
The Sarcoma-Specific Instrument to Longitudinally Assess Health-Related Outcomes of the Routine Care Cycle

 , , , ,
, , , ,
Abstract
:1. Why Do We Need Patient Reported Outcome Measures (PROMs)?
2. Challenges to Introduce PROMs for Sarcoma Patients
3. Which PROMs Are Being Used for Sarcoma Patients?
4. Sarcoma-Specific HRQoL-Instrument Based on Generic PROMs
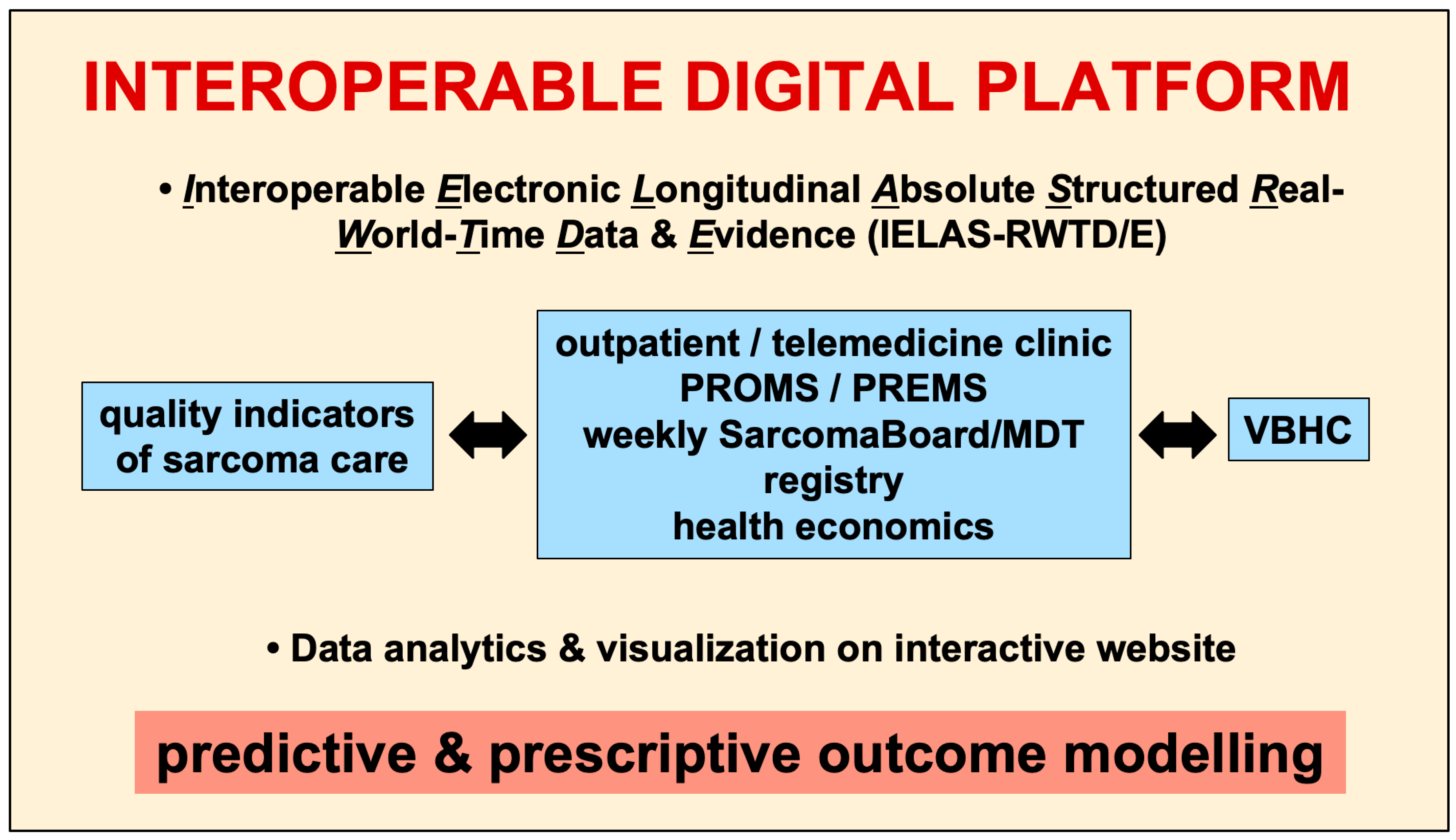
5. Interoperable Digital Platform: Data Assessment and Analysis
6. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Baicker, K.; Chandra, A. Do We Spend Too Much on Health Care? N. Engl. J. Med. 2020, 383, 605–608. [Google Scholar] [CrossRef] [PubMed]
- Ramello, M.; Audisio, R.A. The value of patient centred care in oncology. Eur. J. Surg. Oncol. 2020, 47, 492–494. [Google Scholar] [CrossRef] [PubMed]
- Porter, M.E. Value-based health care delivery. Ann. Surg. 2008, 248, 503–509. [Google Scholar] [CrossRef] [PubMed]
- Gyawali, B.; Booth, C.M. Cancer treatments should benefit patients: A common-sense revolution in oncology. Nat. Med. 2022, 28, 617–620. [Google Scholar] [CrossRef]
- Porter, M.E.; Lee, T.H. From Volume to Value in Health Care: The Work Begins. JAMA 2016, 316, 1047–1048. [Google Scholar] [CrossRef]
- Allen, C.J.; Smith, G.L.; Prakash, L.; Volk, R.J.; Ikoma, N.; Aloia, T.A.; Gottumukkala, V.; Katz, M.H.G. What is “Value”? Results of a Survey of Cancer Patients and Providers. Ann. Surg. Oncol. 2022, 29, 6537–6545. [Google Scholar] [CrossRef]
- Zilchman, E.; Nicklin, W.; Aggarwal, R.; Bates, D. Health Care 2030: The coming transformation. NEJM Catalyst 2021, 1, 1–11. [Google Scholar]
- Kaplan, R.S.; Jehi, L.; Ko, C.Y.; Pusic, A.; Witkowski, M. Health Care Measurements that Improve Patient Outcomes. NEJM Catal. 2021, 2. [Google Scholar] [CrossRef]
- Di Maio, M.; Basch, E.; Denis, F.; Fallowfield, L.J.; Ganz, P.A.; Howell, D.; Kowalski, C.; Perrone, F.; Stover, A.M.; Sundaresan, P.; et al. The role of patient-reported outcome measures in the continuum of cancer clinical care: ESMO Clinical Practice Guideline. Ann. Oncol. 2022, 33, 878–892. [Google Scholar] [CrossRef]
- MacLean, C.H.; Antao, V.C.; Fontana, M.A.; Sandhu, H.S.; McLawhorn, A.S. PROMs: Opportunities, Challenges, and Unfinished Business. NEJM Catal. 2021, 2. [Google Scholar] [CrossRef]
- Calvert, M.J.; Rivera, S.C.; Retzer, A.; Hughes, S.E.; Campbell, L.; Molony-Oates, B.; Aiyegbusi, O.L.; Stover, A.M.; Wilson, R.; McMullan, C.; et al. Patient reported outcome assessment must be inclusive and equitable. Nat. Med. 2022, 28, 1120–1124. [Google Scholar] [CrossRef]
- Retzer, A.; Aiyegbusi, O.L.; Rowe, A.; Newsome, P.N.; Douglas-Pugh, J.; Khan, S.; Mittal, S.; Wilson, R.; O’Connor, D.; Campbell, L.; et al. The value of patient-reported outcomes in early-phase clinical trials. Nat. Med. 2022, 28, 18–20. [Google Scholar] [CrossRef]
- Minvielle, E.; di Palma, M.; Mir, O.; Scotté, F. The use of patient-reported outcomes (PROs) in cancer care: A realistic strategy. Ann. Oncol. 2022, 33, 357–359. [Google Scholar] [CrossRef]
- Porter, M.E.; Larsson, S.; Lee, T.H. Standardizing Patient Outcomes Measurement. N. Engl. J. Med. 2016, 374, 504–506. [Google Scholar] [CrossRef] [Green Version]
- Bartelstein, M.K.; Forsberg, J.A.; Lavery, J.A.; Yakoub, M.A.; Akhnoukh, S.; Boland, P.J.; Fabbri, N.; Healey, J.H. Quantitative Preoperative Patient Assessments Are Related to Survival and Procedure Outcome for Osseous Metastases. J. Bone Oncol. 2022, 34, 100433. [Google Scholar] [CrossRef]
- Viala, M.; Bhakar, A.L.; de la Loge, C.; van de Velde, H.; Esseltine, D.; Chang, M.; Dhawan, R.; Dubois, D. Patient-reported outcomes helped predict survival in multiple myeloma using partial least squares analysis. J. Clin. Epidemiol. 2007, 60, 670–679. [Google Scholar] [CrossRef]
- Herndon, J.E., II; Fleishman, S.; Kornblith, A.B.; Kosty, M.; Green, M.R.; Holland, J. Is quality of life predictive of the survival of patients with advanced nonsmall cell lung carcinoma? Cancer 1999, 85, 333–340. [Google Scholar] [CrossRef]
- Patterson, R.E.; Saquib, N.; Natarajan, L.; Rock, C.L.; Parker, B.A.; Thomson, C.A.; Pierce, J.P. Improvement in self-reported physical health predicts longer survival among women with a history of breast cancer. Breast Cancer Res. Treat. 2011, 127, 541–547. [Google Scholar] [CrossRef] [Green Version]
- Calvert, M.; Kyte, D.; Price, G.; Valderas, J.M.; Hjollund, N.H. Maximising the impact of patient reported outcome assessment for patients and society. BMJ 2019, 364, k5267. [Google Scholar] [CrossRef] [Green Version]
- Hsu, T.; Speers, C.H.; Kennecke, H.F.; Cheung, W.Y. The utility of abbreviated patient-reported outcomes for predicting survival in early stage colorectal cancer. Cancer 2017, 123, 1839–1847. [Google Scholar] [CrossRef] [Green Version]
- Khurana, D.; Leung, G.; Sasaninia, B.; Tran, D.; Khan, M.; Firek, A. The Whole PERSON Health Score: A Patient-Focused Tool to Measure Nonmedical Determinants of Health. NEJM Catalyst 2022, 3. [Google Scholar] [CrossRef]
- Maani, N.; Galea, S. The Role of Physicians in Addressing Social Determinants of Health. JAMA 2020, 323, 1551–1552. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gard, L.A.; Peterson, J.; Miller, C.; Ghosh, N.; Youmans, Q.; Didwania, A.; Persell, S.D.; Jean-Jacques, M.; Ravenna, P.; O’Brien, M.J.; et al. Social Determinants of Health Training in U.S. Primary Care Residency Programs: A Scoping Review. Acad. Med. 2019, 94, 135–143. [Google Scholar] [CrossRef] [Green Version]
- Braveman, P.; Gottlieb, L. The social determinants of health: It’s time to consider the causes of the causes. Public Health Rep. 2014, 129 (Suppl. S2), 19–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Remington, P.L. County Health Rankings and the Cult of the Imperfect. Health Serv. Res. 2015, 50, 1407–1412. [Google Scholar] [CrossRef] [Green Version]
- Williams, P.A.; Zaidi, S.K.; Sengupta, R. AACR Cancer Progress Report 2022: Decoding Cancer Complexity, Integrating Science, and Transforming Patient Outcomes. Clin. Cancer Res. 2022, 28, 4178–4179. [Google Scholar] [CrossRef]
- Fuchs, B.; Bode-Lesniewska, B.; Studer, G.; Breitenstein, S. Wie entwickelt sich die Sarkomchirurgie? Lead. Opin. Orthoädie Traumatol. 2021, 1, 16–18. [Google Scholar]
- Blay, J.Y.; Soibinet, P.; Penel, N.; Bompas, E.; Duffaud, F.; Stoeckle, E.; Mir, O.; Adam, J.; Chevreau, C.; Bonvalot, S.; et al. Improved survival using specialized multidisciplinary board in sarcoma patients. Ann. Oncol. 2017, 28, 2852–2859. [Google Scholar] [CrossRef]
- Blay, J.Y.; Honore, C.; Stoeckle, E.; Meeus, P.; Jafari, M.; Gouin, F.; Anract, P.; Ferron, G.; Rochwerger, A.; Ropars, M.; et al. Surgery in reference centers improves survival of sarcoma patients: A nationwide study. Ann. Oncol. 2019, 30, 1143–1153. [Google Scholar] [CrossRef]
- Blay, J.Y.; Bonvalot, S.; Gouin, F.; Le Cesne, A.; Penel, N. Criteria for reference centers for sarcomas: Volume but also long-term multidisciplinary organisation. Ann. Oncol. 2019, 30, 2008–2009. [Google Scholar] [CrossRef]
- Fayet, Y.; Tetreau, R.; Honore, C.; Le Nail, L.R.; Dalban, C.; Gouin, F.; Causeret, S.; Piperno-Neumann, S.; Mathoulin-Pelissier, S.; Karanian, M.; et al. Determinants of the access to remote specialised services provided by national sarcoma reference centres. BMC Cancer 2021, 21, 631. [Google Scholar] [CrossRef]
- Blay, J.-Y.; Penel, N.; Gouin, F.; Le Cesne, A.; Toulmonde, M. Improving at a nationwide level the management of patients with sarcomas with an expert network. Ann. Oncol. 2022, 33, 659–661. [Google Scholar] [CrossRef]
- Almeida, A.; Martins, T.; Lima, L. Patient-Reported Outcomes in Sarcoma: A scoping review. Eur. J. Oncol. Nurs. 2021, 50, 101897. [Google Scholar] [CrossRef]
- Martins, A.; Bennister, L.; Fern, L.A.; Gerrand, C.; Onasanya, M.; Storey, L.; Wells, M.; Whelan, J.S.; Windsor, R.; Woodford, J.; et al. Development of a patient-reported experience questionnaire for patients with sarcoma: The Sarcoma Assessment Measure (SAM). Qual. Life Res. 2020, 29, 2287–2297. [Google Scholar] [CrossRef]
- Schut, A.-R.W.; Timbergen, M.J.M.; Lidington, E.; Grünhagen, D.J.; van der Graaf, W.T.A.; Sleijfer, S.; van Houdt, W.J.; Bonenkamp, J.J.; Younger, E.; Dunlop, A.; et al. The Evaluation of Health-Related Quality of Life Issues Experienced by Patients with Desmoid-Type Fibromatosis (The QUALIFIED Study)—A Protocol for an International Cohort Study. Cancers 2021, 13, 3068. [Google Scholar] [CrossRef]
- den Hollander, D.; Van der Graaf, W.T.A.; Fiore, M.; Kasper, B.; Singer, S.; Desar, I.M.E.; Husson, O. Unravelling the heterogeneity of soft tissue and bone sarcoma patients’ health-related quality of life: A systematic literature review with focus on tumour location. ESMO Open 2020, 5, e000914. [Google Scholar] [CrossRef]
- den Hollander, D.; Fiore, M.; Martin-Broto, J.; Kasper, B.; Casado Herraez, A.; Kulis, D.; Nixon, I.; Sodergren, S.C.; Eichler, M.; van Houdt, W.J.; et al. Incorporating the Patient Voice in Sarcoma Research: How Can We Assess Health-Related Quality of Life in This Heterogeneous Group of Patients? A Study Protocol. Cancers 2020, 13, 1. [Google Scholar] [CrossRef]
- Pala, L.; Sala, I.; Oriecuia, C.; De Pas, T.; Queirolo, P.; Specchia, C.; Cocorocchio, E.; Ferrucci, P.; Patane, D.; Saponara, M.; et al. Association of Anticancer Immune Checkpoint Inhibitors With Patient-Reported Outcomes Assessed in Randomized Clinical Trials: A Systematic Review and Meta-analysis. JAMA Netw. Open 2022, 5, e2226252. [Google Scholar] [CrossRef]
- Saebye, C.; Amidi, A.; Keller, J.; Andersen, H.; Baad-Hansen, T. Changes in Functional Outcome and Quality of Life in Soft Tissue Sarcoma Patients within the First Year after Surgery: A Prospective Observational Study. Cancers 2020, 12, 463. [Google Scholar] [CrossRef]
- Eichler, M.; Hentschel, L.; Richter, S.; Hohenberger, P.; Kasper, B.; Andreou, D.; Pink, D.; Jakob, J.; Singer, S.; Grutzmann, R.; et al. The Health-Related Quality of Life of Sarcoma Patients and Survivors in Germany-Cross-Sectional Results of a Nationwide Observational Study (PROSa). Cancers 2020, 12, 3590. [Google Scholar] [CrossRef]
- Husson, O.; den Hollander, D.; van der Graaf, W.T.A. The complexity of assessing health-related quality of life among sarcoma patients. Qual. Life Res. 2020, 29, 2613–2614. [Google Scholar] [CrossRef] [PubMed]
- Timbergen, M.J.M.; Schut, A.W.; Grunhagen, D.J.; Sleijfer, S.; Verhoef, C. Active surveillance in desmoid-type fibromatosis: A systematic literature review. Eur. J. Cancer 2020, 137, 18–29. [Google Scholar] [CrossRef] [PubMed]
- Cella, D.; Yount, S.; Rothrock, N.; Gershon, R.; Cook, K.; Reeve, B.; Ader, D.; Fries, J.F.; Bruce, B.; Rose, M.; et al. The Patient-Reported Outcomes Measurement Information System (PROMIS): Progress of an NIH Roadmap cooperative group during its first two years. Med. Care 2007, 45 (Suppl. S1), S3–S11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, L.J.; Tan, R.L.; Luo, N. Measurement Properties of the EQ VAS Around the Globe: A Systematic Review and Meta-Regression Analysis. Value Health 2021, 24, 1223–1233. [Google Scholar] [CrossRef]
- Janssen, B.; Szende, A.; Ramos-Goni, J.M. Data and Methods. In Self-Reported Population Health: An International Perspective based on EQ-5D; Szende, A., Janssen, B., Cabases, J., Eds.; Springer: Dordrecht, The Netherlands, 2014; pp. 7–17. [Google Scholar]
- Derogatis, L. BSI 18: Brief Symptom Inventory 18. Administration, Scoring, and Procedures Manual; NCS Pearson: Minneapolis, MN, USA, 2000. [Google Scholar]
- Lundin, A.; Leijon, O.; Vaez, M.; Hallgren, M.; Torgen, M. Predictive validity of the Work Ability Index and its individual items in the general population. Scand. J. Public Health 2017, 45, 350–356. [Google Scholar] [CrossRef]
- Davis, A.M.; Wright, J.G.; Williams, J.I.; Bombardier, C.; Griffin, A.; Bell, R.S. Development of a measure of physical function for patients with bone and soft tissue sarcoma. Qual. Life Res. 1996, 5, 508–516. [Google Scholar] [CrossRef]
- Enneking, W.F.; Dunham, W.; Gebhardt, M.C.; Malawar, M.; Pritchard, D.J. A system for the functional evaluation of reconstructive procedures after surgical treatment of tumors of the musculoskeletal system. Clin. Orthop. Relat. Res. 1993, 286, 241–246. [Google Scholar] [CrossRef]
- Sprangers, M.A.; Cull, A.; Bjordal, K.; Groenvold, M.; Aaronson, N.K. The European Organization for Research and Treatment of Cancer. Approach to quality of life assessment: Guidelines for developing questionnaire modules. EORTC Study Group on Quality of Life. Qual. Life Res. 1993, 2, 287–295. [Google Scholar] [CrossRef]
- Husson, O.; de Rooij, B.H.; Kieffer, J.; Oerlemans, S.; Mols, F.; Aaronson, N.K.; van der Graaf, W.T.A.; van de Poll-Franse, L.V. The EORTC QLQ-C30 Summary Score as Prognostic Factor for Survival of Patients with Cancer in the "Real-World": Results from the Population-Based PROFILES Registry. Oncologist 2020, 25, e722–e732. [Google Scholar] [CrossRef] [Green Version]
- Wilson, D.A.J.; Gazendam, A.; Visgauss, J.; Perrin, D.; Griffin, A.M.; Chung, P.W.; Catton, C.N.; Shultz, D.; Ferguson, P.C.; Wunder, J.S. Designing a Rational Follow-Up Schedule for Patients with Extremity Soft Tissue Sarcoma. Ann. Surg. Oncol. 2020, 27, 2033–2041. [Google Scholar] [CrossRef]
- Jiang, P.; Sinha, S.; Aldape, K.; Hannenhalli, S.; Sahinalp, C.; Ruppin, E. Big data in basic and translational cancer research. Nat. Rev. Cancer 2022, 22, 625–639. [Google Scholar] [CrossRef]
- Basch, E.; Leahy, A.B.; Dueck, A.C. Benefits of Digital Symptom Monitoring With Patient-Reported Outcomes During Adjuvant Cancer Treatment. J. Clin. Oncol. 2021, 39, 701–703. [Google Scholar] [CrossRef]
- Basch, E.; Deal, A.M.; Dueck, A.C.; Scher, H.I.; Kris, M.G.; Hudis, C.; Schrag, D. Overall Survival Results of a Trial Assessing Patient-Reported Outcomes for Symptom Monitoring During Routine Cancer Treatment. JAMA 2017, 318, 197–198. [Google Scholar] [CrossRef] [Green Version]
- Shojima, H.; Shimomura, A.; Kadowaki, M.; Kawamura, Y.; Shimizu, C. How Can We Evaluate the Electronic Patient-Reported Outcome Appropriately? J. Clin. Oncol. 2021, 39, 2632–2633. [Google Scholar] [CrossRef]
- Concato, J.; Corrigan-Curay, J. Real-World Evidence—Where Are We Now? N. Engl. J. Med. (NEJM) 2022, 386, 1680–1682. [Google Scholar] [CrossRef]
- Penberthy, L.T.; Rivera, D.R.; Lund, J.L.; Bruno, M.A.; Meyer, A.M. An overview of real-world data sources for oncology and considerations for research. CA A Cancer J. Clin. 2021, 72, 287–300. [Google Scholar] [CrossRef]
- Orr, M.N.; Klika, A.K.; Gagnier, J.J.; Bhandari, M.; Piuzzi, N.S. A Call for a Standardized Approach to Reporting Patient-Reported Outcome Measures: Clinical Relevance Ratio. J. Bone Joint Surg. Am. 2021, 103, e91. [Google Scholar] [CrossRef]
- Bandyopadhyay, S.; Baticulon, R.E.; Kadhum, M.; Alser, M.; Ojuka, D.K.; Badereddin, Y.; Kamath, A.; Parepalli, S.A.; Brown, G.; Iharchane, S.; et al. Infection and mortality of healthcare workers worldwide from COVID-19: A systematic review. BMJ Glob. Health 2020, 5, e003097. [Google Scholar] [CrossRef]
- Kaufmann, T.L.; Rocque, G.B. Pathway to Precision Patient-Reported Outcomes. J. Clin. Oncol. 2021, 39, 3770–3772. [Google Scholar] [CrossRef]
- Pranata, S.; Wu, S.V.; Alizargar, J.; Liu, J.H.; Liang, S.Y.; Lu, Y.Y. Precision Health Care Elements, Definitions, and Strategies for Patients with Diabetes: A Literature Review. Int. J. Environ. Res. Public Health 2021, 18, 6535. [Google Scholar] [CrossRef]


{kind=link}
| Challenge | References | Added Value |
|---|---|---|
| Where do we want to go? | [8] | This article describes the transition from the current care to the future state of how our healthcare system will look like in 2030, specifically emphasizing the potential of digital transformation. |
| What is good health? | [18,21,22,23,24,25,26] | These articles define the social determinants of health and the delivery of care. Health behaviors, socioeconomic factors and physical environment contribute 80% to health outcomes, whereas clinical care only contributes the remaining 20% to clinical outcomes. For these reasons, the Whole Person Health Score was created. |
| What is the current problem? | [1,2,6,7,27] | Healthcare costs represent a seemingly unsurmountable problem, and lead us towards an unsustainable trend. While perceptions of value differ among patients and providers, shared decision-making regarding data assessment and documentation remain challenges specifically because most of the healthcare data are unstructured und therefore not ready for analysis. |
| Potential solutions? | [3,4,5] | Improving value benefits may lead to a sustainable health system. A novel ecosystem centers on the shared value being the multidimensional relationship between health outcomes and costs incurred to deliver these, as defined by the value-based healthcare principle. For these reasons, quality of care must be defined and assessed using structured data, to which then cost tags can be attributed which allows the definition of the entire costs of a given diagnosis over the entire care cycle. |
| Why are PROMS important? | [9,10,11,12,13,14,15,16,17,18,19] | These articles summarize how PROMS assess treatment effectiveness and outcome, and show that they can improve survival. PROMS have to be designed such that they cover the entire spectrum of the social determinants of health as suggested by WPHS but are nevertheless disease-specific. |
| Time Point of Assessment & Therapy Status | Type of PROM |
|---|---|
| Work-up at diagnosis Regular visits during therapy | WHO-ECOGPROMIS [43] |
| EQ-VAS [44] | |
| EQ-5D-5L [45] BSI-18 [46] WAI [47] | |
| Biopsy | Mesenchymal Tumor biopsy PROM * |
| (MTBP) | |
| Surgery | TESS (upper/lower extremity) [48] |
| MSTS (upper/lower extremity) [49] | |
| Visceral (TARPSWG) * | |
| Radiation Therapy | Local effects of therapy |
| PRO-CTCAE | |
| Chemotherapy | EORTC-QLQ-C30 [50,51] |
| Follow-up visits after completion of therapy | Combination of above |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mosku, N.; Heesen, P.; Christen, S.; Scaglioni, M.F.; Bode, B.; Studer, G.; Fuchs, B., on behalf of the Swiss Sarcoma Network. The Sarcoma-Specific Instrument to Longitudinally Assess Health-Related Outcomes of the Routine Care Cycle. Diagnostics 2023, 13, 1206. https://doi.org/10.3390/diagnostics13061206
Mosku N, Heesen P, Christen S, Scaglioni MF, Bode B, Studer G, Fuchs B on behalf of the Swiss Sarcoma Network. The Sarcoma-Specific Instrument to Longitudinally Assess Health-Related Outcomes of the Routine Care Cycle. Diagnostics. 2023; 13(6):1206. https://doi.org/10.3390/diagnostics13061206
Chicago/Turabian StyleMosku, Nasian, Philip Heesen, Salome Christen, Mario F. Scaglioni, Beata Bode, Gabriela Studer, and Bruno Fuchs on behalf of the Swiss Sarcoma Network. 2023. "The Sarcoma-Specific Instrument to Longitudinally Assess Health-Related Outcomes of the Routine Care Cycle" Diagnostics 13, no. 6: 1206. https://doi.org/10.3390/diagnostics13061206