechanisms and protective strategies. Int. J. Mol. Sci. 2021, 22, 1864. [Google Scholar] [CrossRef]
- Leonov, S.D.; Khalepo, O.V.; Rodin, A.V.; Karasev, A.S.; Sorokina, A.A.; Panchenkov, D.N. Assessment of the liver microcirculation by laserdoppler flowmetry after extended liver resection in the experiment. Laser Med. 2022, 26, 26–30. (In Russia) [Google Scholar] [CrossRef]
- Mirkin, E.; Savchenko, E. Configuring the Interval Target in a Multilayer Feedforward Neural Network on the Example of the Problem of Medical Diagnostics. Springer Proc. Phys. 2021, 255, 463–475. [Google Scholar] [CrossRef]
- Mirkin, E.L.; Savchenko, E.Y. A New Approach to Constructing a Decentralized Hierarchical Modular Network for Solving Complex Problems in the Paradigm of Training Artificial Neural Networks with a Teacher. Opt. Mem. Neural Netw. Inf. Opt. 2021, 30, 112–130. [Google Scholar] [CrossRef]











Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karseeva, E.; Kolokolnikov, I.; Medvedeva, E.; Savchenko, E. Joint Methodology Based on Optical Densitometry and Dynamic Light Scattering for Liver Function Assessment. Diagnostics 2023, 13, 1269. https://doi.org/10.3390/diagnostics13071269
Karseeva E, Kolokolnikov I, Medvedeva E, Savchenko E. Joint Methodology Based on Optical Densitometry and Dynamic Light Scattering for Liver Function Assessment. Diagnostics. 2023; 13(7):1269. https://doi.org/10.3390/diagnostics13071269
Chicago/Turabian StyleKarseeva, Elina, Ilya Kolokolnikov, Ekaterina Medvedeva, and Elena Savchenko. 2023. "Joint Methodology Based on Optical Densitometry and Dynamic Light Scattering for Liver Function Assessment" Diagnostics 13, no. 7: 1269. https://doi.org/10.3390/diagnostics13071269