

Development and Validation of a Novel Prognostic Tool to Predict Recurrence of Paroxysmal Atrial Fibrillation after the First-Time Catheter Ablation: A Retrospective Cohort Study


Abstract
:1. Introduction
2. Materials and Methods
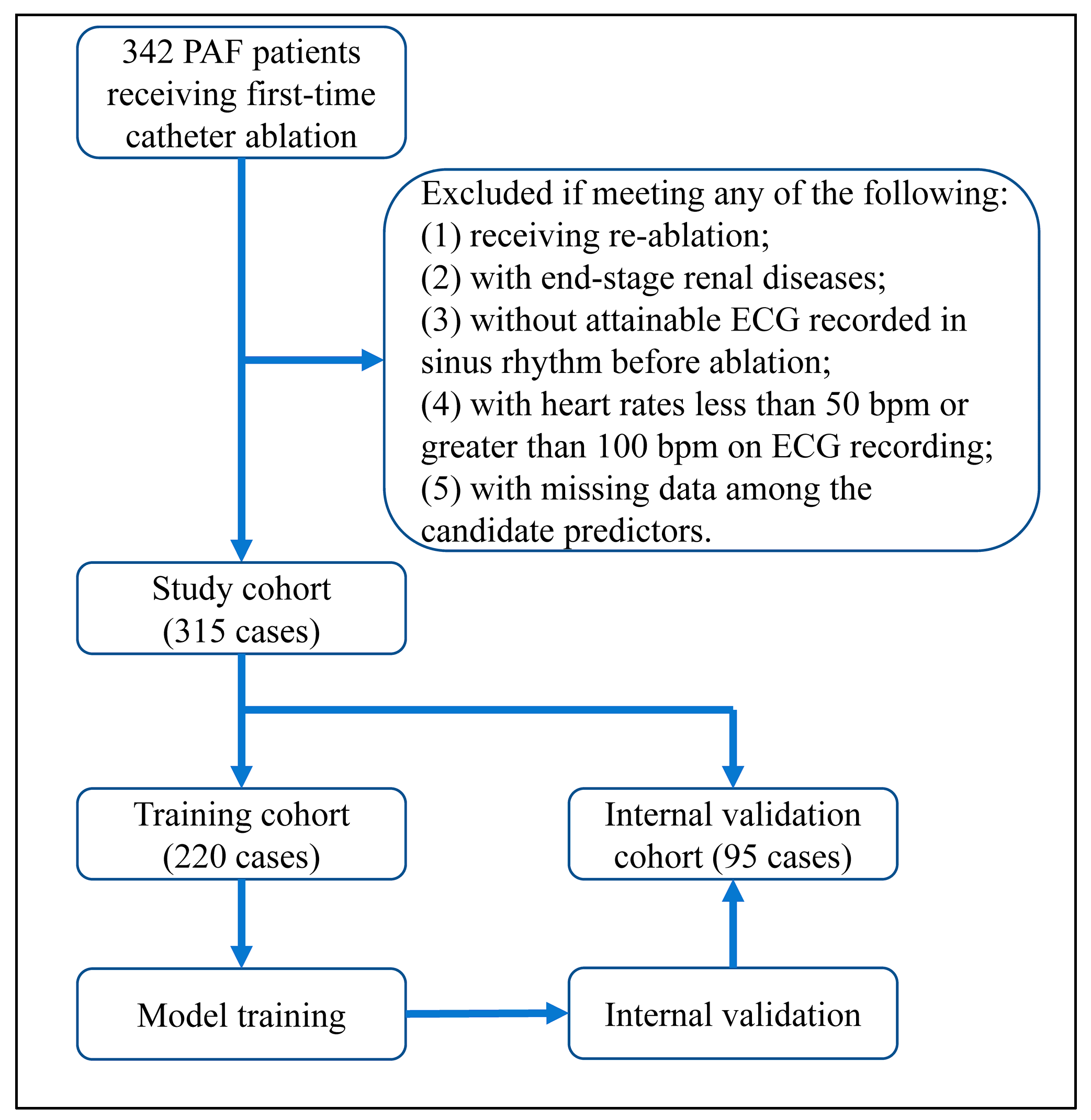
2.1. Inclusion and Exclusion
2.2. Ablation Procedure
2.3. Observation
2.4. Baseline Characteristics
2.5. Candidate Predictors
2.6. Model Construction and Assessment
2.7. Statistical Analyses
3. Results
3.1. Baseline Characteristics and Categorization of Continuous Variables
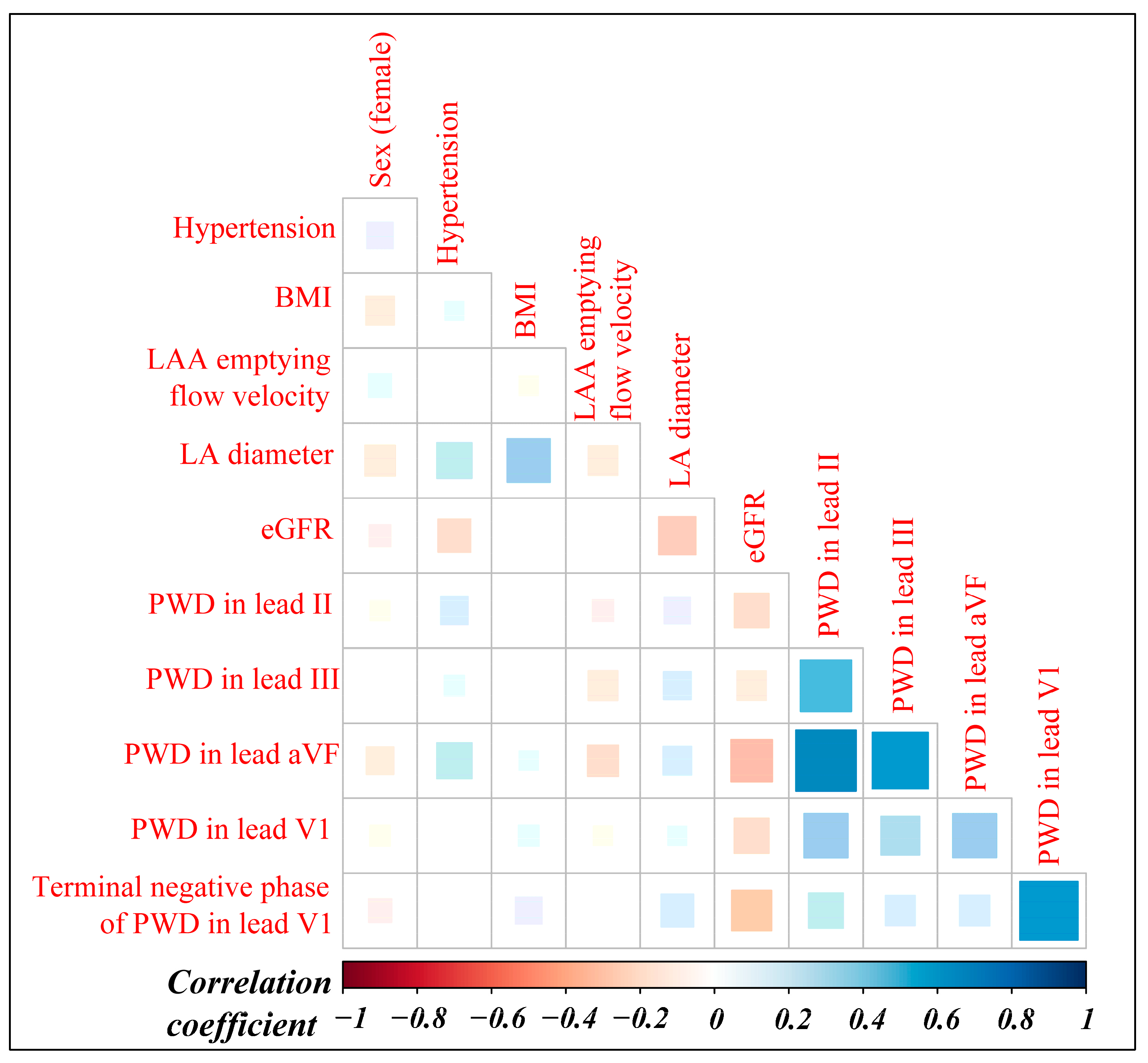
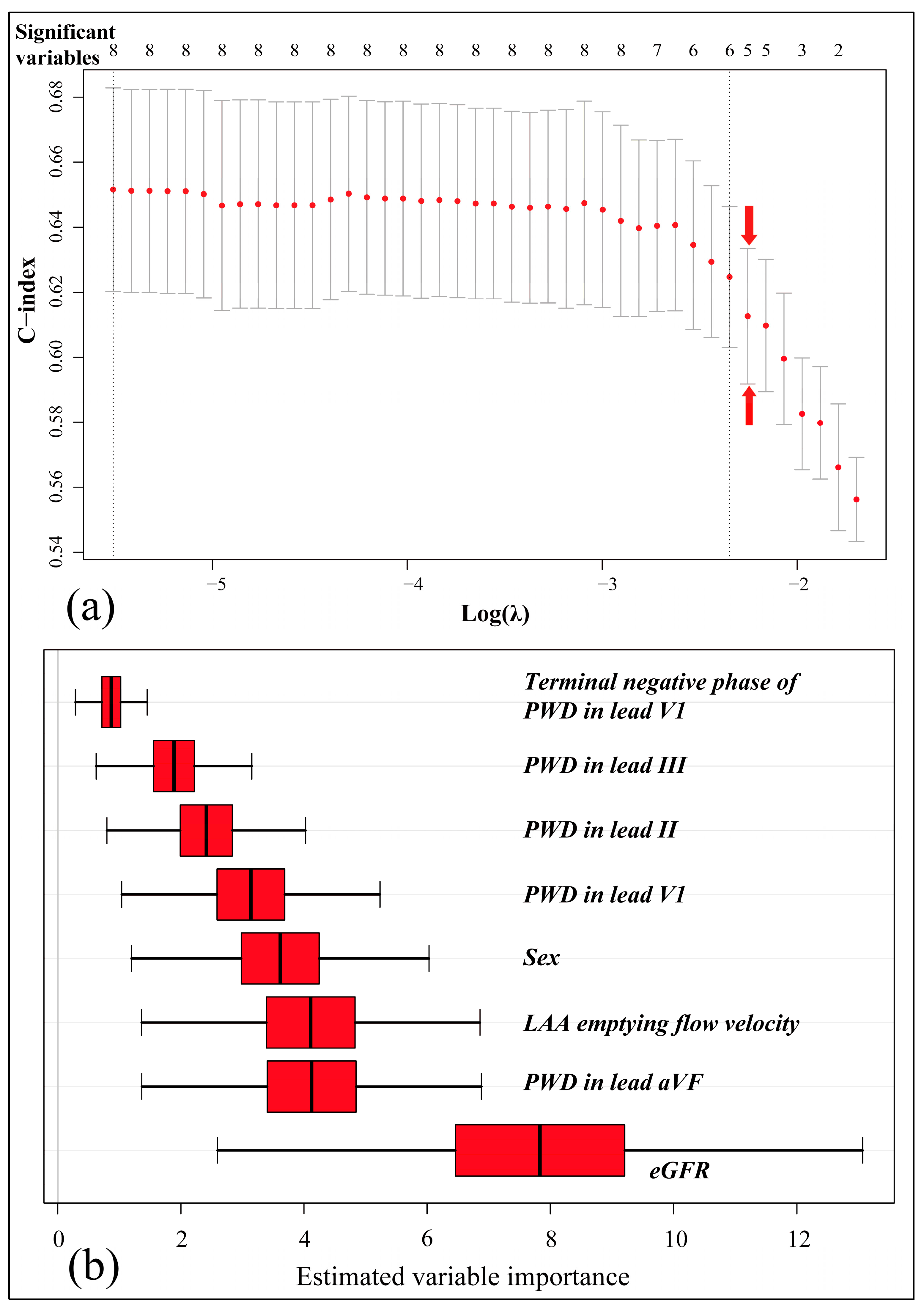
3.2. Variable Selection and Model Construction
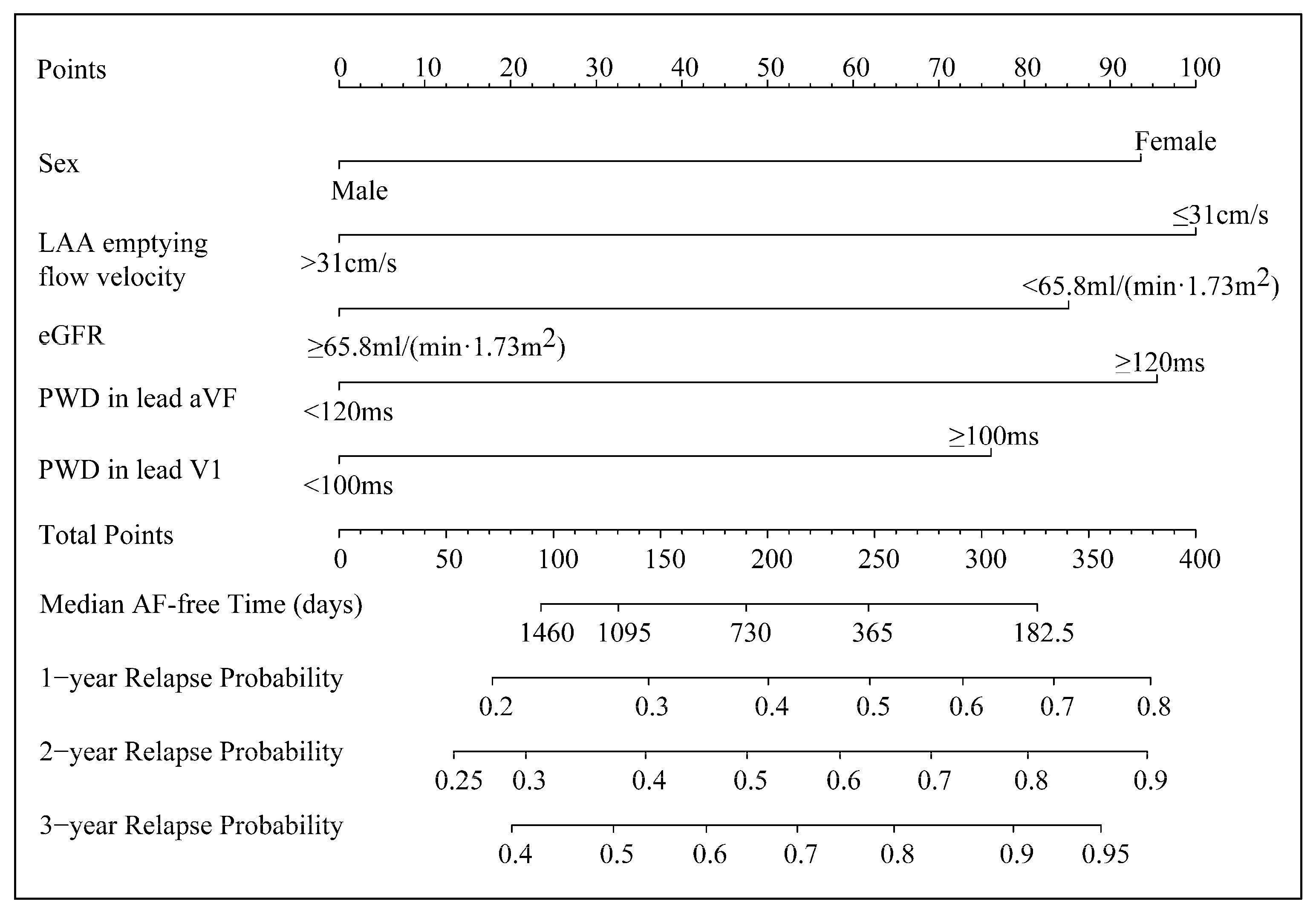
3.3. The Five-Factor Nomogram and Its Application
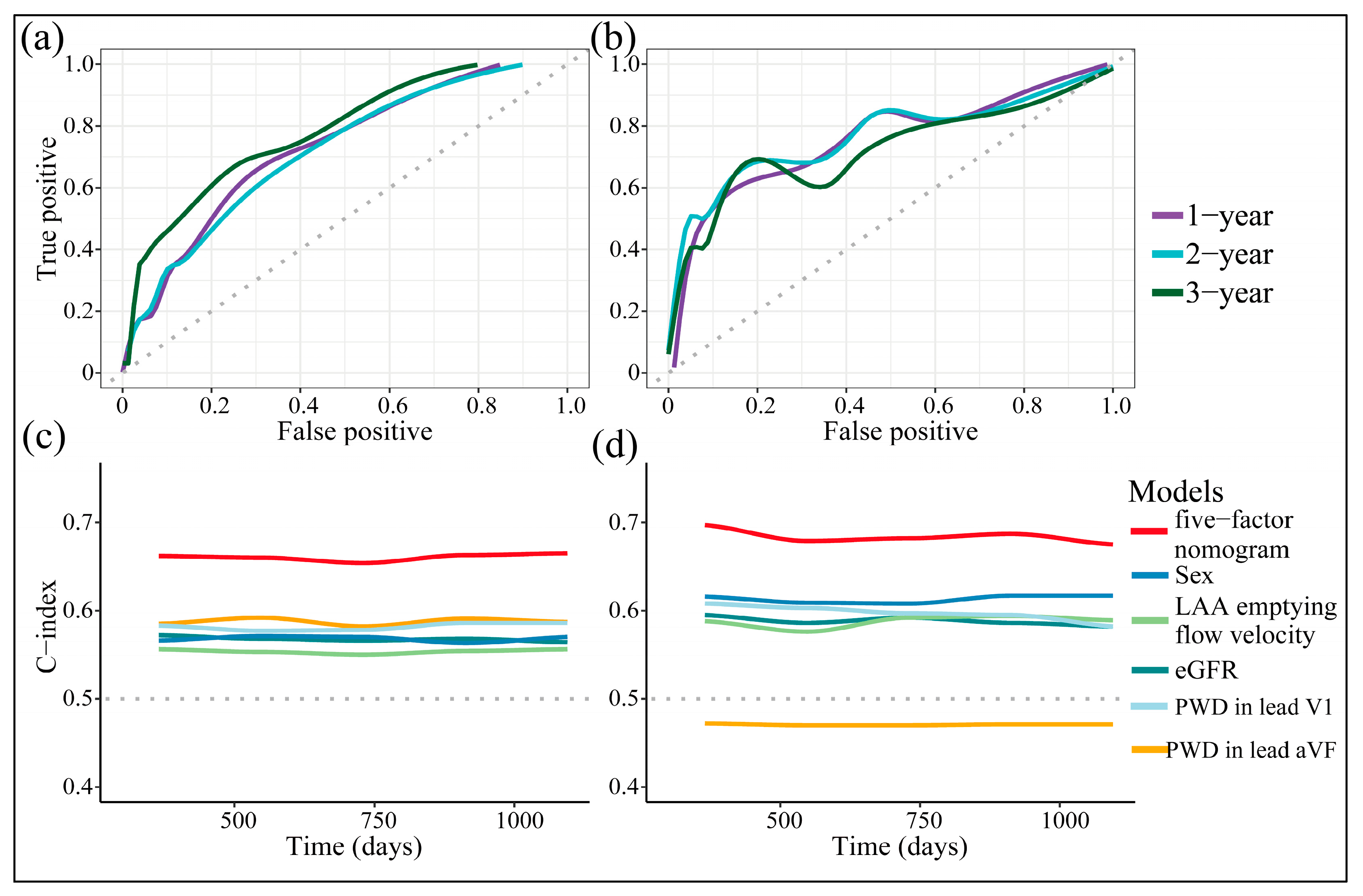
3.4. Discriminative Power
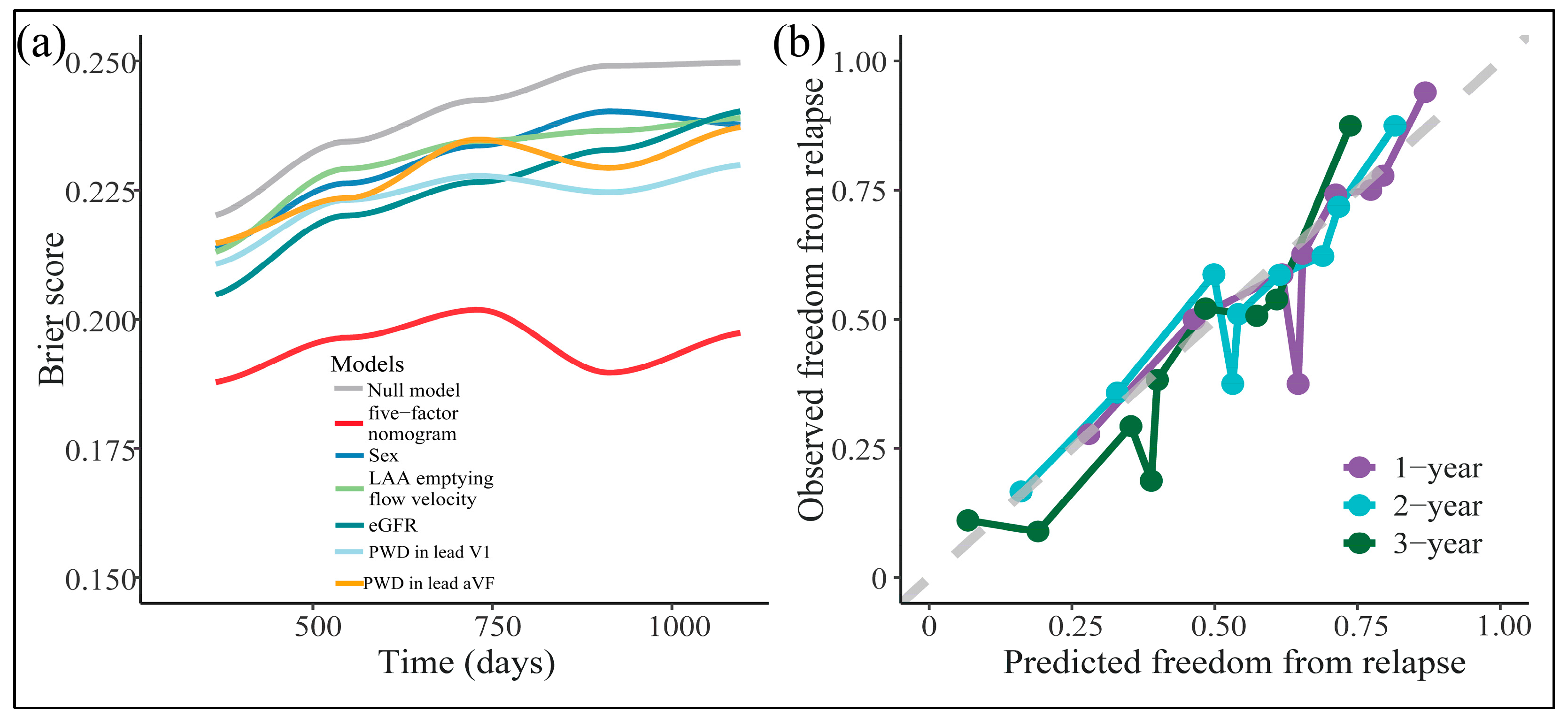
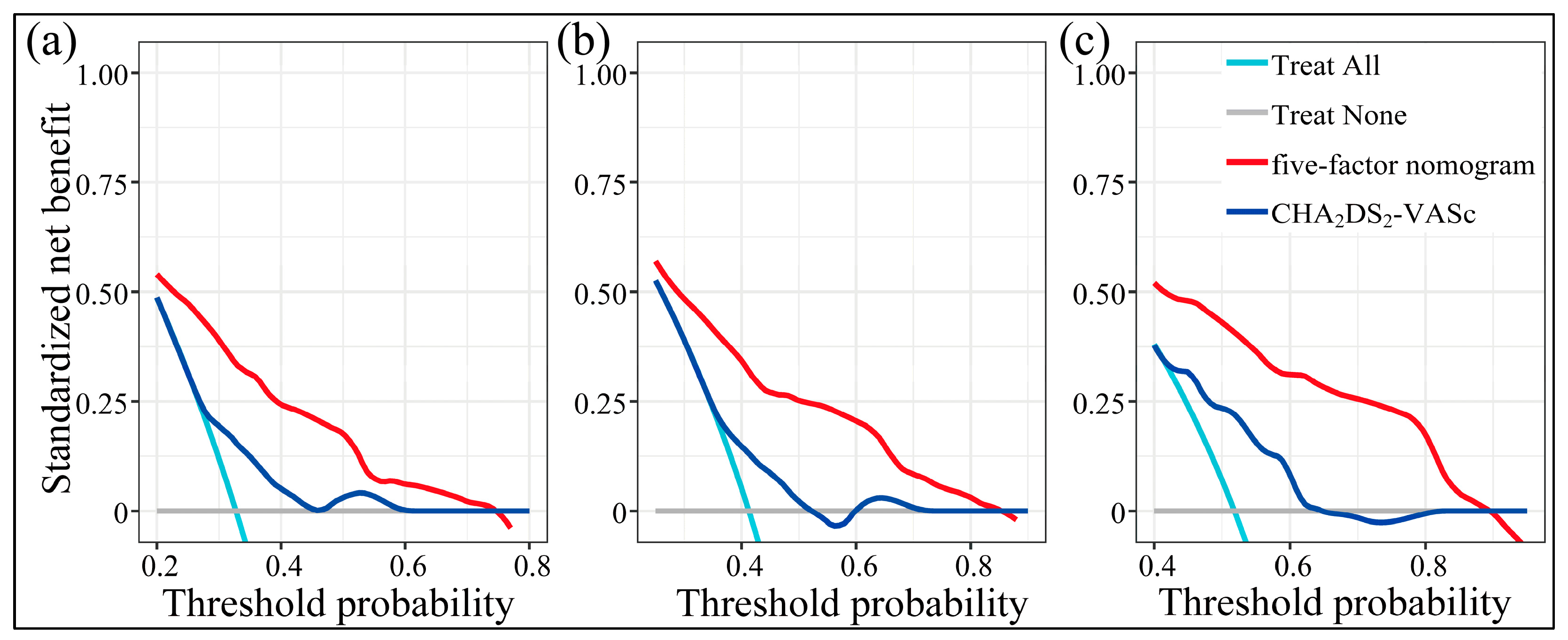
3.5. The Goodness-of-Fit, Calibration, and Clinical Utility
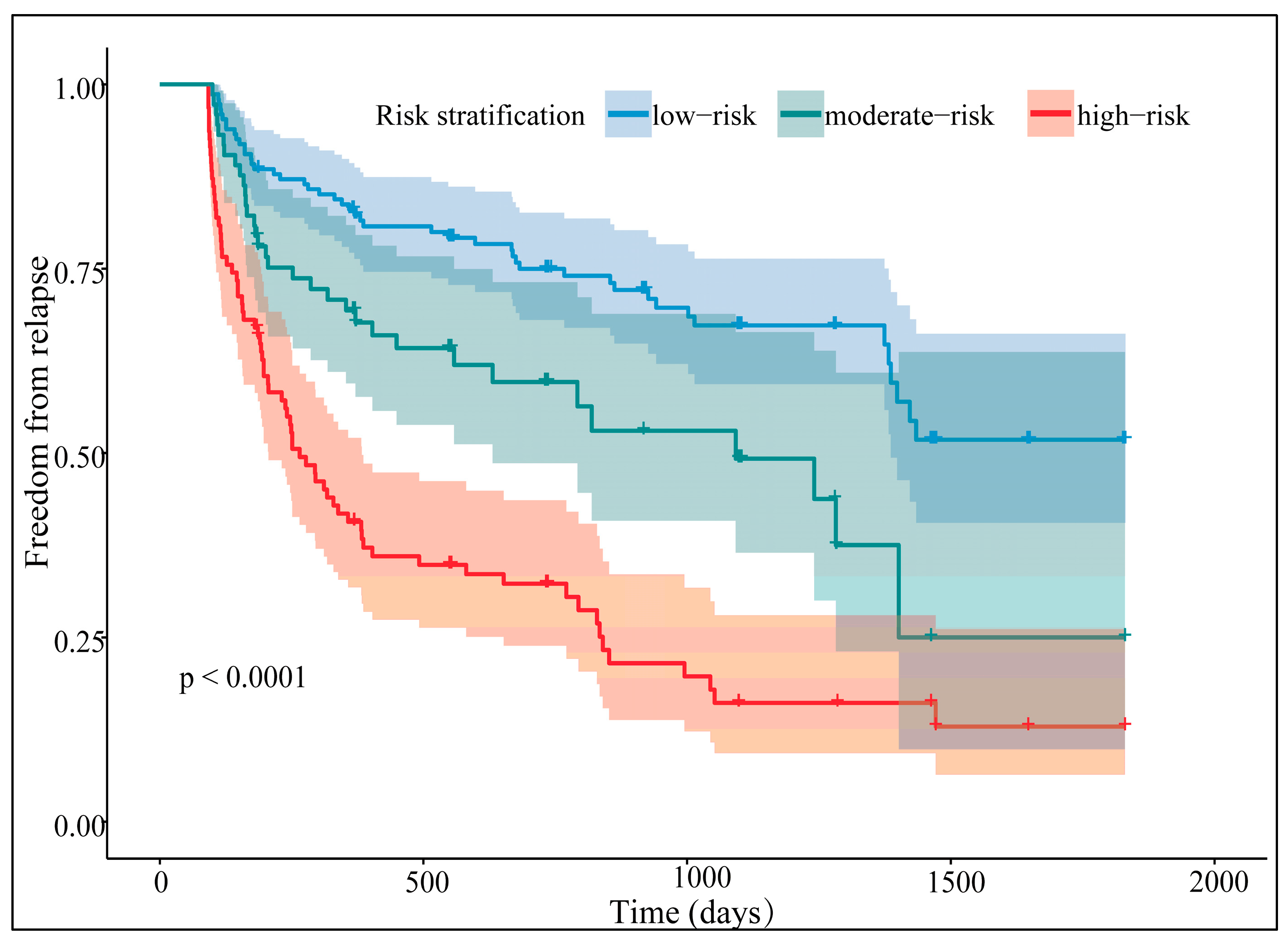
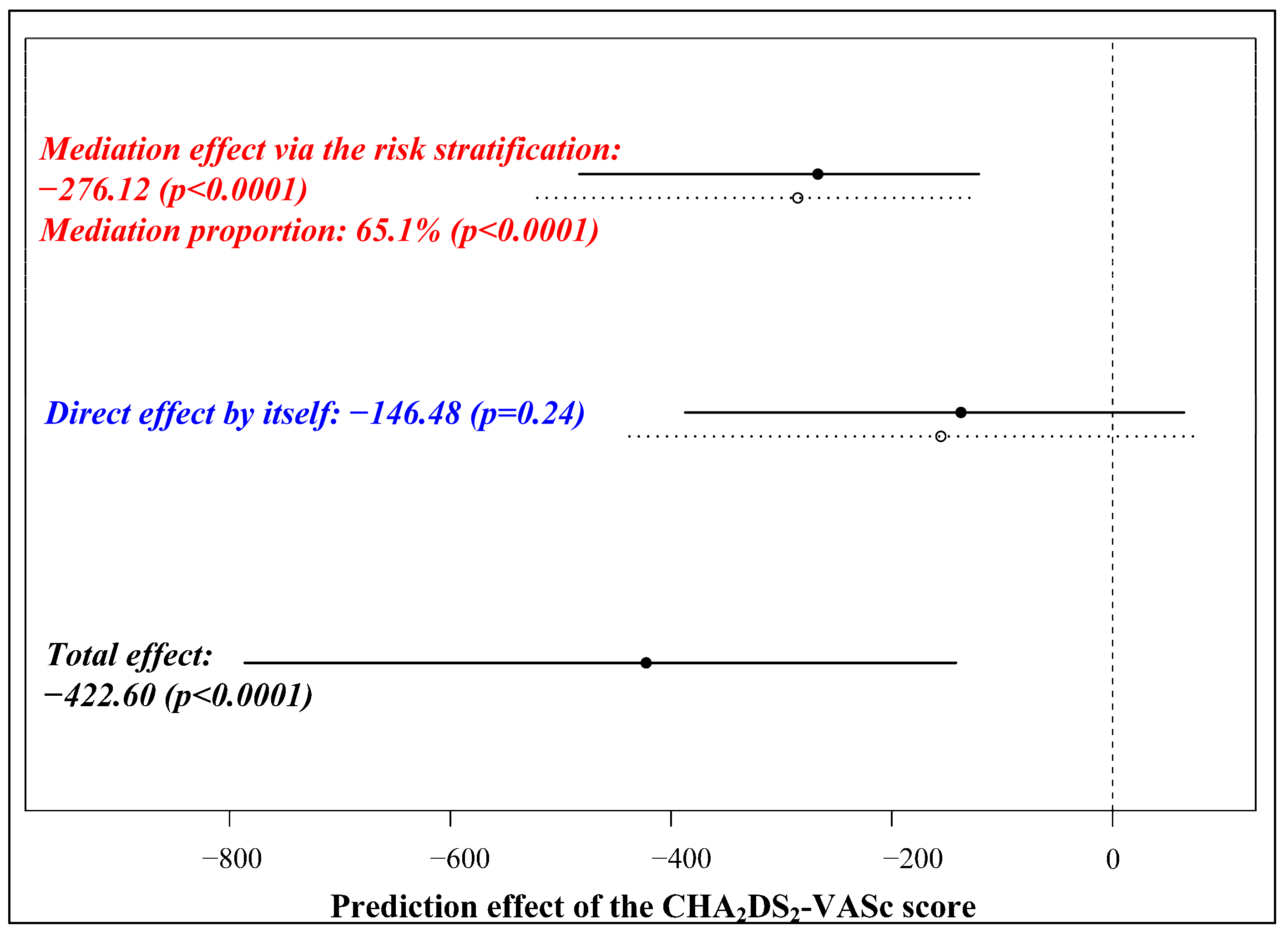
3.6. Risk Stratification and Its Separative Efficacy
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Andrade, J.; Khairy, P.; Dobrev, D.; Nattel, S. The clinical profile and pathophysiology of atrial fibrillation: Relationships among clinical features, epidemiology, and mechanisms. Circ. Res. 2014, 114, 1453–1468. [Google Scholar] [CrossRef] [PubMed]
- Wilber, D.J.; Pappone, C.; Neuzil, P.; De Paola, A.; Marchlinski, F.; Natale, A.; Macle, L.; Daoud, E.G.; Calkins, H.; Hall, B.; et al. Comparison of Antiarrhythmic Drug Therapy and Radiofrequency Catheter Ablation in Patients with Paroxysmal Atrial Fibrillation: A randomized controlled trial. JAMA 2010, 303, 333–340. [Google Scholar] [CrossRef] [PubMed]
- Packer, D.L.; Kowal, R.C.; Wheelan, K.R.; Irwin, J.M.; Champagne, J.; Guerra, P.G.; Dubuc, M.; Reddy, V.; Nelson, L.; Holcomb, R.G.; et al. Cryoballoon Ablation of Pulmonary Veins for Paroxysmal Atrial Fibrillation. J. Am. Coll. Cardiol. 2013, 61, 1713–1723. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andrade, J.G.; Macle, L.; Verma, A.; Deyell, M.W.; Champagne, J.; Dubuc, M.; Leong-Sit, P.; Novak, P.; Roux, J.-F.; Sapp, J.; et al. Quality of Life and Health Care Utilization in the CIRCA-DOSE Study. JACC Clin. Electrophysiol. 2020, 6, 935–944. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, J.C.; Johannessen, A.; Raatikainen, P.; Hindricks, G.; Walfridsson, H.; Kongstad, O.; Pehrson, S.; Englund, A.; Hartikainen, J.; Mortensen, L.S.; et al. Radiofrequency Ablation as Initial Therapy in Paroxysmal Atrial Fibrillation. N. Engl. J. Med. 2012, 367, 1587–1595. [Google Scholar] [CrossRef] [Green Version]
- Andrade, J.G.; Wells, G.A.; Deyell, M.W.; Bennett, M.; Essebag, V.; Champagne, J.; Roux, J.-F.; Yung, D.; Skanes, A.; Khaykin, Y.; et al. Cryoablation or Drug Therapy for Initial Treatment of Atrial Fibrillation. N. Engl. J. Med. 2021, 384, 305–315. [Google Scholar] [CrossRef]
- Parkash, R.; Tang, A.S.; Sapp, J.L.; Wells, G. Approach to the Catheter Ablation Technique of Paroxysmal and Persistent Atrial Fibrillation: A Meta-Analysis of the Randomized Controlled Trials. J. Cardiovasc. Electrophysiol. 2011, 22, 729–738. [Google Scholar] [CrossRef]
- Pranata, R.; Yonas, E.; Vania, R. Prolonged P-wave duration in sinus rhythm pre-ablation is associated with atrial fibrillation recurrence after pulmonary vein isolation—A systematic review and meta-analysis. Ann. Noninvasive Electrocardiol. 2019, 24, e12653. [Google Scholar] [CrossRef] [Green Version]
- Bajraktari, G.; Bytyçi, I.; Henein, M.Y. Left atrial structure and function predictors of recurrent fibrillation after catheter ablation: A systematic review and meta-analysis. Clin. Physiol. Funct. Imaging 2019, 40, 1–13. [Google Scholar] [CrossRef]
- Han, S.; Liu, M.; Jia, R.; Cen, Z.; Guo, R.; Liu, G.; Cui, K. Left atrial appendage function and structure predictors of recurrent atrial fibrillation after catheter ablation: A meta-analysis of observational studies. Front. Cardiovasc. Med. 2022, 9, 1009494. [Google Scholar] [CrossRef]
- Lin, K.J.; Cho, S.I.; Tiwari, N.; Bergman, M.; Kizer, J.R.; Palma, E.C.; Taub, C.C. Impact of metabolic syndrome on the risk of atrial fibrillation recurrence after catheter ablation: Systematic review and meta-analysis. J. Interv. Card. Electrophysiol. 2013, 39, 211–223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Winkle, R.A.; Mead, R.H.; Engel, G.; Kong, M.H.; Fleming, W.; Salcedo, J.; Patrawala, R.A. Impact of obesity on atrial fibrillation ablation: Patient characteristics, long-term outcomes, and complications. Heart Rhythm. 2017, 14, 819–827. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frost, L.; Vestergaard, P.; Mosekilde, L. Hyperthyroidism and Risk of Atrial Fibrillation or Flutter. Arch. Intern. Med. 2004, 164, 1675–1678. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chamberlain, A.M.; Agarwal, S.K.; Folsom, A.R.; Duval, S.; Soliman, E.Z.; Ambrose, M.; Eberly, L.E.; Alonso, A. Smoking and incidence of atrial fibrillation: Results from the Atherosclerosis Risk in Communities (ARIC) Study. Heart Rhythm. 2011, 8, 1160–1166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mont, L.; Elosua, R.; Brugada, J. Endurance sport practice as a risk factor for atrial fibrillation and atrial flutter. Europace 2008, 11, 11–17. [Google Scholar] [CrossRef]
- Vlachos, K.; Mascia, G.; Martin, C.A.; Bazoukis, G.; Frontera, A.; Cheniti, G.; Letsas, K.P.; Efremidis, M.; Georgopoulos, S.; Gkalapis, C.; et al. Atrial fibrillation in Brugada syndrome: Current perspectives. J. Cardiovasc. Electrophysiol. 2020, 31, 975–984. [Google Scholar] [CrossRef]
- Mascia, G.; Arbelo, E.; Solimene, F.; Giaccardi, M.; Brugada, R.; Brugada, J. The long-QT syndrome and exercise practice: The never-ending debate. J. Cardiovasc. Electrophysiol. 2018, 29, 489–496. [Google Scholar] [CrossRef]
- Cheng, X.; Hu, Q.; Gao, L.; Liu, J.; Qin, S.; Zhang, D. Sex-related differences in catheter ablation of atrial fibrillation: A systematic review and meta-analysis. Europace 2019, 21, 1509–1518. [Google Scholar] [CrossRef]
- Deng, H.; Shantsila, A.; Xue, Y.; Bai, Y.; Guo, P.; Potpara, T.S.; Zhan, X.; Fang, X.; Liao, H.; Wu, S.; et al. Renal function and outcomes after catheter ablation of patients with atrial fibrillation: The Guangzhou atrial fibrillation ablation registry. Arch. Cardiovasc. Dis. 2019, 112, 420–429. [Google Scholar] [CrossRef]
- Yanagisawa, S.; Inden, Y.; Kato, H.; Fujii, A.; Mizutani, Y.; Ito, T.; Kamikubo, Y.; Kanzaki, Y.; Ando, M.; Hirai, M.; et al. Impaired renal function is associated with recurrence after cryoballoon catheter ablation for paroxysmal atrial fibrillation: A potential effect of non-pulmonary vein foci. J. Cardiol. 2016, 69, 3–10. [Google Scholar] [CrossRef]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., 3rd; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A New Equation to Estimate Glomerular Filtration Rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef] [PubMed]
- Barrio, I.; Arostegui, I.; Álvarez, M.X.R.; Quintana, J.M. A new approach to categorising continuous variables in prediction models: Proposal and validation. Stat. Methods Med. Res. 2017, 26, 2586–2602. [Google Scholar] [CrossRef] [PubMed]
- Tibshirani, R. The lasso method for variable selection in the Cox model. Stat. Med. 1997, 16, 385–395. [Google Scholar] [CrossRef]
- Ishwaran, H.; Lu, M. Standard errors and confidence intervals for variable importance in random forest regression, classification, and survival. Stat. Med. 2018, 38, 558–582. [Google Scholar] [CrossRef]
- Zhao, Z.; Zhang, F.; Ma, R.; Bo, L.; Zhang, Z.; Zhang, C.; Wang, Z.; Li, C.; Yang, Y. Development and Validation of a Risk Nomogram Model for Predicting Recurrence in Patients with Atrial Fibrillation after Radiofrequency Catheter Ablation. Clin. Interv. Aging 2022, 17, 1405–1421. [Google Scholar] [CrossRef]
- Zhou, X.; Nakamura, K.; Sahara, N.; Takagi, T.; Toyoda, Y.; Enomoto, Y.; Hara, H.; Noro, M.; Sugi, K.; Moroi, M.; et al. Deep Learning-Based Recurrence Prediction of Atrial Fibrillation after Catheter Ablation. Circ. J. 2022, 86, 299–308. [Google Scholar] [CrossRef]
- Wang, T.J.; Parise, H.; Levy, D.; D’Agostino, R.B., Sr.; Wolf, P.A.; Vasan, R.S.; Benjamin, E.J. Obesity and the risk of new-onset atrial fibrillation. JAMA 2004, 292, 2471–2477. [Google Scholar] [CrossRef] [Green Version]
- Recommendations for Cardiac Chamber Quantification by Echocardiography in Adults: An Update from the American Society of Echocardiography and the European Association of, Cardiovascular Imaging. Eur. Heart J.-Cardiovasc. Imaging 2016, 17, 412. [CrossRef]
- Kojodjojo, P.; Peters, N.S.; Davies, D.W.; Kanagaratnam, P. Characterization of the Electroanatomical Substrate in Human Atrial Fibrillation: The Relationship between Changes in Atrial Volume, Refractoriness, Wavefront Propagation Velocities, and AF Burden. J. Cardiovasc. Electrophysiol. 2007, 18, 269–275. [Google Scholar] [CrossRef]
- Li, R.; Yang, X.; Jia, M.; Wang, D.; Cui, X.; Bai, L.; Zhao, L.; Zhang, J. Effectiveness of P-wave ECG index and left atrial appendage volume in predicting atrial fibrillation recurrence after first radiofrequency catheter ablation. BMC Cardiovasc. Disord. 2021, 21, 164. [Google Scholar] [CrossRef]
- Caldwell, J.; Koppikar, S.; Barake, W.; Redfearn, D.; Michael, K.; Simpson, C.; Hopman, W.; Baranchuk, A. Prolonged P-wave duration is associated with atrial fibrillation recurrence after successful pulmonary vein isolation for paroxysmal atrial fibrillation. J. Interv. Card. Electrophysiol. 2014, 39, 131–138. [Google Scholar] [CrossRef] [PubMed]
- Hondo, T.; Okamoto, M.; Yamane, T.; Kawagoe, T.; Karakawa, S.; Yamagata, T.; Matsuura, H.; Kajiyama, G. The Role of the Left Atrial Appendage. A Volume Loading Study in Open-chest Dogs. Jpn. Heart J. 1995, 36, 225–234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- He, Y.; Zhang, B.; Zhu, F.; Hu, Z.; Zhong, J.; Zhu, W. Transesophageal echocardiography measures left atrial appendage volume and function and predicts recurrence of paroxysmal atrial fibrillation after radiofrequency catheter ablation. Echocardiography 2018, 35, 985–990. [Google Scholar] [CrossRef] [PubMed]
- Istratoaie, S.; Vesa, C.; Cismaru, G.; Pop, D.; Roșu, R.; Puiu, M.; Pepine, D.; Ciobanu, C.; Minciuna, I.A.; Simu, G.; et al. Value of Left Atrial Appendage Function Measured by Transesophageal Echocardiography for Prediction of Atrial Fibrillation Recurrence after Radiofrequency Catheter Ablation. Diagnostics 2021, 11, 1465. [Google Scholar] [CrossRef]
- Voroneanu, L.; Covic, A. Arrhythmias in hemodialysis patients. J. Nephrol. 2009, 22, 716–725. [Google Scholar]
- Mohanty, S.; Mohanty, P.; Di Biase, L.; Rong, B.; Burkhardt, D.; Gallinghouse, J.G.; Horton, R.; Sanchez, J.E.; Bailey, S.; Zagrodzky, J.; et al. Baseline B-Type Natriuretic Peptide: A Gender-Specific Predictor of Procedure-Outcome in Atrial Fibrillation Patients Undergoing Catheter Ablation. J. Cardiovasc. Electrophysiol. 2011, 22, 858–865. [Google Scholar] [CrossRef]
- Yu, H.T.; Yang, P.-S.; Kim, T.-H.; Uhm, J.-S.; Kim, J.-Y.; Joung, B.; Lee, M.-H.; Pak, H.-N. Poor Rhythm Outcome of Catheter Ablation for Early-Onset Atrial Fibrillation in Women—Mechanistic Insight. Circ. J. 2018, 82, 2259–2268. [Google Scholar] [CrossRef] [Green Version]
- Odening, K.E.; Deiß, S.; Dilling-Boer, D.; Didenko, M.; Eriksson, U.; Nedios, S.; Ng, F.S.; Luque, I.R.; Borque, P.S.; Vernooy, K.; et al. Mechanisms of sex differences in atrial fibrillation: Role of hormones and differences in electrophysiology, structure, function, and remodelling. Europace 2018, 21, 366–376. [Google Scholar] [CrossRef]
- Akoum, N.; Mahnkopf, C.; Kholmovski, E.G.; Brachmann, J.; Marrouche, N.F. Age and sex differences in atrial fibrosis among patients with atrial fibrillation. Europace 2017, 20, 1086–1092. [Google Scholar] [CrossRef]
- Park, J.H.; Joung, B.; Son, N.-H.; Shim, J.M.; Lee, M.H.; Hwang, C.; Pak, H.-N. The electroanatomical remodelling of the left atrium is related to CHADS2/CHA2DS2VASc score and events of stroke in patients with atrial fibrillation. Europace 2011, 13, 1541–1549. [Google Scholar] [CrossRef] [Green Version]
- Vickers, A.J.; Elkin, E.B. Decision Curve Analysis: A Novel Method for Evaluating Prediction Models. Med. Decis. Mak. 2006, 26, 565–574. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, J.K.; Park, J.; Uhm, J.S.; Joung, B.; Lee, M.H.; Pak, H.N. Low P-wave amplitude (<0.1 mV) in lead I is associated with displaced inter-atrial conduction and clinical recurrence of paroxysmal atrial fibrillation after radiofrequency catheter ablation. Europace 2016, 18, 384–391. [Google Scholar] [CrossRef] [PubMed]
- Park, J.; Kim, T.; Lee, J.S.; Park, J.K.; Uhm, J.S.; Joung, B.; Lee, M.H.; Pak, H. Prolonged PR Interval Predicts Clinical Recurrence of Atrial Fibrillation after Catheter Ablation. J. Am. Heart Assoc. 2014, 3, e001277. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, J.-T.; Dong, J.-Z.; Sang, C.-H.; Tang, R.-B.; Ma, C.-S. Prolonged PR Interval and Risk of Recurrence of Atrial Fibrillation after Catheter Ablation. Int. Heart J. 2014, 55, 126–130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Njoku, A.; Kannabhiran, M.; Arora, R.; Reddy, P.; Gopinathannair, R.; Lakkireddy, D.; Dominic, P. Left atrial volume predicts atrial fibrillation recurrence after radiofrequency ablation: A meta-analysis. Europace 2018, 20, 33–42. [Google Scholar] [CrossRef]
- Scherr, D.; Khairy, P.; Miyazaki, S.; Aurillac-Lavignolle, V.; Pascale, P.; Wilton, S.B.; Ramoul, K.; Komatsu, Y.; Roten, L.; Jadidi, A.; et al. Five-Year Outcome of Catheter Ablation of Persistent Atrial Fibrillation Using Termination of Atrial Fibrillation as a Procedural Endpoint. Circ. Arrhythm. Electrophysiol. 2015, 8, 18–24. [Google Scholar] [CrossRef] [Green Version]
- Metzner, A.; Straube, F.; Tilz, R.R.; Kuniss, M.; Noelker, G.; Tebbenjohanns, J.; Andresen, D.; Wieneke, H.; Stellbrink, C.; Franke, J.; et al. Electrophysiology lab efficiency comparison between cryoballoon and point-by-point radiofrequency ablation: A German sub-analysis of the FREEZE Cohort study. BMC Cardiovasc. Disord. 2023, 23, 8. [Google Scholar] [CrossRef]
- Mascia, G.; Giaccardi, M. A New Era in Zero X-ray Ablation. Arrhythmia Electrophysiol. Rev. 2020, 9, 121–127. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Relapse (n = 153) | Censoring (n = 162) | p |
|---|---|---|---|
| CHA2DS2-VASc score | 2 (2) | 1 (2) | <0.001 |
| Age (years) | 59.77 ± 11.93 | 58.35 ± 10.64 | 0.269 |
| Sex (female), n (%) | 75 (49.02) | 46 (28.40) | <0.001 |
| Hypertension, n (%) | 85 (55.56) | 75 (46.30) | 0.100 |
| Diabetes, n (%) | 24 (15.69) | 22 (13.58) | 0.597 |
| Stroke/TIA, n (%) | 30 (19.61) | 19 (11.73) | 0.054 |
| LVEDd (mm) | 47.82 ± 4.10 | 48.06 ± 4.11 | 0.597 |
| LVEF (%) | 60.54 ± 5.74 | 61.33 ± 4.83 | 0.191 |
| LA diameter (anterior-posterior) (mm) | 36.59 ± 4.54 | 35.81 ± 4.38 | 0.123 |
| LAA emptying flow velocity (cm/s) | 39.58 ± 11.27 | 42.50 ± 11.74 | 0.025 |
| eGFR (mL/(min·1.73 m2)) | 90.43 (27.99) | 90.45 (18.29) | 0.270 |
| BMI (kg/m2) | 23.95 ± 3.20 | 23.94 ± 2.72 | 0.973 |
| NTproBNP, n (%) | 0.076 | ||
| ~150 pg/mL | 76 (49.67) | 89 (54.94) | |
| 150~ pg/mL | 68 (44.45) | 55 (33.95) | |
| missing data | 9 (5.88) | 18 (11.11) | |
| P wave duration | |||
| Lead II (ms) | 121.53 ± 18.32 | 118.65 ± 18.98 | 0.171 |
| Lead III (ms) | 111.99 ± 21.31 | 105.34 ± 21.13 | 0.006 |
| Lead aVF (ms) | 117.72 ± 19.19 | 113.75 ± 20.06 | 0.074 |
| Lead V1 (ms) | 106.52 ± 20.66 | 99.75 ± 19.05 | 0.003 |
| Terminal negative phase in V1 (ms) | 57 (21) | 53 (21) | 0.051 |
| Medications | |||
| ACEI/ARB, n (%) | 47 (30.72) | 45 (27.78) | 0.566 |
| beta-blockers, n (%) | 31 (20.26) | 32 (19.75) | 0.910 |
| amiodarone, n (%) | 118 (77.12) | 138 (85.19) | 0.067 |
| propafenone, n (%) | 14 (9.15) | 7 (4.32) | 0.086 |
| NOACs, n (%) | 136 (88.89) | 146 (90.12) | 0.721 |
| Ablation procedure | |||
| radiofrequency, n (%) | 61 (39.87) | 69 (42.59) | 0.624 |
| cryoballoon, n (%) | 92 (60.13) | 93 (57.41) | 0.624 |
| procedural time (min) | 144.95 ± 41.95 | 142.57 ± 43.33 | 0.620 |
| Additional procedures, n (%) | 23 (15.03) | 26 (16.05) | 0.804 |
| superior vena cava isolation, n (%) | 9 (5.88) | 13 (8.03) | 0.456 |
| linear ablation, n (%) | 5 (3.27) | 2 (1.24) | 0.271 |
| cavo-tricuspid isthmus abaltion, n (%) | 15 (9.80) | 17 (10.49) | 0.839 |
| Univariate Analysis | Lasso-Cox | Stepwise Regression | |||
|---|---|---|---|---|---|
| HR (95% CI) | p | Shrunk HR | HR (95% CI) | p | |
| Sex (female) | 1.79 (1.23–2.62) | 0.003 | 1.15 | 1.83 (1.23–2.71) | 0.003 |
| Hypertension (yes) | 1.11 (0.76–1.63) | 0.594 | |||
| eGFR < 65.8 mL/(min·1.73 m2) | 2.89 (1.77–4.71) | <0.001 | 1.39 | 1.73 (1.01–2.96) | 0.046 |
| LA diameter > 33 mm | 1.31 (0.83–2.09) | 0.246 | |||
| LAA emptying flow velocity ≤ 31 cm/s | 1.89 (1.22–2.94) | 0.005 | 1.12 | 1.90 (1.22–2.98) | 0.005 |
| BMI > 26 kg/m2 | 1.37 (0.90–2.09) | 0.143 | |||
| PWD in lead II ≥ 120 ms | 1.86 (1.26–2.75) | 0.002 | 1 | ||
| PWD in lead III ≥ 120 ms | 1.66 (1.12–2.46) | 0.011 | 1 | ||
| PWD in lead aVF ≥ 120 ms | 2.21 (1.50–3.25) | <0.001 | 1.31 | 1.85 (1.23–2.79) | 0.003 |
| PWD in lead V1 ≥ 100 ms | 2.12 (1.41–3.18) | <0.001 | 1.17 | 1.63 (1.06–2.51) | 0.026 |
| Terminal negative phase of PWD in lead V1 ≥ 60 ms | 1.57 (1.07–2.30) | 0.021 | 1 | ||
| Five-Factor Nomogram vs. CHA2DS2-VASc Score | IDI (95% CI) | p-Value | NRI (95% CI) | p-Value |
|---|---|---|---|---|
| 1-year | 0.108 (0.042–0.176) | <0.001 | 0.317 (0.120–0.423) | <0.001 |
| 2-year | 0.137 (0.069–0.204) | <0.001 | 0.340 (0.188–0.443) | <0.001 |
| 3-year | 0.156 (0.078–0.230) | 0.002 | 0.366 (0.213–0.511) | 0.002 |
| Models | AIC | BIC |
|---|---|---|
| Five-factor nomogram | 1013.40 | 1030.37 |
| Sex | 1041.50 | 1044.90 |
| LAA emptying flow velocity | 1043.34 | 1046.74 |
| eGFR | 1035.97 | 1039.37 |
| PWD in lead aVF | 1034.46 | 1037.86 |
| PWD in lead V1 | 1036.54 | 1039.94 |
| CHA2DS2-VASc score | 1042.86 | 1046.25 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, J.; Chen, H.; Zhang, Q.; Yang, R.; Peng, S.; Wu, Z.; Liu, N.; Tang, L.; Liu, Z.; Zhou, S. Development and Validation of a Novel Prognostic Tool to Predict Recurrence of Paroxysmal Atrial Fibrillation after the First-Time Catheter Ablation: A Retrospective Cohort Study. Diagnostics 2023, 13, 1207. https://doi.org/10.3390/diagnostics13061207
Huang J, Chen H, Zhang Q, Yang R, Peng S, Wu Z, Liu N, Tang L, Liu Z, Zhou S. Development and Validation of a Novel Prognostic Tool to Predict Recurrence of Paroxysmal Atrial Fibrillation after the First-Time Catheter Ablation: A Retrospective Cohort Study. Diagnostics. 2023; 13(6):1207. https://doi.org/10.3390/diagnostics13061207
Chicago/Turabian StyleHuang, Junjie, Hao Chen, Quan Zhang, Rukai Yang, Shuai Peng, Zhijian Wu, Na Liu, Liang Tang, Zhenjiang Liu, and Shenghua Zhou. 2023. "Development and Validation of a Novel Prognostic Tool to Predict Recurrence of Paroxysmal Atrial Fibrillation after the First-Time Catheter Ablation: A Retrospective Cohort Study" Diagnostics 13, no. 6: 1207. https://doi.org/10.3390/diagnostics13061207