
Prospective Evaluation of Quantitative F-18-FDG-PET/CT for Pre-Operative Thoracic Lymph Node Staging in Patients with Lung Cancer as a Target for Computer-Aided Diagnosis

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. PET/CT Imaging
2.3. PET/CT Image Reconstruction
2.4. Quantification
2.5. Statistical Analyses
3. Results
3.1. SUV Measurements
3.2. ROC Analyses and Diagnostic Performance
3.3. Scoring System Adapted from Visual Reading Score
3.4. Dedicated Scoring System
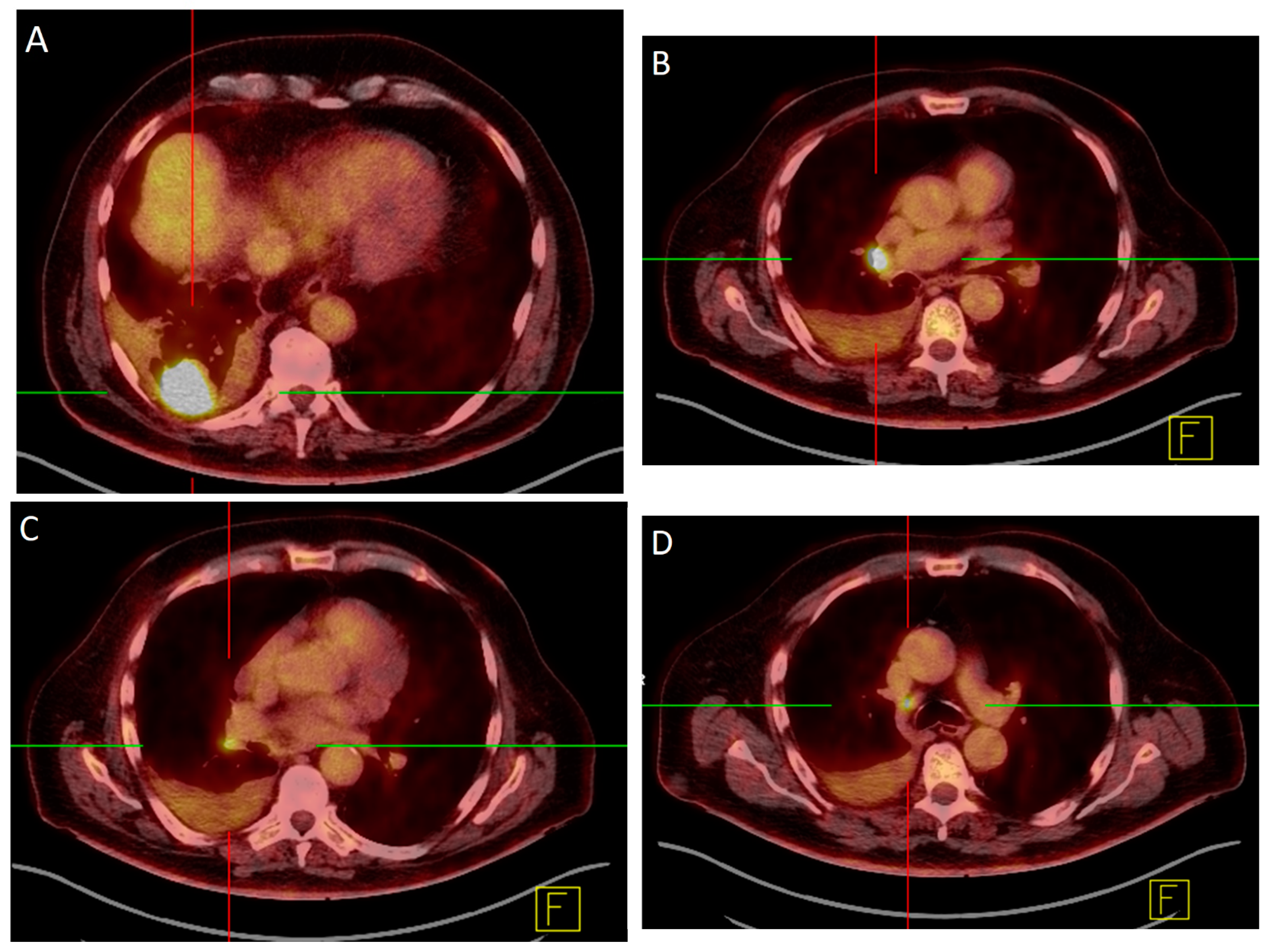
3.5. Patient Examples
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- De Leyn, P.; Dooms, C.; Kuzdzal, J.; Lardinois, D.; Passlick, B.; Rami-Porta, R.; Turna, A.; Van Schil, P.; Venuta, F.; Waller, D.; et al. Revised ESTS Guidelines for Preoperative Mediastinal Lymph Node Staging for Non-Small-Cell Lung Cancer. Eur. J. Cardio-Thorac. Surg. Off. J. Eur. Assoc. Cardio-Thorac. Surg. 2014, 45, 787–798. [Google Scholar] [CrossRef] [PubMed]
- Freixinet Gilart, J.; García, P.G.; de Castro, F.R.; Suárez, P.R.; Rodríguez, N.S.; de Ugarte, A.V. Extended Cervical Mediastinoscopy in the Staging of Bronchogenic Carcinoma. Ann. Thorac. Surg. 2000, 70, 1641–1643. [Google Scholar] [CrossRef] [PubMed]
- Nestle, U.; Schimek-Jasch, T.; Kremp, S.; Schaefer-Schuler, A.; Mix, M.; Küsters, A.; Tosch, M.; Hehr, T.; Eschmann, S.M.; Bultel, Y.-P.; et al. Imaging-Based Target Volume Reduction in Chemoradiotherapy for Locally Advanced Non-Small-Cell Lung Cancer (PET-Plan): A Multicentre, Open-Label, Randomised, Controlled Trial. Lancet Oncol. 2020, 21, 581–592. [Google Scholar] [CrossRef] [PubMed]
- Birim, O.; Kappetein, A.P.; Stijnen, T.; Bogers, A.J.J.C. Meta-Analysis of Positron Emission Tomographic and Computed Tomographic Imaging in Detecting Mediastinal Lymph Node Metastases in Nonsmall Cell Lung Cancer. Ann. Thorac. Surg. 2005, 79, 375–382. [Google Scholar] [CrossRef] [PubMed]
- Inoue, M.; Nakagawa, K.; Fujiwara, K.; Fukuhara, K.; Yasumitsu, T. Results of Preoperative Mediastinoscopy for Small Cell Lung Cancer. Ann. Thorac. Surg. 2000, 70, 1620–1623. [Google Scholar] [CrossRef]
- De Leyn, P.; Lardinois, D.; Van Schil, P.E.; Rami-Porta, R.; Passlick, B.; Zielinski, M.; Waller, D.A.; Lerut, T.; Weder, W. ESTS Guidelines for Preoperative Lymph Node Staging for Non-Small Cell Lung Cancer. Eur. J. Cardio-Thorac. Surg. Off. J. Eur. Assoc. Cardio-Thorac. Surg. 2007, 32, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Schmidt-Hansen, M.; Baldwin, D.R.; Hasler, E.; Zamora, J.; Abraira, V.; Roqué I Figuls, M. PET-CT for Assessing Mediastinal Lymph Node Involvement in Patients with Suspected Resectable Non-Small Cell Lung Cancer. Cochrane Database Syst. Rev. 2014, 2014, CD009519. [Google Scholar] [CrossRef]
- Mattes, M.D.; Moshchinsky, A.B.; Ahsanuddin, S.; Rizk, N.P.; Foster, A.; Wu, A.J.; Ashamalla, H.; Weber, W.A.; Rimner, A. Ratio of Lymph Node to Primary Tumor SUV on PET/CT Accurately Predicts Nodal Malignancy in Non-Small-Cell Lung Cancer. Clin. Lung Cancer 2015, 16, e253–e258. [Google Scholar] [CrossRef]
- Nguyen, P.; Bhatt, M.; Bashirzadeh, F.; Hundloe, J.; Ware, R.; Fielding, D.; Ravi Kumar, A.S. Comparison of Objective Criteria and Expert Visual Interpretation to Classify Benign and Malignant Hilar and Mediastinal Nodes on 18-F FDG PET/CT. Respirology 2015, 20, 129–137. [Google Scholar] [CrossRef] [Green Version]
- Juweid, M.E.; Stroobants, S.; Hoekstra, O.S.; Mottaghy, F.M.; Dietlein, M.; Guermazi, A.; Wiseman, G.A.; Kostakoglu, L.; Scheidhauer, K.; Buck, A.; et al. Use of Positron Emission Tomography for Response Assessment of Lymphoma: Consensus of the Imaging Subcommittee of International Harmonization Project in Lymphoma. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2007, 25, 571–578. [Google Scholar] [CrossRef] [Green Version]
- Rogasch, J.M.M.; Apostolova, I.; Steffen, I.G.; Steinkrüger, F.L.G.A.; Genseke, P.; Riedel, S.; Wertzel, H.; Achenbach, H.J.; Kalinski, T.; Schultz, M.; et al. Standardized Visual Reading of F18-FDG-PET in Patients with Non-Small Cell Lung Cancer Scheduled for Preoperative Thoracic Lymph Node Staging. Eur. J. Radiol. 2016, 85, 1345–1350. [Google Scholar] [CrossRef] [PubMed]
- Rogasch, J.M.M.; Steffen, I.G.; Riedel, S.; Apostolova, I.; Wertzel, H.; Achenbach, H.J.; Steinkrüger, F.L.G.A.; Kalinski, T.; Schultz, M.; Schreiber, J.; et al. Dual Time Point Imaging for F18-FDG-PET/CT Does Not Improve the Accuracy of Nodal Staging in Non-Small Cell Lung Cancer Patients. Eur. Radiol. 2016, 26, 2808–2818. [Google Scholar] [CrossRef] [PubMed]
- Hellwig, D.; Graeter, T.P.; Ukena, D.; Groeschel, A.; Sybrecht, G.W.; Schaefers, H.-J.; Kirsch, C.-M. 18F-FDG PET for Mediastinal Staging of Lung Cancer: Which SUV Threshold Makes Sense? J. Nucl. Med. 2007, 48, 1761–1766. [Google Scholar] [CrossRef] [Green Version]
- Perigaud, C.; Bridji, B.; Roussel, J.C.; Sagan, C.; Mugniot, A.; Duveau, D.; Baron, O.; Despins, P. Prospective Preoperative Mediastinal Lymph Node Staging by Integrated Positron Emission Tomography-Computerised Tomography in Patients with Non-Small-Cell Lung Cancer. Eur. J. Cardio-Thorac. Surg. Off. J. Eur. Assoc. Cardio-Thorac. Surg. 2009, 36, 731–736. [Google Scholar] [CrossRef] [Green Version]
- Boellaard, R.; Delgado-Bolton, R.; Oyen, W.J.G.; Giammarile, F.; Tatsch, K.; Eschner, W.; Verzijlbergen, F.J.; Barrington, S.F.; Pike, L.C.; Weber, W.A.; et al. FDG PET/CT: EANM Procedure Guidelines for Tumour Imaging: Version 2.0. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 328–354. [Google Scholar] [CrossRef] [PubMed]
- Mountain, C.F.; Dresler, C.M. Regional Lymph Node Classification for Lung Cancer Staging. Chest 1997, 111, 1718–1723. [Google Scholar] [CrossRef]
- Suárez-Piñera, M.; Belda-Sanchis, J.; Taus, A.; Sánchez-Font, A.; Mestre-Fusco, A.; Jiménez, M.; Pijuan, L. FDG PET-CT SUVmax and IASLC/ATS/ERS Histologic Classification: A New Profile of Lung Adenocarcinoma with Prognostic Value. Am. J. Nucl. Med. Mol. Imaging 2018, 8, 100–109. [Google Scholar]
- Rau, C.-S.; Kuo, P.-J.; Chien, P.-C.; Huang, C.-Y.; Hsieh, H.-Y.; Hsieh, C.-H. Mortality Prediction in Patients with Isolated Moderate and Severe Traumatic Brain Injury Using Machine Learning Models. PLoS ONE 2018, 13, e0207192. [Google Scholar] [CrossRef] [Green Version]
- Ramos, L.A.; van der Steen, W.E.; Sales Barros, R.; Majoie, C.B.L.M.; van den Berg, R.; Verbaan, D.; Vandertop, W.P.; Zijlstra, I.J.A.J.; Zwinderman, A.H.; Strijkers, G.J.; et al. Machine Learning Improves Prediction of Delayed Cerebral Ischemia in Patients with Subarachnoid Hemorrhage. J. Neurointerv. Surg. 2019, 11, 497–502. [Google Scholar] [CrossRef]
- Lee, H.-C.; Yoon, S.B.; Yang, S.-M.; Kim, W.H.; Ryu, H.-G.; Jung, C.-W.; Suh, K.-S.; Lee, K.H. Prediction of Acute Kidney Injury after Liver Transplantation: Machine Learning Approaches vs. Logistic Regression Model. J. Clin. Med. 2018, 7, 428. [Google Scholar] [CrossRef] [Green Version]
- Tseng, H.-H.; Wei, L.; Cui, S.; Luo, Y.; Ten Haken, R.K.; El Naqa, I. Machine Learning and Imaging Informatics in Oncology. Oncology 2020, 98, 344–362. [Google Scholar] [CrossRef] [PubMed]
- Cho, J.; Choe, J.G.; Pahk, K.; Choi, S.; Kwon, H.R.; Eo, J.S.; Seo, H.J.; Kim, C.; Kim, S. Ratio of Mediastinal Lymph Node SUV to Primary Tumor SUV in (18)F-FDG PET/CT for Nodal Staging in Non-Small-Cell Lung Cancer. Nucl. Med. Mol. Imaging 2017, 51, 140–146. [Google Scholar] [CrossRef] [PubMed]
- Vesselle, H.; Salskov, A.; Turcotte, E.; Wiens, L.; Schmidt, R.; Jordan, C.D.; Vallières, E.; Wood, D.E. Relationship between Non-Small Cell Lung Cancer FDG Uptake at PET, Tumor Histology, and Ki-67 Proliferation Index. J. Thorac. Oncol. Off. Publ. Int. Assoc. Study Lung Cancer 2008, 3, 971–978. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tournoy, K.G.; Maddens, S.; Gosselin, R.; Van Maele, G.; van Meerbeeck, J.P.; Kelles, A. Integrated FDG-PET/CT Does Not Make Invasive Staging of the Intrathoracic Lymph Nodes in Non-Small Cell Lung Cancer Redundant: A Prospective Study. Thorax 2007, 62, 696–701. [Google Scholar] [CrossRef] [Green Version]
- Kubota, K.; Watanabe, H.; Murata, Y.; Yukihiro, M.; Ito, K.; Morooka, M.; Minamimoto, R.; Hori, A.; Shibuya, H. Effects of Blood Glucose Level on FDG Uptake by Liver: A FDG-PET/CT Study. Nucl. Med. Biol. 2011, 38, 347–351. [Google Scholar] [CrossRef]
- Eskian, M.; Alavi, A.; Khorasanizadeh, M.; Viglianti, B.L.; Jacobsson, H.; Barwick, T.D.; Meysamie, A.; Yi, S.K.; Iwano, S.; Bybel, B.; et al. Effect of Blood Glucose Level on Standardized Uptake Value (SUV) in (18)F- FDG PET-Scan: A Systematic Review and Meta-Analysis of 20,807 Individual SUV Measurements. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 224–237. [Google Scholar] [CrossRef] [Green Version]
- Kreissl, M.C.; Stout, D.B.; Wong, K.-P.; Wu, H.-M.; Caglayan, E.; Ladno, W.; Zhang, X.; Prior, J.O.; Reiners, C.; Huang, S.-C.; et al. Influence of Dietary State and Insulin on Myocardial, Skeletal Muscle and Brain [F]-Fluorodeoxyglucose Kinetics in Mice. EJNMMI Res. 2011, 1, 8. [Google Scholar] [CrossRef] [Green Version]
- Busk, M.; Munk, O.L.; Jakobsen, S.; Frøkiær, J.; Overgaard, J.; Horsman, M.R. FDG-PET Reproducibility in Tumor-Bearing Mice: Comparing a Traditional SUV Approach with a Tumor-to-Brain Tissue Ratio Approach. Acta Oncol. 2017, 56, 706–712. [Google Scholar] [CrossRef] [Green Version]
- Viglianti, B.L.; Wong, K.K.; Wimer, S.M.; Parameswaran, A.; Nan, B.; Ky, C.; Townsend, D.M.; Rubello, D.; Frey, K.A.; Gross, M.D. Effect of Hyperglycemia on Brain and Liver (18)F-FDG Standardized Uptake Value (FDG SUV) Measured by Quantitative Positron Emission Tomography (PET) Imaging. Biomed. Pharmacother. 2017, 88, 1038–1045. [Google Scholar] [CrossRef] [Green Version]
- Britz-Cunningham, S.H.; Millstine, J.W.; Gerbaudo, V.H. Improved Discrimination of Benign and Malignant Lesions on FDG PET/CT, Using Comparative Activity Ratios to Brain, Basal Ganglia, or Cerebellum. Clin. Nucl. Med. 2008, 33, 681–687. [Google Scholar] [CrossRef]
- Jones, H.A.; Marino, P.S.; Shakur, B.H.; Morrell, N.W. In Vivo Assessment of Lung Inflammatory Cell Activity in Patients with COPD and Asthma. Eur. Respir. J. 2003, 21, 567–573. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tessler, F.N.; Middleton, W.D.; Grant, E.G.; Hoang, J.K.; Berland, L.L.; Teefey, S.A.; Cronan, J.J.; Beland, M.D.; Desser, T.S.; Frates, M.C.; et al. ACR Thyroid Imaging, Reporting and Data System (TI-RADS): White Paper of the ACR TI-RADS Committee. J. Am. Coll. Radiol. 2017, 14, 587–595. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Lymph node/primary | SUVmax lymph node/SUVmax primary |
| Lymph node/liver | SUVmax lymph node/SUVmax liver |
| Lymph node/brainstem | SUVmax lymph node/SUVmax brainstem |
| Lymph node/lung | SUVmax lymph node/SUVmax healthy lung tissue |
| Benign | Malign | |
|---|---|---|
| SUVmax | 3.45 (1.14–19.00) | 11.00 (2.35–35.55) |
| p < 0.05 | ||
| Lymph node/primary | 0.22 (0.06–1.27) | 0.75 (0.13–2.42) |
| p < 0.05 | ||
| Lymph node/liver | 0.92 (0.28–4.42) | 3.18 (0.63–11.19) |
| p < 0.05 | ||
| Lymph node/brainstem | 0.52 (0.14–3.88) | 1.63 (0.51–8.46) |
| p < 0.05 | ||
| Lymph node/lung | 3.47 (1.08–19.00) | 14.67 (4.60–50.61) |
| p < 0.05 | ||
| Cut-Off (p < 0.001) | AUC | Sens | Spez | PPV | NPV | Acc | |
|---|---|---|---|---|---|---|---|
| SUVmax | 5.495 | 0.92 (CI: 0.85–0.98) | 89.67% | 88.89% | 76.47% | 95.52% | 89.11% |
| Lymph node/primary | 0.457 | 0.86 (CI: 0.78–0.94) | 79.31% | 80.56% | 62.16% | 90.63% | 80.20% |
| Lymph node/liver | 1.374 | 0.91 (CI: 0.85–0.98) | 89.66% | 81.94% | 66.67% | 95.16% | 84.16% |
| Lymph node/brainstem | 0.749 | 0.88 (CI: 0.81–0.95) | 82.76% | 77.78% | 60.00% | 91.80% | 79.21% |
| Lymph node/healthy lung | 4.593 | 0.94 (CI: 0.89–0.98) | 100% | 73.61% | 60.42% | 100% | 81.89% |
| Adapted visual score | ≥3 | 0.81 (CI: 0.72–0.89) | 34.48% | 95.83% | 76.92% | 78.41% | 78.22% |
| Score | ≥3 | 0.93 (CI: 0.88–0.98) | 89.66% | 86.11% | 72.22% | 95.38% | 87.13% |
| ·· | PET Neg | PET Pos | |
|---|---|---|---|
| SUVmax; cut-off 5.495 | Histo neg | 64 | 8 |
| Histo pos | 3 | 26 | |
| Lymph node/primary; cut-off 0.457 | ·· | PET neg | PET pos |
| Histo neg | 58 | 14 | |
| Histo pos | 6 | 23 | |
| Lymph node/liver; cut-off 1.374 | ·· | PET neg | PET pos |
| Histo neg | 59 | 13 | |
| Histo pos | 3 | 26 | |
| Lymph node/brainstem; cut-off 0.749 | ·· | PET neg | PET pos |
| Histo neg | 56 | 16 | |
| Histo pos | 5 | 24 | |
| Lymph node/lung; cut-off 4.593 | ·· | PET neg | PET pos |
| Histo neg | 53 | 19 | |
| Histo pos | 0 | 29 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Genseke, P.; Wielenberg, C.F.; Schreiber, J.; Luecke, E.; Frese, S.; Walles, T.; Kreissl, M.C. Prospective Evaluation of Quantitative F-18-FDG-PET/CT for Pre-Operative Thoracic Lymph Node Staging in Patients with Lung Cancer as a Target for Computer-Aided Diagnosis. Diagnostics 2023, 13, 1263. https://doi.org/10.3390/diagnostics13071263
Genseke P, Wielenberg CF, Schreiber J, Luecke E, Frese S, Walles T, Kreissl MC. Prospective Evaluation of Quantitative F-18-FDG-PET/CT for Pre-Operative Thoracic Lymph Node Staging in Patients with Lung Cancer as a Target for Computer-Aided Diagnosis. Diagnostics. 2023; 13(7):1263. https://doi.org/10.3390/diagnostics13071263
Chicago/Turabian StyleGenseke, Philipp, Christoph Ferdinand Wielenberg, Jens Schreiber, Eva Luecke, Steffen Frese, Thorsten Walles, and Michael Christoph Kreissl. 2023. "Prospective Evaluation of Quantitative F-18-FDG-PET/CT for Pre-Operative Thoracic Lymph Node Staging in Patients with Lung Cancer as a Target for Computer-Aided Diagnosis" Diagnostics 13, no. 7: 1263. https://doi.org/10.3390/diagnostics13071263