1. Introduction
The first confirmed COVID-19 case, according to the World Health Organization (WHO) reports, was in the central Chinese city of Wuhan on 8 December 2019. COVID-19 was reported as an epidemic in January 2020. From that date onwards, new confirmed cases were reported each day and the COVID-19 virus spread to every continent. According to the WHO, the number of confirmed COVID-19 virus cases is more than 416,614,050 and the number of deaths is more than 5,844,095 [
1]. COVID-19 has become a global health crisis and the WHO has declared it a major pandemic. Understanding how the disease spreads and determining how undetected and undocumented cases contribute to the transmission of the virus are major challenges. Although COVID-19 vaccines are available on the market, there is still an inevitable demand for smart healthcare systems for the general population—and, especially, the elderly—so that the expected shortage in doctors in the health sector during the crisis can be promptly addressed. With the spread of COVID-19 to numerous countries in the world, considering the increases in the number of people infected and the number of deaths from day to day, it has become mandatory to diagnose and identify this COVID-19 virus.
All over the world, the COVID-19 virus remains a threat to the economies of countries and the health of people. It has been proven that the disease is transmitted from one person to another and, therefore, delays in discovering the disease lead to the spread of infection through interactions between the healthy and infected patients [
2,
3,
4].
The test to verify a person’s infection with the virus is often implemented by taking samples from the patient’s throat, sputum, or nasopharynx to analyze the PCR of the viral RNA. However, one of the limitations of such tests is their low accuracy [
5,
6,
7,
8]. The diagnosis of COVID-19 based on laboratory tests is costly, laborious, time-consuming, and involves a complicated manual process [
9]. Therefore, it is recommended that this type of test be replaced with chest CT images, which could be used as one type of early investigative test [
3]. The challenge of laboratory testing with CT image analysis is that it demands a radiology expert and takes a significant amount of time. One solution for this challenge is to save valuable time for medical professionals by using an automated analysis system.
Thus, the early diagnosis of COVID-19 would be invaluable in containing the disease outbreak. However, as the diagnosis of COVID-19 based on laboratory tests still displays a low positive rate, as well as being costly, laborious, time-consuming, and manually complicated [
9], suggestions have emerged from specialists recommending the use of radiography screening as a primary tool for checking for COVID-19. With increased numbers of infected patients on a daily basis, especially in the epidemiological setting, the bottleneck for this method is the requirement for a large number of expert X-ray specialists to interpret the CT images. Moreover, the similar and overlapping patterns of lung diseases make it difficult for radiologists to point out these slight differences [
10]. As a result, there is an urgent need to develop intelligent systems to aid radiologists with fast and accurate results.
Artificial intelligence (AI) has made great strides in recent years. Deep learning and the accompanying innovations offer radiologists a chance to change the radiology scene and improve survival rates. Deep learning neural system models have been applied to a few imaging tasks to date, including image segmentation, classification, and object detection. Deep learning techniques are unique compared to classic AI strategies, which are the significant ones. The latter employ feature extraction strategies in preparation for the computation, while deep learning techniques familiarize themselves with the image information without the requirement for feature extraction. Deep learning provides promising solutions for the analysis of medical images in future applications. With the recent advances in machine learning and artificial intelligence applications, especially in the medical field and including medical image processing, artificial intelligence has become a promising tool that can change diagnosis methods. Deep learning networks, as an artificial intelligence tool, have proven successful in image classification with their unique characteristics of being able to learn image representations automatically and mapping features onto continuous vectors that are subsequently used for predictions. AI applications in radiology [
11] are driven by the idea that medical images are sets of data that can be computed by a machine to extract useful information from the properties of the image [
12].
Thus, this paper presents a novel technique for the detection of the COVID-19 virus early on based on X-ray and CT chest radiography image analysis using deep learning algorithms. This methodology can be basically classified as image analysis as it comprises steps such as image acquisition, image preprocessing, feature extraction, and the employment of different classifiers. This paper’s contributions can be outlined as follows: (1) We built promising, fine-tuned DL models capable of diagnosing chest X-ray and CT images that showed improvements in their precision, sensitivity, specificity, F1-scores, accuracy, and data access time. The models for COVID-19 detection were trained and their performances were evaluated using novel samples in order to contribute to the control of the epidemic. (2) The proposed system will reduce the pressure on the national healthcare budget by reducing the cost of the physical tests performed in clinical laboratories. It has been reported that the cost of a PCR test is about USD 120–130 [
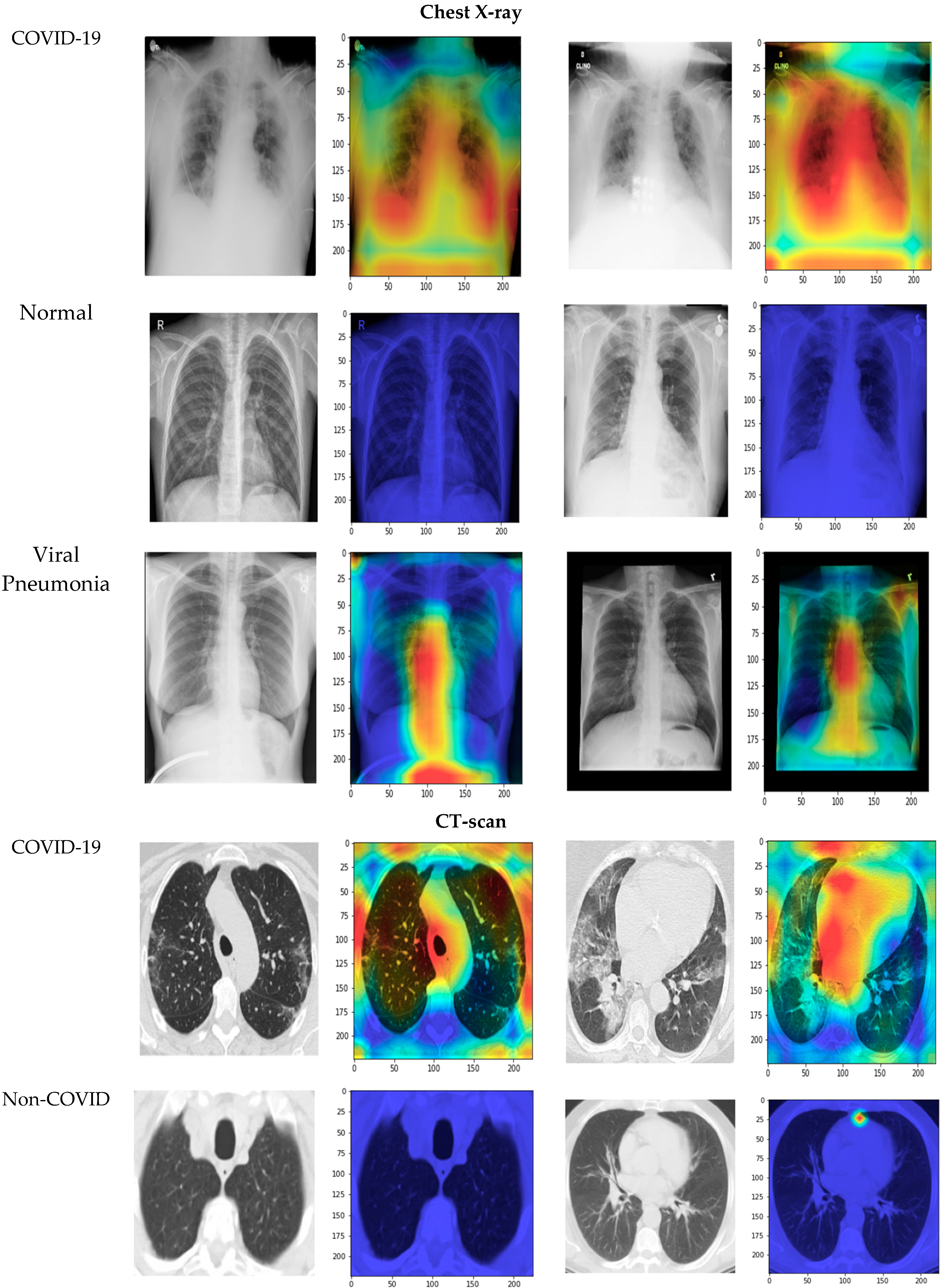
13]. (3) For radiologists, with the spread of COVID-19, a daily flood of CT images need to be analyzed; the proposed techniques can act as an aid for radiologists (regardless of the level of experience) by reducing not only the time required to diagnose CT scans but also the pressure on the radiologist. (4) The disease can be localized by using a Grad-CAM algorithm that visualizes the infected areas of the lungs in chest X-ray and CT images.
The remainder of the paper is laid out as follows:
Section 2 contains a literature review;
Section 3 presents the proposed methodology;
Section 4 contains the experimental results and discussion; and, finally, conclusions are drawn in
Section 5.
2. Literature Review
The attention the COVID-19 virus has received from researchers has led to an enormous number of publications. In this section, most of the recently developed systems applying deep learning techniques to COVID-19 detection are explored. Barstugan et al. [
14] proposed a coronavirus classification technique for CT images based on machine learning methods. The dataset, consisting of patients from Italy, one of the most endemic regions, comprised 618 images, including 219 images from COVID-19 patients, 224 images from influenza-A viral pneumonia patients, and 175 images from healthy cases. Chowdhury [
15] trained four convolutional neural networks (CNNs) to classify CT images into two classes: normal and COVID-19 pneumonia. Linda et al. [
9] proposed COVID-net, which is a deep CNN that can recognize and identify the COVID-19 disease from CT images. Shuai et al. [
16] adapted the Inception transfer learning model to detect COVID-19 in CT images. Ghoshal et al. [
17] presented a Bayesian deep learning classifier to estimate model uncertainty using the transfer learning method with COVID-19 X-ray images. The proposed system differs from the others in tracking disease progression through a deep analysis of the periodical changes in the CT images from the same patient, making it possible to modify treatment and help achieve improved results for patients. It also utilizes an efficient parameterized transfer learning model and smart data augmentation.
Rahimzadeh et al. [
18] proposed a linked CNN dependent on the Xception and ResNet50V2 models to characterize COVID-19 cases from chest X-rays. The created framework utilized a dataset that contained 180 images of COVID-19 patients, 6054 images of pneumonia patients, and 8851 images of typical individuals. For each of the eight preparation stages, 633 pictures were selected. The test results exhibited 99.56% precision with 80.53% of COVID-19 cases. Fan et al. [
19] proposed a multi-kernel attention network to analyze chest X-ray images from COVID-19 patients. Their model has three stages: a feature extraction stage followed by two parallel multi-kernel-size attention modules and, finally, the classification stage. The experimental results demonstrated improved performance in COVID-19 detection and an accuracy of 98.2%.
Loey et al. [
20] presented a generative adversarial network (GAN) using deep learning to analyze COVID-19 from chest X-rays. Their study utilized the three pre-prepared models AlexNet, GoogleNet, and RestNet18. Apostolopoulos et al. [
21] presented an exchange learning technique with a CNN for the analysis of COVID-19 cases using chest X-rays. The framework can detect COVID-19 images using five main models: VGG19, Inception, MobileNet, Xception, and Inception-ResNetV2. VGG19 was chosen as the fundamental learning model and it showed 93.48% accuracy. To detect COVID-19 patients, Panwar et al. [
22] presented a binary image classification task. The input data were classified using a fine-tuned VGG model. Mishra et al. [
23] used deep CNN-based image classification models to differentiate COVID-19 instances using chest CT scan images. Song et al. [
24] employed a linear classifier to extract semantic features from CT scans. Jaiswal et al. [
2] used a DenseNet201-based deep transfer learning (DTL) model to identify patients with COVID-19. The proposed model uses its own training weights to extract features from the ImageNet dataset. Silva et al. [
25] proposed CovidNet, an efficient, voting-based technique for analyzing COVID-19 patterns in CT images.
Allioui et al. [
26] proposed a multi-agent deep learning model for enhancement of COVID-19 CT image segmentation. Their proposal was based on multi-agent deep reinforcement learning (DRL), which utilizes a modified version of the Deep Q-Network. Khan et al. [
27] proposed a COVID-19 detection method for CT images using deep learning, entropy-controlled optimization, and parallel feature fusion techniques. Their method mainly depends on the AlexNet and VGG16 models. The features are extracted and fused using a parallel positive correlation approach. Then, the entropy-controlled firefly optimization method is employed to select the optimal features. Their best achievement was an accuracy rate of 98%. Rehman et al. [
28] proposed a framework for the detection of COVID-19 disease and 14 other types of chest diseases. They employed a convolutional neural network architecture with a soft-max classifier. Then, transfer learning was applied in order to extract deep features, which provided results similar to classic machine learning classification methods. Guo et al. [
29] studied COVID-19 diagnosis from chest CT scans via an ensemble learning method based on ordinal regression. Their proposal relies on multi-binary, neuron stick-breaking, and soft label techniques. Mukherjee et al. [
30] implemented an advanced deep network architecture with two CT image datasets. The authors utilized the transfer learning strategy with custom-sized input tailored to each type of deep architecture in order to improve the performance. Their best models achieved an average accuracy of 99.4%.
Nasiri and Hasani [
31] proposed a method for diagnosing coronavirus disease from X-rays. They used the DenseNet169 deep neural network (DNN). The extracted features were then used as input for the Extreme Gradient Boosting (XGBoost) algorithm to perform the classification task. They achieved accuracy up to 99.78%. Ullah et al. [
32] developed an effective COVID-19 detection technique using the Shufflenet CNN by employing three types of images; i.e., chest radiographs, CT scans, and ECG trace images. Nasiri and Alavi [
33] proposed a pretrained network named DenseNet169 to extract features from X-ray images. Analysis of variance (ANOVA) was employed as a feature selection method to reduce the computation and time complexity. Then, the selected features were classified with Extreme Gradient Boosting (XGBoost). Their proposed method reached 98.72% accuracy for two-class classification and 92% accuracy for multiclass classification.
3. Proposed Methodology
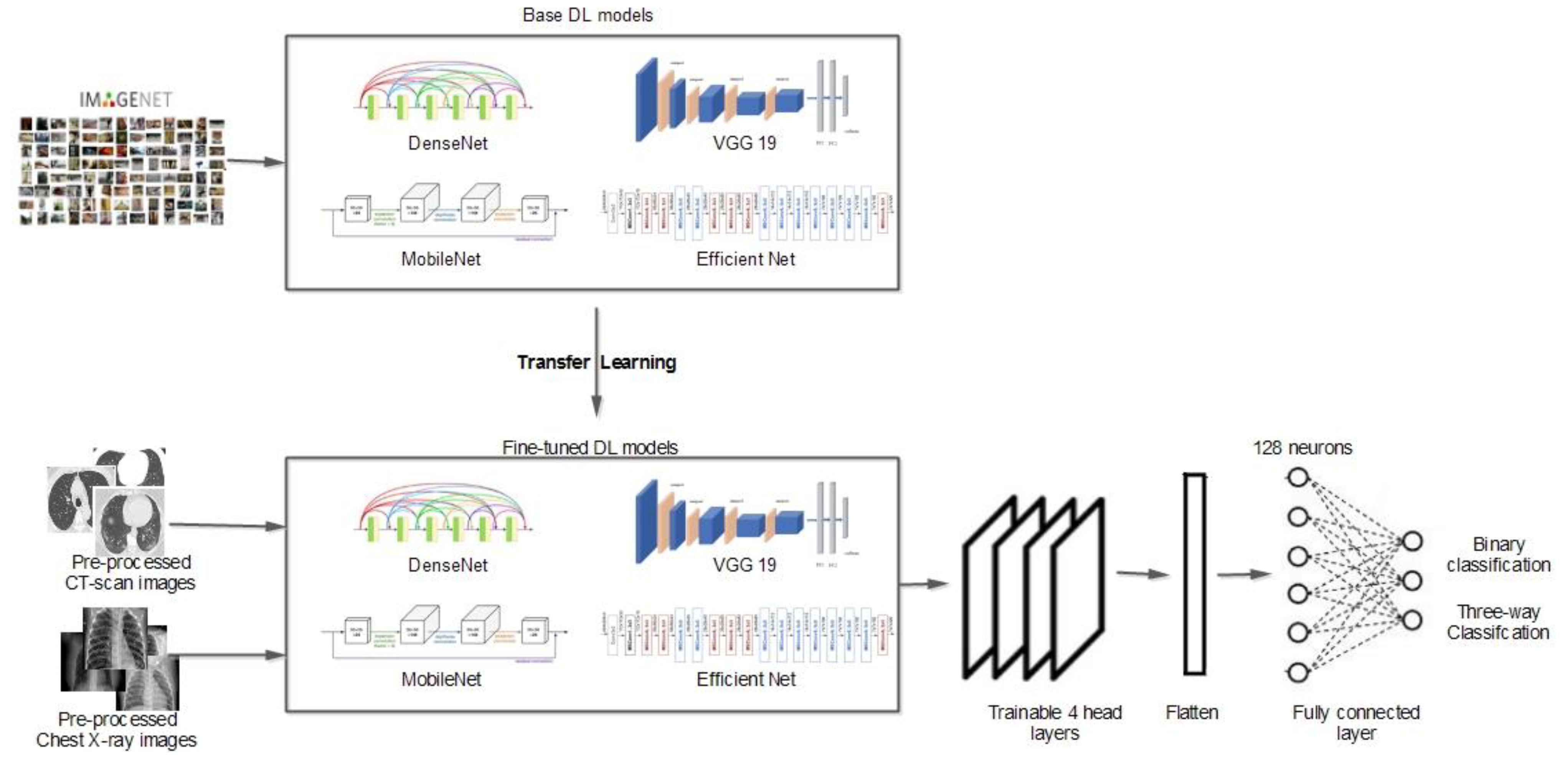
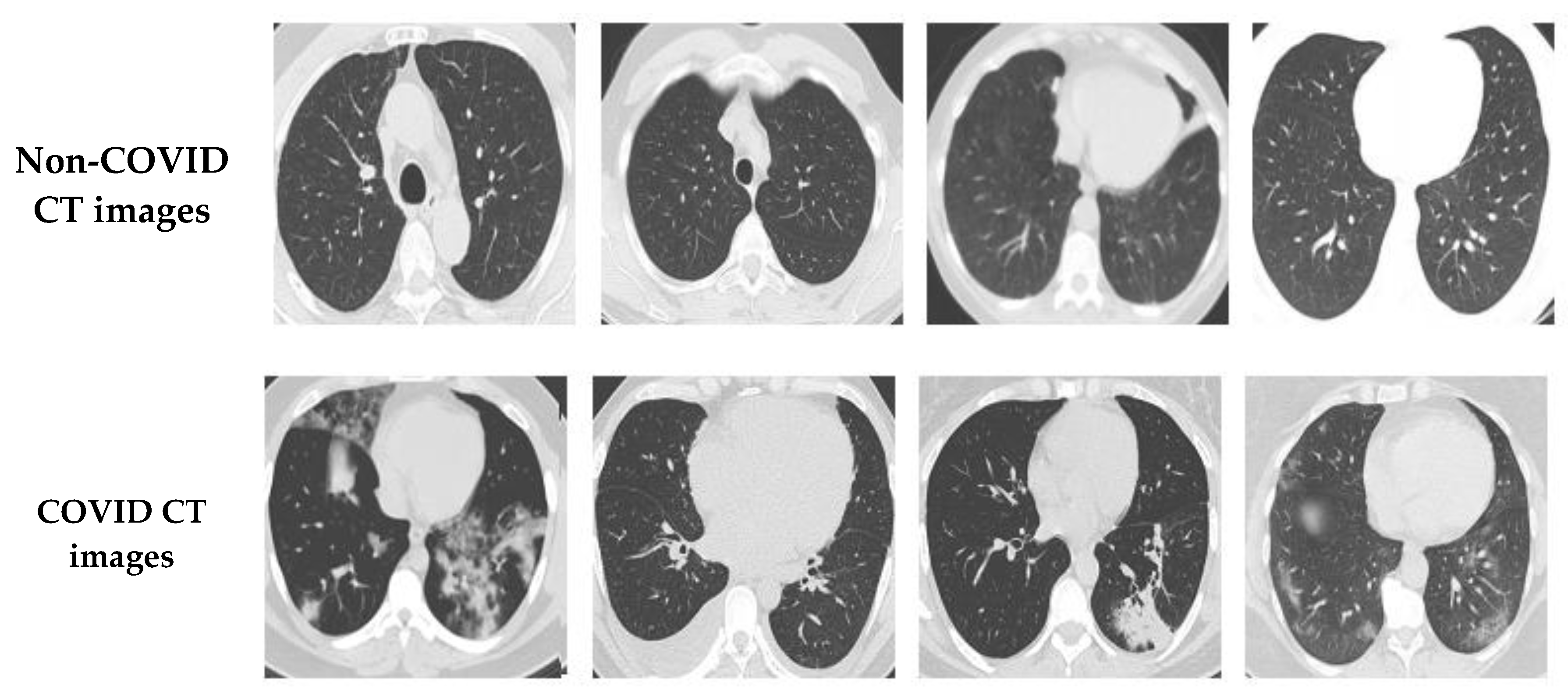
When building the diagnostic DL model, the chest X-ray and CT images were initially collected. In this study, as illustrated in
Figure 1, a publicly available SARS-CoV-2 CT scan dataset was used [
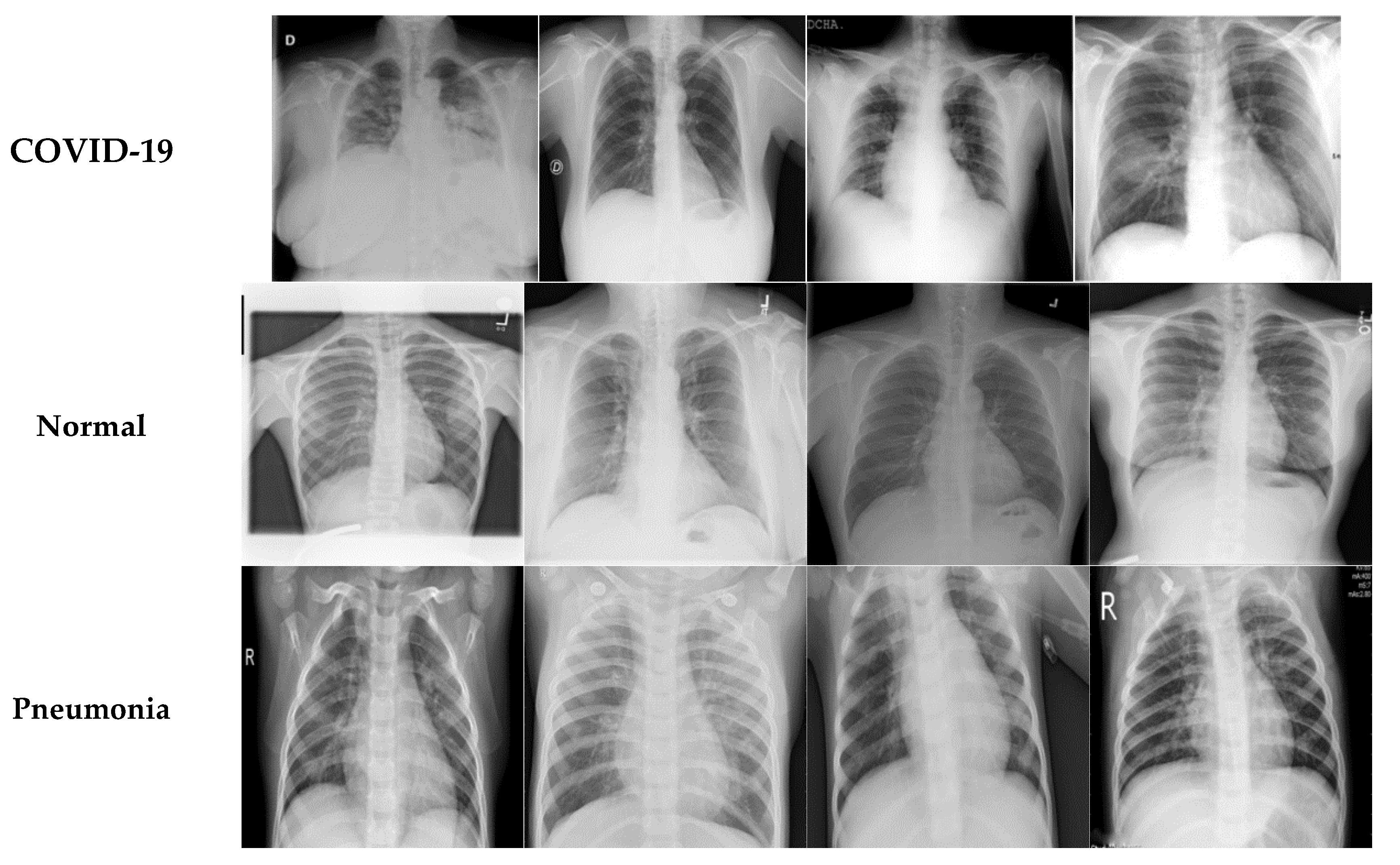
34]. The dataset contained 1252 CT scans positive for COVID-19 and 1230 CT scans from non-infected individuals. Another chest X-ray dataset [
35] with 6939 sample images was also considered in this study, which included three classes (COVID-19, normal, and pneumonia) with 2313 samples for each category.
Section 4.1 provides a detailed description of the datasets utilized. Preprocessing, one of the basic phases in DL learning, is responsible for resizing images to fit the deep learning model. Other processes are also performed to prepare the images for the next phase, such as data augmentation to select the more diverse, more robust datasets to train the model; image grayscale conversion; and image binarization.
Transfer learning is an inevitable step for networks with sparse data (a few hundred or thousand images). Transfer learning is applied to a vast, pretrained network of millions of images. There are two main techniques for applying transfer learning: feature extraction and fine-tuning. For the first technique, only some of the newly added layers are updated and improved during the training phase. In contrast, for the second technique, the weights for all layers are updated, optimized, and customized for the new classification problem. In general, fine-tuning is more effective than the feature extraction technique. Fine-tuning DL models (EfficientB0, VGG-19, DenseNet121, MobileNetV2, etc.) requires extensive resources and time. Initially, the convolution layers learn low-level features and, as the network grows, mid/high-level features are learned. With fine-tuning, these trained low-level features are retained, while the high-level features are trained for new classification problems. In this study, five residual blocks were used: the input, two convolution layers, a max-pooling layer, and an output layer. Subsequently, fine-tuning transfer learning was employed for the first four head layers of the network. The trainable parameters were adjusted along with the supplemented soft-max activation function, which consisted of two or three output neurons relating to binary or three-way classification. Algorithm 1 summarizes the working steps for our DL model.
| Algorithm 1: DL Model Working Steps |
| Input: τ1←Dataset containing SARSCOV2 CT—scans |
| τ2←Dataset containing chest X—ray images |
| α←Learning rate |
| β←Batch size |
| Output: ω←CNN final weights |
| Begin: |
| 1: Set train and test data sizes |
| 2: Calculate train class weights |
| 3: Feed in a base model (IMAGENET weights) // EfficientB0, VGG-19, DenseNet121, EfficientB7, or MobileNetV2 |
| 4: Generate a new model (transfer learning of low layers) |
| 5: Set model’s top layers // average pooling, flatten, dense, dropout |
| 6: Set the initial hyperparameters: α, β, ω |
| 7: Train the base models and store the final weights (ω) |
| 8: While (stopping condition not reached) do |
| 9: Move forward and calculate cross-entropy |
| 10: Move backward and update the optimizer |
| 11: EndWhile |
In this section, the architectures for the CNNs and the transfer learning approach are described. Although CNNs are more similar to vanilla neural networks, the convolution operation is carried out in more than one layer [
36]. A simple neural network layer is presented in Equation (1).
where
is the current layer;
is the first or input layer;
represents the weights for the first layer; and
is the bias. For instance, for the VGG19 Conv layer [
37] in Equation (2), for each channel of x, there is a corresponding channel in the first filter of
. Equation (3) illustrates the output of the final layer.
where
i,
j, and
k correspond to the row, column, and channel for
, respectively;
l,
m, and
n refer to the row, column, and channel number for the filter, respectively; and
k denotes the filter being used for the present epoch.
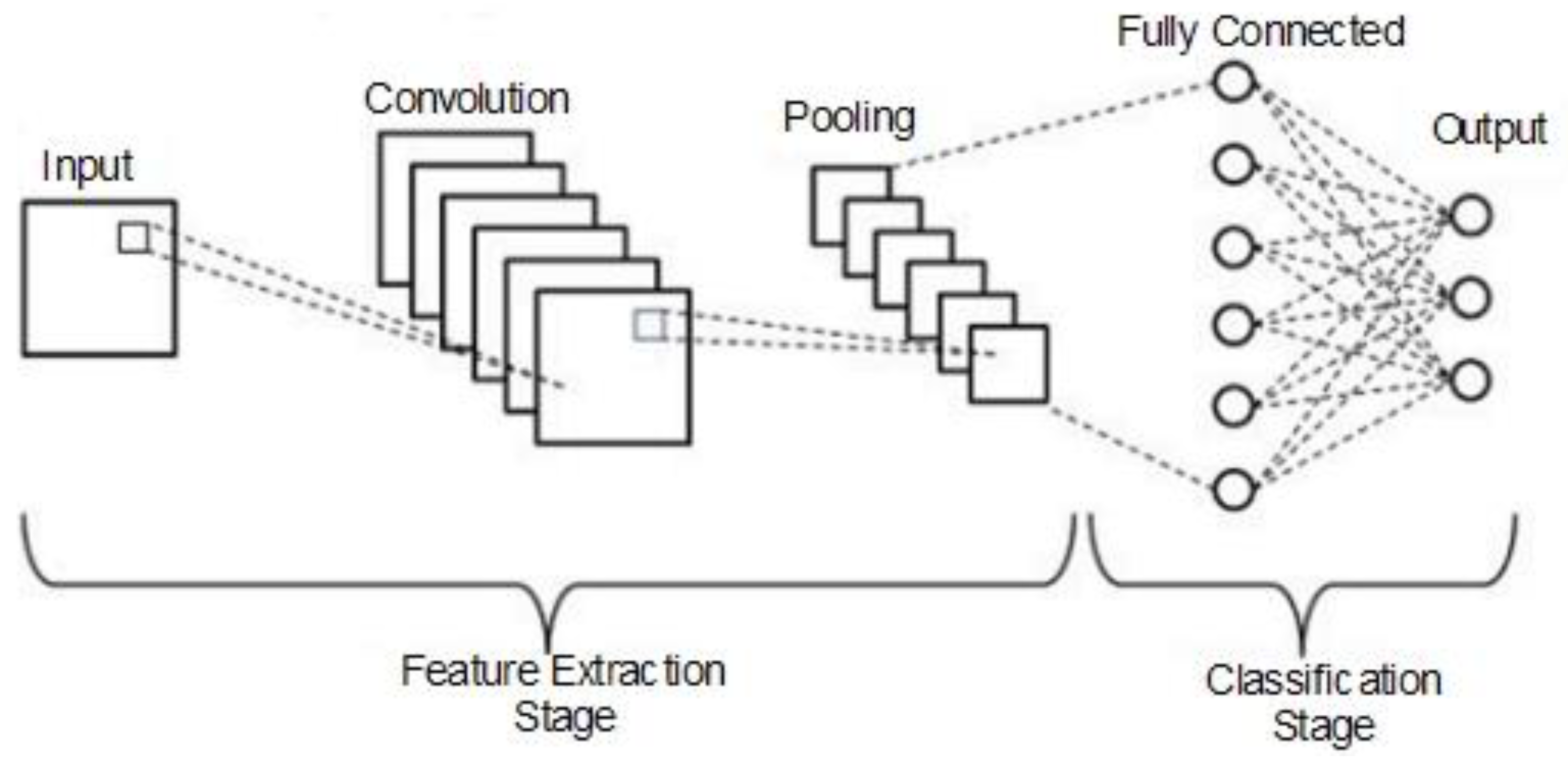
Figure 2 depicts the general convolution operation carried out by the CNNs, which comprised input, convolution, pooling, fully connected, and output layers. The chest X-ray and CT scan dataset images were fed into the input layer.
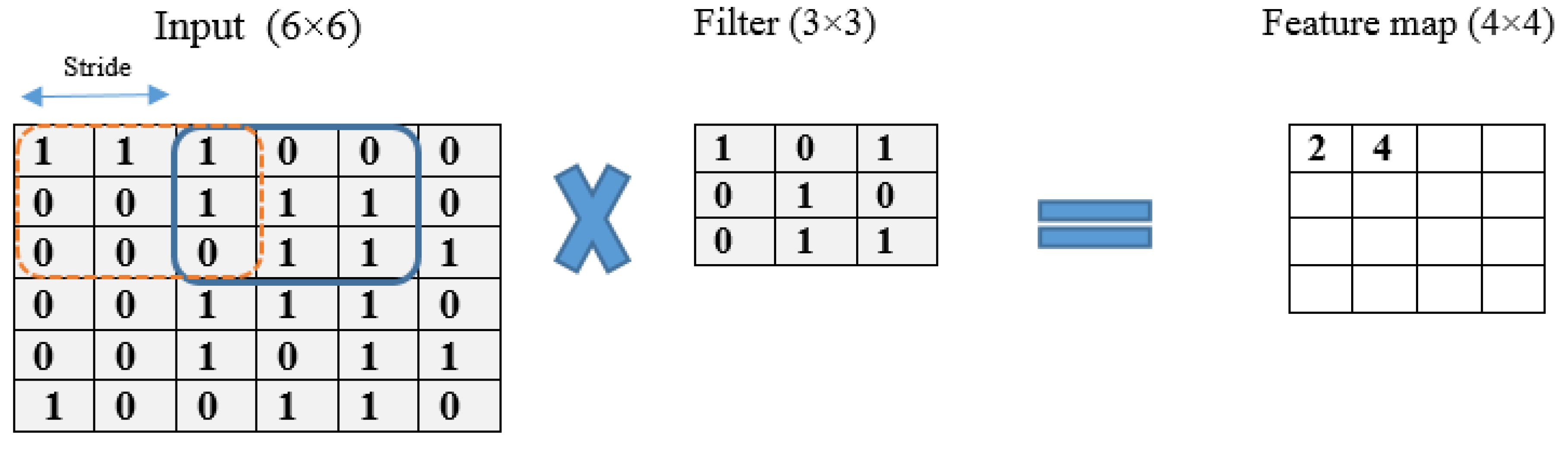
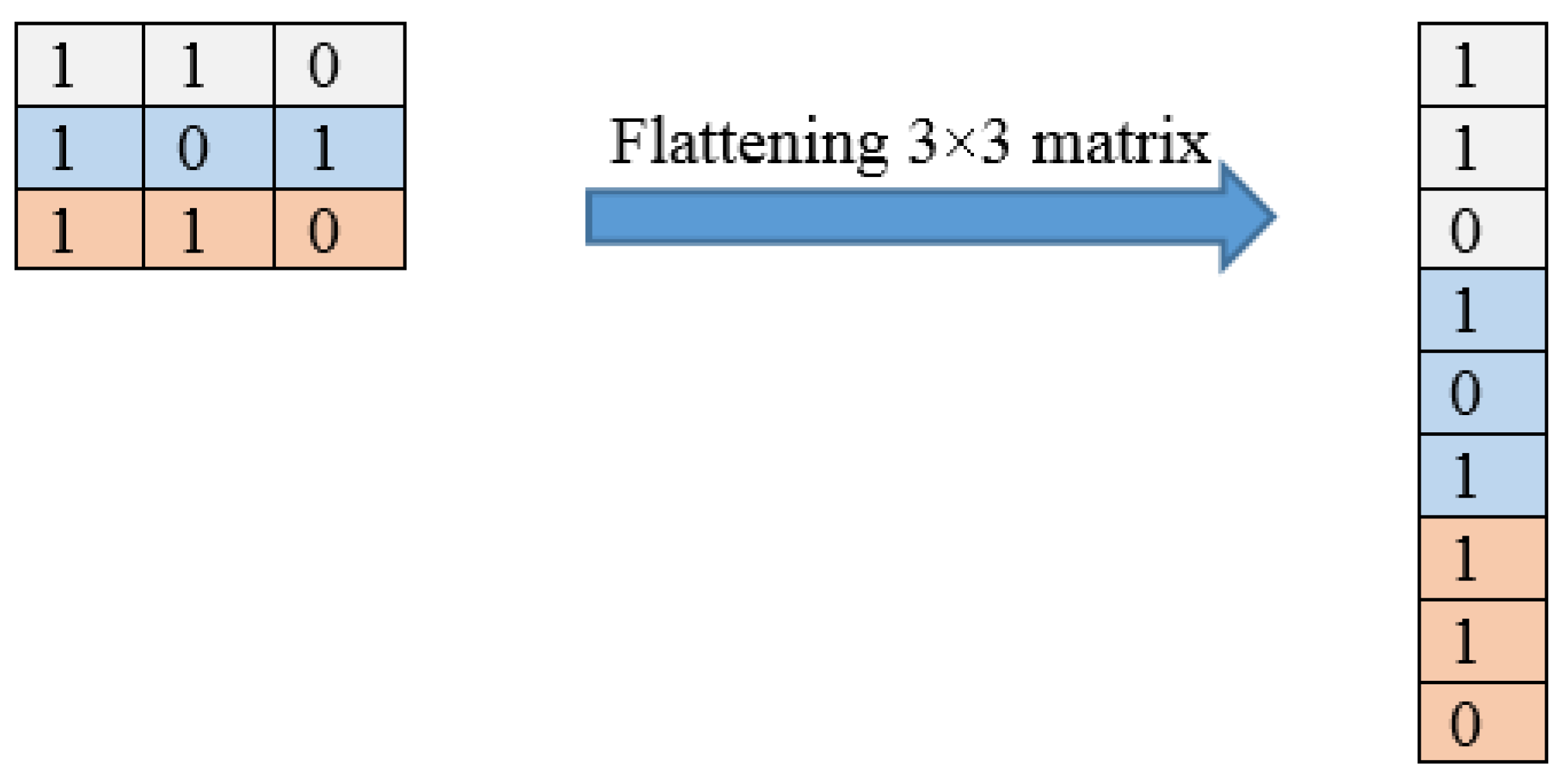
Figure 3 illustrates an example of the convolution operation with a 6 × 6 matrix using a stride of 2 and a 3 × 3 filter. The stride value defines the moving filter window of the input matrix. The pooling layer, which comes after the convolutional layer, is responsible for reducing the network computational loss; it is a fully connected layer where all neurons receive their inputs from the flattened form of the previous convolutional layer, as illustrated in
Figure 4. An example of a flattening operation is depicted in
Figure 5. In our study, some of the popular pooling functions considered were the average, L2 norm, minimum, and maximum functions. In addition, the output layer depends on the number of categories required to train the DL models. In our experiments, two different datasets were utilized: the CT scan dataset, which has a binary classification of COVID and non-COVID; and the chest X-ray dataset, which has a triple classification of COVID-19, normal, and pneumonia classes.
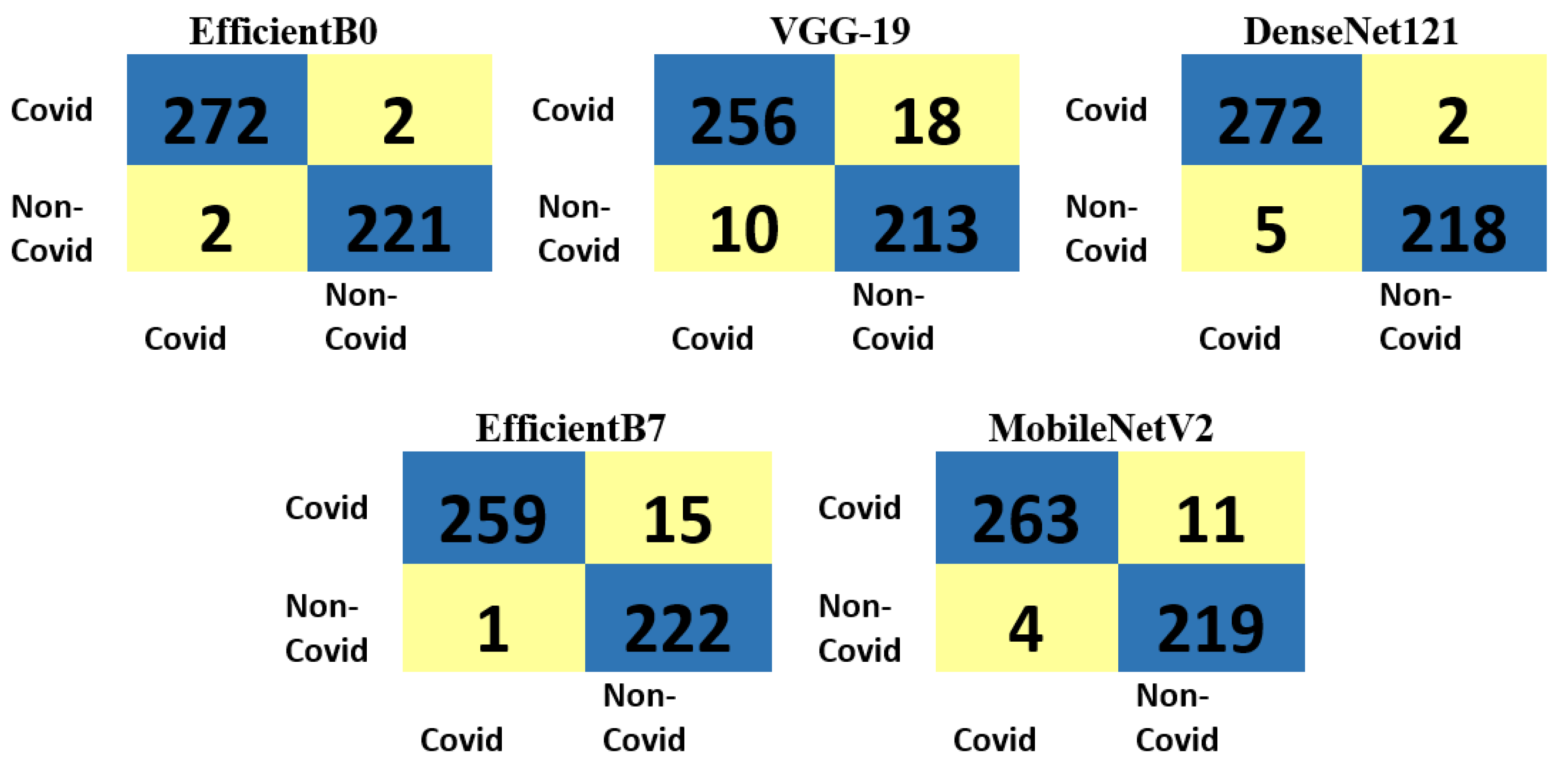
The proposed DL models consider the pretrained weights, which help in learning COVID-19 cases. Three main steps follow: in the first step, the training and test datasets for CT scan or chest X-ray images are prepared. Here, the first CT scan dataset was divided into a training set and testing set, and the training data samples were used to learn the utilized models. The split ratio for the training and testing sets was 978:274 for the COVID-19 class and 1006:223 for the non-COVID class, as presented in
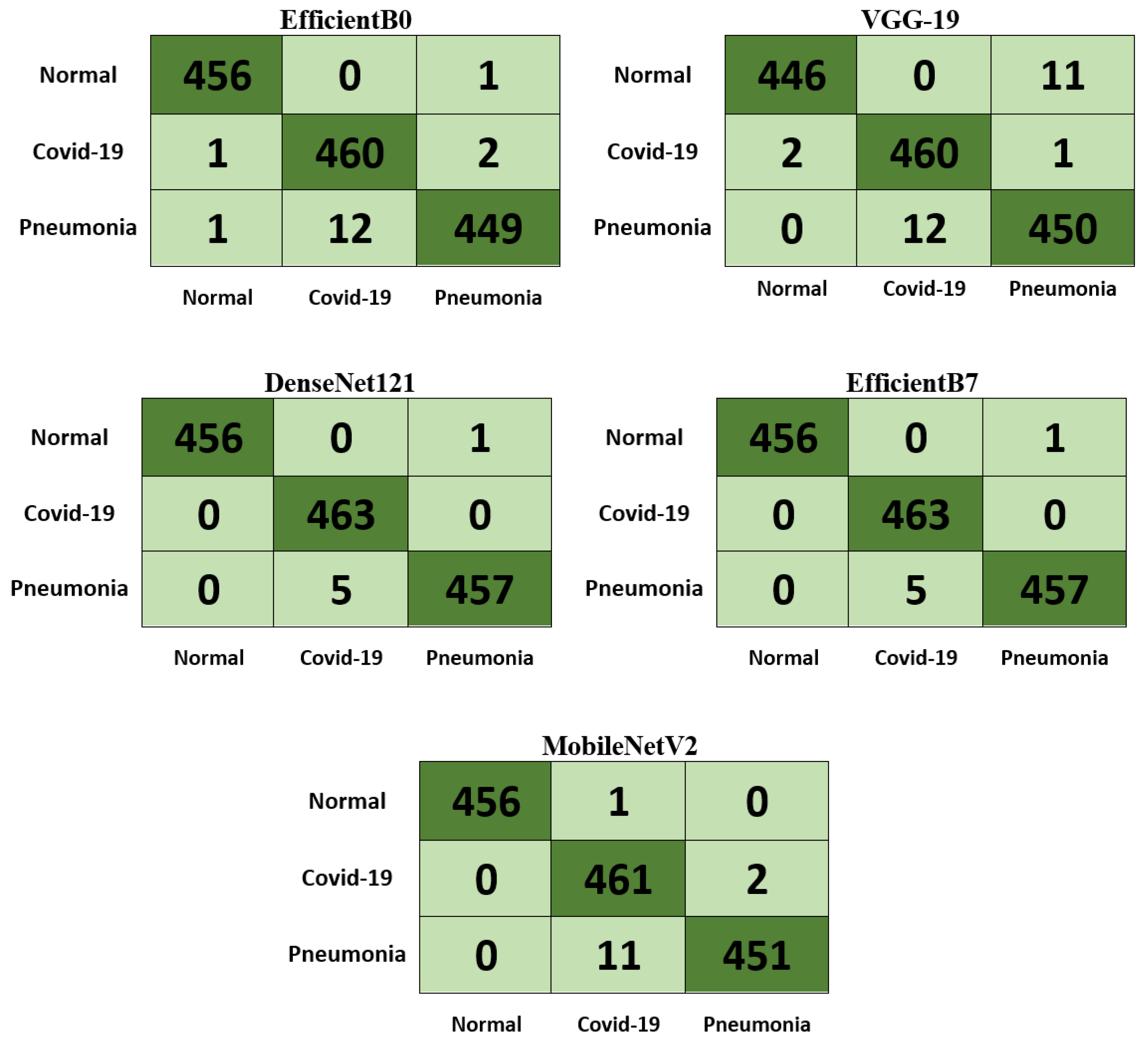
Table 1. Further, for the second chest X-ray dataset, there was an approximately equal distribution between COVID-19, normal, and pneumonia classes, with 1850 for training and 463 for testing, as reported in
Table 2.
In the second step, the base model and the new model are generated. Here, five main models with weights pretrained with ImageNet were used as the base models. The experiments were run many times with the intention of reaching the most suitable hyperparameters, which, in turn, would provide the best results.
Table 3 summarizes the hyperparameters for the different DL models used in this study, and
Table 4 presents the characteristics of the DL model architectures used in our experiments. Finally, in the third step, the trained weights are updated and then stored. Hence, once the forward propagation is completed, the binary cross-entropy loss function (Equation (4)) is calculated for the output layer.
where
y denotes the true value, and
p denotes the probability predicted by the model. Then, when the backpropagation process occurs, it counts the number of changes in the weights. Traveling forward and backward is called one epoch, and during one epoch one sample from the dataset is passed per batch size (BS).
5. Conclusions
In this study, two primary benchmark datasets for CT and X-ray images were used. All images were enhanced and preprocessed as part of the basic DL learning phase. COVID-19 images were classified as positive or negative using a set of fine-tuned transfer learning models. A set of deep learning models were trained and tested in this research study. For the CT scan dataset, all five models provided average accuracy greater than 95%, whereas, for the chest X-ray dataset, all models provided average accuracy greater than 95% except EfficientB7, which achieved 89.04% accuracy. Compared to the methods in the literature, the results show that MobileNetV2 surpassed the best method in terms of sensitivity, specificity, and accuracy, with a training run time of 117.43 s and testing run time of 0.77 s. In addition, DenseNet121 achieved the highest precision, specificity, F1-score, and accuracy for X-ray images with 99.57%, 99.78%, 99.56%, and 99.71% respectively. In the future, a prediction approach based on a combination of these DL models will be considered in order to improve the results. In addition, more complicated and larger datasets will be used for training to assess the robustness of the proposed approach. Moreover, using CT scans for COVID-19 detection may bring extra radiation to patients. In the future, we will consider the radiation dose issue in our proposed models.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}











