
Mammaglobin-A Expression Is Highly Specific for Tumors Derived from the Breast, the Female Genital Tract, and the Salivary Gland
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Tissue Microarrays (TMAs)
2.2. Immunohistochemistry (IHC)
2.3. Statistics
3. Results
3.1. Technical Issues
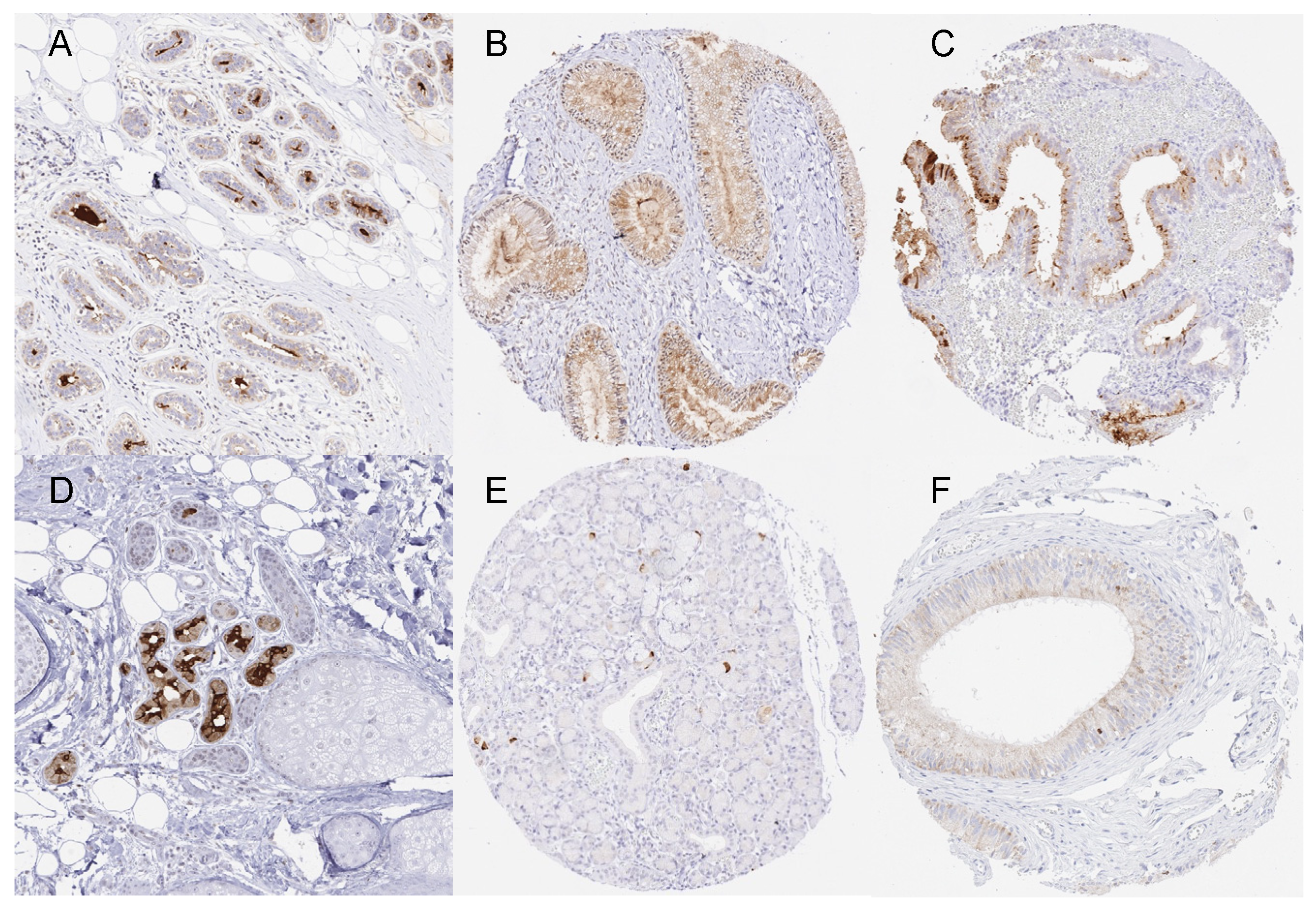
3.2. Mammaglobin-A in Normal Tissue
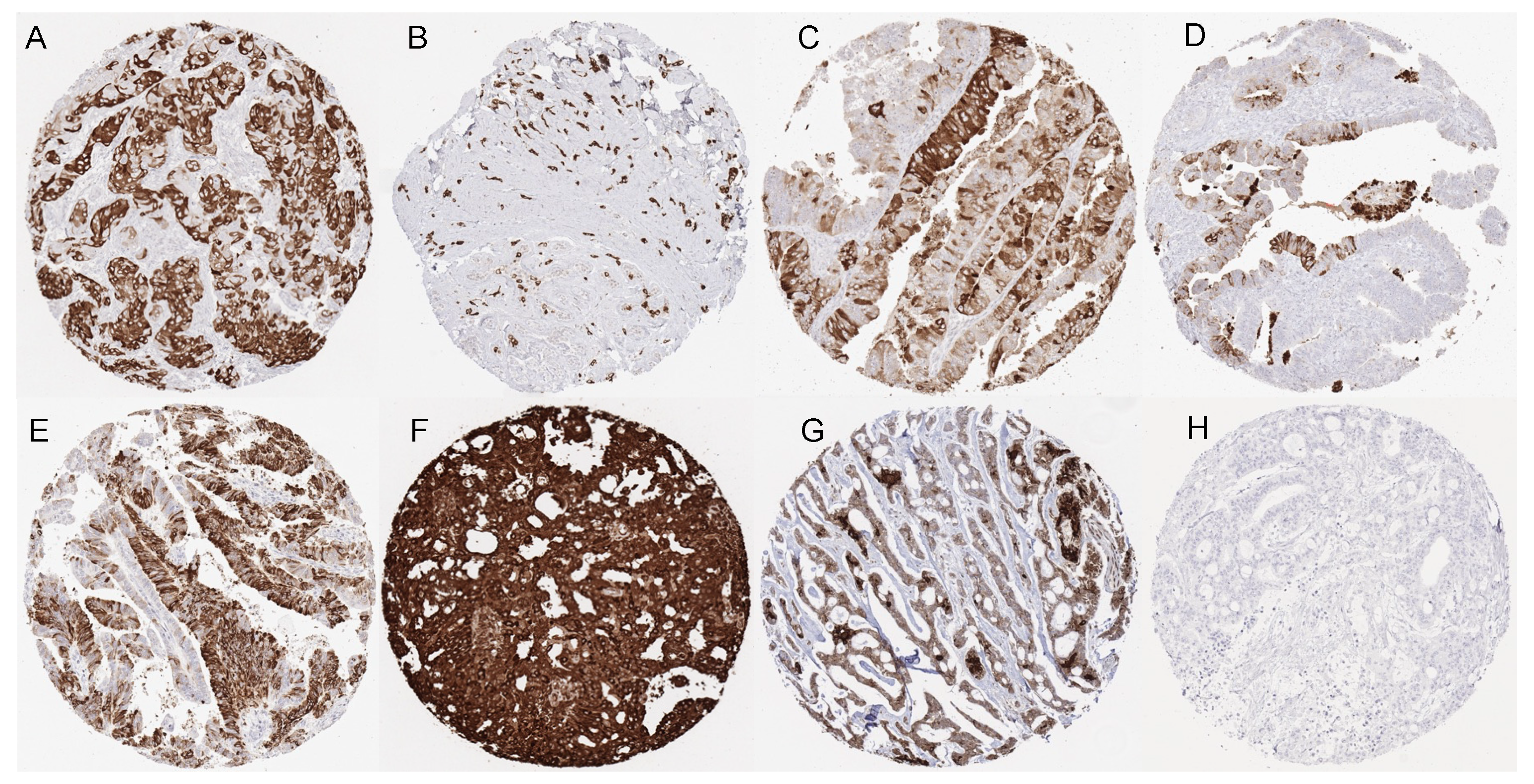
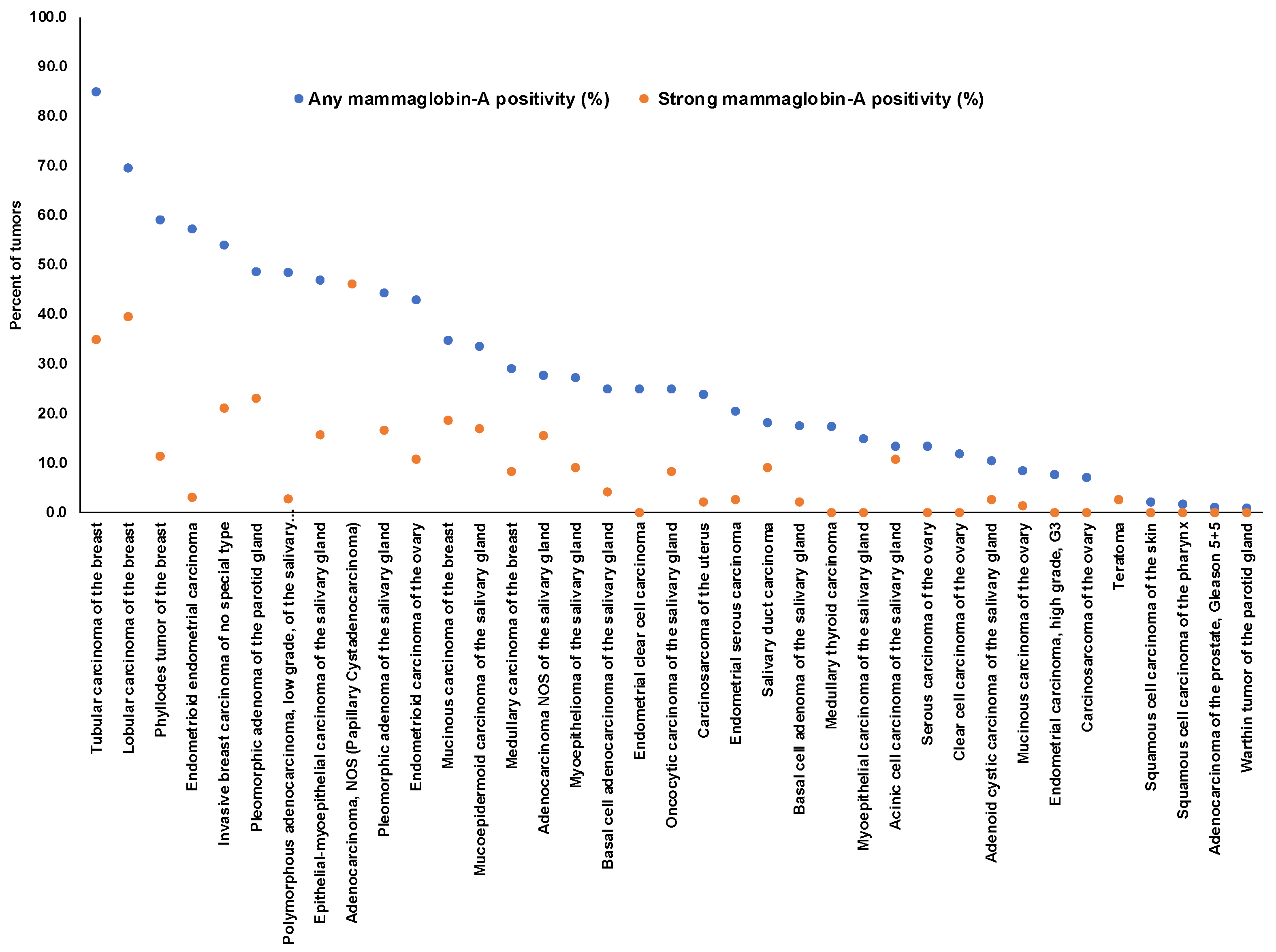
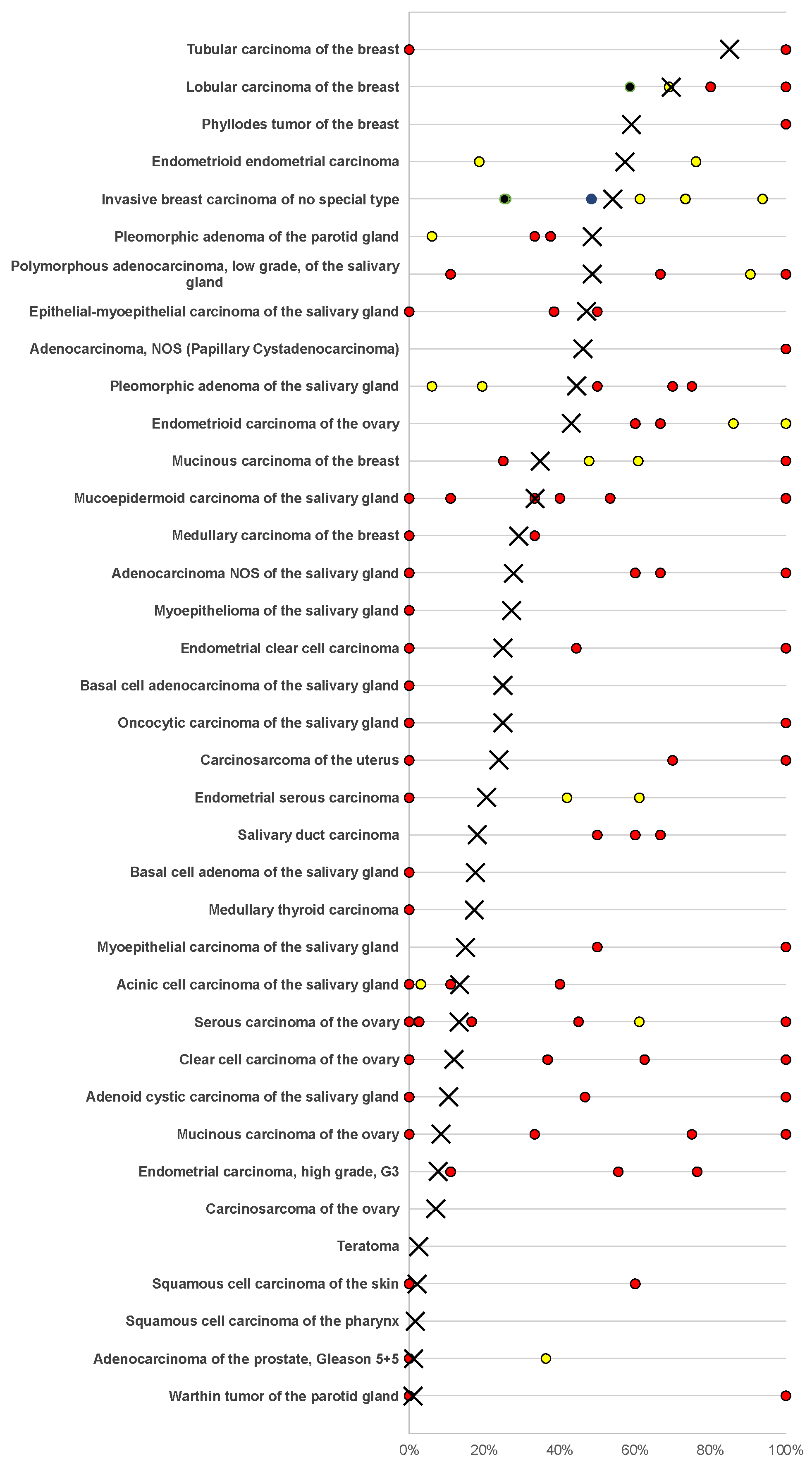
3.3. Mammaglobin-A in Neoplastic Tissues
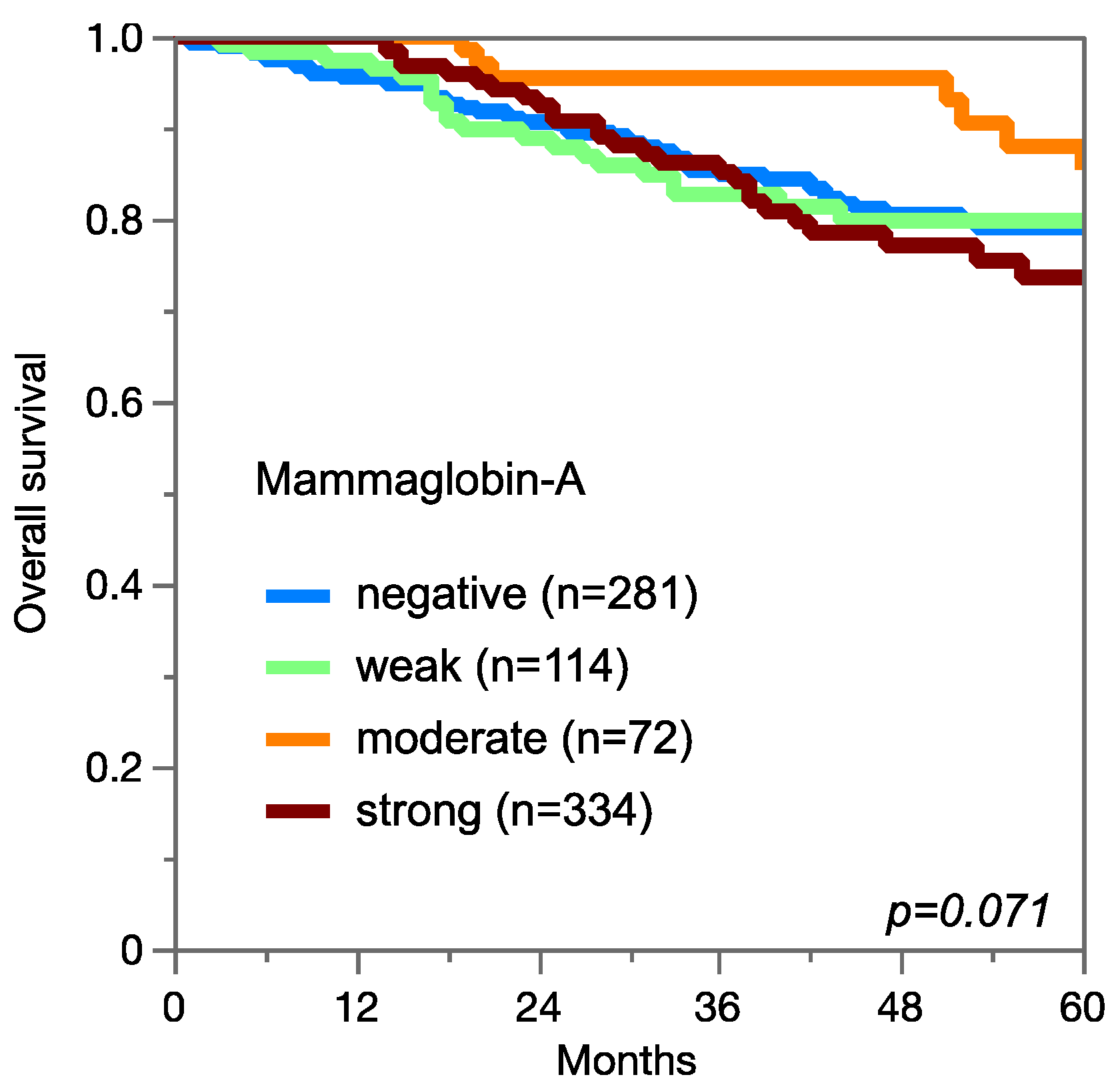
3.4. Mammaglobin-A Expression, Tumor Phenotype, and Prognosis
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Watson, M.A.; Darrow, C.; Zimonjic, D.B.; Popescu, N.C.; Fleming, T.P. Structure and transcriptional regulation of the human mammaglobin gene, a breast cancer associated member of the uteroglobin gene family localized to chromosome 11q13. Oncogene 1998, 16, 817–824. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Watson, M.A.; Watson, M.A.; Fleming, T.P. Mammaglobin, a mammary-specific member of the uteroglobin gene family, is overexpressed in human breast cancer. Cancer. Res. 1996, 56, 860–865. [Google Scholar] [PubMed]
- Ni, J.; Kalff-Suske, M.; Gentz, R.; Schageman, J.; Beato, M.; Klug, J. All human genes of the uteroglobin family are localized on chromosome 11q12.2 and form a dense cluster. Ann. N. Y. Acad. Sci. 2000, 923, 25–42. [Google Scholar] [CrossRef] [PubMed]
- Becker, R.M.; Darrow, C.; Zimonjic, D.B.; Popescu, N.C.; Watson, M.A.; Fleming, T.P. Identification of mammaglobin B, a novel member of the uteroglobin gene family. Genomics 1998, 54, 70–78. [Google Scholar] [CrossRef] [PubMed]
- Brown, N.M.; Stenzel, T.T.; Friedman, P.N.; Henslee, J.; Huper, G.; Marks, J.R. Evaluation of expression based markers for the detection of breast cancer cells. Breast Cancer Res. Treat. 2006, 97, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Mukherjee, A.B.; Kundu, G.C.; Mantile-Selvaggi, G.; Yuan, C.J.; Mandal, A.K.; Chattopadhyay, S.; Zheng, F.; Pattabiraman, N.; Zhang, Z. Uteroglobin: A novel cytokine? Cell Mol. Life Sci. 1999, 55, 771–787. [Google Scholar] [CrossRef]
- Mukherjee, A.B.; Kundu, G.C.; Mandal, A.K.; Pattabiraman, N.; Yuan, C.J.; Zhang, Z. Uteroglobin: Physiological role in normal glomerular function uncovered by targeted disruption of the uteroglobin gene in mice. Am. J. Kidney. Dis. 1998, 32, 1106–1120. [Google Scholar] [CrossRef]
- Miele, L. Antiflammins Bioactive peptides derived from uteroglobin. Ann. N. Y. Acad. Sci. 2000, 923, 128–140. [Google Scholar] [CrossRef]
- Miele, L.; Cordella-Miele, E.; Mukherjee, A.B. Uteroglobin: Structure, molecular biology, and new perspectives on its function as a phospholipase A2 inhibitor. Endocr. Rev. 1987, 8, 474–490. [Google Scholar] [CrossRef]
- Vasanthakumar, G.; Manjunath, R.; Mukherjee, A.B.; Warabi, H.; Schiffmann, E. Inhibition of phagocyte chemotaxis by uteroglobin, an inhibitor of blastocyst rejection. Biochem. Pharmacol. 1988, 37, 389–394. [Google Scholar] [CrossRef]
- Levin, S.W.; Butler, J.D.; Schumacher, U.K.; Wightman, P.D.; Mukherjee, A.B. Uteroglobin inhibits phospholipase A2 activity. Life Sci. 1986, 38, 1813–1819. [Google Scholar] [CrossRef] [PubMed]
- Al Joudi, F.S. Human mammaglobin in breast cancer: A brief review of its clinical utility. Indian J. Med. Res. 2014, 139, 675–685. [Google Scholar] [PubMed]
- Carter, D.; Douglass, J.F.; Cornellison, C.D.; Retter, M.W.; Johnson, J.C.; Bennington, A.A.; Fleming, T.P.; Reed, S.G.; Houghton, R.L.; Diamond, D.L.; et al. Purification and characterization of the mammaglobin/lipophilin B complex, a promising diagnostic marker for breast cancer. Biochemistry 2002, 41, 6714–6722. [Google Scholar] [CrossRef] [PubMed]
- Zafrakas, M.; Petschke, B.; Donner, A.; Fritzsche, F.; Kristiansen, G.; Knuchel, R.; Dahl, E. Expression analysis of mammaglobin A (SCGB2A2) and lipophilin B (SCGB1D2) in more than 300 human tumors and matching normal tissues reveals their co-expression in gynecologic malignancies. BMC Cancer 2006, 6, 88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Z.; Yang, X.; Duan, C.; Li, J.; Tong, R.; Fan, Y.; Feng, J.; Cao, R.; Zhong, W.; Feng, X.; et al. Identification and characterization of mammaglobin-A epitope in heterogenous breast cancers for enhancing tumor-targeting therapy. Signal. Transduct. Target. 2020, 5, 82. [Google Scholar] [CrossRef]
- Picot, N.; Guerrette, R.; Beauregard, A.P.; Jean, S.; Michaud, P.; Harquail, J.; Benzina, S.; Robichaud, G.A. Mammaglobin 1 promotes breast cancer malignancy and confers sensitivity to anticancer drugs. Mol. Carcinog. 2016, 55, 1150–1162. [Google Scholar] [CrossRef]
- Koh, E.H.; Cho, Y.W.; Mun, Y.J.; Ryu, J.H.; Kim, E.J.; Choi, D.S.; Maeng, K.Y.; Han, J.; Kang, D. Upregulation of human mammaglobin reduces migration and invasion of breast cancer cells. Cancer. Investig. 2014, 32, 22–29. [Google Scholar] [CrossRef]
- Sjodin, A.; Ljuslinder, I.; Henriksson, R.; Hedman, H. Mammaglobin and lipophilin B expression in breast tumors and their lack of effect on breast cancer cell proliferation. Anticancer Res. 2008, 28, 1493–1498. [Google Scholar]
- De Lara, S.; Parris, T.Z.; Werner, R.E.; Helou, K.; Kovacs, A. GATA3 as a putative marker of breast cancer metastasis-A retrospective immunohistochemical study. Breast J. 2018, 24, 184–188. [Google Scholar] [CrossRef]
- Talaat, I.M.; Hachim, M.Y.; Hachim, I.Y.; Ibrahim, R.A.E.; Ahmed, M.; Tayel, H.Y. Bone marrow mammaglobin-1 (SCGB2A2) immunohistochemistry expression as a breast cancer specific marker for early detection of bone marrow micrometastases. Sci. Rep. 2020, 10, 13061. [Google Scholar] [CrossRef]
- Shaoxian, T.; Baohua, Y.; Xiaoli, X.; Yufan, C.; Xiaoyu, T.; Hongfen, L.; Rui, B.; Xiangjie, S.; Ruohong, S.; Wentao, Y. Characterisation of GATA3 expression in invasive breast cancer: Differences in histological subtypes and immunohistochemically defined molecular subtypes. J. Clin. Pathol. 2017, 70, 926–934. [Google Scholar] [CrossRef] [PubMed]
- Dyhdalo, K.S.; Booth, C.N.; Brainard, J.A.; Croyle, M.C.; Kolosiwsky, A.M.; Goyal, A.; Gildea, T.R.; Almeida, F.A.; Nassar, A.; Reynolds, J.P. Utility of GATA3, mammaglobin, GCDFP-15, and ER in the detection of intrathoracic metastatic breast carcinoma. J. Am. Soc. Cytopathol. 2015, 4, 218–224. [Google Scholar] [CrossRef] [PubMed]
- Huo, L.; Zhang, J.; Gilcrease, M.Z.; Gong, Y.; Wu, Y.; Zhang, H.; Resetkova, E.; Hunt, K.K.; Deavers, M.T. Gross cystic disease fluid protein-15 and mammaglobin A expression determined by immunohistochemistry is of limited utility in triple-negative breast cancer. Histopathology 2013, 62, 267–274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cimino, P.J., Jr.; Perrin, R.J. Mammaglobin-A immunohistochemistry in primary central nervous system neoplasms and intracranial metastatic breast carcinoma. Appl. Immunohistochem. Mol. Morphol. 2014, 22, 442–448. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sasaki, E.; Tsunoda, N.; Hatanaka, Y.; Mori, N.; Iwata, H.; Yatabe, Y. Breast-specific expression of MGB1/mammaglobin: An examination of 480 tumors from various organs and clinicopathological analysis of MGB1-positive breast cancers. Mod. Pathol. 2007, 20, 208–214. [Google Scholar] [CrossRef] [Green Version]
- Hagemann, I.S.; Pfeifer, J.D.; Cao, D. Mammaglobin expression in gynecologic adenocarcinomas. Hum. Pathol. 2013, 44, 628–635. [Google Scholar] [CrossRef]
- Bellone, S.; Tassi, R.; Betti, M.; English, D.; Cocco, E.; Gasparrini, S.; Bortolomai, I.; Black, J.D.; Todeschini, P.; Romani, C.; et al. Mammaglobin B (SCGB2A1) is a novel tumour antigen highly differentially expressed in all major histological types of ovarian cancer: Implications for ovarian cancer immunotherapy. Br. J. Cancer 2013, 109, 462–471. [Google Scholar] [CrossRef] [Green Version]
- Kandalaft, P.L.; Simon, R.A.; Isacson, C.; Gown, A.M. Comparative Sensitivities and Specificities of Antibodies to Breast Markers GCDFP-15, Mammaglobin A, and Different Clones of Antibodies to GATA-3: A Study of 338 Tumors Using Whole Sections. Appl. Immunohistochem. Mol. Morphol. 2016, 24, 609–614. [Google Scholar] [CrossRef]
- Kononen, J.; Bubendorf, L.; Kallioniemi, A.; Barlund, M.; Schraml, P.; Leighton, S.; Torhorst, J.; Mihatsch, M.J.; Sauter, G.; Kallioniemi, O.P. Tissue microarrays for high-throughput molecular profiling of tumor specimens. Nat. Med. 1998, 4, 844–847. [Google Scholar] [CrossRef]
- Mirlacher, M.; Simon, R. Recipient block TMA technique. Methods Mol. Biol. 2010, 664, 37–44. [Google Scholar]
- Simon, R.; Mirlacher, M.; Sauter, G. Immunohistochemical analysis of tissue microarrays. Methods Mol. Biol. 2010, 664, 113–126. [Google Scholar] [PubMed]
- Uhlen, M.; Bandrowski, A.; Carr, S.; Edwards, A.; Ellenberg, J.; Lundberg, E.; Rimm, D.L.; Rodriguez, H.; Hiltke, T.; Snyder, M.; et al. A proposal for validation of antibodies. Nat. Methods 2016, 13, 823–827. [Google Scholar] [CrossRef]
- Thul, P.J.; Akesson, L.; Wiking, M.; Mahdessian, D.; Geladaki, A.; Ait Blal, H.; Alm, T.; Asplund, A.; Bjork, L.; Breckels, L.M.; et al. A subcellular map of the human proteome. Science 2017, 356, 6340. [Google Scholar] [CrossRef] [PubMed]
- Lizio, M.; Harshbarger, J.; Shimoji, H.; Severin, J.; Kasukawa, T.; Sahin, S.; Abugessaisa, I.; Fukuda, S.; Hori, F.; Ishikawa-Kato, S.; et al. Gateways to the FANTOM5 promoter level mammalian expression atlas. Genome. Biol. 2015, 16, 22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lizio, M.; Abugessaisa, I.; Noguchi, S.; Kondo, A.; Hasegawa, A.; Hon, C.C.; de Hoon, M.; Severin, J.; Oki, S.; Hayashizaki, Y.; et al. Update of the FANTOM web resource: Expansion to provide additional transcriptome atlases. Nucleic. Acids Res. 2019, 47, D752–D758. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Consortium, G.T. The Genotype-Tissue Expression (GTEx) project. Nat. Genet. 2013, 45, 580–585. [Google Scholar]
- Tassi, R.A.; Bignotti, E.; Falchetti, M.; Calza, S.; Ravaggi, A.; Rossi, E.; Martinelli, F.; Bandiera, E.; Pecorelli, S.; Santin, A.D. Mammaglobin B expression in human endometrial cancer. Int. J. Gynecol. Cancer. 2008, 18, 1090–1096. [Google Scholar] [CrossRef]
- Soares, C.D.; de Lima Morais, T.M.; Carlos, R.; Martins, M.D.; de Almeida, O.P.; Mariano, F.V.; Altemani, A. Immunohistochemical expression of mammaglobin in salivary duct carcinomas de novo and salivary duct carcinoma ex pleomorphic adenoma. Hum. Pathol. 2019, 92, 59–66. [Google Scholar] [CrossRef]
- Sauter, G.; Simon, R.; Hillan, K. Tissue microarrays in drug discovery. Nat. Rev. Drug Discov. 2003, 2, 962–972. [Google Scholar] [CrossRef]
- Miettinen, M.; McCue, P.A.; Sarlomo-Rikala, M.; Rys, J.; Czapiewski, P.; Wazny, K.; Langfort, R.; Waloszczyk, P.; Biernat, W.; Lasota, J.; et al. GATA3: A multispecific but potentially useful marker in surgical pathology: A systematic analysis of 2500 epithelial and nonepithelial tumors. Am. J. Surg. Pathol. 2014, 38, 13–22. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Zhang, T. Human mammaglobin: A specific marker for breast cancer prognosis. J. BUON 2016, 21, 35–41. [Google Scholar] [PubMed]
- Lee, G.W.; Kim, J.Y.; Koh, E.H.; Kang, D.; Choi, D.S.; Maeng, K.Y.; Lee, J.S. Plasma human mammaglobin mRNA associated with poor outcome in patients with breast cancer. Genet. Mol. Res. 2012, 11, 4034–4042. [Google Scholar] [CrossRef] [PubMed]
- Nunez-Villar, M.J.; Martinez-Arribas, F.; Pollan, M.; Lucas, A.R.; Sanchez, J.; Tejerina, A.; Schneider, J. Elevated mammaglobin (h-MAM) expression in breast cancer is associated with clinical and biological features defining a less aggressive tumour phenotype. Breast Cancer Res. 2003, 5, R65–R70. [Google Scholar] [CrossRef] [Green Version]
- Raica, M.; Cimpean, A.M.; Meche, A.; Alexa, A.; Suciu, C.; Muresan, A. Analysis of the immunohistochemical expression of mammaglobin A in primary breast carcinoma and lymph node metastasis. Rom. J. Morphol. Embryol. 2009, 50, 341–347. [Google Scholar]
- Span, P.N.; Waanders, E.; Manders, P.; Heuvel, J.J.; Foekens, J.A.; Watson, M.A.; Beex, L.V.; Sweep, F.C. Mammaglobin is associated with low-grade, steroid receptor-positive breast tumors from postmenopausal patients, and has independent prognostic value for relapse-free survival time. J. Clin. Oncol. 2004, 22, 691–698. [Google Scholar] [CrossRef] [PubMed]
- Guan, X.F.; Hamedani, M.K.; Adeyinka, A.; Walker, C.; Kemp, A.; Murphy, L.C.; Watson, P.H.; Leygue, E. Relationship between mammaglobin expression and estrogen receptor status in breast tumors. Endocrine 2003, 21, 245–250. [Google Scholar] [CrossRef] [PubMed]
- Baker, E.; Whiteoak, N.; Hall, L.; France, J.; Wilson, D.; Bhaskar, P. Mammaglobin-A, VEGFR3, and Ki67 in Human Breast Cancer Pathology and Five Year Survival. Breast Cancer Auckl. 2019, 13, 1178223419858957. [Google Scholar] [CrossRef] [PubMed]
- Ni, Y.B.; Tsang, J.Y.; Chan, S.K.; Tse, G.M. GATA-binding protein 3, gross cystic disease fluid protein-15 and mammaglobin have distinct prognostic implications in different invasive breast carcinoma subgroups. Histopathology 2015, 67, 96–105. [Google Scholar] [CrossRef] [PubMed]
- Fritzsche, F.R.; Thomas, A.; Winzer, K.J.; Beyer, B.; Dankof, A.; Bellach, J.; Dahl, E.; Dietel, M.; Kristiansen, G. Co-expression and prognostic value of gross cystic disease fluid protein 15 and mammaglobin in primary breast cancer. Histol. Histopathol. 2007, 22, 1221–1230. [Google Scholar] [PubMed]
- Friedmann-Morvinski, D.; Verma, I.M. Dedifferentiation and reprogramming: Origins of cancer stem cells. EMBO Rep. 2014, 15, 244–253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jopling, C.; Boue, S.; Izpisua Belmonte, J.C. Dedifferentiation, transdifferentiation and reprogramming: Three routes to regeneration. Nat. Rev. Mol. Cell Biol. 2011, 12, 79–89. [Google Scholar] [CrossRef] [PubMed]
- Lerret, N.M.; Rogozinska, M.; Jaramillo, A.; Marzo, A.L. Adoptive transfer of Mammaglobin-A epitope specific CD8 T cells combined with a single low dose of total body irradiation eradicates breast tumors. PLoS ONE 2012, 7, e41240. [Google Scholar] [CrossRef] [Green Version]
- Cui, H.; Zhang, W.; Hu, W.; Liu, K.; Wang, T.; Ma, N.; Liu, X.; Liu, Y.; Jiang, Y. Recombinant mammaglobin A adenovirus-infected dendritic cells induce mammaglobin A-specific CD8+ cytotoxic T lymphocytes against breast cancer cells in vitro. PLoS ONE 2013, 8, e63055. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Viehl, C.T.; Frey, D.M.; Phommaly, C.; Chen, T.; Fleming, T.P.; Gillanders, W.E.; Eberlein, T.J.; Goedegebuure, P.S. Generation of mammaglobin-A-specific CD4 T cells and identification of candidate CD4 epitopes for breast cancer vaccine strategies. Breast Cancer Res. Treat. 2008, 109, 305–314. [Google Scholar] [CrossRef] [PubMed]
- Tiriveedhi, V.; Sarma, N.J.; Subramanian, V.; Fleming, T.P.; Gillanders, W.E.; Mohanakumar, T. Identification of HLA-A24-restricted CD8(+) cytotoxic T-cell epitopes derived from mammaglobin-A, a human breast cancer-associated antigen. Hum. Immunol. 2012, 73, 11–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ilias Basha, H.; Tiriveedhi, V.; Fleming, T.P.; Gillanders, W.E.; Mohanakumar, T. Identification of immunodominant HLA-B7-restricted CD8+ cytotoxic T cell epitopes derived from mammaglobin-A expressed on human breast cancers. Breast Cancer Res. Treat. 2011, 127, 81–89. [Google Scholar] [CrossRef]
- Soysal, S.D.; Muenst, S.; Kan-Mitchell, J.; Huarte, E.; Zhang, X.; Wilkinson-Ryan, I.; Fleming, T.; Tiriveedhi, V.; Mohanakumar, T.; Li, L.; et al. Identification and translational validation of novel mammaglobin-A CD8 T cell epitopes. Breast Cancer Res. Treat. 2014, 147, 527–537. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.W.; Goedegebuure, P.; Gillanders, W.E. Mammaglobin-A is a target for breast cancer vaccination. Oncoimmunology 2016, 5, e1069940. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mammaglobin-A Immunostaining | |||||||
|---|---|---|---|---|---|---|---|
| Tumor Entity | on TMA (n) | Anal. (n) | Neg. (%) | Weak (%) | Mod. (%) | Str. (%) | |
| Tumors of the skin | Pilomatricoma | 35 | 32 | 100.0 | 0.0 | 0.0 | 0.0 |
| Basal cell carcinoma | 88 | 83 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Benign nevus | 29 | 29 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Squamous cell carcinoma of the skin | 90 | 90 | 97.8 | 2.2 | 0.0 | 0.0 | |
| Malignant melanoma | 48 | 45 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Merkel cell carcinoma | 46 | 41 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Tumors of the head and neck | Squamous cell carcinoma of the larynx | 110 | 105 | 100.0 | 0.0 | 0.0 | 0.0 |
| Squamous cell carcinoma of the pharynx | 60 | 59 | 98.3 | 1.7 | 0.0 | 0.0 | |
| Oral squamous cell carcinoma (floor of the mouth) | 130 | 129 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Pleomorphic adenoma of the parotid gland | 50 | 39 | 51.3 | 10.3 | 15.4 | 23.1 | |
| Warthin tumor of the parotid gland | 104 | 98 | 99.0 | 0.0 | 1.0 | 0.0 | |
| Adenocarcinoma, NOS (papillary cystadenocarcinoma) | 14 | 13 | 53.8 | 0.0 | 0.0 | 46.2 | |
| Salivary duct carcinoma | 15 | 11 | 81.8 | 9.1 | 0.0 | 9.1 | |
| Acinic cell carcinoma of the salivary gland | 181 | 148 | 86.5 | 1.4 | 1.4 | 10.8 | |
| Adenocarcinoma NOS of the salivary gland | 109 | 83 | 72.3 | 6.0 | 6.0 | 15.7 | |
| Adenoid cystic carcinoma of the salivary gland | 180 | 114 | 89.5 | 7.9 | 0.0 | 2.6 | |
| Basal cell adenocarcinoma of the salivary gland | 25 | 24 | 75.0 | 20.8 | 0.0 | 4.2 | |
| Basal cell adenoma of the salivary gland | 101 | 91 | 82.4 | 9.9 | 5.5 | 2.2 | |
| Epithelial–myoepithelial carcinoma of the salivary gland | 53 | 51 | 52.9 | 23.5 | 7.8 | 15.7 | |
| Mucoepidermoid carcinoma of the salivary gland | 343 | 259 | 66.4 | 9.7 | 6.9 | 17.0 | |
| Myoepithelial carcinoma of the salivary gland | 21 | 20 | 85.0 | 5.0 | 10.0 | 0.0 | |
| Myoepithelioma of the salivary gland | 11 | 11 | 72.7 | 18.2 | 0.0 | 9.1 | |
| Oncocytic carcinoma of the salivary gland | 12 | 12 | 75.0 | 16.7 | 0.0 | 8.3 | |
| Polymorphous adenocarcinoma, low grade, of the salivary gland | 41 | 35 | 51.4 | 34.3 | 11.4 | 2.9 | |
| Pleomorphic adenoma of the salivary gland | 53 | 36 | 55.6 | 13.9 | 13.9 | 16.7 | |
| Tumors of the lung, pleura, and thymus | Adenocarcinoma of the lung | 246 | 176 | 100.0 | 0.0 | 0.0 | 0.0 |
| Squamous cell carcinoma of the lung | 130 | 69 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Small cell carcinoma of the lung | 20 | 16 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Mesothelioma, epithelioid | 39 | 28 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Mesothelioma, biphasic | 76 | 63 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Thymoma | 29 | 29 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Tumors of the female genital tract | Squamous cell carcinoma of the vagina | 78 | 73 | 100.0 | 0.0 | 0.0 | 0.0 |
| Squamous cell carcinoma of the vulva | 130 | 124 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Squamous cell carcinoma of the cervix | 130 | 125 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Endometrioid endometrial carcinoma | 236 | 225 | 42.7 | 43.6 | 10.7 | 3.1 | |
| Endometrial serous carcinoma | 82 | 73 | 79.5 | 17.8 | 0.0 | 2.7 | |
| Carcinosarcoma of the uterus | 48 | 46 | 76.1 | 21.7 | 0.0 | 2.2 | |
| Endometrial carcinoma, high grade, G3 | 13 | 13 | 92.3 | 7.7 | 0.0 | 0.0 | |
| Endometrial clear cell carcinoma | 8 | 8 | 75.0 | 25.0 | 0.0 | 0.0 | |
| Endometrioid carcinoma of the ovary | 110 | 93 | 57.0 | 25.8 | 6.5 | 10.8 | |
| Serous carcinoma of the ovary, high grade | 559 | 479 | 86.6 | 13.2 | 0.2 | 0.0 | |
| Mucinous carcinoma of the ovary | 96 | 71 | 91.5 | 5.6 | 1.4 | 1.4 | |
| Clear cell carcinoma of the ovary | 50 | 42 | 88.1 | 11.9 | 0.0 | 0.0 | |
| Carcinosarcoma of the ovary | 47 | 42 | 92.9 | 4.8 | 2.4 | 0.0 | |
| Brenner tumor | 9 | 9 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Tumors of the breast | Invasive breast carcinoma of no special type | 1391 | 1214 | 45.9 | 20.6 | 12.4 | 21.2 |
| Lobular carcinoma of the breast | 294 | 260 | 30.4 | 21.2 | 8.8 | 39.6 | |
| Medullary carcinoma of the breast | 26 | 24 | 70.8 | 12.5 | 8.3 | 8.3 | |
| Tubular carcinoma of the breast | 27 | 20 | 15.0 | 35.0 | 15.0 | 35.0 | |
| Mucinous carcinoma of the breast | 58 | 43 | 65.1 | 9.3 | 7.0 | 18.6 | |
| Phyllodes tumor of the breast | 50 | 44 | 40.9 | 34.1 | 13.6 | 11.4 | |
| Tumors of the digestive system | Adenomatous polyp, low-grade dysplasia | 50 | 50 | 100.0 | 0.0 | 0.0 | 0.0 |
| Adenomatous polyp, high-grade dysplasia | 50 | 49 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Adenocarcinoma of the colon | 1932 | 1808 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Gastric adenocarcinoma, diffuse type | 226 | 161 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Gastric adenocarcinoma, intestinal type | 224 | 167 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Gastric adenocarcinoma, mixed type | 62 | 56 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Adenocarcinoma of the esophagus | 133 | 82 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Squamous cell carcinoma of the esophagus | 124 | 71 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Squamous cell carcinoma of the anal canal | 91 | 85 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Cholangiocarcinoma | 50 | 49 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Hepatocellular carcinoma | 50 | 50 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Ductal adenocarcinoma of the pancreas | 662 | 593 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Pancreatic/ampullary adenocarcinoma | 119 | 86 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Acinar cell carcinoma of the pancreas | 14 | 13 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Gastrointestinal stromal tumor (GIST) | 50 | 49 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Tumors of the urinary system | Non-invasive papillary urothelial carcinoma, pTa G2 low grade | 177 | 141 | 100.0 | 0.0 | 0.0 | 0.0 |
| Non-invasive papillary urothelial carcinoma, pTa G2 high grade | 141 | 117 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Non-invasive papillary urothelial carcinoma, pTa G3 | 187 | 113 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Urothelial carcinoma, pT2-4 G3 | 1207 | 825 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Small cell neuroendocrine carcinoma of the bladder | 18 | 18 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Sarcomatoid urothelial carcinoma | 25 | 21 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Clear cell renal cell carcinoma | 858 | 824 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Papillary renal cell carcinoma | 255 | 232 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Clear cell (tubulo) papillary renal cell carcinoma | 21 | 20 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Chromophobe renal cell carcinoma | 131 | 122 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Oncocytoma | 177 | 162 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Tumors of the male genital organs | Adenocarcinoma of the prostate, Gleason 3 + 3 | 83 | 83 | 100.0 | 0.0 | 0.0 | 0.0 |
| Adenocarcinoma of the prostate, Gleason 4 + 4 | 80 | 80 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Adenocarcinoma of the prostate, Gleason 5 + 5 | 85 | 85 | 98.8 | 0.0 | 1.2 | 0.0 | |
| Adenocarcinoma of the prostate (recurrence) | 261 | 254 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Small cell neuroendocrine carcinoma of the prostate | 17 | 15 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Seminoma | 621 | 611 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Embryonal carcinoma of the testis | 50 | 44 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Yolk sac tumor | 50 | 43 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Teratoma | 50 | 38 | 97.4 | 0.0 | 0.0 | 2.6 | |
| Squamous cell carcinoma of the penis | 80 | 79 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Tumors of endocrine organs | Adenoma of the thyroid gland | 50 | 47 | 100.0 | 0.0 | 0.0 | 0.0 |
| Papillary thyroid carcinoma | 50 | 48 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Follicular thyroid carcinoma | 49 | 49 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Medullary thyroid carcinoma | 50 | 46 | 82.6 | 13.0 | 4.3 | 0.0 | |
| Anaplastic thyroid carcinoma | 26 | 24 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Adrenal cortical adenoma | 50 | 44 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Adrenal cortical carcinoma | 26 | 25 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Phaeochromocytoma | 50 | 48 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Pancreas, neuroendocrine tumor (NET) | 46 | 42 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Pancreas, neuroendocrine carcinoma (NEC) | 3 | 3 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Tumors of hematopoietic and lymphoid tissues | Hodgkin lymphoma | 103 | 100 | 100.0 | 0.0 | 0.0 | 0.0 |
| Non-Hodgkin lymphoma | 62 | 61 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Small lymphocytic lymphoma, B-cell type (B-SLL/B-CLL) | 50 | 50 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Diffuse large B-cell lymphoma (DLBCL) | 114 | 114 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Follicular lymphoma | 88 | 88 | 100.0 | 0.0 | 0.0 | 0.0 | |
| T-cell non-Hodgkin lymphoma | 24 | 24 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Mantle cell lymphoma | 18 | 18 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Marginal zone lymphoma | 16 | 16 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Diffuse large B-cell lymphoma (DLBCL) in the testis | 16 | 16 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Burkitt lymphoma | 5 | 3 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Tumors of soft tissue and bone | Tendosynovial giant cell tumor | 45 | 43 | 100.0 | 0.0 | 0.0 | 0.0 |
| Granular cell tumor | 53 | 43 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Leiomyoma | 50 | 47 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Leiomyosarcoma | 87 | 87 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Liposarcoma | 132 | 121 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Malignant peripheral nerve sheath tumor (MPNST) | 13 | 11 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Myofibrosarcoma | 26 | 26 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Angiosarcoma | 73 | 67 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Angiomyolipoma | 91 | 88 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Dermatofibrosarcoma protuberans | 21 | 18 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Ganglioneuroma | 14 | 14 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Kaposi sarcoma | 8 | 5 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Neurofibroma | 117 | 116 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Sarcoma, not otherwise specified (NOS) | 75 | 71 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Paraganglioma | 41 | 41 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Primitive neuroectodermal tumor (PNET) | 23 | 16 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Rhabdomyosarcoma | 7 | 7 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Schwannoma | 121 | 118 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Synovial sarcoma | 12 | 11 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Osteosarcoma | 43 | 36 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Chondrosarcoma | 38 | 17 | 100.0 | 0.0 | 0.0 | 0.0 | |
| Mammaglobin-A IHC | ||||||||
|---|---|---|---|---|---|---|---|---|
| n | Negative (%) | Weak (%) | Moderate (%) | Strong (%) | p | |||
| Breast cancer of no special type (NST) | Tumor stage | pT1 | 601 | 44.3 | 21.5 | 14.1 | 20.1 | 0.1421 |
| pT2 | 411 | 46.5 | 18.5 | 11.7 | 23.4 | |||
| pT3–4 | 84 | 54.8 | 16.7 | 6.0 | 22.6 | |||
| Grade | G1 | 176 | 37.5 | 21.6 | 13.6 | 27.3 | 0.0011 | |
| G2 | 590 | 41.9 | 21.7 | 13.7 | 22.7 | |||
| G3 | 372 | 54.3 | 19.4 | 10.8 | 15.6 | |||
| Nodal stage | pN0 | 515 | 44.1 | 21.6 | 14.6 | 19.8 | 0.3017 | |
| pN1 | 223 | 44.8 | 19.7 | 13.0 | 22.4 | |||
| pN2 | 69 | 53.6 | 15.9 | 5.8 | 24.6 | |||
| pN3 | 56 | 50.0 | 14.3 | 8.9 | 26.8 | |||
| HER2 status | neg | 851 | 47.1 | 20.8 | 11.2 | 20.9 | 0.4501 | |
| pos | 118 | 43.2 | 22.0 | 16.1 | 18.6 | |||
| ER status | neg | 200 | 63.5 | 14.5 | 9.5 | 12.5 | <0.0001 | |
| pos | 717 | 41.6 | 23.0 | 12.8 | 22.6 | |||
| PR status | neg | 390 | 55.4 | 17.7 | 10.5 | 16.4 | <0.0001 | |
| pos | 568 | 40.0 | 23.2 | 13.2 | 23.6 | |||
| Triple negative | no | 756 | 41.7 | 22.6 | 13.4 | 22.4 | <0.0001 | |
| yes | 134 | 75.4 | 10.4 | 5.2 | 9.0 | |||
| Endometrioid endometrial cancers | Tumor stage | pT1 | 113 | 33.6 | 48.7 | 14.2 | 3.5 | 0.0198 |
| pT2 | 24 | 50.0 | 37.5 | 12.5 | 0.0 | |||
| pT3–4 | 35 | 48.6 | 51.4 | 0.0 | 0.0 | |||
| pN0 | 50 | 36.0 | 56.0 | 6.0 | 2.0 | 0.0986 | ||
| Nodal stage | pN+ | 30 | 63.3 | 33.3 | 3.3 | 0.0 | ||
| Endometrioid ovarian cancer | Tumor stage | pT1 | 22 | 40.9 | 31.8 | 9.1 | 18.2 | 0.1686 |
| pT2 | 4 | 100.0 | 0.0 | 0.0 | 0.0 | |||
| pT3 | 5 | 80.0 | 20.0 | 0.0 | 0.0 | |||
| Nodal stage | pN0 | 20 | 40.0 | 35.0 | 10.0 | 15.0 | 0.3835 | |
| pN1 | 7 | 71.4 | 14.3 | 0.0 | 14.3 | |||
| Serous ovarian cancers | Tumor stage | pT1 | 31 | 77.4 | 22.6 | 0.0 | 0.0 | 0.2 |
| pT2 | 40 | 92.5 | 7.5 | 0.0 | 0.0 | |||
| pT3 | 245 | 88.2 | 11.8 | 0.0 | 0.0 | |||
| Nodal stage | pN0 | 78 | 83.3 | 16.7 | 0.0 | 0.0 | 0.3767 | |
| pN1 | 153 | 87.6 | 12.4 | 0.0 | 0.0 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gorbokon, N.; Timm, P.; Dum, D.; Menz, A.; Büscheck, F.; Völkel, C.; Hinsch, A.; Lennartz, M.; Luebke, A.M.; Hube-Magg, C.; et al. Mammaglobin-A Expression Is Highly Specific for Tumors Derived from the Breast, the Female Genital Tract, and the Salivary Gland. Diagnostics 2023, 13, 1202. https://doi.org/10.3390/diagnostics13061202
Gorbokon N, Timm P, Dum D, Menz A, Büscheck F, Völkel C, Hinsch A, Lennartz M, Luebke AM, Hube-Magg C, et al. Mammaglobin-A Expression Is Highly Specific for Tumors Derived from the Breast, the Female Genital Tract, and the Salivary Gland. Diagnostics. 2023; 13(6):1202. https://doi.org/10.3390/diagnostics13061202
Chicago/Turabian StyleGorbokon, Natalia, Patrick Timm, David Dum, Anne Menz, Franziska Büscheck, Cosima Völkel, Andrea Hinsch, Maximilian Lennartz, Andreas M Luebke, Claudia Hube-Magg, and et al. 2023. "Mammaglobin-A Expression Is Highly Specific for Tumors Derived from the Breast, the Female Genital Tract, and the Salivary Gland" Diagnostics 13, no. 6: 1202. https://doi.org/10.3390/diagnostics13061202