
Rare Benign Tumors and Tumor-like Lesions of the Hand without Skin Damage—Clinical, Imagistic and Histopathological Diagnosis, Retrospective Study
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
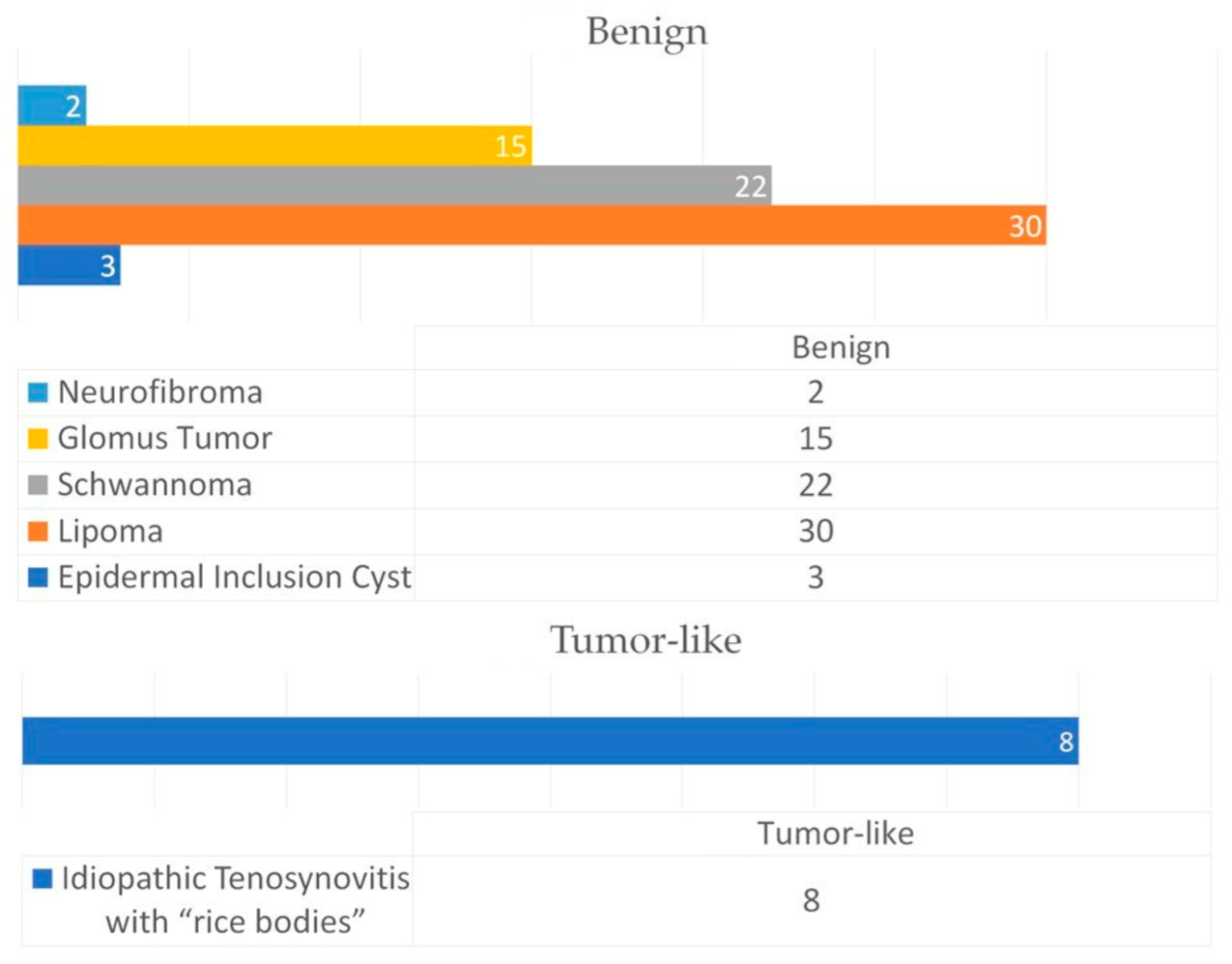
3. Results
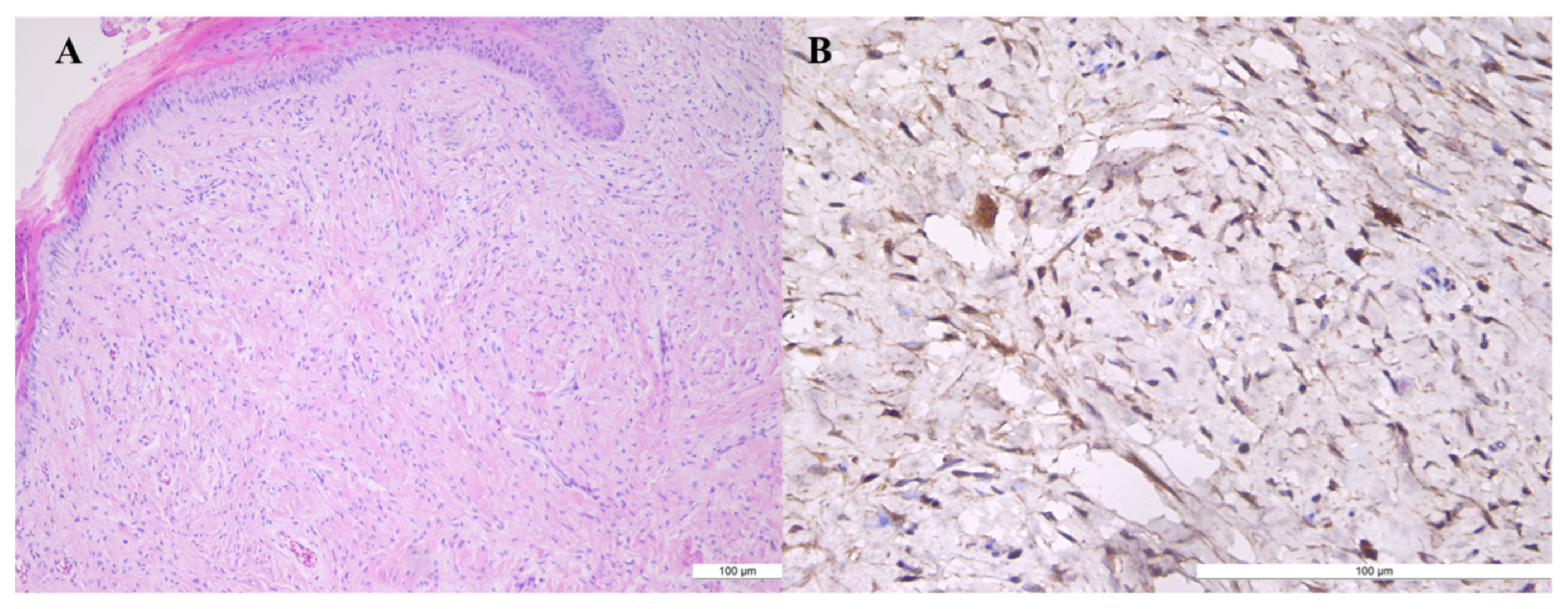
3.1. Neurofibroma
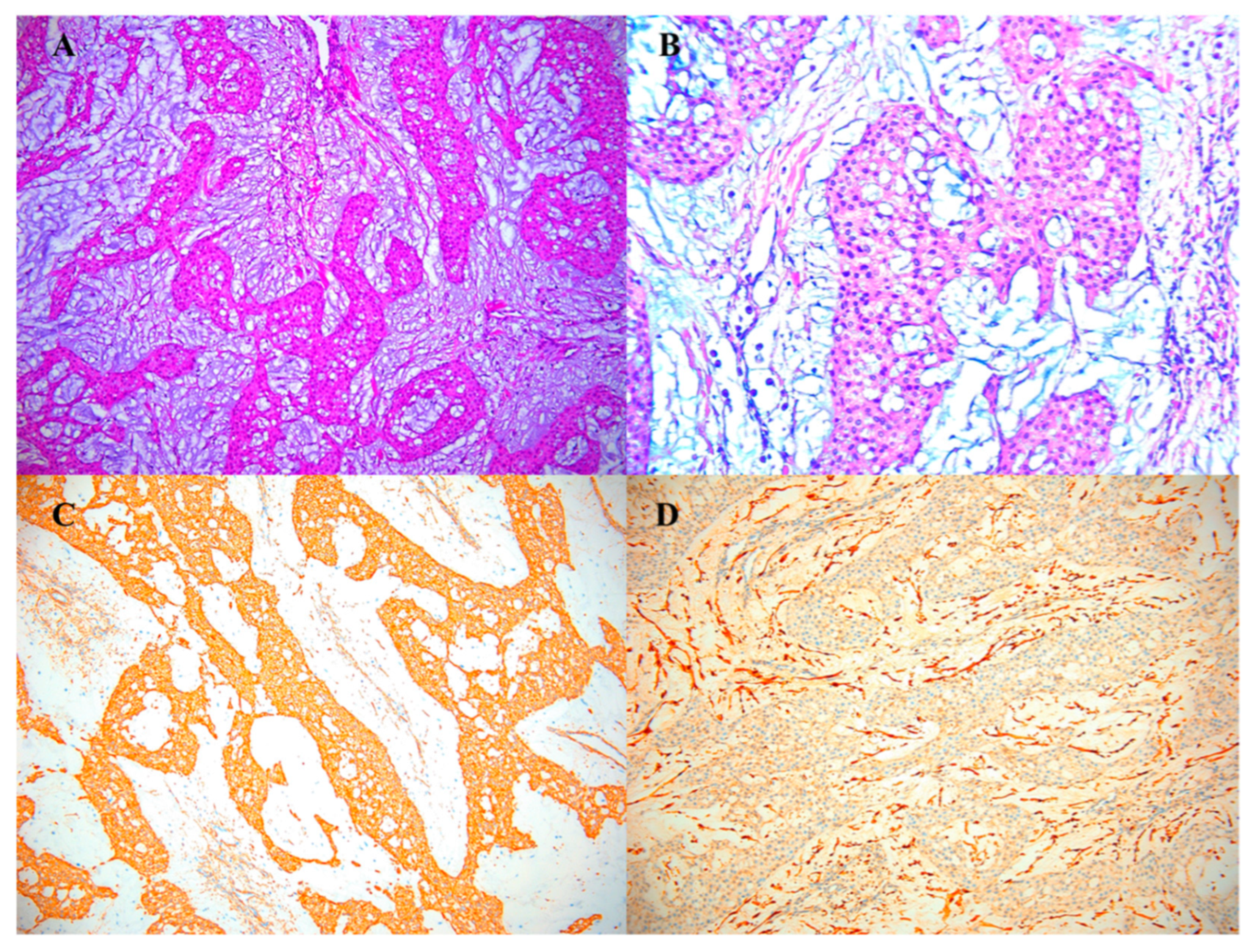
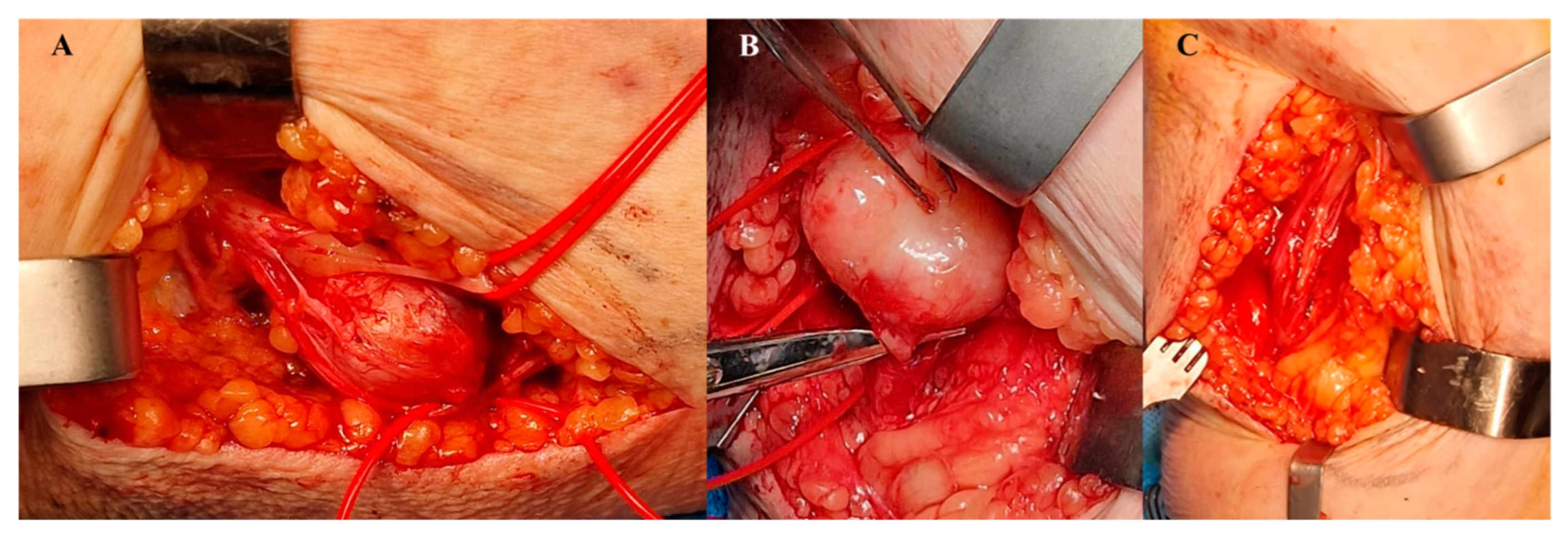
3.2. Glomus Tumors
3.3. Schwannoma
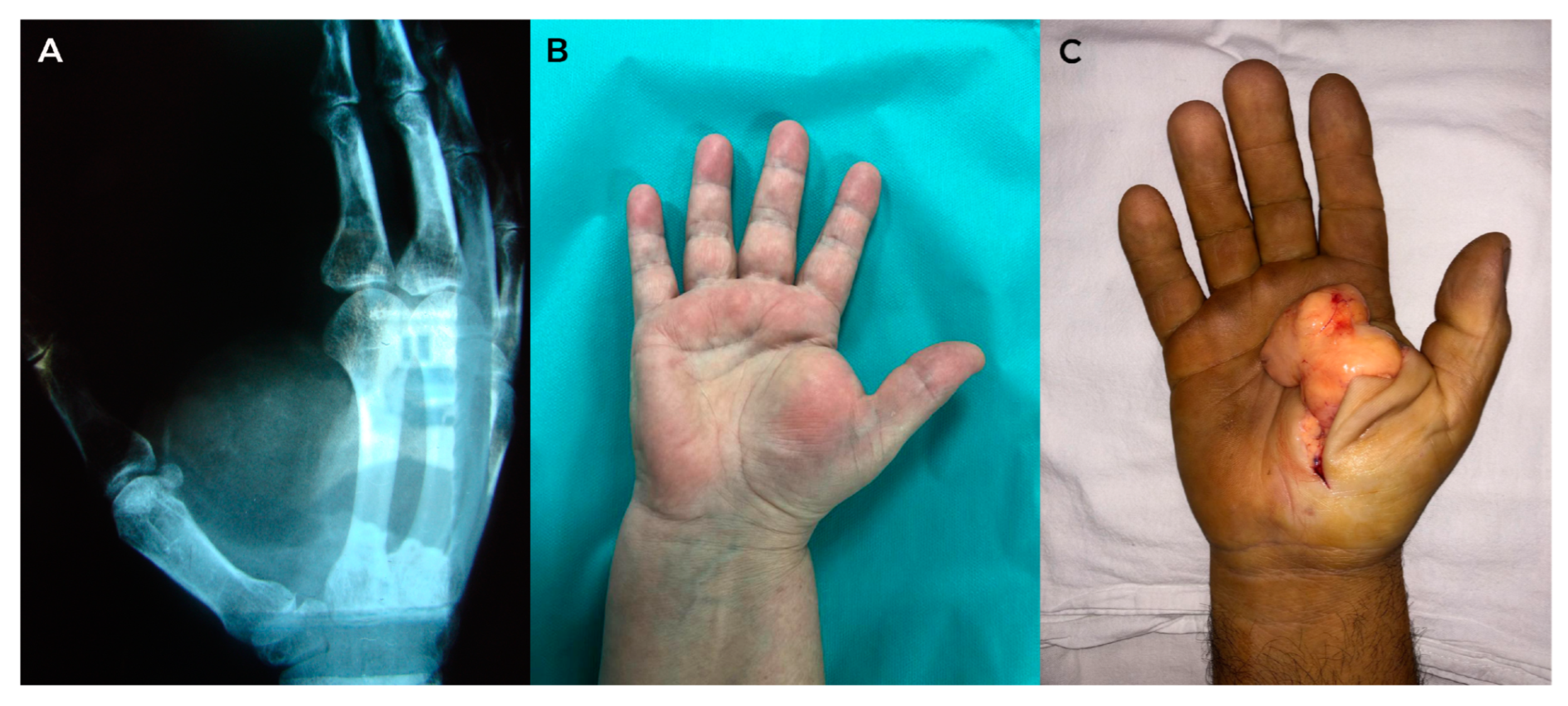
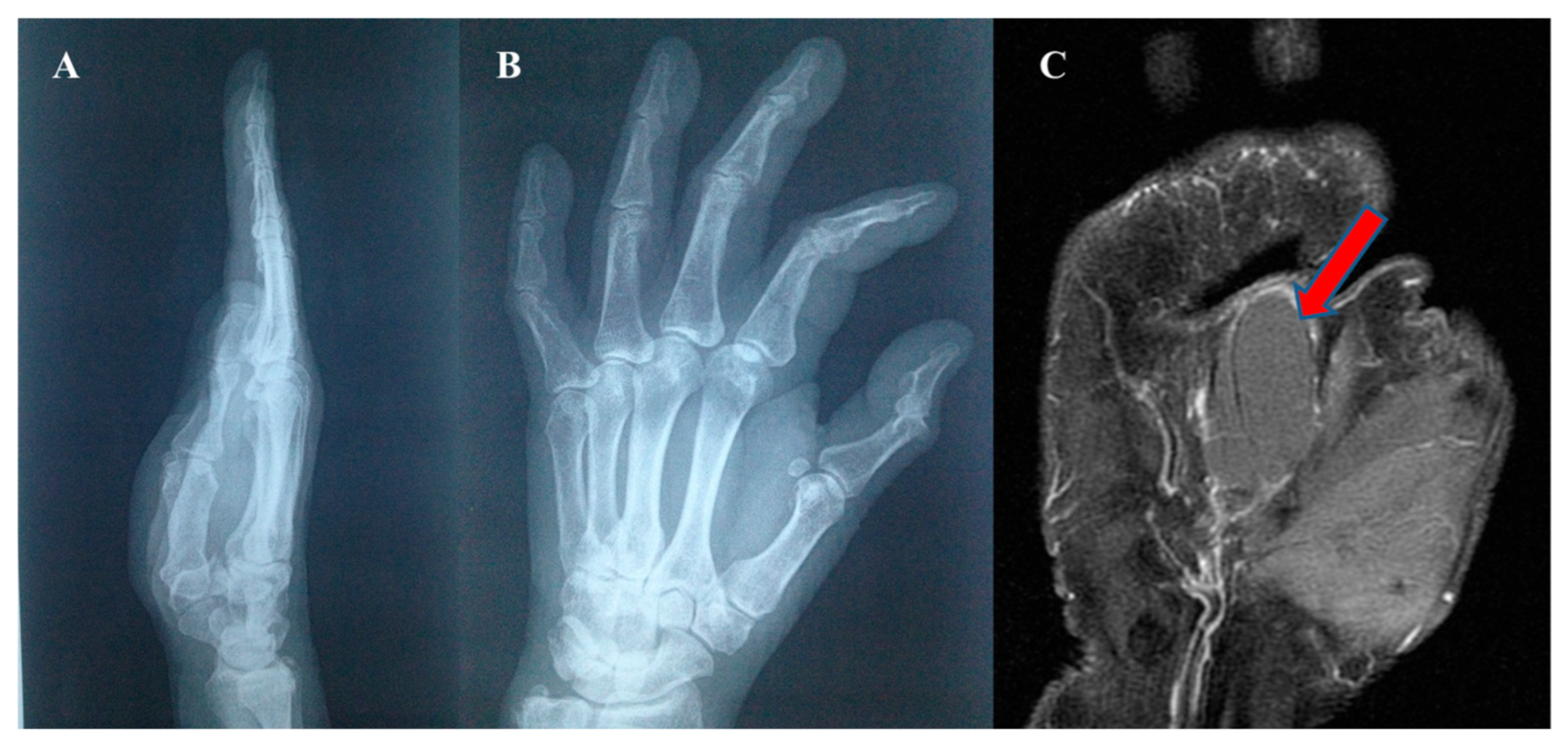
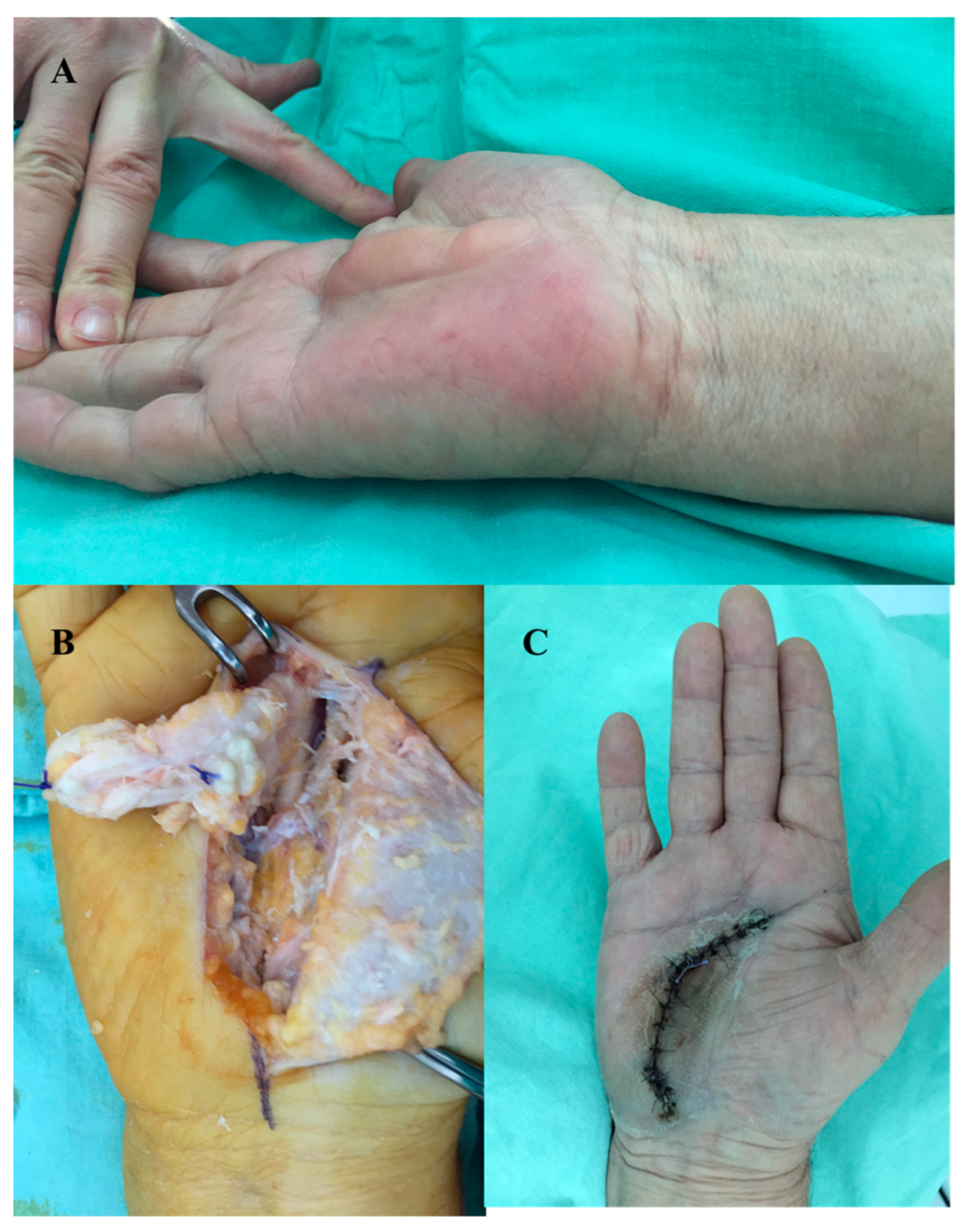
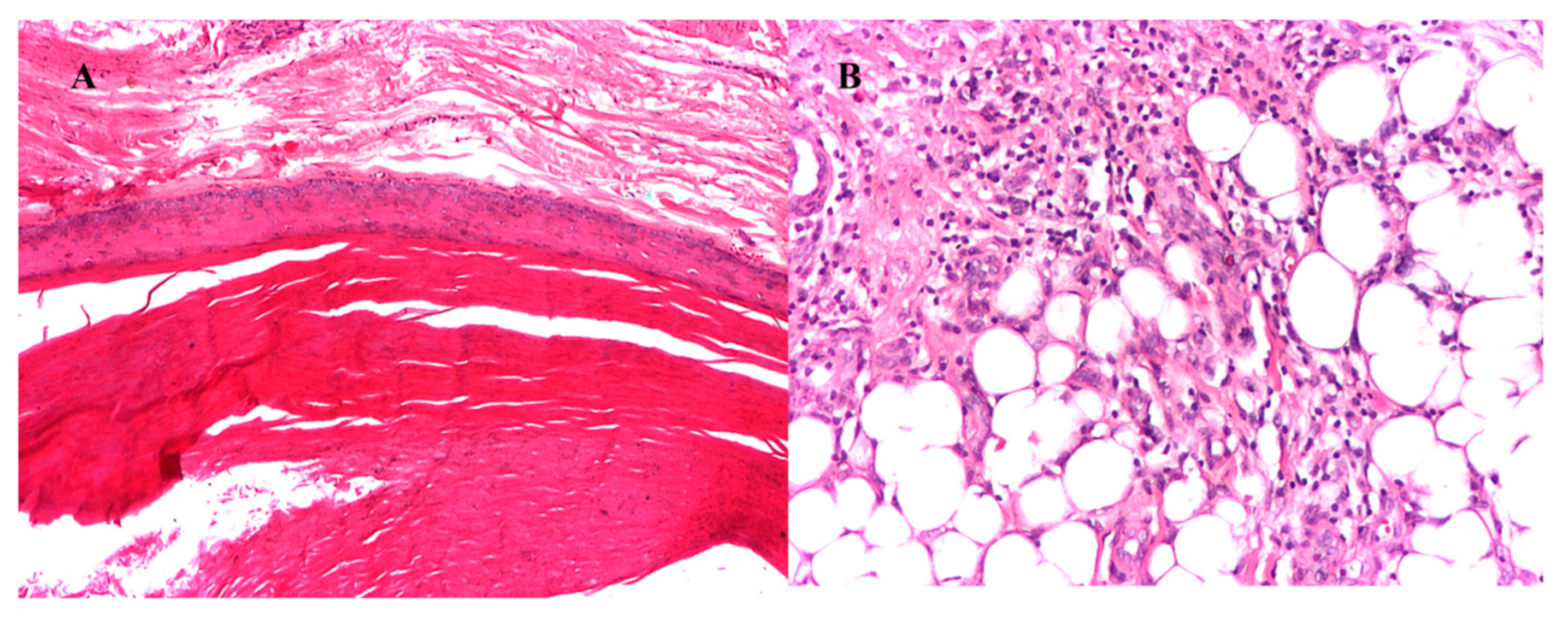
3.4. Lipoma
3.5. Epidermal Inclusion Cyst
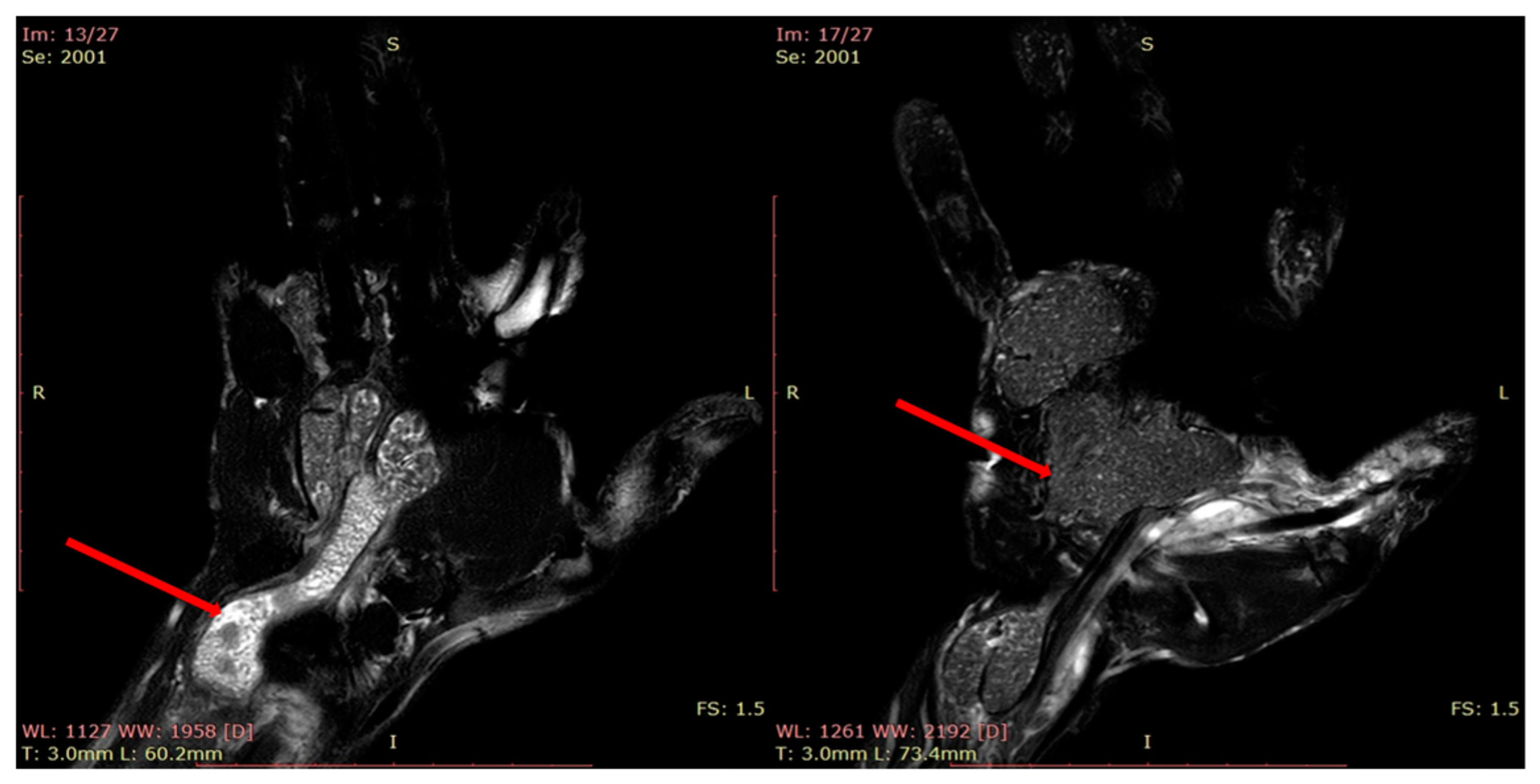
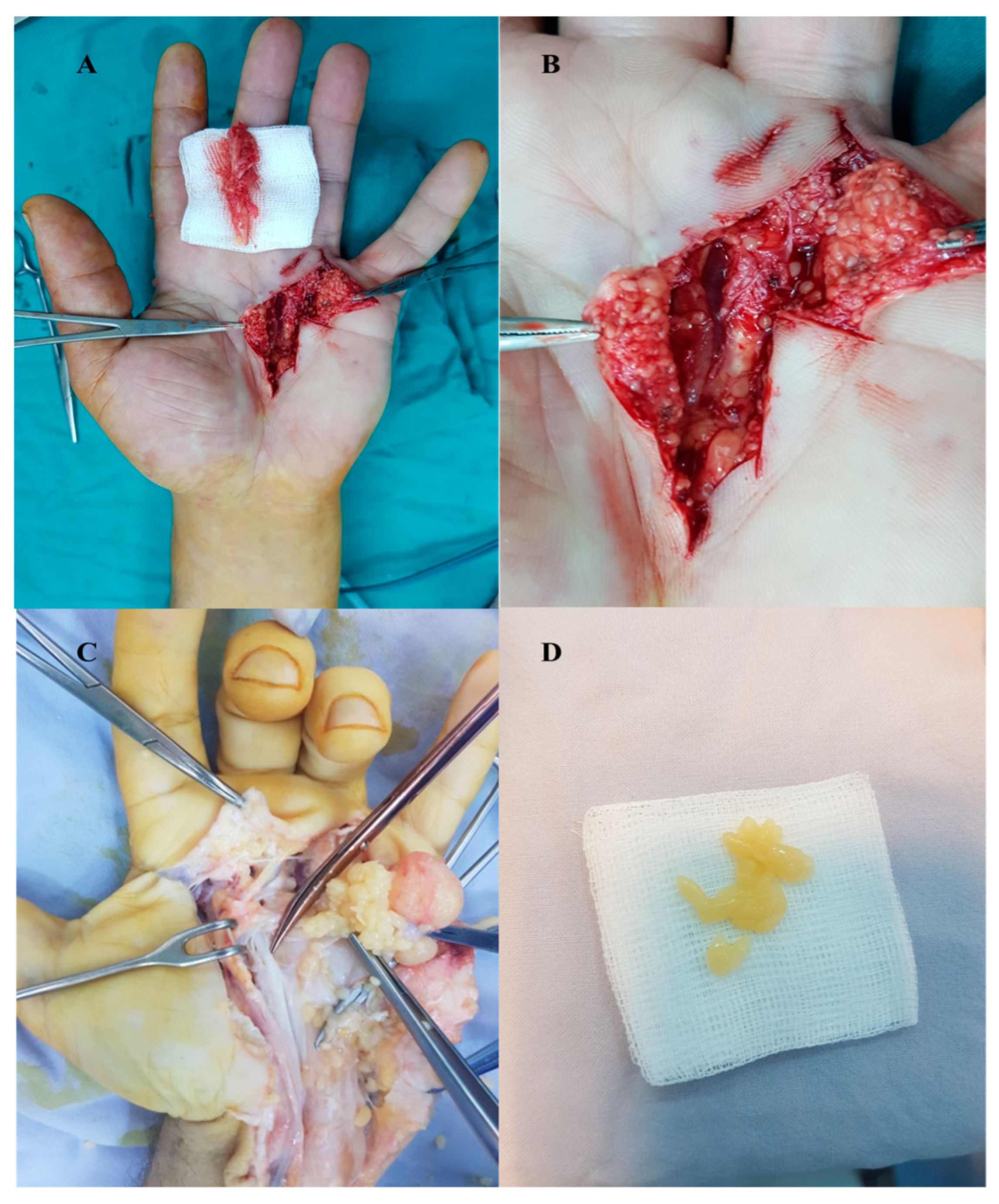
3.6. Idiopathic Tenosynovitis with “Rice Bodies”
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nepal, P.; Songme, S.; Alam, S.I.; Gandhi, D.; Ghimire, N.; Ojili, V. Common Soft Tissue Tumors Involving the Hand with Histopathological Correlation. J. Clin. Imaging Sci. 2019, 9, 15. [Google Scholar] [CrossRef]
- Pertea, M.; Filip, A.; Huzum, B.; Lunca, S.; Carp, C.; Mitrea, M.; Toader, P.; Luca, S.; Moraru, D.C.; Poroch, V.; et al. Schwannoma of the Upper Limb: Retrospective Study of a Rare Tumor with Uncommon Locations. Diagnostics 2022, 12, 1319. [Google Scholar] [CrossRef]
- Rodriguez, F.J.; Folpe, A.L.; Giannini, C.; Perry, A. Pathology of Peripheral Nerve Sheath Tumors: Diagnostic Overview and Update on Selected Diagnostic Problems. Acta Neuropathol. 2012, 123, 295–319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pertea, M.; Lunca, S.; Filip, A.; Moraru, D.C.; Carp, C.; Pinzaru, R.; Poroch, V.; Veliceasa, B. Atypical Sites of the Lipoma on the Hand and Fingers: Clinical and Imaging Features and Surgical Outcomes. Diagnostics 2022, 12, 2286. [Google Scholar] [CrossRef] [PubMed]
- Magro, G.; Broggi, G.; Angelico, G.; Puzzo, L.; Vecchio, G.M.; Virzì, V.; Ruggieri, M. Practical Approach to Histological Diagnosis of Peripheral Nerve Sheath Tumors: An Update. Diagnostics 2022, 12, 1463. [Google Scholar] [CrossRef]
- Zhou, H.Y.; Jiang, S.; Ma, F.X.; Lu, H. Peripheral nerve tumors of the hand: Clinical features, diagnosis, and treatment. World J. Clin. Cases 2020, 8, 5086–5098. [Google Scholar] [CrossRef]
- Shimosawa, H.; Susa, M.; Honma, T.; Hiraishi, E.; Sakihara, H. Soft tissue mixed tumor of the hand. Rare Tumors 2009, 1, 90–92. [Google Scholar] [CrossRef] [PubMed]
- Pagonis, T.; Givissis, P.; Christodoulou, A. Complications arising from a misdiagnosed giant lipoma of the hand and palm: A case report. J. Med. Case Rep. 2011, 5, 552. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nadar, M.M.; Bartoli, C.R.; Kasdan, M.L. Lipomas of the hand: A review and 13 patient case series. Eplasty 2010, 10, e66. [Google Scholar]
- Pertea, M.; Terinte, C.; Poroch, V.; Velenciuc, N.; Lunca, S. Nail bed solitary neurofibroma. Medicine 2018, 98, e14111-4. [Google Scholar] [CrossRef]
- Perţea, M.; Veliceasa, B.; Velenciuc, N.; Terinte, C.; Mitrea, M.; Ciobanu, P.; Alexa, O.; Luncă, S. Idiopathic tenosynovitis with rice bodies. Rom. J. Morphol. Embryol. 2020, 61, 457–463. [Google Scholar] [CrossRef]
- Yavari, M.; Afshar, A.; Shahraki, S.S.; Tabrizi, A.; Doorandish, N. Management of Symptomatic Lipoma of the Hand: A Case Series and Review of Literature. Arch. Bone Jt. Surg. 2022, 10, 530–535. [Google Scholar] [PubMed]
- Al Lahham, S.; Aljassem, G.; Omari, R.Y.; Alyazji, Z.; Sada, R.; Asnaf, A.; Abuelgasim, M. Diffuse Type Neurofibroma of the Forearm. Plast. Reconstr. Surg. Glob. Open 2022, 10, E4341. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.S.; Lee, D.G.; Lee, D.H.; Hwang, J.H.; Lee, S.Y. Slowly growing solitary neurofibroma of the thumb: A case report. Medicine 2021, 15, e23611. [Google Scholar] [CrossRef] [PubMed]
- Lodi, G.; Sannino, M.; Canarozzo, G.; Bennardo, L.; Nistico, S.P. Pulsed laser prior to CO2 laser ablation to treat multiple cutaneous neurofibromas in von Recklinghausen’s disease: A case report. Dermatol. Ther. 2022, 35, e15355. [Google Scholar] [CrossRef]
- Pertea, M.; Poroch, V.; Velenciuc, N.; Mitrea, M.; Lunca, S.; Terinte, C.; Filip, A.; Alexa, O.; Veliceasa, B. Clinical, histopathological and immunohistochemical features of glomus tumor of the nail bed. Rom. J. Morphol. Embriol. 2020, 62, 233–238. [Google Scholar] [CrossRef] [PubMed]
- Dasgupta, R.; Kumar, B. Giant Schwannoma on Thenar Aspect of the Hand: A Rare Case Report. Niger. J. Surg. 2021, 27, 75–77. [Google Scholar] [CrossRef] [PubMed]
- Pertea, M.; Poroch, V.; Issa, R.; Grosu, O.M.; Luncă, S. Large sized epidermal inclusion cyst of the palm-clincal, laboratory and histological findings. Rom. J. Funct. Clin. Macro Microsc. Anat. Anthropol. Rev. Rom. Anat. Funct. Clin. Macro Microsc. Antropol. 2016, 15, 329–333. [Google Scholar]
- Tian, Y.; Zhou, H.B.; Kai Yi, K.; Wang, K.J. Idiopathic tenosynovitis of the wrist with multiple rice bodies: A case report and review of literature. World J. Clin. Cases 2022, 16, 11908–11920. [Google Scholar] [CrossRef]
- Jiang, S.; Shen, H.; Lu, H. Multiple schwannomas of the digital nerves and common palmar digital nerves: An unusual case report of multiple schwannomas in one hand. Medicine 2019, 98, e14605. [Google Scholar] [CrossRef] [PubMed]
- Troy, J.; Barnes, C.; Gaviria, A.; Payne, W. Schwannoma in Digital Nerve: A Rare Case Report. Eplasty 2015, 15, ic56. [Google Scholar]
- Refalo, A.; Mallina, R. Benign Schwannoma of the Thumb; a diagnostic challenge. Radiol. Case Rep. 2022, 17, 477–480. [Google Scholar] [CrossRef]
- Lee, S.J.; Yoon, S.T. Ultrasonographic and Clinical Characteristics of Schwannoma of the Hand. Clin. Orthop. Surg. 2017, 9, 91–95. [Google Scholar] [CrossRef] [PubMed]
- Shinohara, T.; Hirata, H. Glomus Tumor Originating from a Digital Nerve. Plast. Reconstr. Surg. Glob. Open 2019, 7, e2053. [Google Scholar] [CrossRef] [PubMed]
- Jawalkar, H.; Maryada, V.R.; Brahmajoshyula, V.; Kumar, V.; Kotha, G. Subungual glomus tumors of the hand: Treated by transungual excision. Indian J. Orthop. 2015, 49, 403–407. [Google Scholar] [CrossRef] [PubMed]
- Singh, D.; Garg, R.S.; Vikas; Garg, Y.; Arora, V. Glomus tumor—A Rarity; M.R.I—A big help in early Diagnosis. J. Ortop. Case Rep. 2016, 6, 38–39. [Google Scholar]
- Mavric, M.; LaChaud, G.; Nguyev, A.; Scott, M.A.; Dry, S.M.; James, A.W. Clinical and histopathological diagnosis of glomus tumor: An institutional experience of 138 cases. Int. J. Surg. Pathol. 2015, 23, 181–188. [Google Scholar]
- Tellier, B.; Gabrian, M.; Jaquet, J.B. Carpal tunnel syndrome caused by a giant lipoma of the hand: A case report. Int. J. Surg. Case Rep. 2021, 80, 105647. [Google Scholar] [CrossRef]
- Kim, H.W.; Lee, K.J.; Choi, S.K.; Jang, I.T.; Lee, H.J. A large palmar lipoma arising from flexor tenosynovium of the hand causing digital nerve compression: A case report. Jt. Dis. Relat. Surg. 2021, 32, 230–233. [Google Scholar] [CrossRef]
- Kim, K.S.; Lee, H.; Lim, D.S.; Hwang, J.H.; Lee, S.Y. Giant lipoma in the hand: A case report. Medicine 2019, 98, e18434. [Google Scholar] [CrossRef] [PubMed]
- Park, H.Y.; Sur, Y.J.; Kim, Y.V. Epidermal Inclusion Cyst after Carpal Tunnel Release: A Case Report. J. Wrist Surg. 2016, 5, 67–70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gomi, M.; Naito, K.; Obayashi, O. A large epidermoid cyst developing in the palm: A case report. Int. J. Surg. Case Rep. 2013, 4, 773–777. [Google Scholar] [CrossRef] [Green Version]
- Teh, J. Ultrasound of soft tissue masses of the hand. J. Ultrason. 2012, 12, 381–401. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hewitt, C.; Man, K.; Prashanth, N.; Kubba, F.; Shaerf, D. Case Report of a Distal Phalanx Interosseous Epidermoid Inclusion Cyst Presenting as an Enchondroma. J. Orthop. Case Rep. 2022, 12, 62–65. [Google Scholar] [CrossRef]
- Reda, F.M.; Grimi Talal, G.; Moncef, B.; Reda-Allah, B.; Omar, L.M.; Saleh, B.M. Mass of the thenar eminence hiding idiopathic massive rice bodies formation with a compression of the median nerve: Case report and review of the literature. Int. J. Surg. Case Rep. 2018, 50, 28–31. [Google Scholar] [CrossRef] [PubMed]
- Perdikakis, E.; Tsifountoudis, I.; Kalaitzoglou, I.; Rountas, C.; Malliaropoulos, N.; Maffulli, N. Soft tissue pseudotumours: A pictorial review with emphasis on MRI. Muscles Ligaments Tendons J. 2017, 7, 353–375. [Google Scholar] [CrossRef] [PubMed]
- Ge, L.; Zhang, L.; Lu, L. Stenosing tenosynovitis with rice bodies formation diagnosed by ultrasound: A case report. Medicine 2022, 18, e28871. [Google Scholar] [CrossRef] [PubMed]















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Diagnostic | Cases | F | M | Age (Mean) | History | |
|---|---|---|---|---|---|---|
| 1 | Neurofibroma | 2 | 2 | 0 | 34 y | 9 m–1 y |
| 2 | Glomus Tumor | 15 | 13 | 2 | 40.13 y | 6 m–3 y |
| 3 | Schwanomma | 22 | 19 | 3 | 54.49 y | 1–3 y |
| 4 | Lipoma | 30 | 13 | 17 | 53.06 y | 1–8 y |
| 5 | Inclusion Epidermal Cyst | 3 | 0 | 3 | 45 y | 4–12 y |
| 6 | Idiopathic Tenosynovitis with “rice bodies” | 8 | 3 | 5 | 54.87 y | 1–4 y |
| Diagnostic | Clinical Findings | Clinical Tests | Macroscopic Intraoperative Aspects | |
|---|---|---|---|---|
| 1 | Neurofibroma |
|
| Solid, well-defined nodule-like tumor. White-pink aspect in cases with nail bed involvement |
| 2 | Glomus Tumor |
|
| Nodular lesion of small dimensions, well defined, with translucent or white wall |
| 3 | Schwanomma |
|
| Consistent tumor mass, well defined, mobile in the transverse plane, translucent white |
| 4 | Lipoma |
|
| Relatively mobile tumor mass with a soft consistency was detected in cases with wrist, thenar eminence and finger location. Immobile tumor mass in cases with mid-palm localization |
| 5 | Inclusion Epidermal Cyst |
|
| Relatively firm, fixed on deep planes, covered by teguments with normal appearance. Thin white capsule, relatively friable, with yogurt-like content, in some cases with intimate contact with other structures (tendons, vascular-nerve bundles) |
| 6 | Idiopathic Tenosynovitis with “rice bodies” |
|
|
| Diagnostic | Rx Exam | USG | MRI | |
|---|---|---|---|---|
| 1 | Neurofibroma |
| Nodular tumor mass, well delimited, with polycyclic appearance, hypoechoic | - |
| 2 | Glomus Tumor |
| Difficult to examine due to the pain produced by simple touch. Small, well-defined, hypoechoic tumor. Echo-doppler—intratumoral vascularization | - |
| 3 | Schwanomma | The tumor mass is well-defined, hypoechoic, homogeneous, in direct connection with the peripheral nerve from which it originates | Tumor mass with moderate hyperintense feature in T1-weighted images and hyperintense feature on fluid-sensitive aspects | |
| 4 | Lipoma |
| Well-defined hyperechoic, homogeneous tumor mass. Vascularization: absent | Well-defined tumor mass within its own capsule, with lipomatous signal (hypersignal in T1 and T2 and hyposignal in STIR images). In some cases—fine septa inside the tumor with discrete gadolinophilia |
| 5 | Inclusion Epidermal Cyst |
| Well-defined tumor mass with a relatively thick wall and homogeneous content | Well-defined cystic tumor formation, with hypersignal in T2 and hyposignal in T1 |
| 6 | Idiopathic Tenosynovitis with “rice bodies” |
| Well-defined tumor mass with both solid and liquid content (mixed) | Well-defined lobular, multiloculated tumor formation, heterogeneous with hyposignal in T1 and iso/hypersignal in T2. Numerous small hyposignal areas in T2; T1-weighted sequence showing a mass with low signal intensity surrounding the tendons |
| Diagnostic | HP | IHC | ||
| 1 | Neurofibroma | Non-incapsulated, low and moderate cellularity, cells loosely arranged; spindle shape cells with small amount of cytoplasm; cells with smaller size than schwannoma cells; cells with round, ovoid or comma-shaped nuclei separated by collagen fibers and myxoidmateria, lnerve not often identified especially in solitary tumors. | S100 | + |
| CD34 | + | |||
| 2 | Glomus Tumor | Insular and trabecular architecture; the presence of a fibrous capsule at the periphery; small, uniform, well-demarcated glomerular cells; small round nuclei centrally located in the cell; homogeneous chromatin; pale nucleoli; amphophilic or pale eosinophilic cytoplasm. | α-SMA | + |
| CD34 | + | |||
| h-Caldesmon | + | |||
| S100 | − | |||
| CK AE1/AE3 | − | |||
| P63 | − | |||
| 3 | Schwanomma | Encapsulated biphasic tumors with compact areas of spindle cells (Antoni A) alternating with loose foci (Antoni B); some hypercellularity; infrequent collagen bundles; Verocay bodies showing palisade; nerves often identifiable; o NF1, occasionally NF2. Cystic degeneration can sometimes be visualized. | S100 | + |
| CD34 | + | |||
| Collagen IV | + | |||
| SMA | − | |||
| 4 | Lipoma | Mature adipose tissue; the fat contains small capillaries within thin fibrous strands; thin fibrous capsule is often seen; necrosis and other inflammatory changes may be seen when lipomas are traumatized. | - | |
| 5 | Inclusion Epidermal Cyst | Cyst lining by stratified squamous epithelium with a granular layer—key feature. No significant nuclear atypia. Contains keratin–acellular, lamellar appearance.+/− Granulomatous inflammation due to rupture. | - | |
| 6 | Idiopathic Tenosynovitis with “rice bodies” | Proliferative synovitis with synovial cell hyperplasia and hypertrophy; Fibrin organized in the form of rice bodies, some nodules with central cartilaginous transformation; Fibrotic nodules surrounded by histiocytes; Epithelioid granulomas with multinucleated giant cell, some of them Langhans cell-like. | - | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pertea, M.; Grosu, O.M.; Filip, A.; Moraru, D.C.; Luca, S.; Fotea, M.-C.; Lunca, S.; Olinici, D.; Poroch, V.; Carp, C.; et al. Rare Benign Tumors and Tumor-like Lesions of the Hand without Skin Damage—Clinical, Imagistic and Histopathological Diagnosis, Retrospective Study. Diagnostics 2023, 13, 1204. https://doi.org/10.3390/diagnostics13061204
Pertea M, Grosu OM, Filip A, Moraru DC, Luca S, Fotea M-C, Lunca S, Olinici D, Poroch V, Carp C, et al. Rare Benign Tumors and Tumor-like Lesions of the Hand without Skin Damage—Clinical, Imagistic and Histopathological Diagnosis, Retrospective Study. Diagnostics. 2023; 13(6):1204. https://doi.org/10.3390/diagnostics13061204
Chicago/Turabian StylePertea, Mihaela, Oxana Madalina Grosu, Alexandru Filip, Dan Cristian Moraru, Stefana Luca, Madalina-Cristina Fotea, Sorinel Lunca, Doinita Olinici, Vladimir Poroch, Claudiu Carp, and et al. 2023. "Rare Benign Tumors and Tumor-like Lesions of the Hand without Skin Damage—Clinical, Imagistic and Histopathological Diagnosis, Retrospective Study" Diagnostics 13, no. 6: 1204. https://doi.org/10.3390/diagnostics13061204